
Highly Aggressive Osteosarcoma of the Ethmoids and Maxillary Sinus-A Case of Successful Surgery and Proton Beam Radiotherapy in a 65-Year-Old Man

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report (Observation)
3. Discussion
- Clinical investigation of all parts of the head and neck (endoscopy to provide evidence of tumour).
- A tissue sample can be taken, if it is a safe procedure.
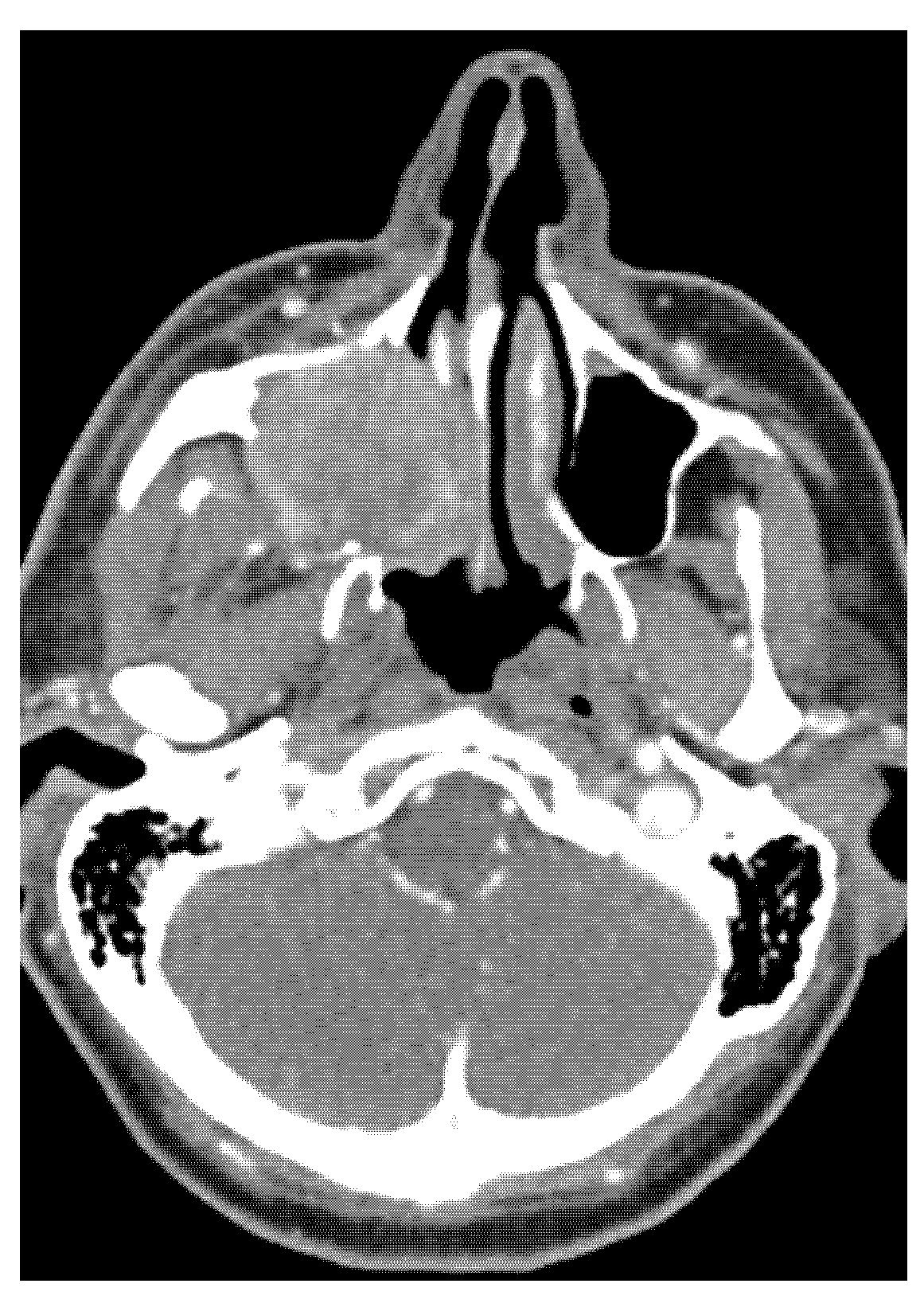
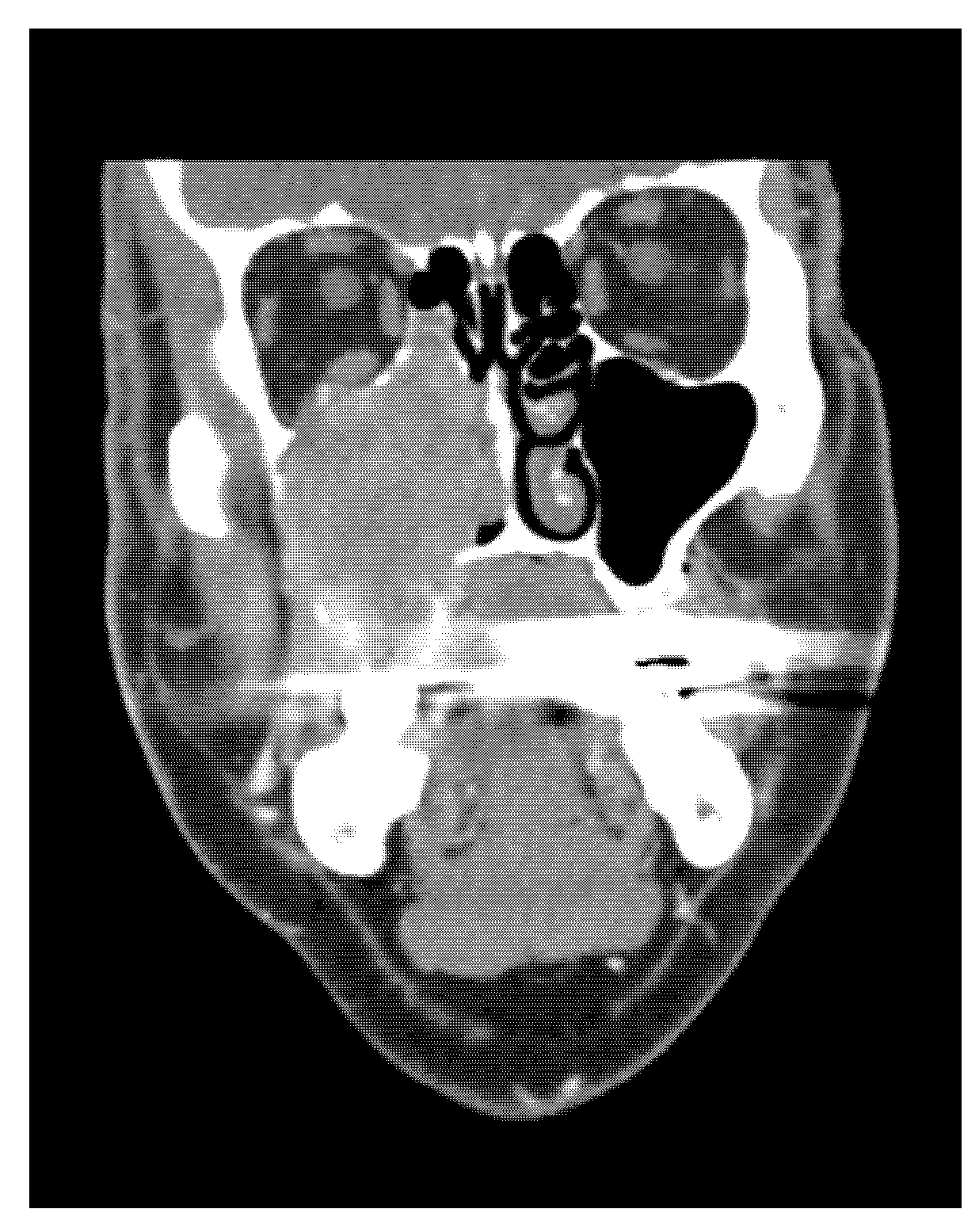
- CT, MRI scan (size, spread, and metastases of tumour mass), if necessary, PET scan, and USG.
