
In-Hospital Clinical Outcomes in Patients with Fragility Fractures of the Lumbar Spine, Thoracic Spine, and Pelvic Ring: A Comparison of Data before and after Certification as a DGU® Geriatric Trauma Centre

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Certification as a DGU® Geriatric Trauma Centre (GTC)
2.2. Study Population
2.3. Demographic Characteristics and Medical Complexity of the Study Population
2.4. In-Hospital Courses before and after GTC Certification
2.5. New in-Hospital Findings and Diagnoses
2.6. Adapted Clavien–Dindo Scoring System in Trauma (ACDiT)
2.7. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Medical Complexity of the Study Population
3.2. In-Hospital Course before and after GTC Certification
3.3. New in-Hospital Findings and Diagnoses
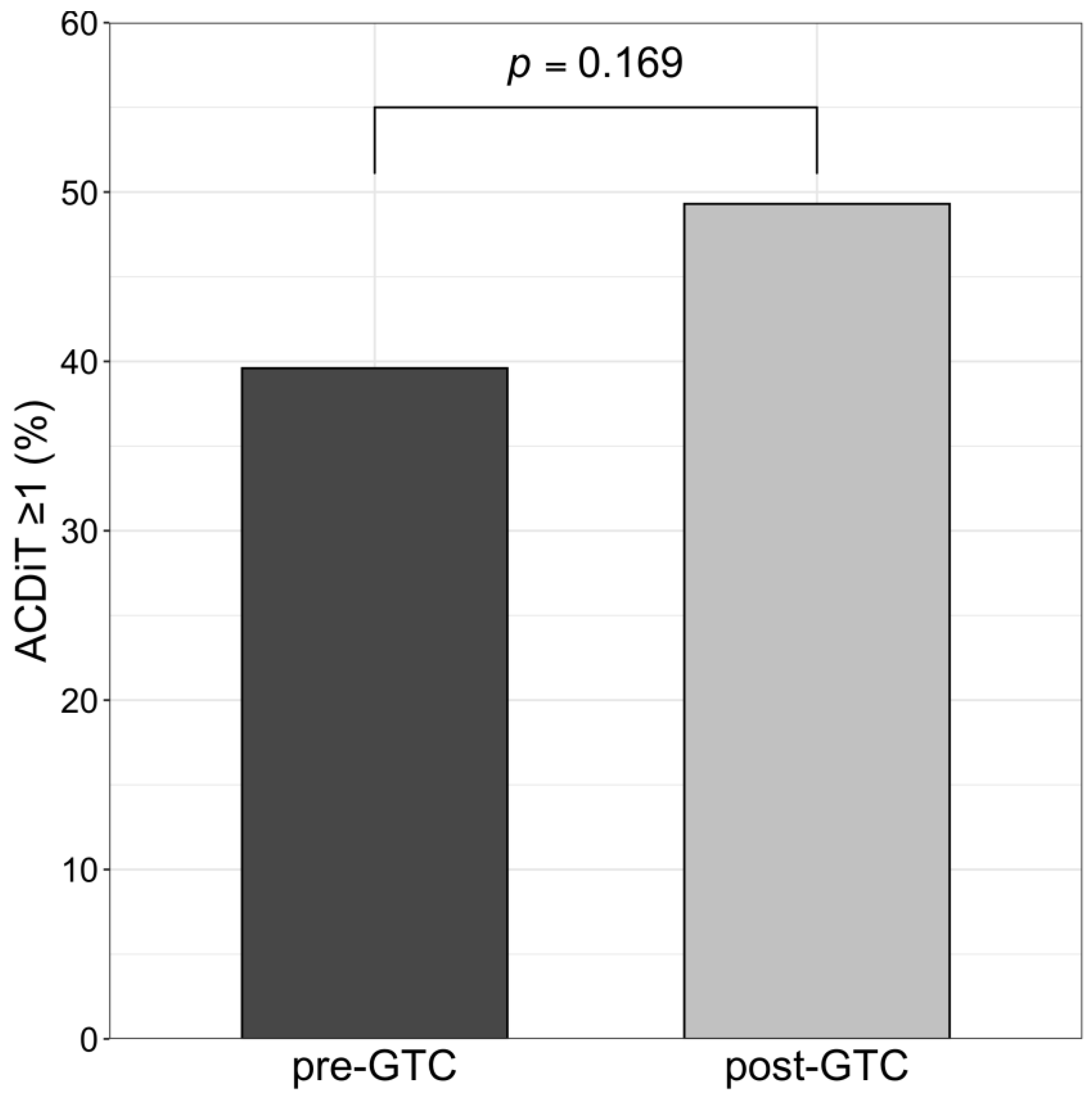
3.4. Adapted Clavien–Dindo Scoring System in Trauma (ACDiT)
4. Discussion
- LOS tended to decrease, and persistent low level of in-hospital mortality was observed in both groups, despite increased medical complexity in the post-GTC group (characterised by significantly increased age and higher use of VKAs and DOACs).
