
Prediction of Emergency Cesarean Section Using Machine Learning Methods: Development and External Validation of a Nationwide Multicenter Dataset in Republic of Korea

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
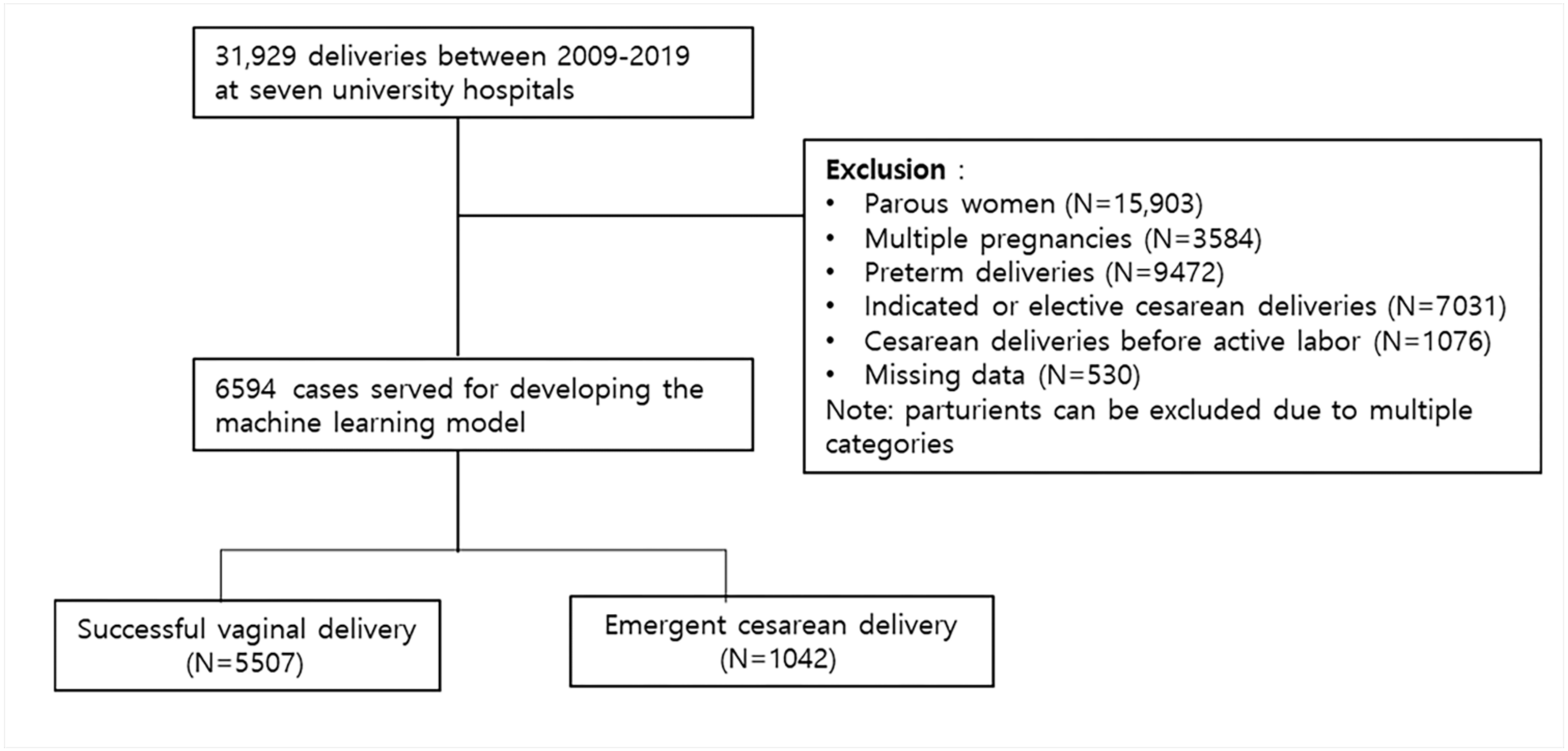
2.2. Study Population
2.3. Variables
2.4. Machine Learning
2.4.1. Dataset
2.4.2. Data Sampling Algorithms
Random Under-Sampling/Oversampling
Tomek Link
Condensed Nearest Neighbor (CNN)
One-Sided Selection (OSS)
Edited Nearest Neighbors (ENN)
Neighbor Cleaning Rule (NCR)
Synthetic Minority Oversampling Technique (SMOTE)
Adaptive Synthetic Sampling (ADASYN)
Borderline SMOTE
2.4.3. Learning Algorithms
Logistic Regression
Random Forest
Gradient Boosting, LGBM, XGBoost
SVM
KNN
Ensembles: Voting, Stacking
2.4.4. Model Evaluation and Validation
2.4.5. Software and Statistical Tools
2.5. External Validation
3. Results
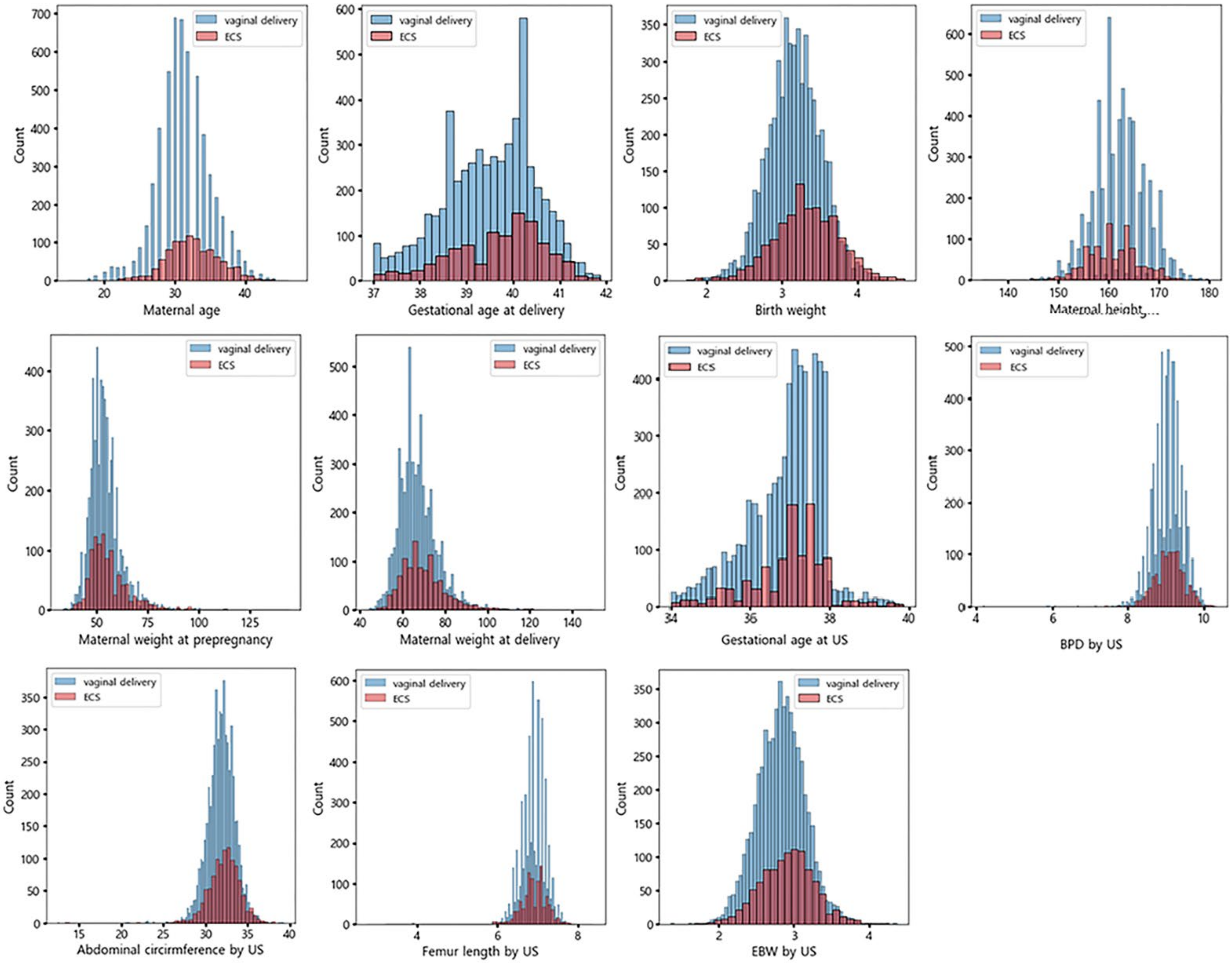
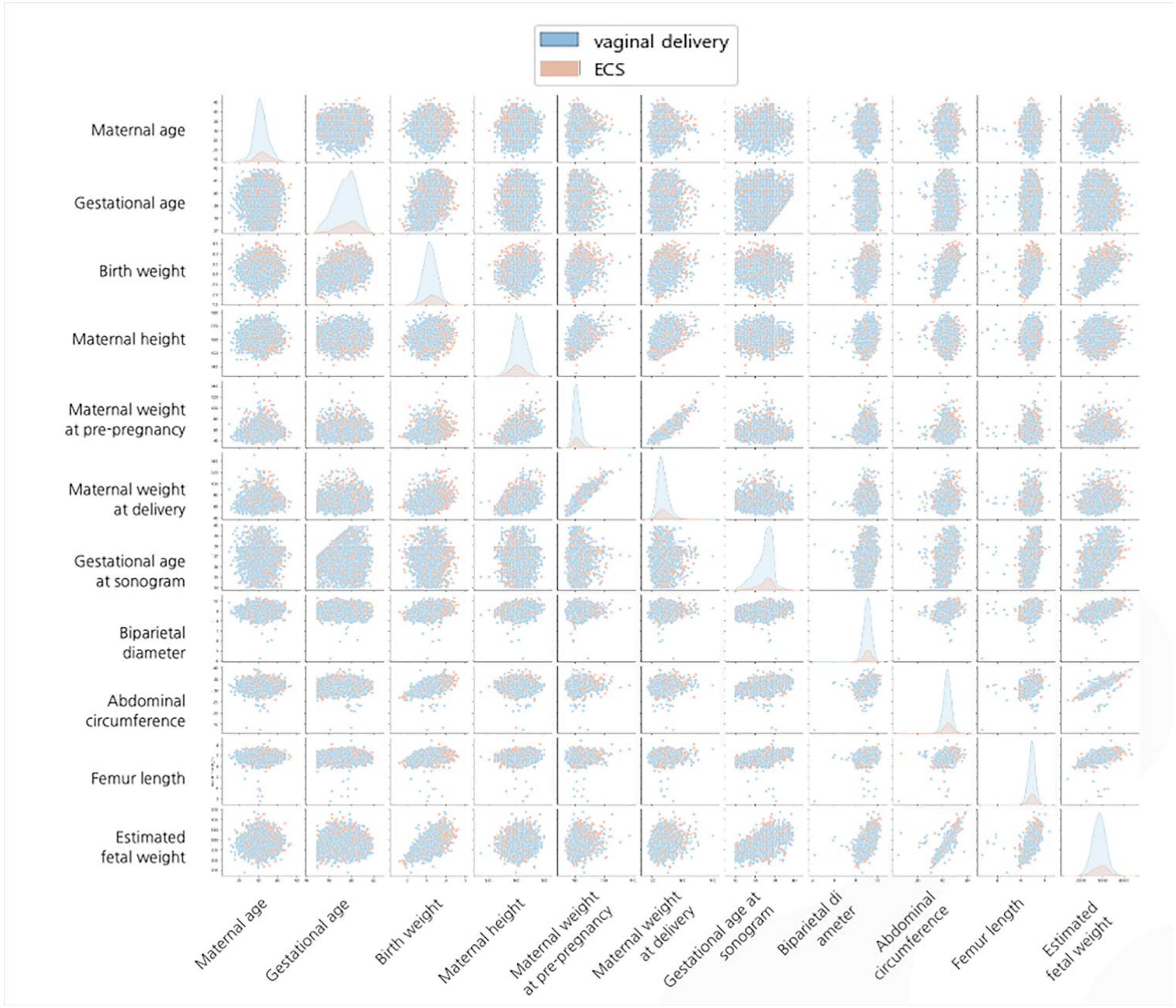
3.1. Patient Characteristics
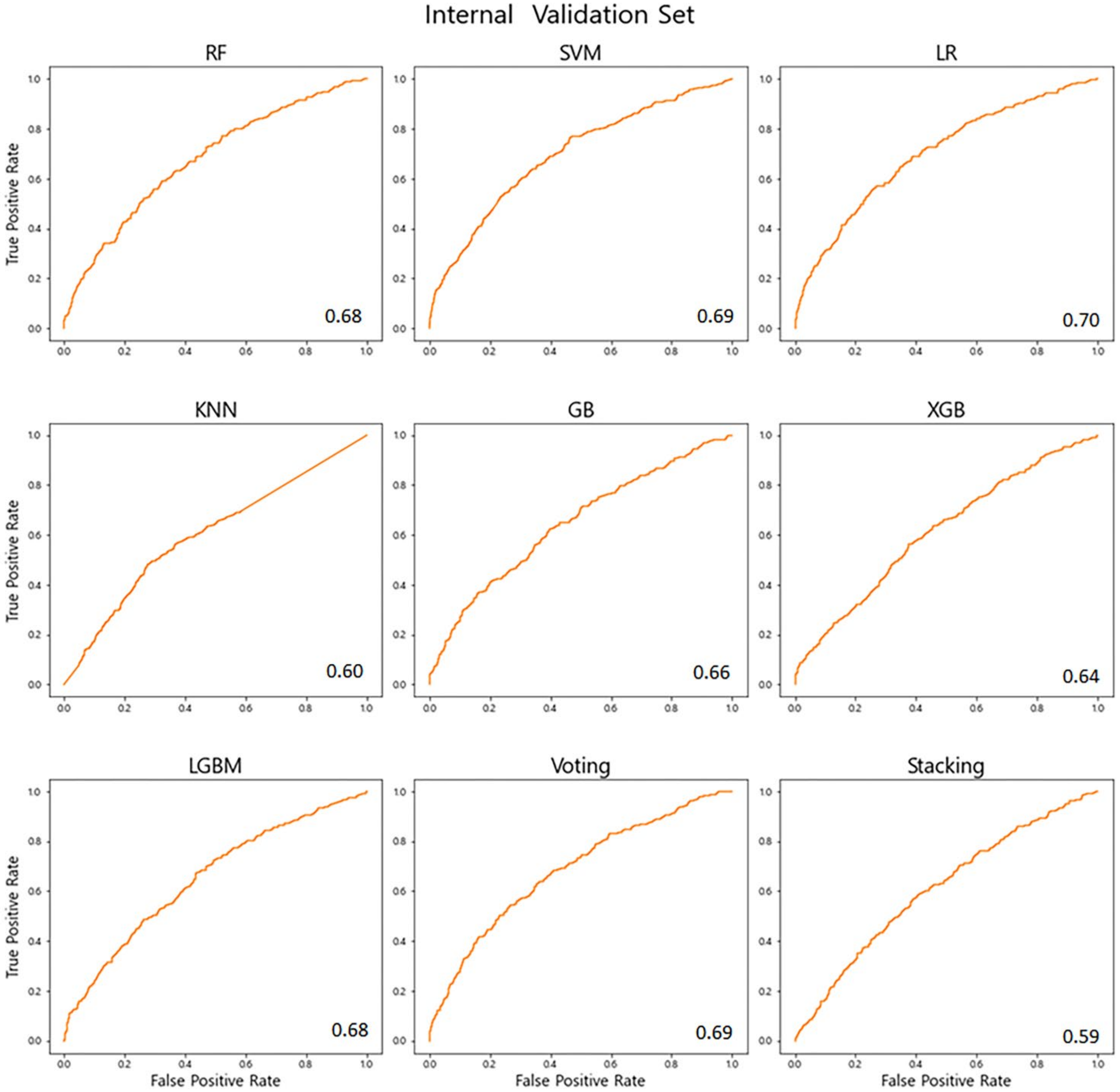
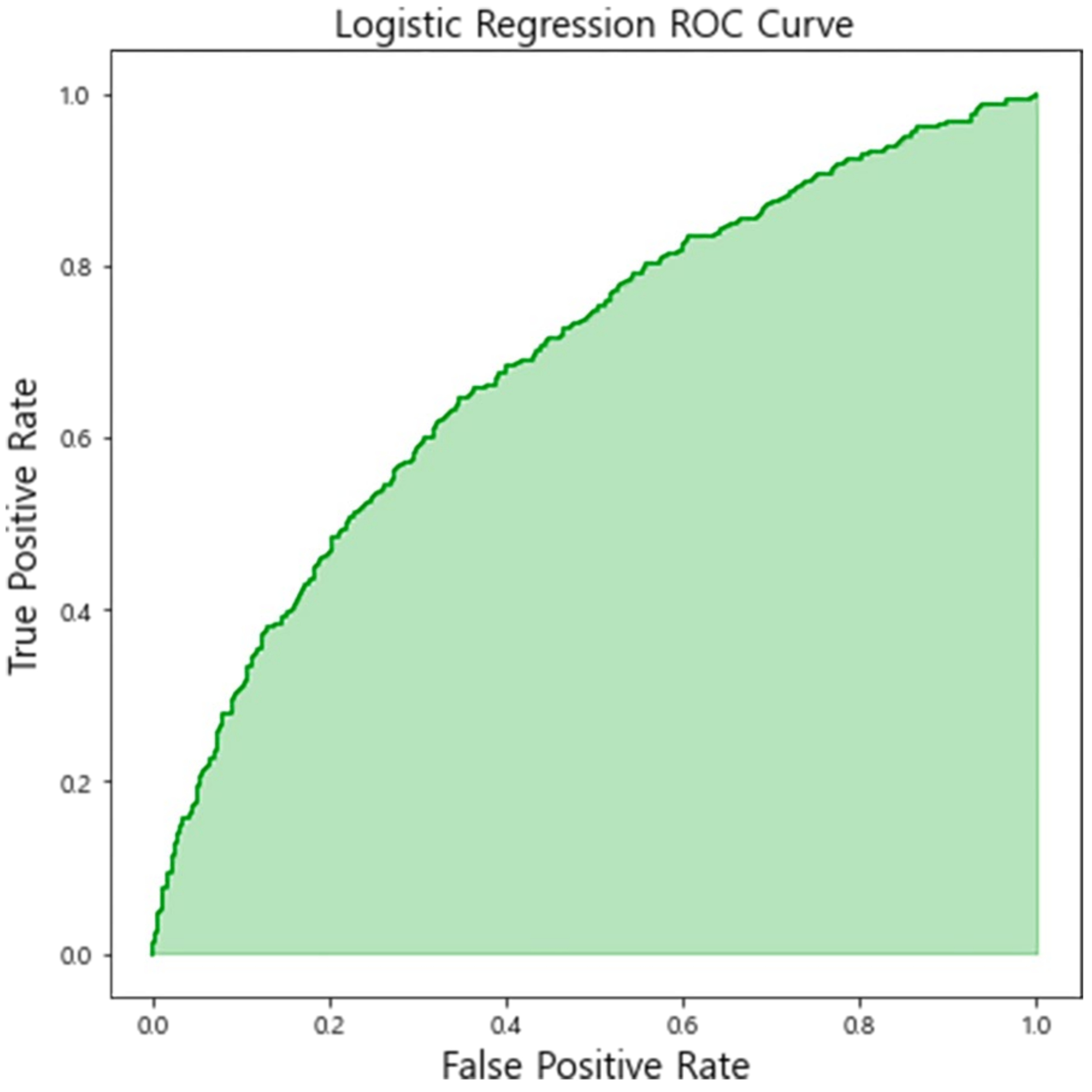
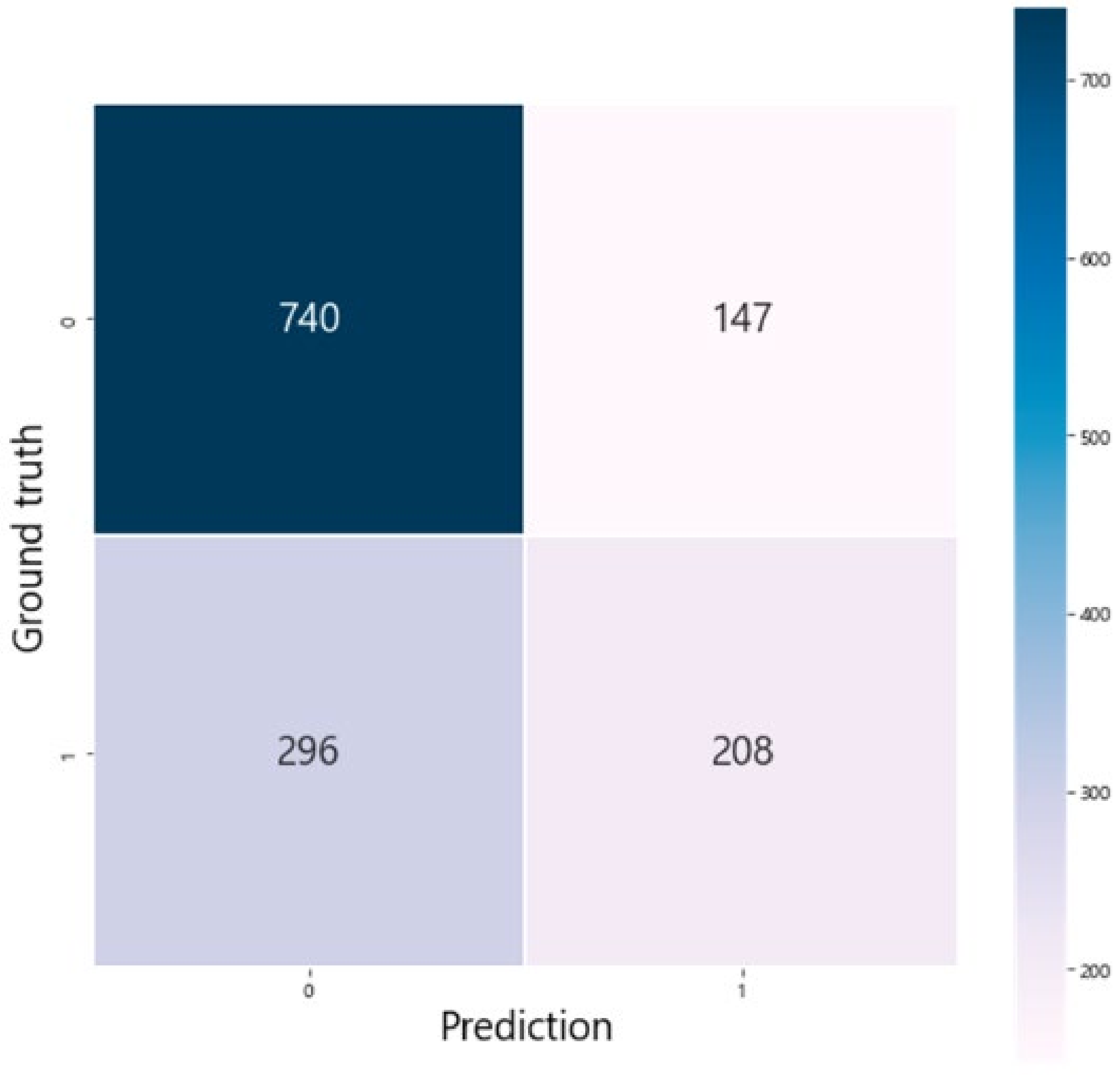
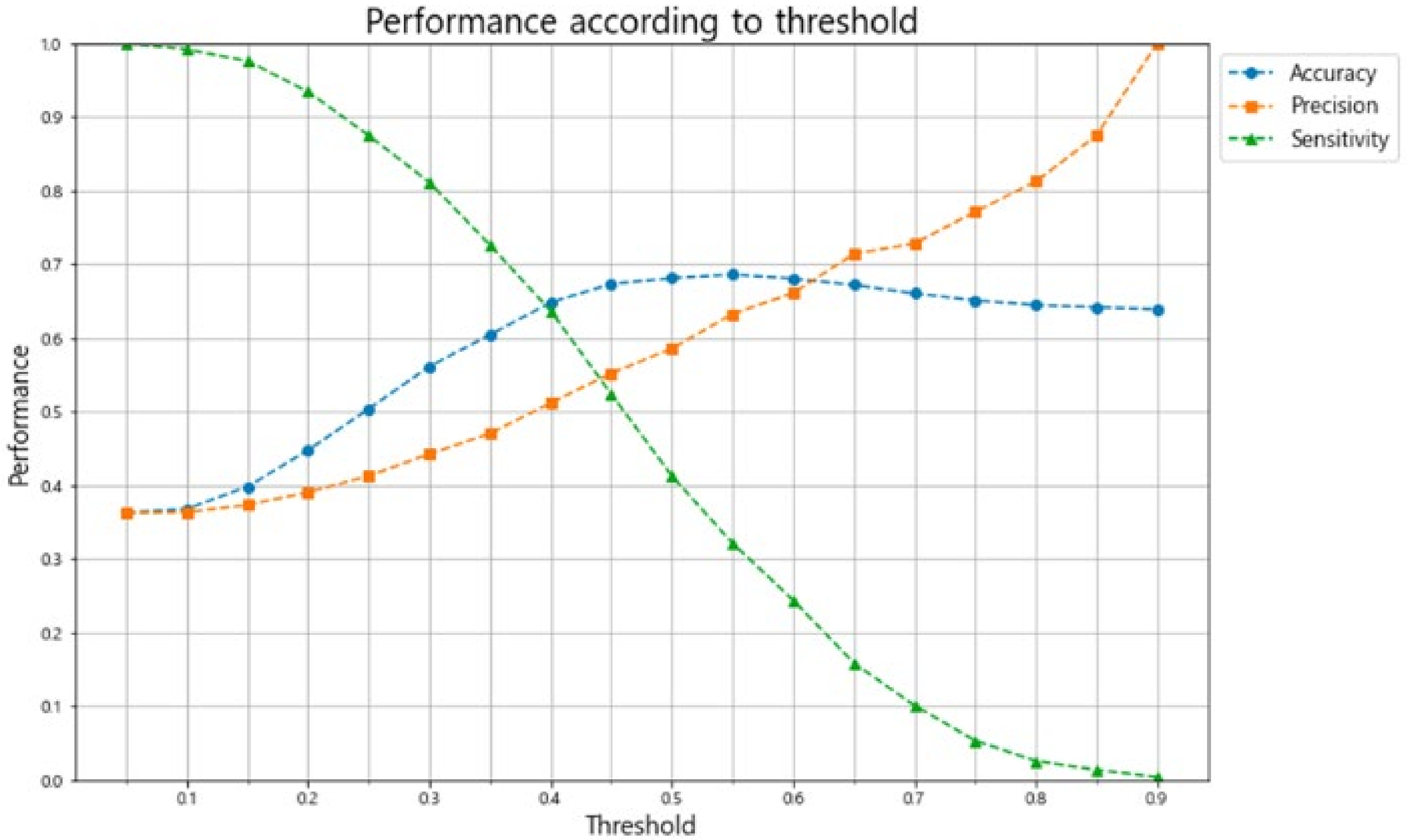
3.2. Model Performance
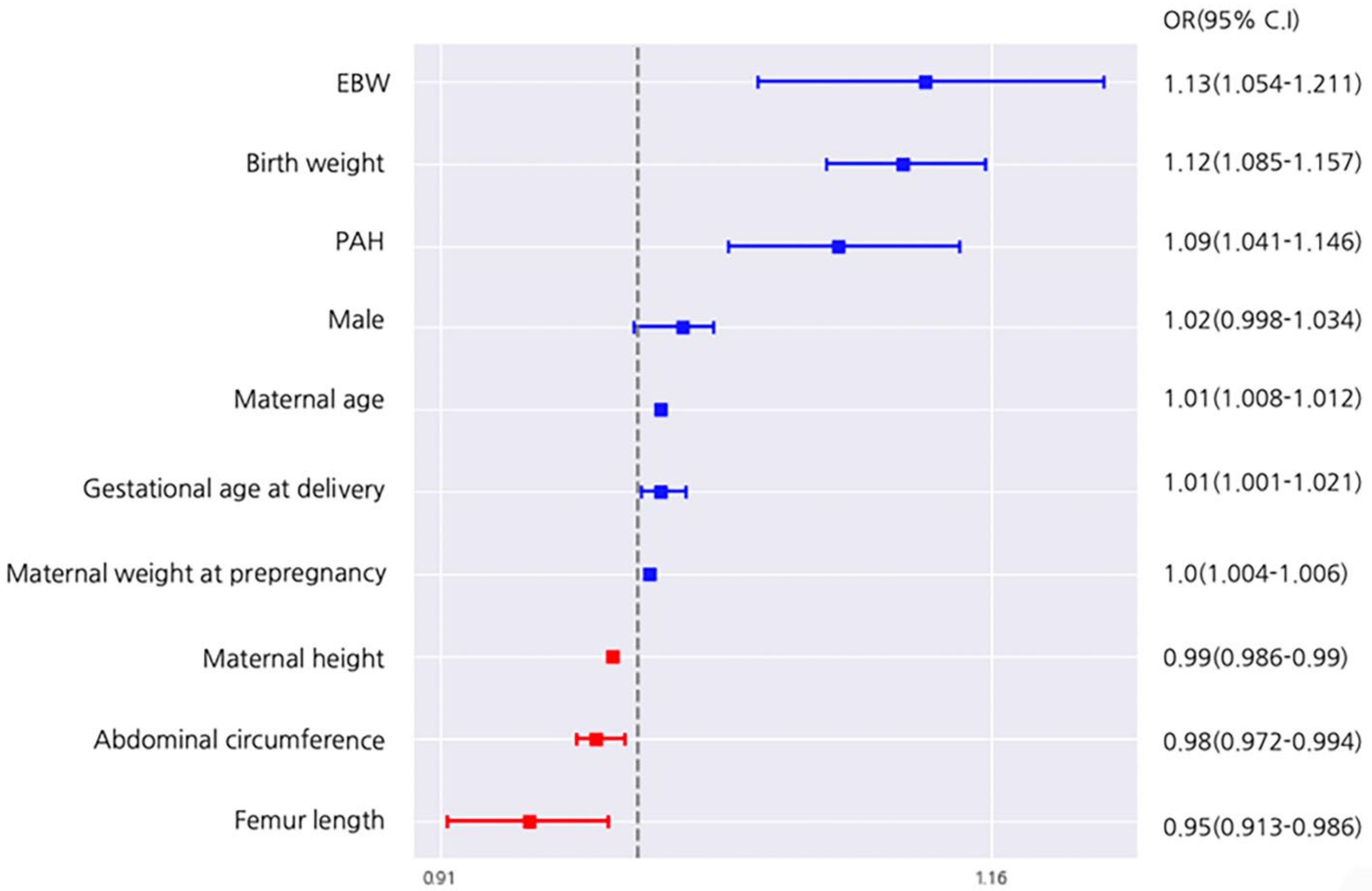
3.3. Variable Influence on the Prediction Model
3.4. External Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Betran, A.P.; Ye, J.; Moller, A.-B.; Souza, J.P.; Zhang, J. Trends and projections of caesarean section rates: Global and regional estimates. BMJ Glob. Health 2021, 6, e005671. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Lee, D.; Kim, J.; Noh, E.; Ahn, K.-H.; Hong, S.-C.; Kim, H.-J.; Oh, M.-J.; Cho, G.J. Secular trends in cesarean sections and risk factors in South Korea (2006–2015). Obstet. Gynecol. Sci. 2020, 63, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Ye, J.; Moller, A.-B.; Zhang, J.; Gulmezoglu, A.M.; Torloni, M.R. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990–2014. PLoS ONE 2016, 11, e0148343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Callaghan, M.; MacLennan, A. Cesarean Delivery and Cerebral Palsy: A systematic review and meta-analysis. Obstet. Gynecol. 2013, 122, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- Pires-Menard, A.; Flatley, C.; Kumar, S. Severe neonatal outcomes associated with emergency cesarean section at term. J. Matern. Fetal Neonatal Med. 2021, 34, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Briand, V.; Dumont, A.; Abrahamowicz, M.; Sow, A.; Traore, M.; Rozenberg, P.; Watier, L.; Fournier, P. Maternal and Perinatal Outcomes by Mode of Delivery in Senegal and Mali: A Cross-Sectional Epidemiological Survey. PLoS ONE 2012, 7, e47352. [Google Scholar] [CrossRef]
- Grace, L.; Greer, R.M.; Kumar, S. Perinatal consequences of a category 1 caesarean section at term. BMJ Open 2015, 5, e007248. [Google Scholar] [CrossRef] [Green Version]
- Lucas, D.N.; Yentis, S.M.; Kinsella, S.M.; Holdcroft, A.; May, A.E.; Wee, M.; Robinson, P.N. Urgency of caesarean section: A new classification. J. R. Soc. Med. 2000, 93, 346–350. [Google Scholar] [CrossRef] [Green Version]
- Wood, S.L.; Tang, S.; Crawford, S. Cesarean delivery in the second stage of labor and the risk of subsequent premature birth. Am. J. Obstet. Gynecol. 2017, 217, 63.e1–63.e10. [Google Scholar] [CrossRef]
- Pergialiotis, V.; Vlachos, D.G.; Rodolakis, A.; Haidopoulos, D.; Thomakos, N.; Vlachos, G.D. First versus second stage C/S maternal and neonatal morbidity: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 175, 15–24. [Google Scholar] [CrossRef]
- Burke, N.; Burke, G.; Breathnach, F.; McAuliffe, F.; Morrison, J.J.; Turner, M.; Dornan, S.; Higgins, J.R.; Cotter, A.; Geary, M.; et al. Prediction of cesarean delivery in the term nulliparous woman: Results from the prospective, multicenter Genesis study. Am. J. Obstet. Gynecol. 2017, 216, 598.e1–598.e11. [Google Scholar] [CrossRef] [PubMed]