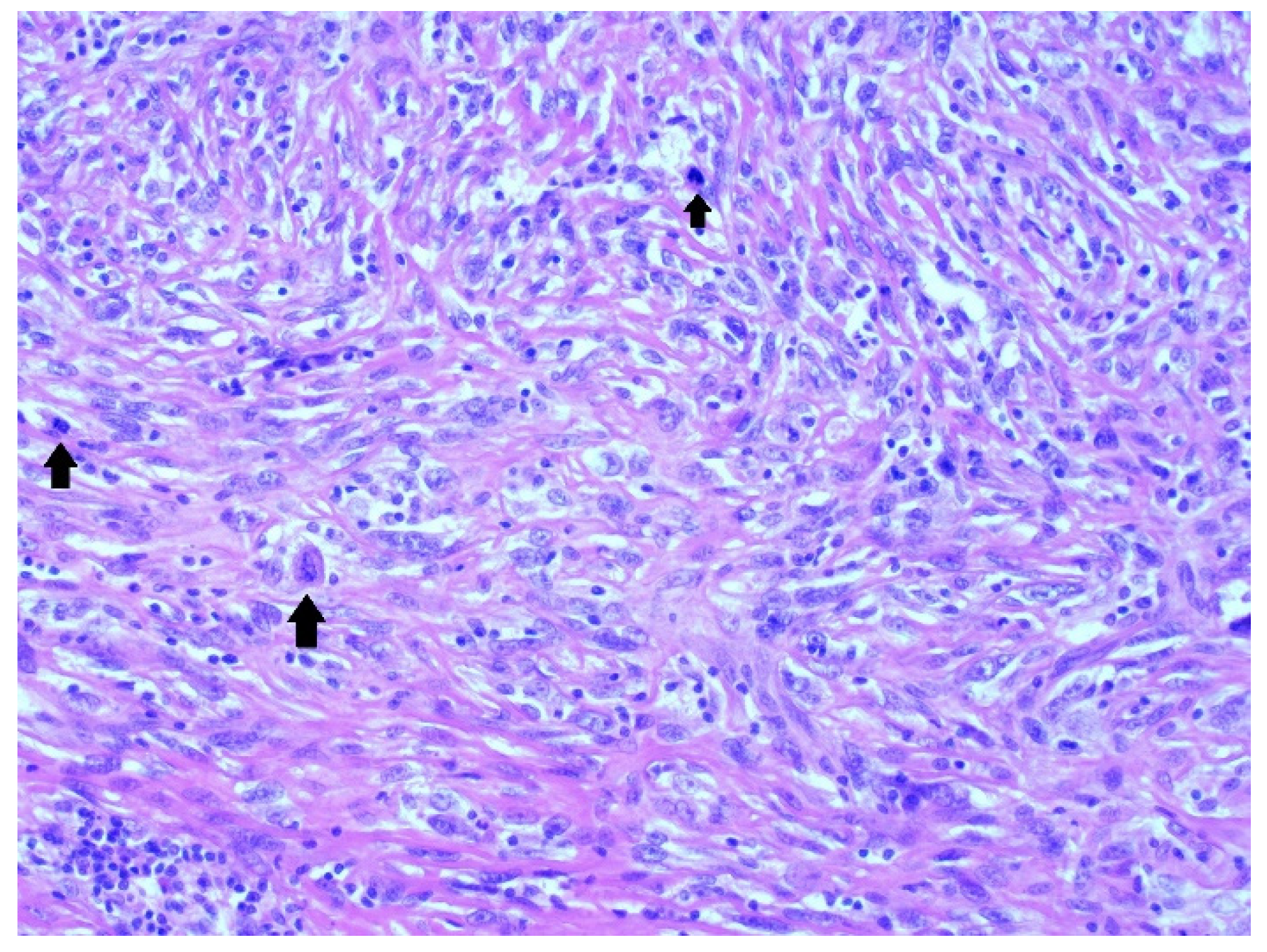
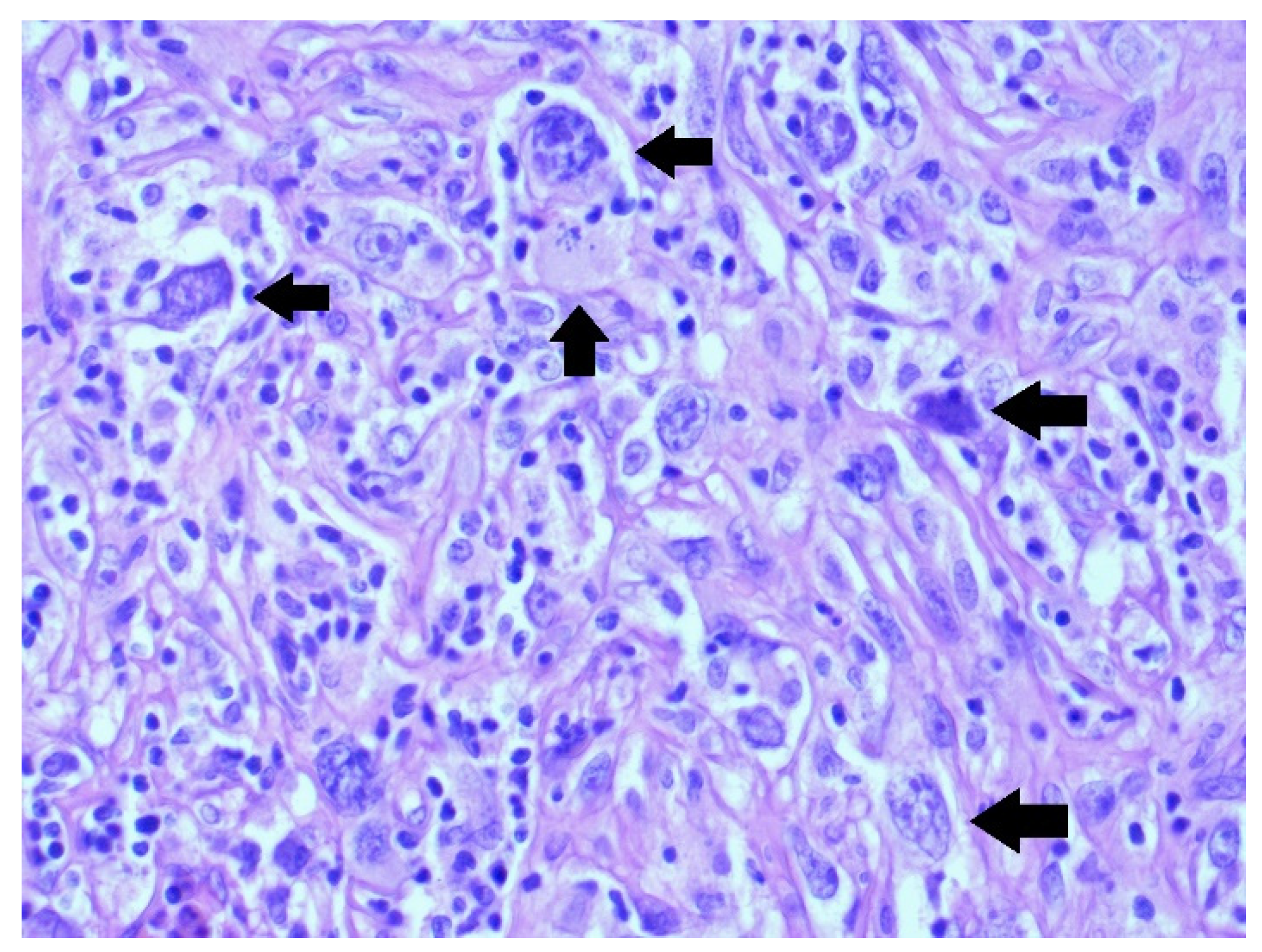
- Histopathology: complete investigation and extensive immunohistochemistry tests are necessary.
- Surgery: surgical therapy must be radical; the surgical margins are very important for grading of sarcomas in general.
- Radiotherapy: beam therapy (photon, proton, or isotope) depends on staging, including grading, histological type of sarcoma, and the radicality of surgery when performed.
- Chemotherapy: for aggressive histological subtypes of osteosarcoma, chemotherapy is necessary in many cases, a combination of vincristine, doxorubicin, cyclophosphamide, and etoposide have been used.
- A clinical report including endoscopic methods, Narrow band imaging endoscopy (NBI) and Ultrasonography (USG) every 4 months;
- MRI, once yearly (PET scan if necessary).
