
Non-Respiratory Symptoms of Patients Infected with SARS-CoV-2 (Coronavirus Disease 2019): Lessons from Their Initial Presentation at the Hospital

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Laboratory Confirmation of SARS-CoV-2 Infection
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdullahi, A.; Candan, S.A.; Abba, M.A.; Bello, A.H.; AlShehri, M.A.; Victor, E.A.; Umar, N.A.; Kundakci, B. Neurological and musculoskeletal features of COVID-19: A systematic review and meta-analysis. Front. Neurol. 2020, 11, 687. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total. Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Cipollaro, L.; Giordano, L.; Padulo, J.; Oliva, F.; Maffulli, N. Musculoskeletal symptoms in SARS-CoV-2 (COVID-10) patients. J. Orthop. Surg. Res. 2020, 15, 178. [Google Scholar] [CrossRef] [PubMed]
- Disser, N.P.; De Micheli, A.J.; Schonk, M.M.; Konnaris, M.A.; Piacentini, A.N.; Edon, D.L.; Toresdahl, B.G.; Rodeo, S.A.; Casey, E.K.; Mendias, C.L. Musculoskeletal consequences of COVID-19. J. Bone Joint. Surg. Am. 2020, 102, 1197–1204. [Google Scholar] [CrossRef]
- Xu, X.-W.; Wu, X.-X.; Jiang, X.-G.; Xu, K.-J.; Ying, L.-J.; Ma, C.-L.; Li, S.-B.; Wang, H.-Y.; Zhang, S.; Gao, H.-N.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-CoV-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, m606. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Yang, B.; Li, Q.; Wen, L.; Zhang, R. Clinical features of 69 cases with coronavirus disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 769–777. [Google Scholar] [CrossRef] [Green Version]
- Song, X.; Delaney, M.; Shah, R.K.; Campos, J.M.; Wessel, D.L.; DeBiasi, R.L. Comparison of clinical features of COVID-19 vs seasonal influenza A and B in US children. JAMA Netw. Open 2020, 3, e2020495. [Google Scholar] [CrossRef]