- Levine, L.D.; Downes, K.L.; Parry, S.; Elovitz, M.; Sammel, M.D.; Srinivas, S.K. A validated calculator to estimate risk of cesarean after an induction of labor with an unfavorable cervix. Am. J. Obstet. Gynecol. 2018, 218, 254.e1–254.e7. [Google Scholar] [CrossRef] [PubMed]
- Tolcher, M.C.; Holbert, M.R.; Weaver, A.L.; McGree, M.E.; Olson, J.E.; El-Nashar, S.A.; Famuyide, A.; Brost, B. Predicting Cesarean Delivery After Induction of Labor Among Nulliparous Women at Term. Obstet. Gynecol. 2015, 126, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Mardy, A.H.; Ananth, C.V.; Grobman, W.A.; Gyamfi-Bannerman, C. A prediction model of vaginal birth after cesarean in the preterm period. Am. J. Obstet. Gynecol. 2016, 215, 513.e1–513.e7. [Google Scholar] [CrossRef]
- Meyer, R.; Hendin, N.; Zamir, M.; Mor, N.; Levin, G.; Sivan, E.; Aran, D.; Tsur, A. Implementation of machine learning models for the prediction of vaginal birth after cesarean delivery. J. Matern. Fetal Neonatal Med. 2020, 25, 1–7. [Google Scholar] [CrossRef]
- Lipschuetz, M.; Guedalia, J.; Rottenstreich, A.; Persky, M.N.; Cohen, S.M.; Kabiri, D.; Levin, G.; Yagel, S.; Unger, R.; Sompolinsky, Y. Prediction of vaginal birth after cesarean deliveries using machine learning. Am. J. Obstet. Gynecol. 2020, 222, 613.e1–613.e12. [Google Scholar] [CrossRef]
- Tsur, A.; Batsry, L.; Toussia-Cohen, S.; Rosenstein, M.G.; Barak, O.; Brezinov, Y.; Yoeli-Ullman, R.; Sivan, E.; Sirota, M.; Druzin, M.L.; et al. Development and validation of a machine-learning model for prediction of shoulder dystocia. Ultrasound Obstet. Gynecol. 2020, 56, 588–596. [Google Scholar] [CrossRef]
- Eide, K.T.; Morken, N.-H.; Bærøe, K. Maternal reasons for requesting planned cesarean section in Norway: A qualitative study. BMC Pregnancy Childbirth 2019, 19, 102. [Google Scholar] [CrossRef]