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soufflet, E.; Thibaut, F. Case report of maxillary osteosarcoma with up-to date review. J. Oral Med. Oral Surg. 2020, 26, 15. [Google Scholar] [CrossRef]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. Clin. Orthop. Relat. Res. 1980, 153, 106–120. [Google Scholar] [CrossRef]
- Murphey, M.D.; Kransdorf, M.J. Staging and Classification of Primary Musculoskeletal Bone and Soft-Tissue Tumors According to the 2020 WHO Update, From the AJR Special Series on Cancer Staging. AJR Am. J. Roentgenol. 2021, 217, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- ElKordy, M.A.; ElBaradie, T.S.; ElSebai, H.I.; KhairAlla, S.M.; Amin, A.A.E. Osteosarcoma of the jaw: Challenges in the diagnosis and treatment. J. Egypt. Natl. Cancer Inst. 2018, 30, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.; Kent, P.M. Young Adult with Osteosarcoma of the Mandible and the Challenge in Management: Review of the Pediatric and Adult Literatures. J. Pediatr. Hematol. Oncol. 2019, 41, 21–27. [Google Scholar] [CrossRef]
- Pires, M.D.; Martins, J.N.R.; Dias, G.S.; Doutel, D.; Ordinola-Zapata, R. Osteosarcoma of the anterior maxilla mimicking a periapical pathology: A case report. Aust. Endod. J. 2021, 47, 656–663. [Google Scholar] [CrossRef]
- Paparella, M.L.; Olvi, L.G.; Brandizzi, D.; Keszler, A.; Santini-Araujo, E.; Cabrini, R.L. Osteosarcoma of the jaw: An analysis of a series of 74 cases. Histopathology 2013, 63, 551–557. [Google Scholar] [CrossRef]
- Chbicheb, S.; Oujilal, A.; Wady, W. A propos d’un ostéosarcome maxillaire. Méd. Buccale Chir. Buccale 2007, 13, 205–212. [Google Scholar] [CrossRef]
- Hajji, F.; Meziane, M.; Boulaadas, M.; Benhalima, H.; Kzadri, M. Ostéosarcome des maxillaires: Présentation de deux cas. Méd. Buccale Chir. Buccale 2011, 17, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Luo, Z.; Chen, W.; Shen, X.; Qin, G.; Yuan, J.; Hu, B.; Lyu, J.; Wen, C.; Xu, W. Head and neck osteosarcoma: CT and MR imaging features. Dentomaxillofac. Radiol. 2020, 49, 20190202. [Google Scholar] [CrossRef]
- Chen, Y.; Shen, Q.; Gokavarapu, S.; Lin, C.; Yahiya; Cao, W.; Chauhan, S.; Liu, Z.; Ji, T.; Tian, Z. Osteosarcoma of head and neck: A retrospective study on prognostic factors from a single institute database. Oral Oncol. 2016, 58, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mücke, T.; Mitchell, D.A.; Tannapfel, A.; Wolff, K.D.; Loeffelbein, D.J.; Kanatas, A. Effect of neoadjuvant treatment in the management of osteosarcomas of the head and neck. J. Cancer Res. Clin. Oncol. 2014, 140, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Laskar, S.; Kakoti, S.; Khanna, N.; Manjali, J.J.; Mangaj, A.; Puri, A.; Gulia, A.; Nayak, P.; Pai, P.; Nair, D.; et al. Outcomes of osteosarcoma, chondrosarcoma and chordoma treated with image guided-intensity modulated radiation therapy. Radiother. Oncol. 2021, 164, 216–222. [Google Scholar] [CrossRef]
- Shim, T.; Chillakuru, Y.; Darwish, C.; Chalif, E.; Strum, D.; Benito, D.A.; Mulcahy, C.F.; Monfared, A. Head and neck osteosarcomas: Analysis of treatment trends and survival outcomes in the United States (2004–2016). Head Neck 2021, 43, 3294–3305. [Google Scholar] [CrossRef]
- Brady, J.S.; Chung, S.Y.; Marchiano, E.; Eloy, J.A.; Baredes, S.; Park, R.C.W. Pediatric head and neck bone sarcomas: An. analysis of 204 cases. Int. J. Pediatr. Otorhinolaryngol. 2017, 100, 71–76. [Google Scholar] [CrossRef]
