
Role of Catechol-O-methyltransferase Val158Met Polymorphism on Transcranial Direct Current Stimulation in Swallowing

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
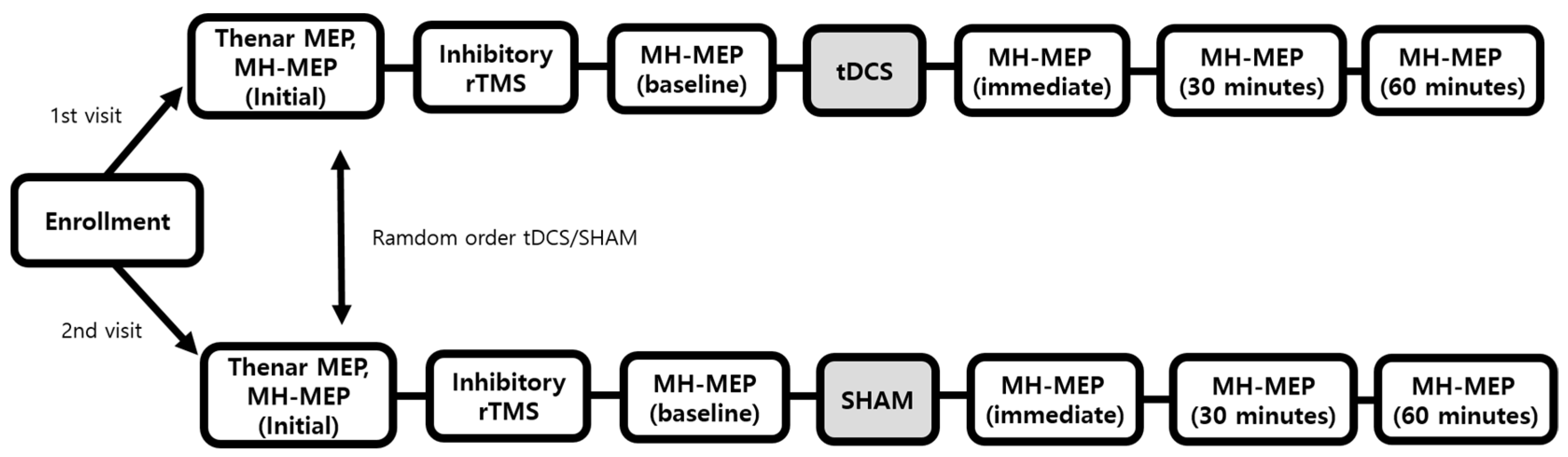
2.1. Participants and Study Design
2.2. DNA Sampling and Genotyping