- Olieman, R.M.; Siemonsma, F.; Bartens, M.A.; Garthus-Niegel, S.; Scheele, F.; Honig, A. The effect of an elective cesarean section on maternal request on peripartum anxiety and depression in women with childbirth fear: A systematic review. BMC Pregnancy Childbirth 2017, 17, 195. [Google Scholar] [CrossRef]
- Chen, I.; Opiyo, N.; Tavender, E.; Mortazhejri, S.; Rader, T.; Petkovic, J.; Yogasingam, S.; Taljaard, M.; Agarwal, S.; Laopaiboon, M.; et al. Non-clinical interventions for reducing unnecessary caesarean section. Cochrane Database Syst. Rev. 2018, 2018, CD005528. [Google Scholar] [CrossRef]
- Smith, G.C.S.; Smith, M.F.S.; McNay, M.B.; Fleming, J.E.E. The relation between fetal abdominal circumference and birthweight: Findings in 3512 pregnancies. BJOG Int. J. Obstet. Gynaecol. 1997, 104, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Lemaître, G.; Nogueira, F.; Aridas, C.K. Imbalanced-learn: A python toolbox to tackle the curse of imbalanced datasets in machine learning. J. Mach. Learn. Res. 2017, 18, 559–563. [Google Scholar]
- Dubey, R.; Zhou, J.; Wang, Y.; Thompson, P.M.; Ye, J.; The Alzheimer’s Disease Neuroimaging Initiative. Analysis of sampling techniques for imbalanced data: An n = 648 ADNI study. NeuroImage 2014, 87, 220–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estabrooks, A.; Jo, T.; Japkowicz, N. A Multiple Resampling Method for Learning from Imbalanced Data Sets. Comput. Intell. 2004, 20, 18–36. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.L. Asymptotic Properties of Nearest Neighbor Rules Using Edited Data. IEEE Trans. Syst. Man Cybern. 1972, 2, 408–421. [Google Scholar] [CrossRef] [Green Version]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- He, H.; Bai, Y.; Garcia, E.A.; Li, S. ADASYN: Adaptive synthetic sampling approach for imbalanced learning. In Proceedings of the IEEE International Joint Conference on Neural Networks (IEEE World Congress on Computational Intelligence), Hong Kong, China, 1–8 June 2008; pp. 1322–1328. