Positron Emission Tomography in the Diagnosis and Management of Coronary Artery Disease

Abstract
:1. Introduction
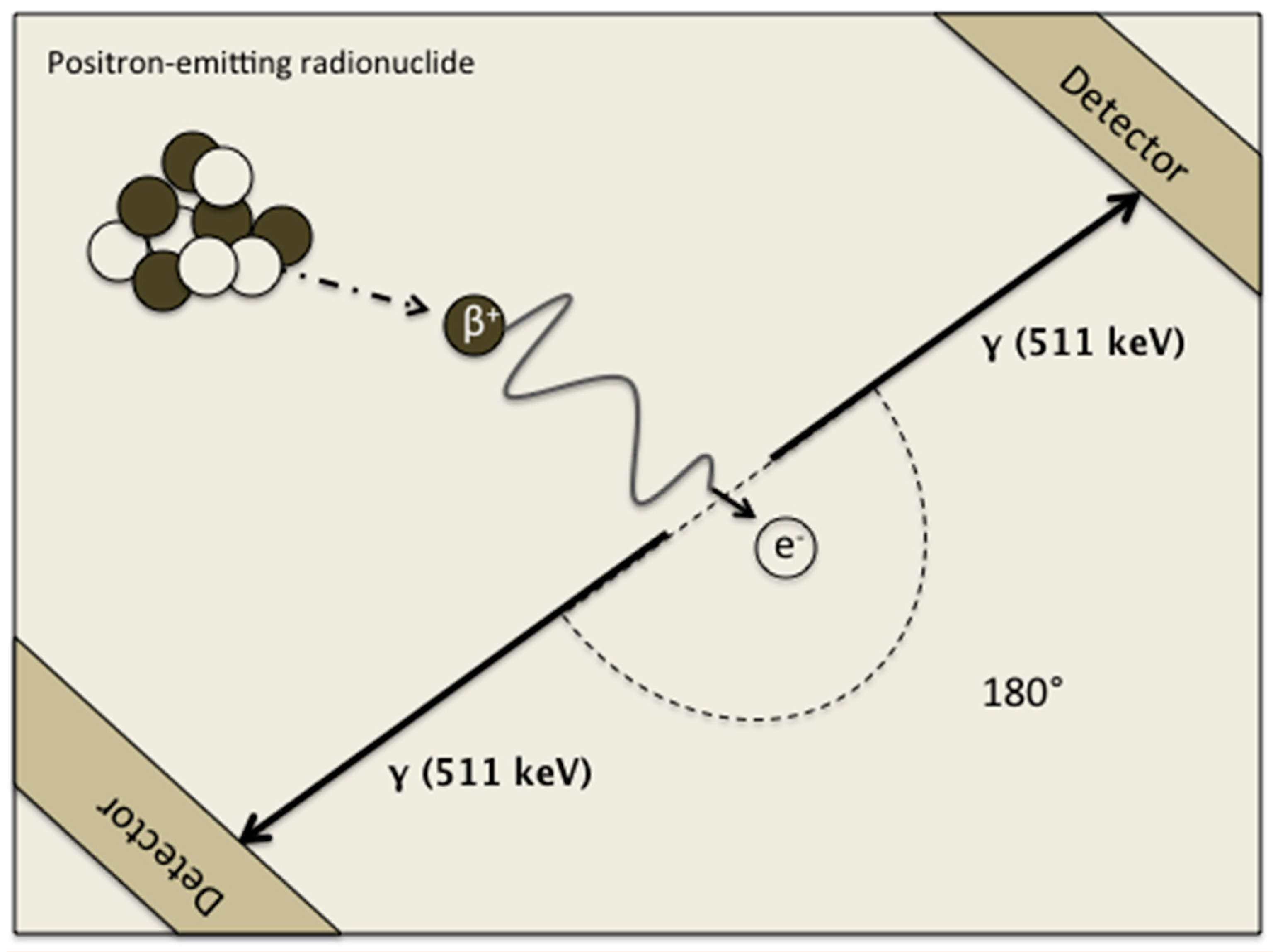
2. Positron Annihilation
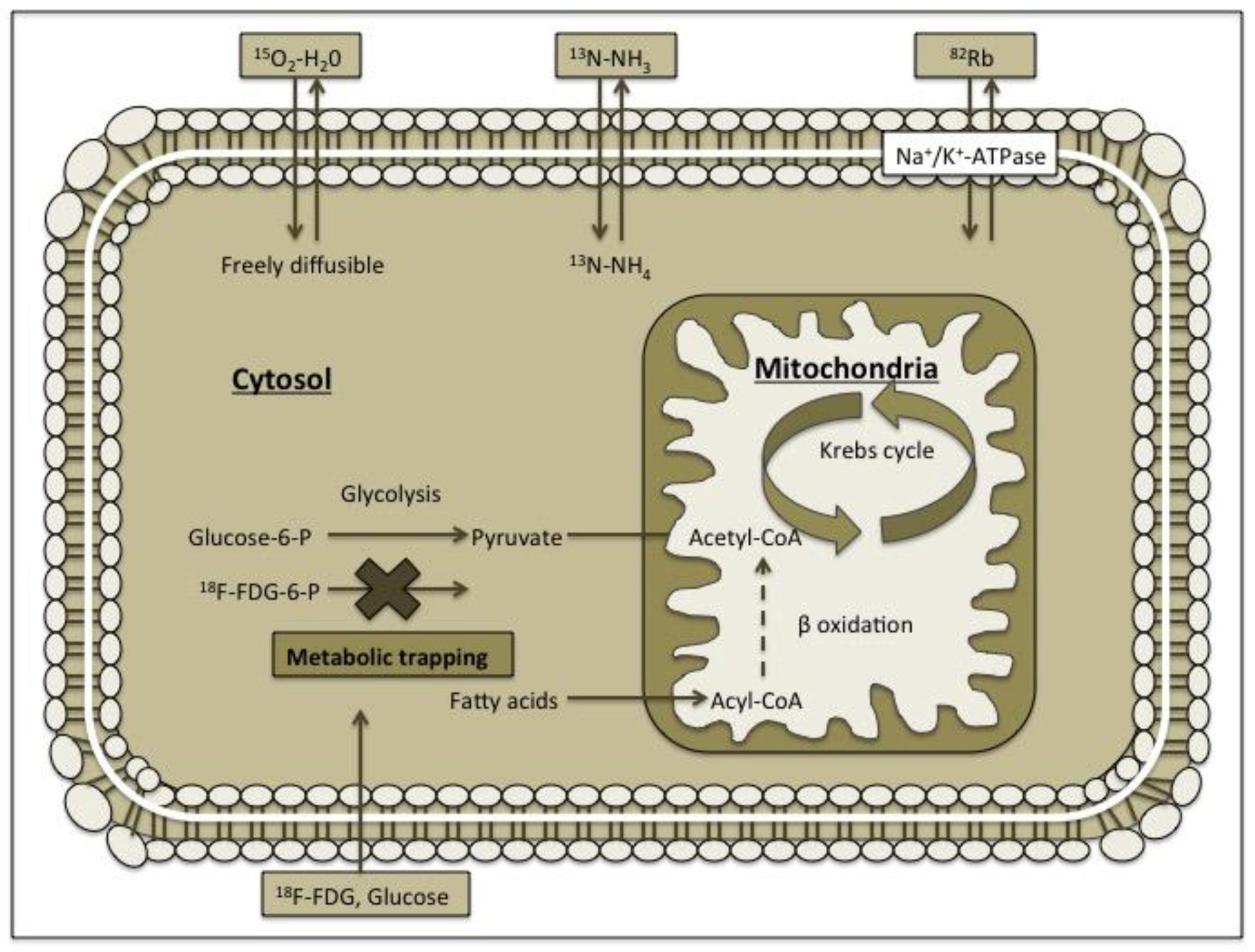
3. Radiopharmaceuticals
4. Assessment of Myocardial Viability with Positron Emission Tomography (PET)
5. PET Perfusion Imaging and Myocardial Blood Flow
- Identification of subclinical CAD. SPECT myocardial perfusion imaging is a traditional evaluation of symptomatic patients with known or suspected CAD [71,72,73]. However, the early stages with the functional microvascular dysfunction remain undetected with SPECT but can be identified by PET by quantifying hyperaemic MBF or MBF in absolute terms [1,69,74,75,76].
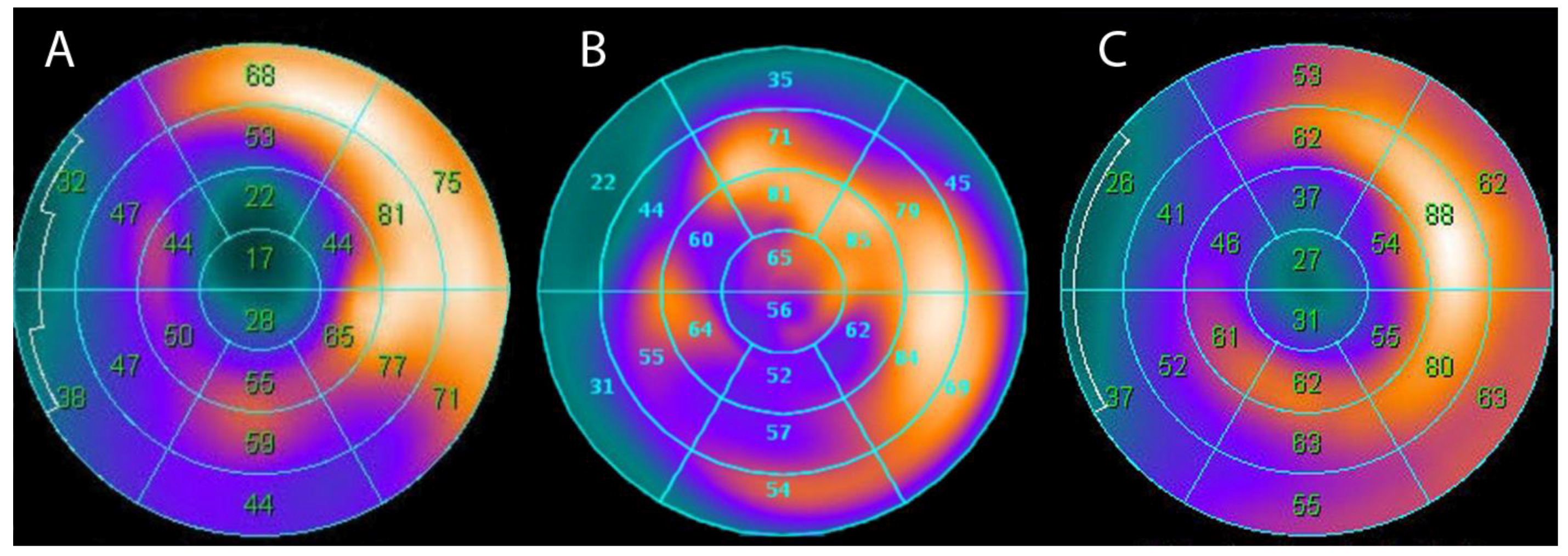
- Enhanced characterization of CAD burden and identification of “balanced” decrease of MBF in all vascular territories. Patients with multivessel CAD may show normal SPECT results due to an absolute decrease of radiotracer uptake in the left ventricle (LV) myocardium. Previous studies have disclosed that SPECT perfusion imaging can detect approximately only 10% of patients with severe three-vessel CAD or significant left main coronary artery (LMA) stenosis (≥50%) [77,78]. If the gated SPECT images are applied, the identification of these patients can be improved to 25% [79]. In diffuse atherosclerosis, PET can identify the hemodynamically significant culprit single lesion along with the true extent of ischemia in a multivessel territory [80,81].