- Contini, C.; Caselli, E.; Martini, F.; Maritati, M.; Torreggiani, E.; Seraceni, S.; Vesce, F.; Perri, P.; Rizzo, L.; Tognon, M. COVID-19 is a multifaceted challenging pandemic which needs urgent public health interventions. Microorganisms 2020, 8, 1228. [Google Scholar] [CrossRef]
- Shen, C.; Tan, M.; Song, X.; Zhang, G.; Liang, J.; Yu, H.; Wang, C. Comparative analysis of early-stage clinical features between COVID-19 and influenza A H1N1 virus pneumonia. Front. Public Health. 2020, 8, 206. [Google Scholar] [CrossRef]
- Zayet, S.; Lepiller, Q.; Zahra, H.; Royer, P.Y.; Toko, L.; Gendrin, V.; Klopfenstein, T. Clinical features of COVID-19 and influenza: A comparative study on Nord Fracnce-Comte cluster. Microbes Infect. 2020, 22, 481–488. [Google Scholar] [CrossRef]
- Jin, X.; Lian, J.S.; Hu, J.H.; Gao, J.; Zheng, L.; Zhang, Y.M.; Hao, S.R.; Jia, H.Y.; Cai, H.; Zhang, X.L.; et al. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Casey, P.; Ang, Y.; Sultan, J. COVID-19-induced sarcopenia and physical deconditioning may require reassessment of surgical risk for patients with cancer. World J. Surg. Oncol. 2021, 19, 8. [Google Scholar] [CrossRef]
- Du, Y.; Tu, L.; Zhu, P.; Mu, M.; Wang, R.; Yang, P.; Wang, X.; Hu, C.; Ping, R.; Hu, P.; et al. Clinical features of 85 fatal cases of COVID-19 from Wuhan, A retrospective observational study. Am. J. Respirat. Crit. Care Med. 2020, 201, 1372–1379. [Google Scholar] [CrossRef] [Green Version]
- Kucuk, A.; Cure, M.C.; Cure, E. Can COVID-19 cause myalgia with a completely different mechanism? A hypothesis. Clin. Rheumatol. 2020, 39, 2103–2104. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Joob, B.; Wiwanitkit, V. Arthralgia as an initial presentation of COVID-19: Observation. Rheumatol. Int. 2020, 40, 823. [Google Scholar] [CrossRef] [Green Version]