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Wang, W.Y.; Mao, B.H. Borderline-SMOTE: A new over-sampling method in imbalanced data sets learning. In Proceedings of the International Conference on Intelligent Computing, Hefei, China, 23–26 August 2005; pp. 878–887. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- LightGBM. Available online: https://lightgbm.readthedocs.io/ (accessed on 29 March 2022).
- XGBoost. Available online: https://xgboost.readthedocs.io/ (accessed on 29 March 2022).
- Pandas. Available online: https://pandas.pydata.org/ (accessed on 28 March 2022).
- MatPlotLib. Available online: https://matplotlib.org/ (accessed on 28 March 2022).
- Lee, K.-S.; Kim, H.Y.; Lee, S.J.; Kwon, S.O.; Na, S.; Hwang, H.S.; Park, M.H.; Ahn, K.H.; Korean Society of Ultrasound in Obstetrics and Gynecology Research Group. Prediction of newborn’s body mass index using nationwide multicenter ultrasound data: A machine-learning study. BMC Pregnancy Childbirth 2021, 21, 172. [Google Scholar] [CrossRef]
- Treacy, A.; Robson, M.; O’Herlihy, C. Dystocia increases with advancing maternal age. Am. J. Obstet. Gynecol. 2006, 195, 760–763. [Google Scholar] [CrossRef]
- Kwawukume, E.; Ghosh, T.; Wilson, J. Maternal height as a predictor of vaginal delivery. Int. J. Gynecol. Obstet. 1993, 41, 27–30. [Google Scholar] [CrossRef]
- Lipschuetz, M.; Cohen, S.M.; Israel, A.; Baron, J.; Porat, S.; Valsky, D.V.; Yagel, O.; Amsalem, H.; Kabiri, D.; Gilboa, Y.; et al. Sonographic large fetal head circumference and risk of cesarean delivery. Am. J. Obstet. Gynecol. 2018, 218, 339.e1–339.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witter, F.R.; Caulfield, L.E.; Stoltzfus, R.J. Influence of maternal anthropometric status and birth weight on the risk of cesarean delivery. Obstet. Gynecol. 1995, 85, 947–951. [Google Scholar] [CrossRef]