6. Integration or Fusion of Different Imaging Modalities
7. Conclusions
Conflicts of Interest
References
- Schindler, T.H.; Facta, A.D.; Prior, J.O.; Cadenas, J.; Zhang, X.L.; Li, Y.; Sayre, J.; Goldin, J.; Schelbert, H.R. Structural alterations of the coronary arterial wall are associated with myocardial flow heterogeneity in type 2 diabetes mellitus. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Vedanthan, R.; Fuster, V. Disease Prevention: The moving target of global cardiovascular health. Nat. Rev. Cardiol. 2009, 6, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Ter-Pogossian, M.M.; Phelps, M.E.; Hoffman, E.J.; Mullani, N.A. A positron-emission transaxial tomograph for nuclear imaging (PETT). Radiology 1975, 114, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Gaemperli, O.; Kaufmann, P.A. PET and PET/CT in cardiovascular disease. Ann. N. Y. Acad. Sci. 2011, 1228, 109–136. [Google Scholar] [CrossRef]
- Townsend, D.W. Positron emission tomography/computed tomography. Semin. Nucl. Med. 2008, 38, 152–166. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.; Nekolla, S.G.; Bengel, F.M.; Momose, M.; Sammer, A.; Haas, F.; Schnackenburg, B.; Delius, W.; Mudra, H.; Wolfram, D.; et al. Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: Comparison with positron emission tomography. Circulation 2002, 105, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Schwitter, J.; DeMarco, T.; Kneifel, S.; von Schulthess, G.K.; Jorg, M.C.; Arheden, H.; Ruhm, S.; Stumpe, K.; Buck, A.; Parmley, W.W.; et al. Magnetic resonance-based assessment of global coronary flow and flow reserve and its relation to left ventricular functional parameters: A comparison with positron emission tomography. Circulation 2000, 101, 2696–2702. [Google Scholar] [CrossRef] [PubMed]
- Vogel, R.; Indermuhle, A.; Reinhardt, J.; Meier, P.; Siegrist, P.T.; Namdar, M.; Kaufmann, P.A.; Seiler, C. The quantification of absolute myocardial perfusion in humans by contrast echocardiography: Algorithm and validation. J. Am. Coll. Cardiol. 2005, 45, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Di Carli, M.F.; Lipton, M.J. Cardiac PET and PET/CT Imaging; Springer: Berlin, Germany, 2007; pp. 19–33. [Google Scholar]
- Tillisch, J.; Brunken, R.; Marshall, R.; Schwaiger, M.; Mandelkern, M.; Phelps, M.; Schelbert, H. Reversibility of cardiac wall-motion abnormalities predicted by positron tomography. N. Engl. J. Med. 1986, 314, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Schinkel, A.F.; Bax, J.J.; Poldermans, D.; Elhendy, A.; Ferrari, R.; Rahimtoola, S.H. Hibernating myocardium: Diagnosis and patient outcomes. Curr. Probl. Cardiol. 2007, 32, 375–410. [Google Scholar] [CrossRef] [PubMed]
- Beanlands, R.S.; Nichol, G.; Huszti, E.; Humen, D.; Racine, N.; Freeman, M.; Gulenchyn, K.Y.; Garrard, L.; deKemp, R.; Guo, A.; et al. F-18-fluorodeoxyglucose positron emission tomography imaging-assisted management of patients with severe left ventricular dysfunction and suspected coronary disease: A randomized, controlled trial (PARR-2). J. Am. Coll. Cardiol. 2007, 50, 2002–2012. [Google Scholar] [CrossRef] [PubMed]
- Camici, P.; Ferrannini, E.; Opie, L.H. Myocardial metabolism in ischemic heart disease: Basic principles and application to imaging by positron emission tomography. Prog. Cardiovasc. Dis. 1989, 32, 217–238. [Google Scholar] [CrossRef]
- Wijns, W.; Vatner, S.F.; Camici, P.G. Hibernating myocardium. N. Engl. J. Med. 1998, 339, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Schelbert, H.R.; Bax, J.J. The need for standardisation of cardiac FDG PET imaging in the evaluation of myocardial viability in patients with chronic ischaemic left ventricular dysfunction. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Phelps, M.E.; Hoffman, E.J.; Selin, C.; Huang, S.C.; Robinson, G.; MacDonald, N.; Schelbert, H.; Kuhl, D.E. Investigation of [18F]2-fluoro-2-deoxyglucose for the measure of myocardial glucose metabolism. J. Nucl. Med. 1978, 19, 1311–1319. [Google Scholar] [PubMed]
- Araujo, L.I.; Lammertsma, A.A.; Rhodes, C.G.; McFalls, E.O.; Iida, H.; Rechavia, E.; Galassi, A.; De Silva, R.; Jones, T.; Maseri, A. Noninvasive quantification of regional myocardial blood flow in coronary artery disease with oxygen-15-labeled carbon dioxide inhalation and positron emission tomography. Circulation 1991, 83, 875–885. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, S.R.; Herrero, P.; Markham, J.; Weinheimer, C.J.; Walsh, M.N. Noninvasive quantitation of myocardial blood flow in human subjects with oxygen-15-labeled water and positron emission tomography. J. Am. Coll. Cardiol. 1989, 14, 639–652. [Google Scholar] [CrossRef] [Green Version]