- Kalavrezos, N.; Sinha, D. Head and neck sarcomas in adulthood: Current trends and evolving management concepts. Br. J. Oral. Maxillofac. Surg. 2020, 58, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Yamaoka, M.; Akiyama, M.; Yokokawa, Y.; Terao, Y.; Yokoi, K.; Kato, T.; Fukushima, T.; Sakurai, H.; Ida, H. Multidisciplinary therapy including proton beam radiotherapy for a Ewing sarcoma family tumor of maxillary sinus in a 4-year-old girl. Head Neck 2013, 35, E386–E390. [Google Scholar] [CrossRef] [PubMed]
- Boon, E.; van der Graaf, W.T.; Gelderblom, H.; Tesselaar, M.E.; van Es, R.J.; Oosting, S.F.; de Bree, R.; van Meerten, E.; Hoeben, A.; Smeele, L.E.; et al. Impact of chemotherapy on the outcome of osteosarcoma of the head and neck in adults. Head Neck 2017, 39, 140–146. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. The TNM Classification of Malignant Tumours, 8th ed.; Wiley Blackwell: Oxford, UK, 2017; pp. 36–39. [Google Scholar]
- Han, S.; Yin, X.; Xu, W.; Wang, Y.; Han, W. The Management of Head and Neck Sarcoma. J. Craniofac. Surg. 2020, 31, e189–e192. [Google Scholar] [CrossRef]
- Seng, D.; Wu, J.; Fang, Q.; Liu, F. Prognosis of osteosarcomas in the mandible: 15-year experience of 55 patients. Medicine 2019, 98, e13875. [Google Scholar] [CrossRef]
- Jung, J.H.; Huh, K.H.; Yong, T.H.; Kang, J.H.; Kim, J.E.; Yi, W.J.; Heo, M.S.; Lee, S.S. Differentiation of osteosarcoma from osteomyelitis using microarchitectural analysis on panoramic radiographs. Sci Rep. 2022, 12, 12339. [Google Scholar] [CrossRef]
- Sain, B.; Gupta, A.; Ghosh, S.; Mondal, R.R.; Bhattacharya, S.; Ghose, A. Osteosarcoma of the maxilla presenting as a chronic pyogenic abscess: A case report. Int. J. Surg. Case Rep. 2021, 87, 106425. [Google Scholar] [CrossRef]
- Gore, M.R. Treatment, outcomes, and demographics in sinonasal sarcoma: A systematic review of the literature. BMC Ear Nose Throat Disord. 2018, 18, 4. [Google Scholar] [CrossRef] [Green Version]
- Yao, W.; Hou, J.; Liu, G.; Wu, F.; Yan, Q.; Guo, L.; Wang, C. LncRNA CBR3-AS1 promotes osteosarcoma progression through the network of miR-140-5p/DDX54-NUCKS1-mTOR signaling pathway. Mol. Ther. Oncol. 2022, 25, 189–200. [Google Scholar] [CrossRef]
- Lu, J.; Kang, X.; Wang, Z.; Zhao, G.; Jiang, B. The activity level of follicular helper T cells in the peripheral blood of osteosarcoma patients is associated with poor prognosis. Bioengineered 2022, 13, 3751–3759. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Astl, J.; Belsan, T.; Michnova, L.; Kubeš, J.; Filipovsky, T.; Blecha, J.; Holy, R. Highly Aggressive Osteosarcoma of the Ethmoids and Maxillary Sinus-A Case of Successful Surgery and Proton Beam Radiotherapy in a 65-Year-Old Man. Medicina 2022, 58, 1141. https://doi.org/10.3390/medicina58091141
Astl J, Belsan T, Michnova L, Kubeš J, Filipovsky T, Blecha J, Holy R. Highly Aggressive Osteosarcoma of the Ethmoids and Maxillary Sinus-A Case of Successful Surgery and Proton Beam Radiotherapy in a 65-Year-Old Man. Medicina. 2022; 58(9):1141. https://doi.org/10.3390/medicina58091141
Chicago/Turabian StyleAstl, Jaromír, Tomas Belsan, Ludmila Michnova, Jiří Kubeš, Tomas Filipovsky, Jiri Blecha, and Richard Holy. 2022. "Highly Aggressive Osteosarcoma of the Ethmoids and Maxillary Sinus-A Case of Successful Surgery and Proton Beam Radiotherapy in a 65-Year-Old Man" Medicina 58, no. 9: 1141. https://doi.org/10.3390/medicina58091141