- Ciaffi, J.; Meliconi, R.; Ruscitti, P.; Berardicurti, O.; Giacomelli, R.; Ursini, F. Rheumatic manifestations of COVID-19: A systematic review and meta-analysis. BMC Rheumatol. 2020, 4, 65. [Google Scholar] [CrossRef]
- Redd, W.D.; Zhou, J.C.; Hathorn, K.E.; Mccarty, T.R.; Bazarbashi, A.N.; Thompson, C.C.; Shen, L.; Chan, W.W. Prevalence and characteristics of gastrointestinal symptoms in patients with severe acute respiratory syndrome coronavirus 2 infection in the United States: A multicenter cohort study. Gastroenterology 2020, 159, 765–767. [Google Scholar] [CrossRef]
- Zhou, Y.; Han, T.; Chen, J.; Hou, C.; Hua, L.; He, S.; Guo, Y.; Zhang, S.; Wang, Y.; Yuan, J.; et al. Clinical and autoimmune characteristics of severe and critical cases of COVID-19. Clin. Transl. Sci. 2020, 13, 1077–1086. [Google Scholar] [CrossRef]
- Chen, T.; Dai, Z.; Mo, P.; Li, X.; Ma, Z.; Song, S.; Chen, X.; Luo, M.; Liang, K.; Gao, S.; et al. Clinical characteristics and outcomes of older patients with coronavirus disease 2019 (COVID-19) in Wuhan, China: A single-centered, retrospective study. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1788–1795. [Google Scholar] [CrossRef]
- Mo, P.; Xing, Y.; Xiao, Y.; Deng, L.; Zhao, Q.; Wang, H.; Xiong, Y.; Cheng, Z.; Gao, S.; Liang, K.; et al. Clinical characteristics of refractory COVID-19 pneumonia in Wuhan, China. Clin. Infect. Dis. 2020, 270, ciaa270. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All (n = 79) | Male (n = 47) | Female (n = 32) | p-Value | |
|---|---|---|---|---|
| Age | 44.08 ± 17.53 | 42.21 ± 16.76 | 46.81 ± 18.52 | 0.353 |