- Stirnemann, J.; Villar, J.; Salomon, L.J.; Ohuma, E.; Ruyan, P.; Altman, D.G.; Nosten, F.; Craik, R.; Munim, S.; Ismail, L.C.; et al. International estimated fetal weight standards of the INTERGROWTH-21(st) Project. Ultrasound Obstet. Gynecol. 2017, 49, 478–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coomarasamy, A.; Connock, M.; Thornton, J.; Khan, K.S. Accuracy of ultrasound biometry in the prediction of macrosomia: A systematic quantitative review. BJOG 2005, 112, 1461–1466. [Google Scholar] [CrossRef]
- Grobman, W.A.; Rice, M.M.; Reddy, U.M.; Tita, A.T.; Silver, R.M.; Mallett, G.; Hill, K.; Thom, E.A.; El-Sayed, Y.Y.; Perez-Delboy, A.; et al. Labor Induction versus Expectant Management in Low-Risk Nulliparous Women. New Engl. J. Med. 2018, 379, 513–523. [Google Scholar] [CrossRef]
- Froehlich, R.J.; Sandoval, G.; Bailit, J.L.; Grobman, W.A.; Reddy, U.M.; Wapner, R.; Varner, M.W.; Thorp, J.M.; Prasad, M.; Tita, A.; et al. Association of Recorded Estimated Fetal Weight and Cesarean Delivery in Attempted Vaginal Delivery at Term. Obstet. Gynecol. 2016, 128, 487–494. [Google Scholar] [CrossRef]
- Guedalia, J.; Lipschuetz, M.; Novoselsky-Persky, M.; Cohen, S.M.; Rottenstreich, A.; Levin, G.; Yagel, S.; Unger, R.; Sompolinsky, Y. Real-time data analysis using a machine learning model significantly improves prediction of successful vaginal deliveries. Am. J. Obstet. Gynecol. 2020, 223, 437.e1–437.e15. [Google Scholar] [CrossRef]
- Kamel, R.A.; Negm, S.M.; Youssef, A.; Bianchini, L.; Brunelli, E.; Pilu, G.; Soliman, M.; Nicolaides, K.H. Predicting cesarean delivery for failure to progress as an outcome of labor induction in term singleton pregnancy. Am. J. Obstet. Gynecol. 2021, 224, 609.e601–609.e611. [Google Scholar] [CrossRef]
- ACOG. ACOG Committee Opinion No. 761: Cesarean Delivery on Maternal Request. Obstet. Gynecol. 2019, 133, e73–e77. [Google Scholar] [CrossRef]