2.3. Motor-Evoked Potential and Cortical Excitability
2.4. Inhibitory Repetitive Transcranial Magnetic Stimulation
2.5. Transcranial Direct Current Stimulation
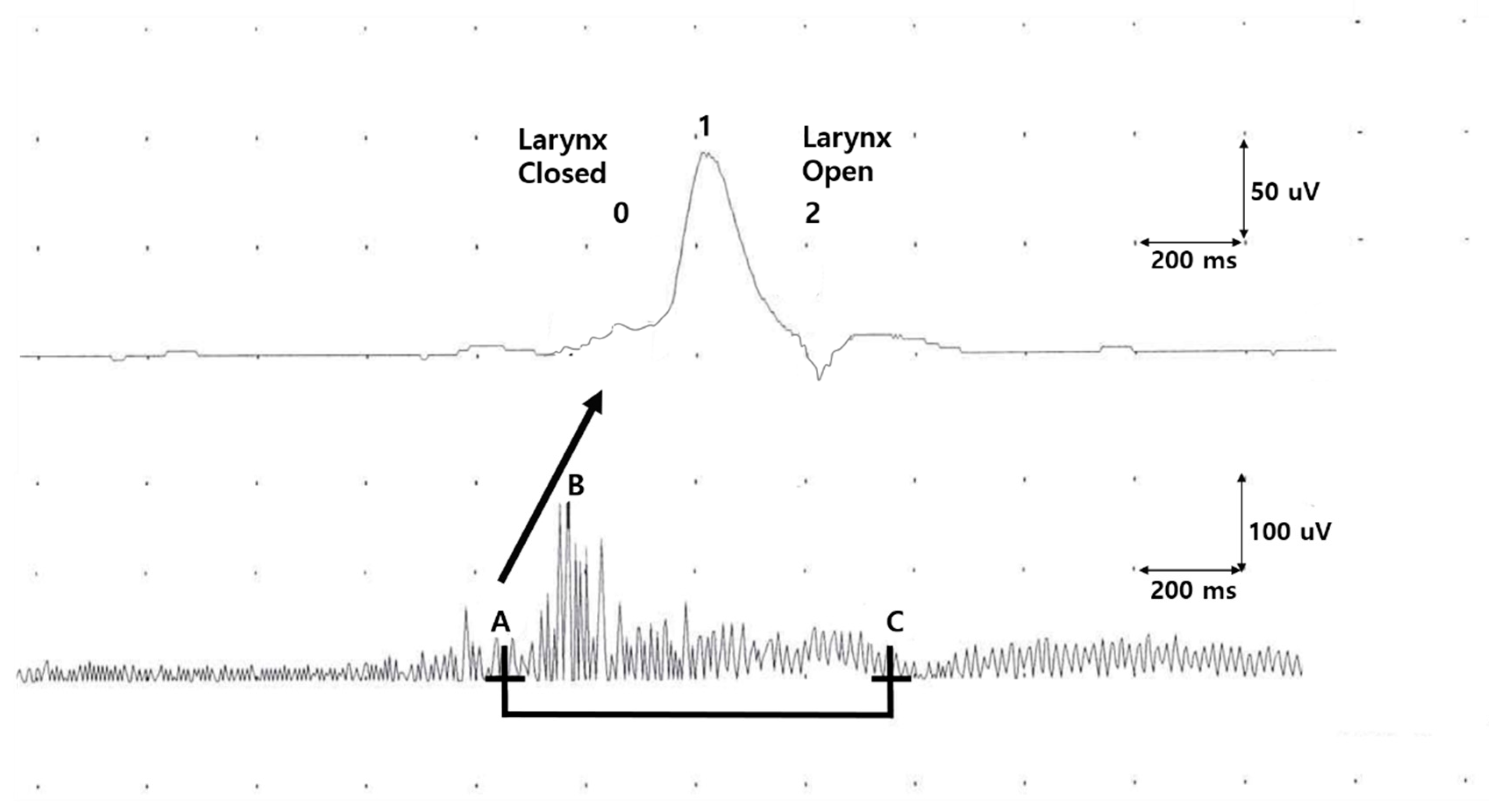
2.6. Electrophyioslogical Evaluation of Oropharyngeal Swallowing Function
2.7. Statistical Analysis