- The detection of UTIs increased, and a tendency toward more delirium diagnoses in the post-GTC group was observed.
- Despite the increased medical complexity of geriatric patients, we observed no difference in the necessity for deviations from initial management plans (grade ≥ 1 ACDiT).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ström, O.; Borgström, F.; Kanis, J.A.; Compston, J.; Cooper, C.; McCloskey, E.V.; Jonsson, B.G. Osteoporosis: Burden, health care provision and opportunities in the EU. Arch. Osteoporos. 2011, 6, 59–155. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef]
- Ensrud, K.E. Epidemiology of Fracture Risk with Advancing Age. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2013, 68, 1236–1242. [Google Scholar] [CrossRef]
- Hadji, P.; Klein, S.; Gothe, H.; Häussler, B.; Kless, T.; Schmidt, T.; Steinle, T.; Verheyen, F.; Linder, R. The Epidemiology of Osteoporosis. Dtsch. Aerzteblatt Online 2013, 110, 52–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberkircher, L.; Ruchholtz, S.; Rommens, P.M.; Hofmann, A.; Bücking, B.; Krüger, A. Osteoporotic Pelvic Fractures. Dtsch. Aerzteblatt Online 2018, 115, 70–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannus, P.; Parkkari, J.; Niemi, S.; Sievänen, H. Low-Trauma Pelvic Fractures in Elderly Finns in 1970–2013. Calcif. Tissue Int. 2015, 97, 577–580. [Google Scholar] [CrossRef]
- Halvachizadeh, S.; Gröbli, L.; Berk, T.; Jensen, K.O.; Hierholzer, C.; Bischoff-Ferrari, H.A.; Pfeifer, R.; Pape, H.-C. The effect of geriatric comanagement (GC) in geriatric trauma patients treated in a level 1 trauma setting: A comparison of data before and after the implementation of a certified geriatric trauma center. PLoS ONE 2021, 16, e0244554. [Google Scholar] [CrossRef] [PubMed]
- Garwe, T.; Stewart, K.E.; Stoner, J.A.; Newgard, C.D.; Scott, M.; Zhang, Y.; Cathey, T.; Sacra, J.; Albrecht, R.M. Out-of-hospital and Inter-hospital Under-triage to Designated Tertiary Trauma Centers among Injured Older Adults: A 10-year Statewide Geospatial-Adjusted Analysis. Prehospital Emerg. Care 2017, 21, 734–743. [Google Scholar] [CrossRef]
- Keller, J.M.; Sciadini, M.F.; Sinclair, E.; O’Toole, R.V. Geriatric Trauma. J. Orthop. Trauma 2012, 26, e161–e165. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.G. Special considerations in geriatric injury. Curr. Opin. Crit. Care 2003, 9, 535–539. [Google Scholar] [CrossRef]
- Rommens, P.M.; Wagner, D.; Hofmann, A. Fragility Fractures of the Pelvis. JBJS Rev. 2017, 5. [Google Scholar] [CrossRef]
- Cotton, B.A.; McCarthy, J.J.; Holcomb, J.B. Acutely Injured Patients on Dabigatran. N. Engl. J. Med. 2011, 365, 2039–2040. [Google Scholar] [CrossRef] [PubMed]
- Bonville, D.J.; Ata, A.; Jahraus, C.B.; Arnold-Lloyd, T.; Salem, L.; Rosati, C.; Stain, S.C. Impact of preinjury warfarin and antiplatelet agents on outcomes of trauma patients. Surgery 2011, 150, 861–868. [Google Scholar] [CrossRef]
- Boyd, R.; Hawthorne, J.; Wallace, W.; Worlock, P.; Compton, E. The Nottingham Orthogeriatric unit after 1000 admissions. Injury 1983, 15, 193–196. [Google Scholar] [CrossRef]
