
Corneal Endothelial Cell Loss after Ciliary Sulcus Placement of Ahmed Glaucoma Valve in Patients with Noninfectious Uveitic Glaucoma


Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Objectives
2.3. Data Collection
2.4. Diagnosis
2.5. Surgery
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Suttorp-Schulten, A.; Rothova, A. The Possible Impact of Uveitis in Blindness: A Literature Survey. Br. J. Ophthalmol. 1996, 80, 844–848. [Google Scholar] [CrossRef] [Green Version]
- Siddique, S.S.; Suelves, A.M.; Baheti, U.; Foster, C.S. Glaucoma and Uveitis. Surv. Ophthalmol. 2013, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sung, V.C.T.; Barton, K. Management of Inflammatory Glaucomas. Curr. Opin. Ophthalmol. 2004, 15, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Alfawaz, A.M.; Holland, G.N.; Yu, F.; Margolis, M.S.; Giaconi, J.A.A.; Aldave, A.J. Corneal Endothelium in Patients with Anterior Uveitis. Ophthalmology 2016, 123, 1637–1645. [Google Scholar] [CrossRef] [PubMed]
- Hirooka, K.; Nitta, E.; Ukegawa, K.; Sato, S.; Kiuchi, Y. Effect of trabeculectomy on corneal endothelial cell loss. Br. J. Ophthalmol. 2020, 104, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Hirooka, K.; Yuasa, Y.; Okumichi, H.; Tokumo, K.; Kawano, R.; Kiuchi, Y. Determinants of corneal endothelial cell loss after sulcus placement of Ahmed and Baerveldt drainage device surgery. Br. J. Ophthalmol. 2021, 105, 925–928. [Google Scholar] [CrossRef]
- Jabs, D.A.; Nussenblatt, R.B.; Rosenbaum, J.T. Standardization of uveitis nomenclature for reporting clinical data. Results of the first international workshop. Am. J. Ophthalmol. 2005, 140, 509–516. [Google Scholar] [CrossRef]
- Mochizuki, M.; Smith, J.R.; Takase, H.; Kaburaki, T.; Acharya, N.R.; Rao, N.A. Revised criteria of International Workshop on Ocular Sarcoidosis (IWOS) for the diagnosis of ocular sarcoidosis. Br. J. Ophthalmol. 2019, 103, 1418–1422. [Google Scholar] [CrossRef]
- Read, R.W.; Holland, G.N.; Rao, N.A.; Tabbara, K.F.; Ohno, S.; Arellanes-Garcia, L.; Pivetti-Pezzi, P.; Tessler, H.H.; Usui, M. Revised Diagnostic Criteria for Vogt-Koyanagi-Harada Disease: Report of an International Committee on Nomenclature. Am. J. Ophthalmol. 2001, 131, 647–652. [Google Scholar] [CrossRef]
- Chu, X.K.; Chan, C.C. Sympathetic ophthalmia: To the twenty-first century and beyond. J. Ophthalmic Inflamm. Infect. 2013, 3, 49. [Google Scholar] [CrossRef]