- Nieminen, K.; Stephansson, O.; Ryding, E.L. Women’s fear of childbirth and preference for cesarean section – a cross-sectional study at various stages of pregnancy in Sweden. Acta Obstet. Gynecol. Scand. 2009, 88, 807–813. [Google Scholar] [CrossRef]
- Stützer, P.P.; Berlit, S.; Lis, S.; Schmahl, C.; Sütterlin, M.; Tuschy, B. Elective Caesarean section on maternal request in Germany: Factors affecting decision making concerning mode of delivery. Arch. Gynecol. Obstet. 2017, 295, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Ruppel, H.; Liu, V.X.; Kipnis, P.; Hedderson, M.M.; Greenberg, M.; Forquer, H.; Lawson, B.; Escobar, G.J. Development and Validation of an Obstetric Comorbidity Risk Score for Clinical Use. Women’s Health Rep. 2021, 2, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Kleinrouweler, C.E.; Cheong-See, F.M.; Collins, G.; Kwee, A.; Thangaratinam, S.; Khan, K.S.; Mol, B.W.J.; Pajkrt, E.; Moons, K.G.; Schuit, E. Prognostic models in obstetrics: Available, but far from applicable. Am. J. Obstet. Gynecol. 2016, 214, 79–90.e36. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Successful Vaginal Delivery (n = 5507) | Emergent Cesarean Section (n = 1042) | p-Value |
|---|---|---|---|
| Maternal age, yr | 31.29 ± 3.8 | 32.49 ± 3.95 | <0.001 |
| Gestational age, w | 39.49 ± 0.99 | 39.67 ± 0.99 | <0.001 |
| Birth weight, gm | 3.17 ± 0.36 | 3.31 ± 0.44 | <0.001 |
| Maternal height, cm | 162.24 ± 5.02 | 160.93 ± 5.14 | <0.001 |
| Maternal weight at pre-pregnancy, kg | 53.96 ± 7.93 | 56.05 ± 9.97 | <0.001 |
| Maternal weight at delivery, kg | 67.13 ± 9.11 | 69.92 ± 10.72 | <0.001 |
| Gestational age at sonogram, w | 36.9 ± 0.95 | 36.96 ± 0.95 | 0.075 |
| Sonographic parameters, cm | |||
| Biparietal diameter | 9.05 ± 0.37 | 9.09 ± 0.37 | <0.001 |
| Abdominal circumference | 31.88 ± 1.62 | 32.23 ± 1.88 | <0.001 |
| Femur length | 6.9 ± 0.31 | 6.92 ± 0.33 | 0.125 |