- Mukherjee, K.; Brooks, S.E.; Barraco, R.D.; Como, J.J.; Hwang, F.; Robinson, B.R.H.; Crandall, M.L. Elderly adults with isolated hip fractures- orthogeriatric care versus standard care: A practice management guideline from the Eastern Association for the Surgery of Trauma. J. Trauma Acute Care Surg. 2019, 88, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Rapp, K.; Becker, C.; Todd, C.; Rothenbacher, D.; Schulz, C.; König, H.-H.; Liener, U.; Hartwig, E.; Büchele, G. The Association Between Orthogeriatric Co-Management and Mortality Following Hip Fracture. Dtsch. Aerzteblatt Online 2020, 117, 53–59. [Google Scholar] [CrossRef]
- Körner, M. Interprofessional teamwork in medical rehabilitation: A comparison of multidisciplinary and interdisciplinary team approach. Clin. Rehabil. 2010, 24, 745–755. [Google Scholar] [CrossRef]
- Olotu, C.; Weimann, A.; Bahrs, C.; Schwenk, W.; Scherer, M.; Kiefmann, R. The Perioperative Care of Older Patients. Dtsch. Aerzteblatt Online 2019, 116, 63–69. [Google Scholar] [CrossRef]
- Vuillemin, N.; Pape, H.-C.; Rommens, P.; Lippuner, K.; Siebenrock, K.-A.; Keel, M.; Bastian, J. A Bibliometric Analysis of Fragility Fractures: Top 50. Medicina 2021, 57, 639. [Google Scholar] [CrossRef]
- Maier, G.S.; Kolbow, K.; Lazovic, D.; Horas, K.; Roth, K.E.; Seeger, J.B.; Maus, U. Risk factors for pelvic insufficiency fractures and outcome after conservative therapy. Arch. Gerontol. Geriatr. 2016, 67, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Krause, U.; Jung, K. Geriatric Fracture Centre (German Trauma Society): Guidelines and certification to improve geriatric trauma care. Innov. Surg. Sci. 2016, 1, 79–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knobe, M.; Böttcher, B.; Coburn, M.; Friess, T.; Bollheimer, L.C.; Heppner, H.J.; Werner, C.J.; Bach, J.-P.; Wollgarten, M.; Poßelt, S.; et al. AltersTraumaZentrum DGU®: Evaluation klinischer und ökonomischer Parameter. Unfallchirurg 2018, 122, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Hafner, T.; Kollmeier, A.; Laubach, M.; Knobe, M.; Hildebrand, F.; Pishnamaz, M. Care of Geriatric Patients with Lumbar Spine, Pelvic, and Acetabular Fractures before and after Certification as a Geriatric Trauma Center DGU®: A Retrospective Cohort Study. Medicina 2021, 57, 794. [Google Scholar] [CrossRef]
- Bücking, B.; Neuerburg, C.; Knobe, M.; Liener, U.; Bücking, B.; Neuerburg, C.; Knobe, M.; Liener, U. Versorgung von Patienten mit Fragilitätsfrakturen. Unfallchirurg 2019, 122, 755–761. [Google Scholar] [CrossRef]
- Sieber, C.C. Der ältere Patient—Wer ist das? Internist 2007, 48, 1190–1194. [Google Scholar] [CrossRef]
- Safford, M.M.; Allison, J.J.; Kiefe, C.I. Patient Complexity: More Than Comorbidity. The Vector Model of Complexity. J. Gen. Intern. Med. 2007, 22, 382–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCusker, J.; Bellavance, F.; Cardin, S.; Trepanier, S.; Verdon, J.; Ardman, O. Detection of Older People at Increased Risk of Adverse Health Outcomes After an Emergency Visit: The ISAR Screening Tool. J. Am. Geriatr. Soc. 1999, 47, 1229–1237. [Google Scholar] [CrossRef]