| Smoking status | 0.497 | |||
| None | 29 (36.7) | 17 (36.2) | 12 (37.5) | |
| Active | 48 (60.8) | 28 (59.6) | 20 (62.5) | |
| Former | 2 (2.5) | 2 (4.2) | ||
| Exposure history | 0.501 | |||
| Family cluster | 16 (20.3) | 9 (19.1) | 7 (21.9) | |
| Work related | 20 (25.3) | 10 (21.3) | 10 (31.2) | |
| Other | 43 (54.4) | 28 (59.6) | 15 (46.9) | |
| Co-morbidities | ||||
| All | 30 (38) | 17 (36.2) | 13 (40.6) | 0.653 |
| Hypertension | 22 (27.8) | 13 (27.7) | 9 (28.1) | 0.964 |
| Cardiovascular disease | 10 (12.7) | 4 (8.5) | 6 (18.8) | 0.179 |
| Diabetes Mellitus | 5 (6.3) | 4 (8.5) | 1 (3.1) | 0.334 |
| Hypothyroidism | 5 (6.3) | 3 (6.4) | 2 (6.2) | 0.981 |
| Dislipidemia | 7 (8.9) | 4 (8.5) | 3 (9.3) | 0.894 |
| Asthma | 3 (3.8) | 1 (2.1) | 2 (6.2) | 0.406 |
| Depression | 5 (6.3) | 3 (6.4) | 2 (6.2) | 0.981 |
| GERD | 4 (5.1) | 2 (4.3) | 2 (6.2) | 0.691 |
| Orthopaedic procedures | 8 (10.1) | 6 (12.8) | 2 (6.2) | 0.346 |
| Orthopaedic history | 20 (25.3) | 10 (21.3) | 10 (31.3) | 0.317 |
| Hospitalization | 23 (29.1) | 14 (29.8) | 9 (28.1) | 0.873 |
| Days of hospitalization | 13.26 ± 7.89 | 11.64 ± 7.49 | 15.78 ± 8.27 | 0.336 |
| All (n = 79) | Male (n = 47) | Female (n = 32) | p-Value | |
|---|---|---|---|---|
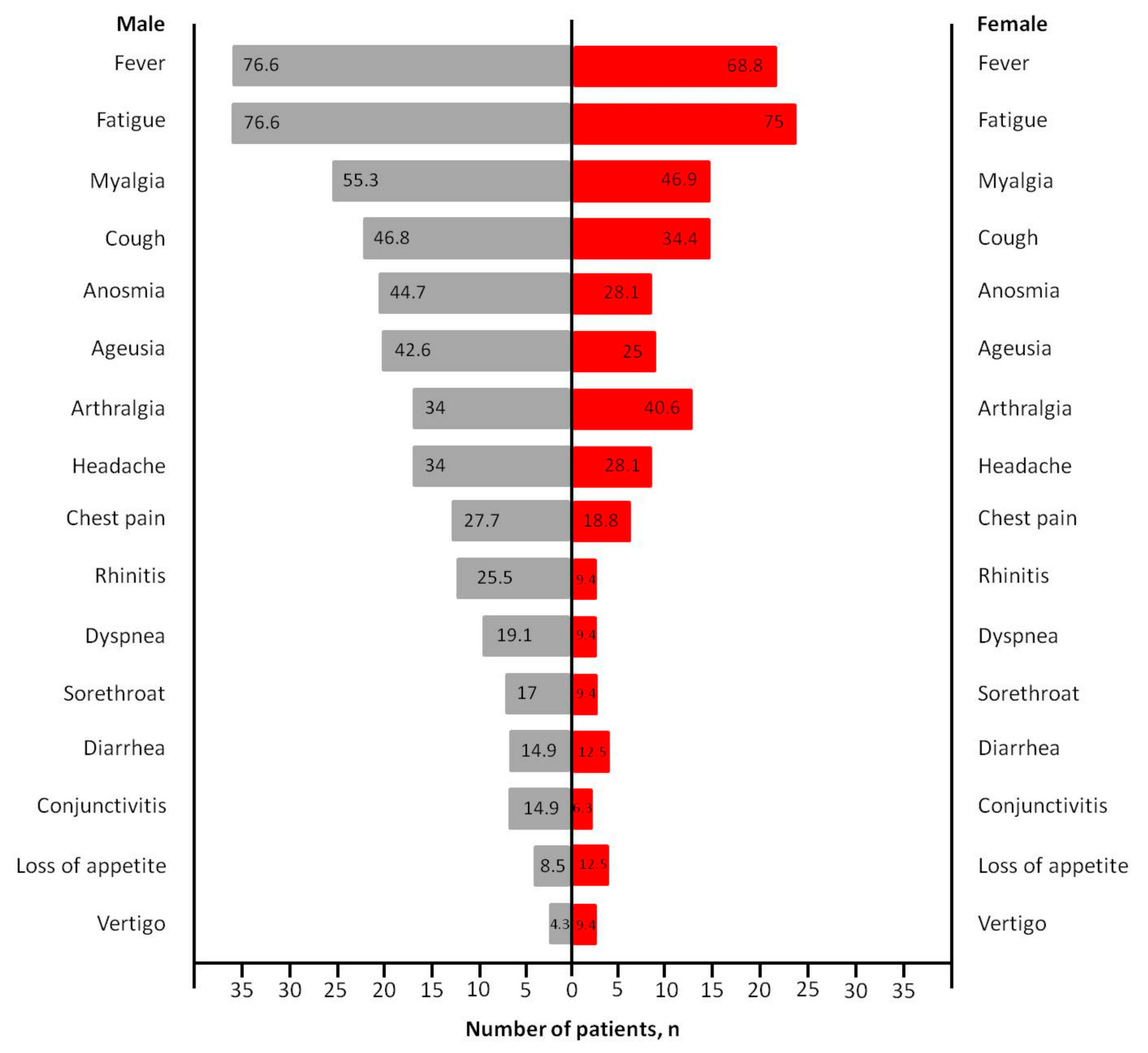
| Symptoms | ||||
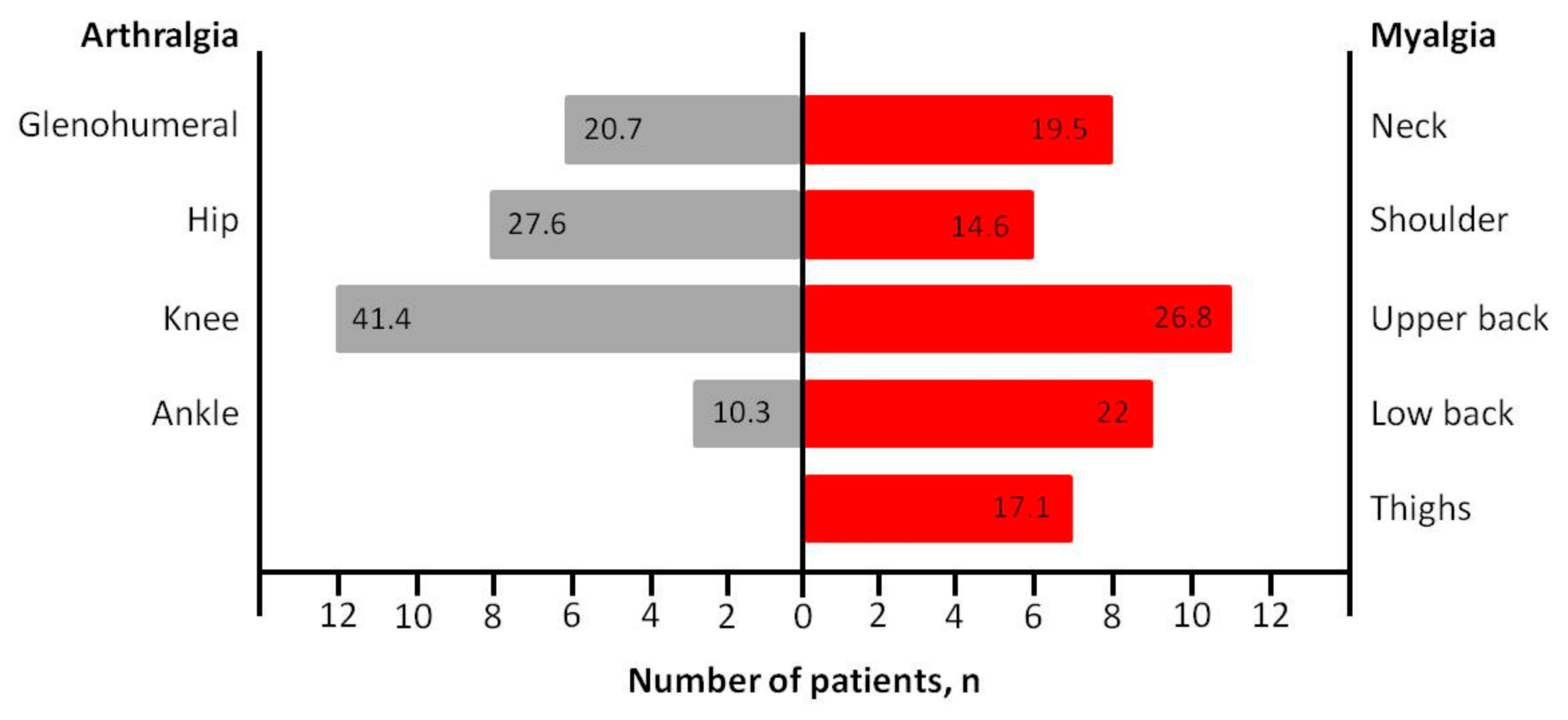
| Arthralgia | 29 (36.7) | 16 (34) | 13 (40.6) | 0.551 |
| Myalgia | 41 (51.9) | 26 (55.3) | 15 (46.9) | 0.461 |
| Fatigue | 60 (75.9) | 36 (76.6) | 24 (75) | 0.871 |
| Fever | 58 (73.4) | 36 (76.6) | 22 (68.8) | 0.438 |
| Chest pain | 19 (24.1) | 13 (27.7) | 6 (18.8) | 0.363 |
| Cough | 33 (41.8) | 22 (46.8) | 11 (34.4) | 0.271 |
| Anosmia | 30 (38) | 21 (44.7) | 9 (28.1) | 0.137 |