- Schelbert, H.R.; Phelps, M.E.; Hoffman, E.J.; Huang, S.C.; Selin, C.E.; Kuhl, D.E. Regional myocardial perfusion assessed with N-13 labeled ammonia and positron emission computerized axial tomography. Am. J. Cardiol. 1979, 43, 209–218. [Google Scholar] [CrossRef]
- Hutchins, G.D.; Schwaiger, M.; Rosenspire, K.C.; Krivokapich, J.; Schelbert, H.; Kuhl, D.E. Noninvasive quantification of regional blood flow in the human heart using N-13 ammonia and dynamic positron emission tomographic imaging. J. Am. Coll. Cardiol. 1990, 15, 1032–1042. [Google Scholar] [CrossRef]
- Herrero, P.; Markham, J.; Shelton, M.E.; Weinheimer, C.J.; Bergmann, S.R. Noninvasive quantification of regional myocardial perfusion with rubidium-82 and positron emission tomography. Exploration of a mathematical model. Circulation 1990, 82, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Nekolla, S.G.; Reder, S.; Saraste, A.; Higuchi, T.; Dzewas, G.; Preissel, A.; Huisman, M.; Poethko, T.; Schuster, T.; Yu, M.; et al. Evaluation of the novel myocardial perfusion positron-emission tomography tracer 18F-BMS-747158-02: Comparison to 13N-ammonia and validation with microspheres in a pig model. Circulation 2009, 119, 2333–2342. [Google Scholar] [CrossRef] [PubMed]
- Maddahi, J.; Czernin, J.; Lazewatsky, J.; Huang, S.C.; Dahlbom, M.; Schelbert, H.; Sparks, R.; Ehlgen, A.; Crane, P.; Zhu, Q.; et al. Phase I, first-in-human study of BMS747158, a novel 18F-labeled tracer for myocardial perfusion PET: Dosimetry, biodistribution, safety, and imaging characteristics after a single injection at rest. J. Nucl. Med. 2011, 52, 1490–1498. [Google Scholar] [CrossRef] [PubMed]
- Berman, D.S.; Maddahi, J.; Tamarappoo, B.K.; Czernin, J.; Taillefer, R.; Udelson, J.E.; Gibson, C.M.; Devine, M.; Lazewatsky, J.; Bhat, G.; et al. Phase II safety and clinical comparison with single-photon emission computed tomography myocardial perfusion imaging for detection of coronary artery disease: Flurpiridaz F 18 positron emission tomography. J. Am. Coll. Cardiol. 2013, 61, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Uren, N.G.; Melin, J.A.; De Bruyne, B.; Wijns, W.; Baudhuin, T.; Camici, P.G. Relation between myocardial blood flow and the severity of coronary-artery stenosis. N. Engl. J. Med. 1994, 330, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, P.A.; Gnecchi-Ruscone, T.; Yap, J.T.; Rimoldi, O.; Camici, P.G. Assessment of the reproducibility of baseline and hyperemic myocardial blood flow measurements with 15O-labeled water and PET. J. Nucl. Med. 1999, 40, 1848–1856. [Google Scholar] [PubMed]
- Kaufmann, P.A.; Gnecchi-Ruscone, T.; di Terlizzi, M.; Schafers, K.P.; Luscher, T.F.; Camici, P.G. Coronary heart disease in smokers: Vitamin C restores coronary microcirculatory function. Circulation 2000, 102, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Gaemperli, O.; Schepis, T.; Koepfli, P.; Siegrist, P.T.; Fleischman, S.; Nguyen, P.; Olmsted, A.; Wang, W.; Lieu, H.; Kaufmann, P.A. Interaction of caffeine with regadenoson-induced hyperemic myocardial blood flow as measured by positron emission tomography: A randomized, double-blind, placebo-controlled crossover trial. J. Am. Coll. Cardiol. 2008, 51, 328–329. [Google Scholar] [CrossRef] [PubMed]
- Wyss, C.A.; Koepfli, P.; Mikolajczyk, K.; Burger, C.; von Schulthess, G.K.; Kaufmann, P.A. Bicycle exercise stress in PET for assessment of coronary flow reserve: Repeatability and comparison with adenosine stress. J. Nucl. Med. 2003, 44, 146–154. [Google Scholar] [PubMed]
- Maddahi, J.; Packard, R.R. Cardiac PET perfusion tracers: Current status and future directions. Semin. Nucl. Med. 2014, 44, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Schafers, K.P.; Spinks, T.J.; Camici, P.G.; Bloomfield, P.M.; Rhodes, C.G.; Law, M.P.; Baker, C.S.; Rimoldi, O. Absolute quantification of myocardial blood flow with H(2)(15)O and 3-dimensional PET: An experimental validation. J. Nucl. Med. 2002, 43, 1031–1040. [Google Scholar] [PubMed]
- Bol, A.; Melin, J.A.; Vanoverschelde, J.L.; Baudhuin, T.; Vogelaers, D.; De Pauw, M.; Michel, C.; Luxen, A.; Labar, D.; Cogneau, M.; et al. Direct comparison of [13N]ammonia and [15O]water estimates of perfusion with quantification of regional myocardial blood flow by microspheres. Circulation 1993, 87, 512–525. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, S.R.; Fox, K.A.; Rand, A.L.; McElvany, K.D.; Welch, M.J.; Markham, J.; Sobel, B.E. Quantification of regional myocardial blood flow in vivo with H215O. Circulation 1984, 70, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Selwyn, A.P.; Allan, R.M.; L’Abbate, A.; Horlock, P.; Camici, P.; Clark, J.; O’Brien, H.A.; Grant, P.M. Relation between regional myocardial uptake of rubidium-82 and perfusion: Absolute reduction of cation uptake in ischemia. Am. J. Cardiol. 1982, 50, 112–121. [Google Scholar] [CrossRef]