- Scharf, A.-C.; Gronewold, J.; Dahlmann, C.; Schlitzer, J.; Kribben, A.; Gerken, G.; Rassaf, T.; Kleinschnitz, C.; Dodel, R.; Frohnhofen, H.; et al. Health outcome of older hospitalized patients in internal medicine environments evaluated by Identification of Seniors at Risk (ISAR) screening and geriatric assessment. BMC Geriatr. 2019, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Wolters, U.; Wolf, T.; Stützer, H.; Schröder, T. ASA classification and perioperative variables as predictors of postoperative outcome. Br. J. Anaesth. 1996, 77, 217–222. [Google Scholar] [CrossRef]
- Irlbeck, T.; Zwißler, B.; Bauer, A. ASA-Klassifikation. Anaesthesist 2016, 66, 5–10. [Google Scholar] [CrossRef]
- Tran, A.; Mai, T.; El-Haddad, J.; Lampron, J.; Yelle, J.-D.; Pagliarello, G.; Matar, M. Preinjury ASA score as an independent predictor of readmission after major traumatic injury. Trauma Surg. Acute Care Open 2017, 2, e000128. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, R.; Baker, G.; Macdonald, J.; Thompson, N.W. Co-morbidities in Patients with a Hip Fracture. Ulster Med J. 2019, 88, 162–166. [Google Scholar] [PubMed]
- Geissler, A.; Scheller-Kreinsen, D.; Quentin, W.; Busse, R. Germany: Understanding G-DRGs. Diagnosis-Related Groups in Europe: Moving Towards Transparency, Efficiency and Quality in Hospitals; Open University Press: Maidenhead, UK, 2011; pp. 243–272. [Google Scholar]
- Naumann, D.N.; Vincent, L.E.; Pearson, N.; Beaven, A.; Smith, I.M.; Smith, K.; Toman, E.; Dorrance, H.R.; Porter, K.; Wade, C.E.; et al. An adapted Clavien-Dindo scoring system in trauma as a clinically meaningful nonmortality endpoint. J. Trauma Acute Care Surg. 2017, 83, 241–248. [Google Scholar] [CrossRef] [PubMed]
- World Health, O. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Atinga, A.; Shekkeris, A.; Fertleman, M.; Batrick, N.; Kashef, E.; Dick, E. Trauma in the elderly patient. Br. J. Radiol. 2018, 91, 20170739. [Google Scholar] [CrossRef]
- Mangram, A.J.; Mitchell, C.D.; Shifflette, V.K.; Lorenzo, M.; Truitt, M.S.; Goel, A.; Lyons, M.A.; Nichols, D.J.; Dunn, E.L. Geriatric trauma service. J. Trauma: Inj. Infect. Crit. Care 2012, 72, 119–122. [Google Scholar] [CrossRef]
- Blauth, M.; Joeris, A.; Rometsch, E.; Espinoza-Rebmann, K.; Wattanapanom, P.; Jarayabhand, R.; Poeze, M.; Wong, M.K.; Kwek, E.B.K.; Hegeman, J.H.; et al. Geriatric fracture centre vs usual care after proximal femur fracture in older patients: What are the benefits? Results of a large international prospective multicentre study. BMJ Open 2021, 11, e039960. [Google Scholar] [CrossRef]
- Grund, S.; Roos, M.; Duchene, W.; Schuler, M. Treatment in a Center for Geriatric Traumatology. Dtsch. Aerzteblatt Online 2015, 112, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Pablos-Hernández, C.; González-Ramírez, A.; Ms, C.D.C.; Luis, M.M.; García-Iglesias, M.A.; Julián-Enriquez, J.M.; Rodríguez-Sánchez, E.; Blanco, J.F. Time to Surgery Reduction in Hip Fracture Patients on an Integrated Orthogeriatric Unit: A Comparative Study of Three Healthcare Models. Orthop. Surg. 2020, 12, 457–462. [Google Scholar] [CrossRef] [Green Version]