| Ageusia | 28 (35.4) | 20 (42.6) | 8 (25) | 0.109 |
| Headache | 25 (31.6) | 16 (34) | 9 (28.1) | 0.579 |
| Blood tests | ||||
| WBC | 6711.8 ± 2983.5 | 7228.5 ± 3399.4 | 6096.7 ± 2330 | 0.326 |
| Hb | 13.9 ± 1.5 | 14.3 ± 1.2 | 13.3 ± 1.6 | 0.031 |
| Hct | 40.9 ± 5.2 | 42.1 ± 5.8 | 39.5 ± 4 | 0.006 |
| INR | 1.08 ± 0.09 | 1.07 ± 0.07 | 1.08 ± 0.12 | 0.982 |
| CRP | 6.2 ± 4.3 | 6.7 ± 4.02 | 5.6 ± 4.6 | 0.155 |
| Procalcitonin | 0.22 ± 0.27 | 0.22 ± 0.31 | 0.22 ± 0.23 | 0.755 |
| D-Dimers | 922.9 ± 776.4 | 940 ± 649.2 | 902.5 ± 921.8 | 0.480 |
| Radiologic imaging (X-ray) | ||||
| Normal | 59 (74.7) | 32 (68.1) | 27 (84.4) | 0.239 |
| Unilateral pneumonia | 15 (19) | 12 (25.5) | 3 (9.4) | |
| Bilateral pneumonia | 5 (6.3) | 3 (6.4) | 2 (6.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasiliadis, A.V.; Tsatlidou, M.; Metaxiotis, D.; Psomiadis, C.; Beletsiotis, A.; Arvaniti, K. Non-Respiratory Symptoms of Patients Infected with SARS-CoV-2 (Coronavirus Disease 2019): Lessons from Their Initial Presentation at the Hospital. Medicina 2021, 57, 344. https://doi.org/10.3390/medicina57040344
Vasiliadis AV, Tsatlidou M, Metaxiotis D, Psomiadis C, Beletsiotis A, Arvaniti K. Non-Respiratory Symptoms of Patients Infected with SARS-CoV-2 (Coronavirus Disease 2019): Lessons from Their Initial Presentation at the Hospital. Medicina. 2021; 57(4):344. https://doi.org/10.3390/medicina57040344
Chicago/Turabian StyleVasiliadis, Angelo V., Maria Tsatlidou, Dimitrios Metaxiotis, Charalampos Psomiadis, Anastasios Beletsiotis, and Kostoula Arvaniti. 2021. "Non-Respiratory Symptoms of Patients Infected with SARS-CoV-2 (Coronavirus Disease 2019): Lessons from Their Initial Presentation at the Hospital" Medicina 57, no. 4: 344. https://doi.org/10.3390/medicina57040344