- Lautamaki, R.; George, R.T.; Kitagawa, K.; Higuchi, T.; Merrill, J.; Voicu, C.; DiPaula, A.; Nekolla, S.G.; Lima, J.A.; Lardo, A.C.; et al. Rubidium-82 PET-CT for quantitative assessment of myocardial blood flow: Validation in a canine model of coronary artery stenosis. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Herrero, P.; Hartman, J.J.; Green, M.A.; Anderson, C.J.; Welch, M.J.; Markham, J.; Bergmann, S.R. Regional myocardial perfusion assessed with generator-produced copper-62-PTSM and PET. J. Nucl. Med. 1996, 37, 1294–1300. [Google Scholar] [PubMed]
- Fukushima, K.; Javadi, M.S.; Higuchi, T.; Lautamaki, R.; Merrill, J.; Nekolla, S.G.; Bengel, F.M. Prediction of short-term cardiovascular events using quantification of global myocardial flow reserve in patients referred for clinical 82Rb PET perfusion imaging. J. Nucl. Med. 2011, 52, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Ziadi, M.C.; Dekemp, R.A.; Williams, K.A.; Guo, A.; Chow, B.J.; Renaud, J.M.; Ruddy, T.D.; Sarveswaran, N.; Tee, R.E.; Beanlands, R.S. Impaired myocardial flow reserve on rubidium-82 positron emission tomography imaging predicts adverse outcomes in patients assessed for myocardial ischemia. J. Am. Coll. Cardiol. 2011, 58, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Farhad, H.; Dunet, V.; Bachelard, K.; Allenbach, G.; Kaufmann, P.A.; Prior, J.O. Added prognostic value of myocardial blood flow quantitation in rubidium-82 positron emission tomography imaging. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 1203–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murthy, V.L.; Naya, M.; Foster, C.R.; Hainer, J.; Gaber, M.; Di Carli, G.; Blankstein, R.; Dorbala, S.; Sitek, A.; Pencina, M.J.; et al. Improved cardiac risk assessment with noninvasive measures of coronary flow reserve. Circulation 2011, 124, 2215–2224. [Google Scholar] [CrossRef] [PubMed]
- Muzik, O.; Beanlands, R.S.; Hutchins, G.D.; Mangner, T.J.; Nguyen, N.; Schwaiger, M. Validation of nitrogen-13-ammonia tracer kinetic model for quantification of myocardial blood flow using PET. J. Nucl. Med. 1993, 34, 83–91. [Google Scholar] [PubMed]
- Bellina, C.R.; Parodi, O.; Camici, P.; Salvadori, P.A.; Taddei, L.; Fusani, L.; Guzzardi, R.; Klassen, G.A.; L’Abbate, A.L.; Donato, L. Simultaneous in vitro and in vivo validation of nitrogen-13-ammonia for the assessment of regional myocardial blood flow. J. Nucl. Med. 1990, 31, 1335–1343. [Google Scholar] [PubMed]
- Choi, Y.; Huang, S.C.; Hawkins, R.A.; Kim, J.Y.; Kim, B.T.; Hoh, C.K.; Chen, K.; Phelps, M.E.; Schelbert, H.R. Quantification of myocardial blood flow using 13N-ammonia and PET: Comparison of tracer models. J. Nucl. Med. 1999, 40, 1045–1055. [Google Scholar] [PubMed]
- Chow, B.J.; Beanlands, R.S.; Lee, A.; DaSilva, J.N.; deKemp, R.A.; Alkahtani, A.; Ruddy, T.D. Treadmill exercise produces larger perfusion defects than dipyridamole stress N-13 ammonia positron emission tomography. J. Am. Coll. Cardiol. 2006, 47, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Huisman, M.C.; Higuchi, T.; Reder, S.; Nekolla, S.G.; Poethko, T.; Wester, H.J.; Ziegler, S.I.; Casebier, D.S.; Robinson, S.P.; Schwaiger, M. Initial characterization of an 18F-labeled myocardial perfusion tracer. J. Nucl. Med. 2008, 49, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Kim, H.S.; Le, U.N.; Jiang, S.N.; Kim, H.J.; Lee, K.C.; Woo, S.K.; Chung, J.; Kim, H.S.; Bom, H.S.; et al. Evaluation of a mitochondrial voltage sensor, (18F-fluoropentyl)triphenylphosphonium cation, in a rat myocardial infarction model. J. Nucl. Med. 2012, 53, 1779–1785. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Kim, H.J.; Yu, K.H.; Min, J.J. Synthesis of [18F]-labeled (2-(2-fluoroethoxy)ethyl)tris(4-methoxyphenyl)phosphonium cation as a potential agent for positron emission tomography myocardial imaging. Nucl. Med. Biol. 2012, 39, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Kim, H.J.; Yu, K.H.; Min, J.J. Synthesis of [18F]-labeled (6-fluorohexyl)triphenylphosphonium cation as a potential agent for myocardial imaging using positron emission tomography. Bioconj. Chem. 2012, 23, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Dilsizian, V.; Taillefer, R. Journey in evolution of nuclear cardiology: Will there be another quantum leap with the F-18-labeled myocardial perfusion tracers? JACC Cardiovasc. Imaging 2012, 5, 1269–1284. [Google Scholar] [CrossRef] [PubMed]