- Jabs, D.A.; Brezin, A.P.; Levinson, R.D.; McCluskey, P.; Oden, N.; Palestine, A.G.; Read, R.W.; Thorne, J.E.; Trusko, B.E.; Vitale, A.; et al. Classification Criteria for Multifocal Choroiditis with Panuveitis. Am. J. Ophthalmol. 2021, 228, 152–158. [Google Scholar] [CrossRef]
- Abu El-Asrar, A.M.; Herbort, C.P.; Tabbara, K.F. Retinal vasculitis. Ocul. Immunol. Inflamm. 2005, 13, 415–433. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, T.G.; Zacharopoulos, I.P.; Pasquale, L.R.; Christen, W.B.; Netland, P.A.; Foster, C.S. Long-term Results of Ahmed Glaucoma Valve Implantation for Uveitic Glaucoma. Am. J. Ophthalmol. 2007, 144, 62–69.e2. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kim, Y.H.; Kim, K.E.; Ahn, J. Comparison of Surgical Outcomes between Trabeculectomy with Mitomycin C and Ahmed Valve Implantation with Mitomycin C in Eyes with Uveitic Glaucoma. J. Clin. Med. 2022, 11, 1368. [Google Scholar] [CrossRef]
- Bettis, D.I.; Morshedi, R.G.; Chaya, C.; Goldsmith, J.; Crandall, A.; Zabriskie, N. Trabeculectomy with mitomycin c or ahmed valve implantation in eyes with uveitic glaucoma. J. Glaucoma. 2015, 24, 591–599. [Google Scholar] [CrossRef]
- Gedde, S.J.; Schiffman, J.C.; Feuer, W.J.; Herndon, L.W.; Brandt, J.D.; Budenz, D.L. Treatment outcomes in the tube versus trabeculectomy (TVT) study after five years of follow-up. Am. J. Ophthalmol. 2012, 153, 789–803.e2. [Google Scholar] [CrossRef] [Green Version]
- Laule, A.; Cable, M.K.; Hoffman, C.E.; Hanna, C. Endothelial Cell Population Changes of Human Cornea During Life. Arch. Ophthalmol. 1978, 96, 2031–2035. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, K.N.; Kim, C.S. Changes in Corneal Endothelial Cell after Ahmed Glaucoma Valve Implantation and Trabeculectomy: 1-Year Follow-up. Korean J. Ophthalmol. 2016, 30, 416–425. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Liu, Y.; Thanapaisal, S.; Oatts, J.; Luo, Y.; Ying, G.-S.; Wang, J.; McLeod, S.D.; Gedde, S.J.; Han, Y. The Effect of Tube Location on Corneal Endothelial Cells in Patients with Ahmed Glaucoma Valve. Ophthalmology 2021, 128, 218–226. [Google Scholar] [CrossRef]
- Kim, J.Y.; Lee, J.S.; Lee, T.; Seo, D.; Choi, W.; Bae, H.W.; Kim, C.Y. Corneal endothelial cell changes and surgical results after Ahmed glaucoma valve implantation: Ciliary sulcus versus anterior chamber tube placement. Sci. Rep. 2021, 11, 12986. [Google Scholar] [CrossRef]