| Estimated fetal weight | 2831.84 ± 320.48 | 2908.89 ± 365.84 | <0.001 |
| Neonate male sex | 2779 (50.46%) | 580 (55.66%) | 0.002 |
| Pregnancy-associated hypertension | 167 (3.03%) | 61 (5.85%) | <0.001 |
| Gestational diabetes | 253 (4.59%) | 62 (5.95%) | 0.072 |
| Algorithm | Accuracy | Precision | Sensitivity | F1_Score | Specificity |
|---|---|---|---|---|---|
| Logistic Regression | 0.78 | 0.35 | 0.43 | 0.39 | 0.85 |
| Voting | 0.83 | 0.38 | 0.17 | 0.23 | 0.95 |
| SVM | 0.77 | 0.31 | 0.37 | 0.34 | 0.85 |
| Random Forest | 0.83 | 0.42 | 0.19 | 0.26 | 0.95 |
| LGBM | 0.85 | 0.55 | 0.15 | 0.23 | 0.98 |
| Gradient Boosting | 0.83 | 0.36 | 0.12 | 0.19 | 0.96 |
| XGBoost | 0.82 | 0.34 | 0.12 | 0.17 | 0.96 |
| KNN | 0.69 | 0.24 | 0.42 | 0.3 | 0.74 |
| Stacking | 0.83 | 0.35 | 0.09 | 0.14 | 0.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wie, J.H.; Lee, S.J.; Choi, S.K.; Jo, Y.S.; Hwang, H.S.; Park, M.H.; Kim, Y.H.; Shin, J.E.; Kil, K.C.; Kim, S.M.; et al. Prediction of Emergency Cesarean Section Using Machine Learning Methods: Development and External Validation of a Nationwide Multicenter Dataset in Republic of Korea. Life 2022, 12, 604. https://doi.org/10.3390/life12040604
Wie JH, Lee SJ, Choi SK, Jo YS, Hwang HS, Park MH, Kim YH, Shin JE, Kil KC, Kim SM, et al. Prediction of Emergency Cesarean Section Using Machine Learning Methods: Development and External Validation of a Nationwide Multicenter Dataset in Republic of Korea. Life. 2022; 12(4):604. https://doi.org/10.3390/life12040604
Chicago/Turabian StyleWie, Jeong Ha, Se Jin Lee, Sae Kyung Choi, Yun Sung Jo, Han Sung Hwang, Mi Hye Park, Yeon Hee Kim, Jae Eun Shin, Ki Cheol Kil, Su Mi Kim, and et al. 2022. "Prediction of Emergency Cesarean Section Using Machine Learning Methods: Development and External Validation of a Nationwide Multicenter Dataset in Republic of Korea" Life 12, no. 4: 604. https://doi.org/10.3390/life12040604