- Rischpler, C.; Park, M.J.; Fung, G.S.; Javadi, M.; Tsui, B.M.; Higuchi, T. Advances in PET myocardial perfusion imaging: F-18 labeled tracers. Ann. Nucl. Med. 2012, 26, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nekolla, S.G.; Saraste, A. Novel F-18-labeled PET myocardial perfusion tracers: Bench to bedside. Curr. Cardiol. Rep. 2011, 13, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Camici, P.G.; Prasad, S.K.; Rimoldi, O.E. Stunning, hibernation, and assessment of myocardial viability. Circulation 2008, 117, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Barnes, E.; Dutka, D.P.; Khan, M.; Camici, P.G.; Hall, R.J. Effect of repeated episodes of reversible myocardial ischemia on myocardial blood flow and function in humans. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H1603–H1608. [Google Scholar] [CrossRef] [PubMed]
- Pagano, D.; Fath-Ordoubadi, F.; Beatt, K.J.; Townend, J.N.; Bonser, R.S.; Camici, P.G. Effects of coronary revascularisation on myocardial blood flow and coronary vasodilator reserve in hibernating myocardium. Heart 2001, 85, 208–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Underwood, S.R.; Bax, J.J.; vom Dahl, J.; Henein, M.Y.; Knuuti, J.; van Rossum, A.C.; Schwarz, E.R.; Vanoverschelde, J.L.; van der Wall, E.E.; Wijns, W. Imaging techniques for the assessment of myocardial hibernation. Report of a Study Group of the European Society of Cardiology. Eur. Heart J. 2004, 25, 815–836. [Google Scholar] [CrossRef] [PubMed]
- Desideri, A.; Cortigiani, L.; Christen, A.I.; Coscarelli, S.; Gregori, D.; Zanco, P.; Komorovsky, R.; Bax, J.J. The extent of perfusion-F18-fluorodeoxyglucose positron emission tomography mismatch determines mortality in medically treated patients with chronic ischemic left ventricular dysfunction. J. Am. Coll. Cardiol. 2005, 46, 1264–1269. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.; Calvert, M.; Freemantle, N.; Arrow, Y.; Ball, S.G.; Bonser, R.S.; Chattopadhyay, S.; Norell, M.S.; Pennell, D.J.; Senior, R. The Heart Failure Revascularisation Trial (HEART). Eur. J. Heart Fail. 2011, 13, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonow, R.O.; Maurer, G.; Lee, K.L.; Holly, T.A.; Binkley, P.F.; Desvigne-Nickens, P.; Drozdz, J.; Farsky, P.S.; Feldman, A.M.; Doenst, T.; et al. Myocardial viability and survival in ischemic left ventricular dysfunction. N. Engl. J. Med. 2011, 364, 1617–1625. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.N.; Khattar, R.S.; Senior, R. The hibernating myocardium: Current concepts, diagnostic dilemmas, and clinical challenges in the post-STICH era. Eur. Heart J. 2013, 34, 1323–1336. [Google Scholar] [CrossRef] [PubMed]
- Perrone-Filardi, P.; Pinto, F.J. Looking for myocardial viability after a STICH trial: Not enough to close the door. J. Nucl. Med. 2012, 53, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Allman, K.C.; Shaw, L.J.; Hachamovitch, R.; Udelson, J.E. Myocardial viability testing and impact of revascularization on prognosis in patients with coronary artery disease and left ventricular dysfunction: A meta-analysis. J. Am. Coll. Cardiol. 2002, 39, 1151–1158. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Rev. Esp. Cardiol. 2016, 69, 1167. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Visser, F.C.; Poldermans, D.; Elhendy, A.; Cornel, J.H.; Boersma, E.; Valkema, R.; Van Lingen, A.; Fioretti, P.M.; Visser, C.A. Relationship between preoperative viability and postoperative improvement in LVEF and heart failure symptoms. J. Nucl. Med. 2001, 42, 79–86. [Google Scholar] [PubMed]
- Beanlands, R.S.; Ruddy, T.D.; deKemp, R.A.; Iwanochko, R.M.; Coates, G.; Freeman, M.; Nahmias, C.; Hendry, P.; Burns, R.J.; Lamy, A.; et al. Positron emission tomography and recovery following revascularization (PARR-1): The importance of scar and the development of a prediction rule for the degree of recovery of left ventricular function. J. Am. Coll. Cardiol. 2002, 40, 1735–1743. [Google Scholar] [CrossRef]
- Ling, L.F.; Marwick, T.H.; Flores, D.R.; Jaber, W.A.; Brunken, R.C.; Cerqueira, M.D.; Hachamovitch, R. Identification of therapeutic benefit from revascularization in patients with left ventricular systolic dysfunction: Inducible ischemia versus hibernating myocardium. Circ. Cardiovasc. Imaging 2013, 6, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Namdar, M.; Rager, O.; Priamo, J.; Frei, A.; Noble, S.; Amzalag, G.; Ratib, O.; Nkoulou, R. Prognostic value of revascularising viable myocardium in elderly patients with stable coronary artery disease and left ventricular dysfunction: A PET/CT study. Int. J. Cardiovasc. Imaging 2018. [Google Scholar] [CrossRef] [PubMed]
- Machac, J. Cardiac positron emission tomography imaging. Semin. Nucl. Med. 2005, 35, 17–36. [Google Scholar] [CrossRef] [PubMed]