- Godinho, G.; Barbosa-Breda, J.; Oliveira-Ferreira, C.; Madeira, C.; Melo, A.; Falcão-Reis, F.; Estrela-Silva, S. Anterior Chamber Versus Ciliary Sulcus Ahmed Glaucoma Valve Tube Placement: Longitudinal Evaluation of Corneal Endothelial Cell Profiles. J. Glaucoma. 2021, 30, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Harada, Y.; Fukuda, K.; Nakahira, A.; Tada, K.; Sumi, T.; Fukushima, A. Requirement of longer term antiviral therapy in patients with cytomegalovirus anterior uveitis with corneal endothelial cell damage. Clin. Ophthalmol. 2018, 12, 1311–1316. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients (n) | 27 |
| Eye (n) | 27 |
| Age (y) | 67.4 ± 11.8 |
| Age at uveitis diagnosis (y) | 56.0 ± 17.5 |
| Follow up period until surgery (y) | 11.4 ± 13.9 |
| Gender (M/F) | 14/13 |
| Type of noninfectious uvea n. (%) | |
| Retinal vasculitis | 5(18.5%) |
| Multifocal choroiditis | 3 (11.1%) |
| Chronic iridocyclitis | 10 (37.0%) |
| Sarcoidosis | 4 (14.8%) |
| Vogt–Koyanagi–Harada disease | 3 (11.1%) |
| Fuchs iridocyclitis | 1 (3.7%) |
| Sympathetic ophthalmia | 1 (3.7%) |
| Anterior uveitis n. (%) | 11 (40.7%) |
| Bilateral/unilateral | 21/6 |
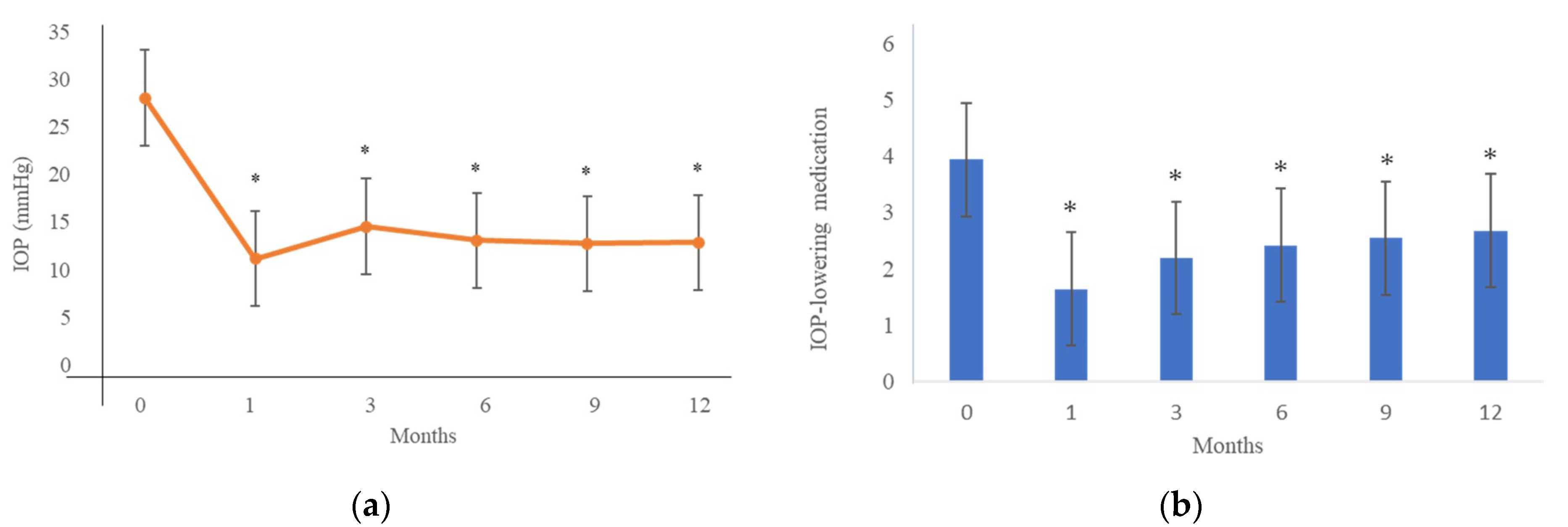
| Preoperative IOP (mmHg) | 28.7 ± 9.6 |
| Preoperative IOP-lowering medications (n) | 3.9 ± 0.7 |
| Preoperative intraocular surgeries (n) | |
| None | 3 |
| Cataract | 24 |
| Glaucoma surgery | 9 |
| Vitrectomy | 7 |
| Preoperative CECD (cells/mm2) | 2431.4 ± 367.5 |
| Preoperative central cornea thickness (μm) | 494.0 ± 32.8 |
| Preoperative number of relapses per year | 0.9 ± 0.9 |
| Preoperative flare measurement (ph/ms) | 30.8 ± 11.8 |
| Follow-Up Period | N | CECD (cells/mm2) | Reduction (%) * | p Value a |
|---|---|---|---|---|
| Baseline | 27 | 2431.4 ± 367.5 | ||
| 3 months | 22 | 2307.7 ± 391.0 | 3.69 ± 13.67 | 0.119 |
| 6 months | 26 | 2322.3 ± 378.7 | 4.28 ± 10.15 | 0.059 |
| 9 months | 22 | 2306.4 ± 365.1 | 3.26 ± 10.93 | 0.103 |
| 12 months | 27 | 2360.5 ± 391.3 | 2.73 ± 9.29 | 0.074 |
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| Factors | β | SE(β) | p Value | β | SE(β) | p Value | |
| Age | −0.060 | 0.104 | 0.565 | ||||
| Gender (Female) | 0.411 | 1.221 | 0.738 | ||||
| Type of uveitis | |||||||
| Retinal vasculitis | −2.377 | 2.910 | 0.423 | ||||
| Multifocal choroiditis | 1.862 | 3.513 | 0.601 | ||||