- Dakhil, S.; Thingstad, P.; Frihagen, F.; Johnsen, L.G.; Lydersen, S.; Skovlund, E.; Wyller, T.B.; Sletvold, O.; Saltvedt, I.; Watne, L.O. Orthogeriatrics prevents functional decline in hip fracture patients: Report from two randomized controlled trials. BMC Geriatr. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Della Rocca, G.J.; Moylan, K.C.; Crist, B.D.; Volgas, D.A.; Stannard, J.P.; Mehr, D.R. Comanagement of Geriatric Patients With Hip Fractures. Geriatr. Orthop. Surg. Rehabil. 2013, 4, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Halvachizadeh, S.; Baradaran, L.; Cinelli, P.; Pfeifer, R.; Sprengel, K.; Pape, H.-C. How to detect a polytrauma patient at risk of complications: A validation and database analysis of four published scales. PLoS ONE 2020, 15, e0228082. [Google Scholar] [CrossRef]
- Pawelec, G. Immunity and ageing in man. Exp. Gerontol. 2006, 41, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Alpay, Y.; Aykın, N.; Korkmaz, P.; Güldüren, H.M.; Çağlan, F. Urinary tract infections in the geriatric patients. Pak. J. Med. Sci. 2018, 34, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Olufajo, O.A.; Tulebaev, S.; Javedan, H.; Gates, J.; Wang, J.; Duarte, M.; Kelly, E.; Lilley, E.; Salim, A.; Cooper, Z. Integrating Geriatric Consults into Routine Care of Older Trauma Patients: One-Year Experience of a Level I Trauma Center. J. Am. Coll. Surg. 2016, 222, 1029–1035. [Google Scholar] [CrossRef]
- Gillis, A.J.; MacDonald, B. Unmasking delirium. Can. Nurse 2006, 102, 18–24. [Google Scholar]
- Goldberg, T.E.; Chen, C.; Wang, Y.; Jung, E.; Swanson, A.; Ing, C.; Garcia, P.S.; Whittington, R.A.; Moitra, V. Association of Delirium With Long-term Cognitive Decline. JAMA Neurol. 2020, 77, 1373–1381. [Google Scholar] [CrossRef]
- Thein, M.Z.A.; Pereira, J.; Nitchingham, A.; Caplan, G.A. A call to action for delirium research: Meta-analysis and regression of delirium associated mortality. BMC Geriatr. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Folbert, E.C.E.; Smit, R.S.; van der Velde, D.; Regtuijt, E.M.M.; Klaren, M.H.; Hegeman, J.H.H. Geriatric Fracture Center. Geriatr. Orthop. Surg. Rehabil. 2012, 3, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Kusen, J.Q.; Schafroth, B.; Poblete, B.; Van Der Vet, P.C.R.; Link, B.C.; Wijdicks, F.J.G.; Babst, R.; Beeres, F.J.P. The implementation of a Geriatric Fracture Centre for hip fractures to reduce mortality and morbidity: An observational study. Arch. Orthop. Trauma Surg. 2019, 139, 1705–1712. [Google Scholar] [CrossRef]
- Lundstrãm, M.; Edlund, A.; Karlsson, S.; Brã¤Nnstrãm, B.; Bucht, G.; Gustafson, Y. A Multifactorial Intervention Program Reduces the Duration of Delirium, Length of Hospitalization, and Mortality in Delirious Patients. J. Am. Geriatr. Soc. 2005, 53, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Van Der Vlegel, M.; Haagsma, J.A.; Geraerds, A.J.L.M.; De Munter, L.; De Jongh, M.A.C.; Polinder, S. Health care costs of injury in the older population: A prospective multicentre cohort study in the Netherlands. BMC Geriatr. 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, M.; Bottle, A.; Long, S.; Aylin, P. Multi-Morbidity in Hospitalised Older Patients: Who Are the Complex Elderly? PLoS ONE 2015, 10, e0145372. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Pre-GTC (n = 111) | Post-GTC (n = 108) | p Value | |