- Schindler, T.H.; Schelbert, H.R.; Quercioli, A.; Dilsizian, V. Cardiac PET imaging for the detection and monitoring of coronary artery disease and microvascular health. JACC Cardiovasc. Imaging 2010, 3, 623–640. [Google Scholar] [CrossRef] [PubMed]
- Schindler, T.H.; Zhang, X.L.; Vincenti, G.; Mhiri, L.; Lerch, R.; Schelbert, H.R. Role of PET in the evaluation and understanding of coronary physiology. J. Nucl. Cardiol. 2007, 14, 589–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camici, P.G.; Crea, F. Coronary microvascular dysfunction. N. Engl. J. Med. 2007, 356, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Neglia, D.; Michelassi, C.; Trivieri, M.G.; Sambuceti, G.; Giorgetti, A.; Pratali, L.; Gallopin, M.; Salvadori, P.; Sorace, O.; Carpeggiani, C.; et al. Prognostic role of myocardial blood flow impairment in idiopathic left ventricular dysfunction. Circulation 2002, 105, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Shaw, L.J.; Min, J.K.; Hachamovitch, R.; Peterson, E.D.; Hendel, R.C.; Woodard, P.K.; Berman, D.S.; Douglas, P.S. Cardiovascular imaging research at the crossroads. JACC Cardiovasc. Imaging 2010, 3, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Hachamovitch, R.; Kang, X.; Amanullah, A.M.; Abidov, A.; Hayes, S.W.; Friedman, J.D.; Cohen, I.; Thomson, L.E.; Germano, G.; Berman, D.S. Prognostic implications of myocardial perfusion single-photon emission computed tomography in the elderly. Circulation 2009, 120, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Herzog, B.A.; Husmann, L.; Valenta, I.; Gaemperli, O.; Siegrist, P.T.; Tay, F.M.; Burkhard, N.; Wyss, C.A.; Kaufmann, P.A. Long-term prognostic value of 13N-ammonia myocardial perfusion positron emission tomography added value of coronary flow reserve. J. Am. Coll. Cardiol. 2009, 54, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schindler, T.H.; Campisi, R.; Dorsey, D.; Prior, J.O.; Olschewski, M.; Sayre, J.; Schelbert, H.R. Effect of hormone replacement therapy on vasomotor function of the coronary microcirculation in post-menopausal women with medically treated cardiovascular risk factors. Eur. Heart J. 2009, 30, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Schindler, T.H.; Cardenas, J.; Prior, J.O.; Facta, A.D.; Kreissl, M.C.; Zhang, X.L.; Sayre, J.; Dahlbom, M.; Licinio, J.; Schelbert, H.R. Relationship between increasing body weight, insulin resistance, inflammation, adipocytokine leptin, and coronary circulatory function. J. Am. Coll. Cardiol. 2006, 47, 1188–1195. [Google Scholar] [CrossRef] [PubMed]
- Lima, R.S.; Watson, D.D.; Goode, A.R.; Siadaty, M.S.; Ragosta, M.; Beller, G.A.; Samady, H. Incremental value of combined perfusion and function over perfusion alone by gated SPECT myocardial perfusion imaging for detection of severe three-vessel coronary artery disease. J. Am. Coll. Cardiol. 2003, 42, 64–70. [Google Scholar] [CrossRef]
- Berman, D.S.; Kang, X.; Slomka, P.J.; Gerlach, J.; de Yang, L.; Hayes, S.W.; Friedman, J.D.; Thomson, L.E.; Germano, G. Underestimation of extent of ischemia by gated SPECT myocardial perfusion imaging in patients with left main coronary artery disease. J. Nucl. Cardiol. 2007, 14, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.H.; Kastner, R.J.; Calnon, D.A.; Segalla, D.; Beller, G.A.; Watson, D.D. Quantitative gated single photon emission computed tomography imaging: A counts-based method for display and measurement of regional and global ventricular systolic function. J. Nucl. Cardiol. 1997, 4, 451–463. [Google Scholar] [CrossRef]
- Gould, K.L. Does coronary flow trump coronary anatomy? JACC Cardiovasc. Imaging 2009, 2, 1009–1023. [Google Scholar] [CrossRef] [PubMed]
- Gould, K.L. Coronary flow reserve and pharmacologic stress perfusion imaging: Beginnings and evolution. JACC Cardiovasc. Imaging 2009, 2, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Dayanikli, F.; Grambow, D.; Muzik, O.; Mosca, L.; Rubenfire, M.; Schwaiger, M. Early detection of abnormal coronary flow reserve in asymptomatic men at high risk for coronary artery disease using positron emission tomography. Circulation 1994, 90, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Gimelli, A.; Schneider-Eicke, J.; Neglia, D.; Sambuceti, G.; Giorgetti, A.; Bigalli, G.; Parodi, G.; Pedrinelli, R.; Parodi, O. Homogeneously reduced versus regionally impaired myocardial blood flow in hypertensive patients: Two different patterns of myocardial perfusion associated with degree of hypertrophy. J. Am. Coll. Cardiol. 1998, 31, 366–373. [Google Scholar] [CrossRef]
- Di Carli, M.F.; Janisse, J.; Grunberger, G.; Ager, J. Role of chronic hyperglycemia in the pathogenesis of coronary microvascular dysfunction in diabetes. J. Am. Coll. Cardiol. 2003, 41, 1387–1393. [Google Scholar] [CrossRef]