| Chronic iridocyclitis | −0.596 | 2.360 | 0.803 | ||||
| Sarcoidosis | −2.030 | 3.150 | 0.526 | ||||
| Vogt–Koyanagi–Harada disease | −1.729 | 3.513 | 0.627 | ||||
| Anterior uveitis | −1.002 | 1.228 | 0.421 | ||||
| Unilateral | 3.896 | 1.247 | 0.004 | −7.130 | 2.603 | 0.011 | |
| Age at uveitis diagnosis | 0.055 | 0.069 | 0.431 | ||||
| Follow up period until surgery | −0.129 | 0.085 | 0.143 | −0.090 | 0.078 | 0.259 | |
| Preoperative intraocular surgery | −0.728 | 1.331 | 0.589 | ||||
| Preoperative trabeculectomy | 0.972 | 1.282 | 0.455 | ||||
| Combined with cataract surgery | −0.223 | 1.445 | 0.878 | ||||
| Preoperative laser flare | 0.011 | 0.042 | 0.791 | ||||
| Improvement of ocular inflammation | −1.357 | 1.260 | 0.291 | ||||
| Preoperative IOP | 0.076 | 0.128 | 0.557 | ||||
| Preoperative CECD | 0.001 | 0.003 | 0.803 | ||||
| Preoperative IOP-lowering medications | 1.107 | 1.751 | 0.532 | ||||
| Anterior chamber depth | −4.801 | 3.450 | 0.177 | ||||
| Follow-Up Period | Unilateral (n = 6) | P a | Bilateral (n = 25) | P b | P c | ||
|---|---|---|---|---|---|---|---|
| CECD (cells/mm2) | Reduction (%)* | CECD (cells/mm2) | Reduction (%)* | ||||
| Baseline | 2467.6 ± 363.7 | 2421.1 ± 522.5 | |||||
| 6 months | 2084.4 ± 244.1 | 14.89 ± 9.62 | 0.021 | 2393.7 ± 387.1 | 1.10 ± 8.06 | 0.460 | 0.001 |
| 12 months | 2198.5 ± 397.1 | 11.02 ± 7.19 | 0.012 | 2406.9 ± 386.7 | 3.70 ± 8.53 | 0.745 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komatsu, K.; Harada, Y.; Hiyama, T.; Sada, I.; Hirooka, K.; Kiuchi, Y. Corneal Endothelial Cell Loss after Ciliary Sulcus Placement of Ahmed Glaucoma Valve in Patients with Noninfectious Uveitic Glaucoma. J. Pers. Med. 2022, 12, 2075. https://doi.org/10.3390/jpm12122075
Komatsu K, Harada Y, Hiyama T, Sada I, Hirooka K, Kiuchi Y. Corneal Endothelial Cell Loss after Ciliary Sulcus Placement of Ahmed Glaucoma Valve in Patients with Noninfectious Uveitic Glaucoma. Journal of Personalized Medicine. 2022; 12(12):2075. https://doi.org/10.3390/jpm12122075
Chicago/Turabian StyleKomatsu, Kaori, Yosuke Harada, Tomona Hiyama, Ikuyo Sada, Kazuyuki Hirooka, and Yoshiaki Kiuchi. 2022. "Corneal Endothelial Cell Loss after Ciliary Sulcus Placement of Ahmed Glaucoma Valve in Patients with Noninfectious Uveitic Glaucoma" Journal of Personalized Medicine 12, no. 12: 2075. https://doi.org/10.3390/jpm12122075