|---|---|---|---|
| Age (years), median (IQR) | 80.0 (76.0–84.0) | 82.0 (77.3–86.8) | 0.016 b |
| Sex (female), n (%) | 86 (77.5) | 74 (68.5) | 0.135 |
| BMI (kg/m2), mean (SD) † | 25.8 (4.5) | 24.6 (4.2) | 0.078 b |
| ISAR score (IQR) | 3.0 (1.0–4.0) ‡‡ | ||
| ASA class, n (%) | |||
| ASA 1 and ASA 2 | 32 (28.8) | 26 (24.1) | 0.475 |
| ASA 3 and higher | 79 (71.2) | 82 (75.9) | |
| Anticoagulant medication, n (%) †† | |||
| None | 44 (39.6) | 46 (42.6) | 0.007 |
| VKAs or DOACs | 12 (10.8) | 23 (21.3) | |
| APDs | 36 (32.4) | 18 (16.7) | |
| Heparin and heparinoids | 16 (14.4) | 7 (6.5) | |
| Dementia, n (%) ‡ | 24 (21.6) | 17 (15.7) | 0.279 |
| Age-adjusted Charlson Comorbidity Index, median (IQR) ‡ | 5.0 (5.0–6.0) | 6.0 (5.0–7.0) | 0.261 c |
| Pre-GTC (n = 111) | Post-GTC (n = 108) | p Value | |
|---|---|---|---|
| Fracture site | |||
| Thoracic spine, n (%) | 42 (37.8) | 25 (23.1) | 0.026 |
| Lumbar spine, n (%) | 44 (39.6) | 44 (40.7) | |
| Pelvic ring, n (%) | 25 (22.5) | 39 (36.1) | |
| Non-surgical treatment, n (%) | 47 (42.3) | 56 (51.9) | 0.159 |
| LOS (days), median (IQR) | 9.0 (6.0–13.0) | 7.0 (5.0–11.8) | 0.076 b |
| Mortality, n (%) | 1 (0.9) | 4 (3.7) | 0.208 c |
| Pre-GTC (n = 111) | Post-GTC (n = 108) | p Value | |
|---|---|---|---|
| Delirium, n (%) | 7 (6.3) | 14 (13.0) | 0.094 |
| Cardiological, n (%) | 13 (11.7) | 9 (8.3) | 0.406 |
| Pulmonary, n (%) | 17 (15.3) | 19 (17.6) | 0.649 |
| Gastrointestinal, n (%) | 9 (8.1) | 4 (3.7) | 0.168 |
| Urinary tract infection, n (%) | 18 (16.2) | 38 (35.2) | 0.001 |
| Anaemia, n (%) | 20 (18.0) | 14 (13.0) | 0.302 |
| Electrolyte disorder, n (%) | 37 (33.3) | 27 (25.0) | 0.175 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laubach, M.; Gruchow, L.C.; Hafner, T.; Migliorini, F.; Knobe, M.; Hildebrand, F.; Pishnamaz, M. In-Hospital Clinical Outcomes in Patients with Fragility Fractures of the Lumbar Spine, Thoracic Spine, and Pelvic Ring: A Comparison of Data before and after Certification as a DGU® Geriatric Trauma Centre. Medicina 2021, 57, 1197. https://doi.org/10.3390/medicina57111197
Laubach M, Gruchow LC, Hafner T, Migliorini F, Knobe M, Hildebrand F, Pishnamaz M. In-Hospital Clinical Outcomes in Patients with Fragility Fractures of the Lumbar Spine, Thoracic Spine, and Pelvic Ring: A Comparison of Data before and after Certification as a DGU® Geriatric Trauma Centre. Medicina. 2021; 57(11):1197. https://doi.org/10.3390/medicina57111197
Chicago/Turabian StyleLaubach, Markus, Laura Christine Gruchow, Tobias Hafner, Filippo Migliorini, Matthias Knobe, Frank Hildebrand, and Miguel Pishnamaz. 2021. "In-Hospital Clinical Outcomes in Patients with Fragility Fractures of the Lumbar Spine, Thoracic Spine, and Pelvic Ring: A Comparison of Data before and after Certification as a DGU® Geriatric Trauma Centre" Medicina 57, no. 11: 1197. https://doi.org/10.3390/medicina57111197