- Tio, R.A.; Dabeshlim, A.; Siebelink, H.M.; de Sutter, J.; Hillege, H.L.; Zeebregts, C.J.; Dierckx, R.A.; van Veldhuisen, D.J.; Zijlstra, F.; Slart, R.H. Comparison between the prognostic value of left ventricular function and myocardial perfusion reserve in patients with ischemic heart disease. J. Nucl. Med. 2009, 50, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Adenaw, N.; Salerno, M. PET/MRI: Current state of the art and future potential for cardiovascular applications. J. Nucl. Cardiol. 2013, 20, 976–989. [Google Scholar] [CrossRef] [PubMed]
- Valenta, I.; Quercioli, A.; Schindler, T.H. Diagnostic value of PET-measured longitudinal flow gradient for the identification of coronary artery disease. JACC Cardiovasc. Imaging 2014, 7, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Dey, D.; Diaz Zamudio, M.; Schuhbaeck, A.; Juarez Orozco, L.E.; Otaki, Y.; Gransar, H.; Li, D.; Germano, G.; Achenbach, S.; Berman, D.S.; et al. Relationship between Quantitative Adverse Plaque Features from Coronary Computed Tomography Angiography and Downstream Impaired Myocardial Flow Reserve by 13N-Ammonia Positron Emission Tomography: A Pilot Study. Circul. Cardiovasc. Imaging 2015, 8, e003255. [Google Scholar] [CrossRef] [PubMed]
- Pelizzari, C.A.; Chen, G.T.; Spelbring, D.R.; Weichselbaum, R.R.; Chen, C.T. Accurate three-dimensional registration of CT, PET, and/or MR images of the brain. J. Comput. Assist. Tomogr. 1989, 13, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.P.; Mazziotta, J.C.; Cherry, S.R. MRI-PET registration with automated algorithm. J. Comput. Assist. Tomogr. 1993, 17, 536–546. [Google Scholar] [CrossRef] [PubMed]
- Pichler, B.J.; Judenhofer, M.S.; Catana, C.; Walton, J.H.; Kneilling, M.; Nutt, R.E.; Siegel, S.B.; Claussen, C.D.; Cherry, S.R. Performance test of an LSO-APD detector in a 7-T MRI scanner for simultaneous PET/MRI. J. Nucl. Med. 2006, 47, 639–647. [Google Scholar] [PubMed]
- Krizsan, A.K.; Lajtos, I.; Dahlbom, M.; Daver, F.; Emri, M.; Kis, S.A.; Opposits, G.; Pohubi, L.; Potari, N.; Hegyesi, G.; et al. Promising Future: Comparable Imaging Capability of MRI-Compatible Silicon Photomultiplier and Conventional Photosensor Preclinical PET Systems. J. Nucl. Med. 2015, 56, 1948–1953. [Google Scholar] [CrossRef] [PubMed]
- Robson, P.M.; Dey, D.; Newby, D.E.; Berman, D.; Li, D.; Fayad, Z.A.; Dweck, M.R. MR/PET Imaging of the Cardiovascular System. JACC Cardiovasc. Imaging 2017, 10, 1165–1179. [Google Scholar] [CrossRef] [PubMed]
- Munoz, C.; Kunze, K.P.; Neji, R.; Vitadello, T.; Rischpler, C.; Botnar, R.M.; Nekolla, S.G.; Prieto, C. Motion-corrected whole-heart PET-MR for the simultaneous visualisation of coronary artery integrity and myocardial viability: An initial clinical validation. Eur. J. Nucl. Med. Mol. Imaging 2018. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tracer | Physical Half-Life | Uptake Mechanism | Radionuclide Production | Cyclotron on/off-Site |
|---|---|---|---|---|
| 15O-H2O | 2.06 min | Free diffusion (perfusion) | Cyclotron | on-site |
| 82Rb | 1.25 min | Na/K-ATPase (perfusion) | 82Sr/82Rb generator | off-site |
| 13N-NH3 | 9.96 min | Diffusion/metabolic trapping (perfusion) | Cyclotron | on-site |
| 18F-FDG | 109 min | Glucose transport/hexokinase (viability) | Cyclotron | off-site |
| 15O-H20 | 13N-NH3 | 82Rb | 18F Flurpiridaz | |
|---|---|---|---|---|
| Positron range (mm) | 4.14 | 2.53 | 8.6 | 1.03 |
| Image resolution | Intermediate | Intermediate-high | Lowest | Highest |
| Myocardial extraction fraction | 100% | 80% | 65% | 94% |
| Pharmacological stress imaging protocol | Feasible | Feasible | Feasible | Feasible |
| Treadmill exercise Imaging protocol | Not feasible | Feasible but not practical | Not feasible | Feasible |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazakauskaitė, E.; Žaliaduonytė-Pekšienė, D.; Rumbinaitė, E.; Keršulis, J.; Kulakienė, I.; Jurkevičius, R. Positron Emission Tomography in the Diagnosis and Management of Coronary Artery Disease. Medicina 2018, 54, 47. https://doi.org/10.3390/medicina54030047
Kazakauskaitė E, Žaliaduonytė-Pekšienė D, Rumbinaitė E, Keršulis J, Kulakienė I, Jurkevičius R. Positron Emission Tomography in the Diagnosis and Management of Coronary Artery Disease. Medicina. 2018; 54(3):47. https://doi.org/10.3390/medicina54030047
Chicago/Turabian StyleKazakauskaitė, Eglė, Diana Žaliaduonytė-Pekšienė, Eglė Rumbinaitė, Justas Keršulis, Ilona Kulakienė, and Renaldas Jurkevičius. 2018. "Positron Emission Tomography in the Diagnosis and Management of Coronary Artery Disease" Medicina 54, no. 3: 47. https://doi.org/10.3390/medicina54030047