3. Results
3.1. Assessments at the Enrollment
3.2. Post-Inhibitory rTMS (Baseline Assessment)
3.3. Dysphagia Reversal, tDCS Versus Sham Session
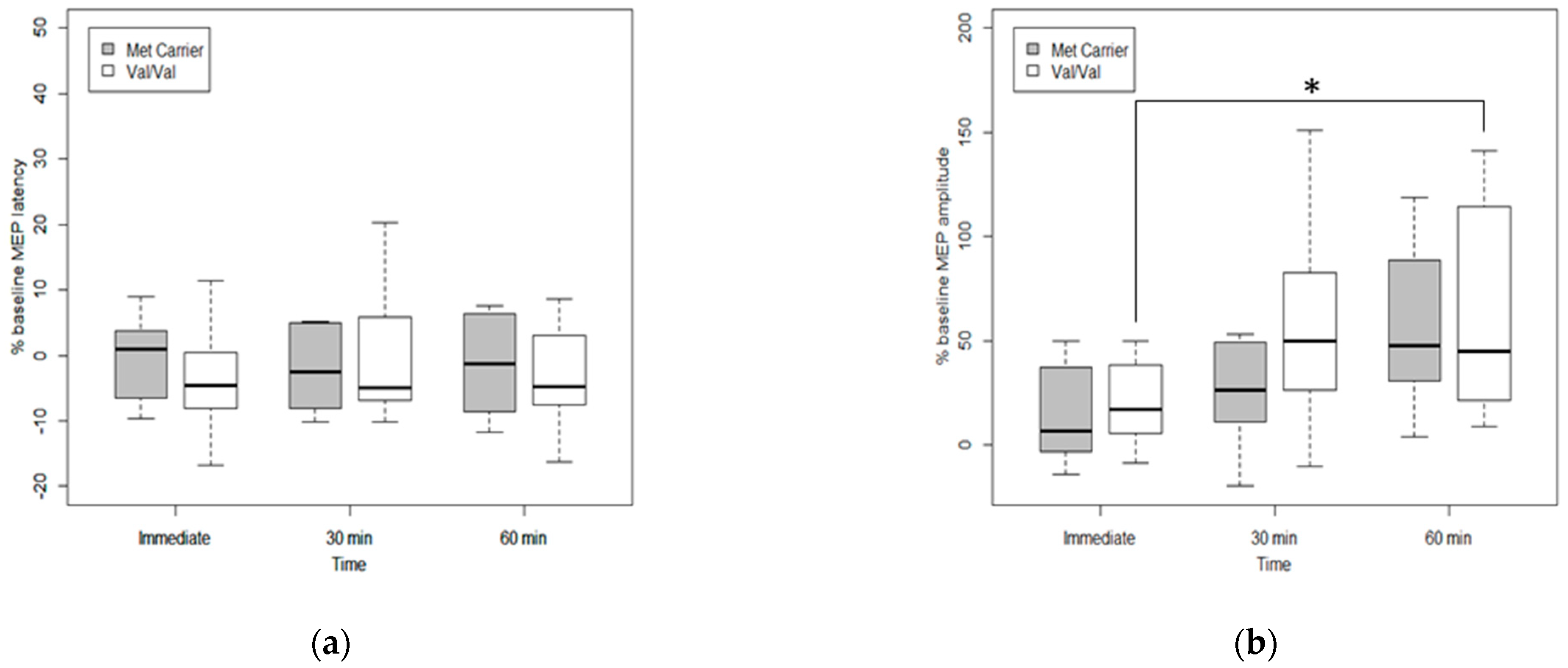
3.4. Effects of Genetic Polymorphism on Cortical Excitability after tDCS
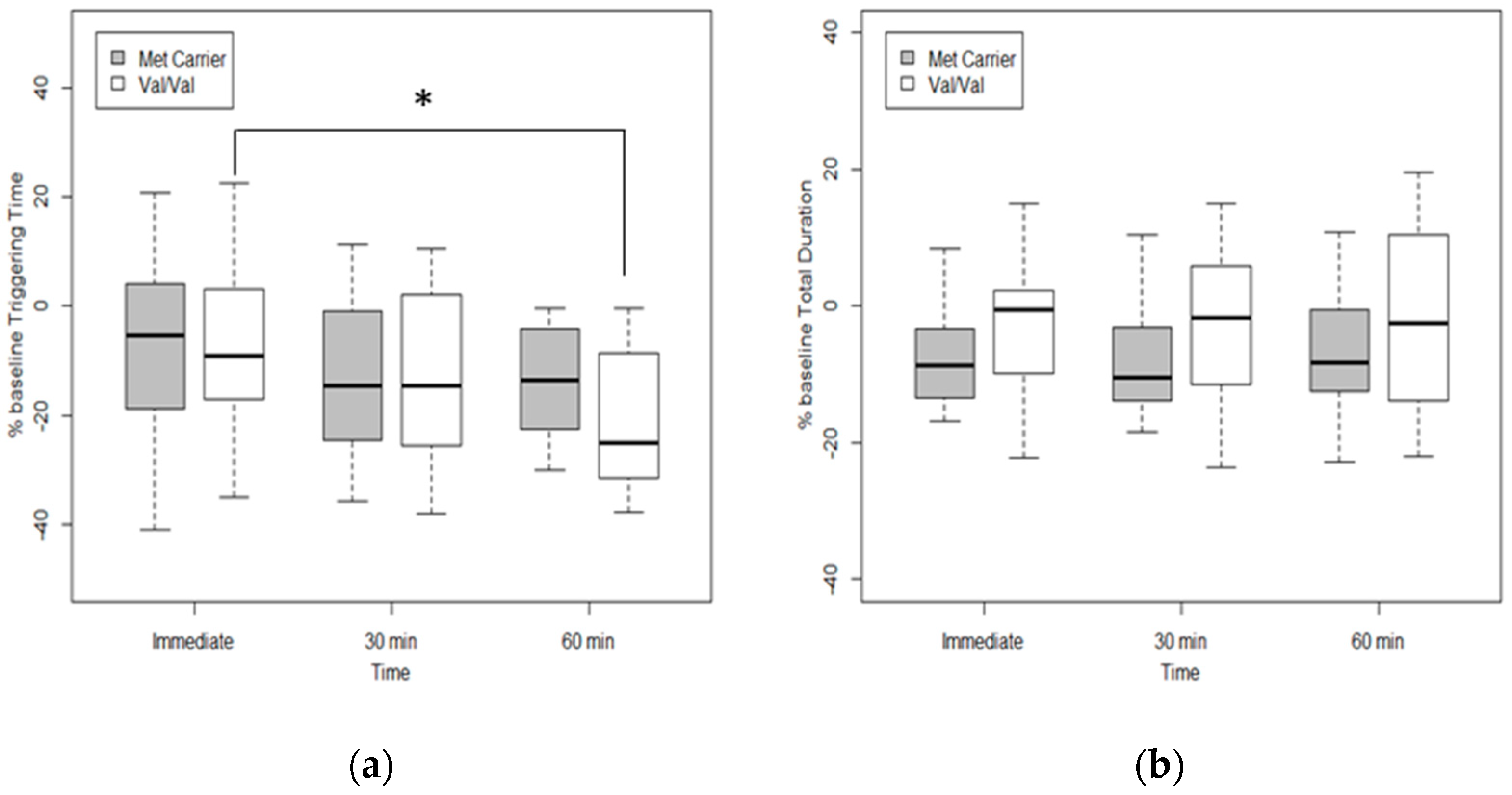
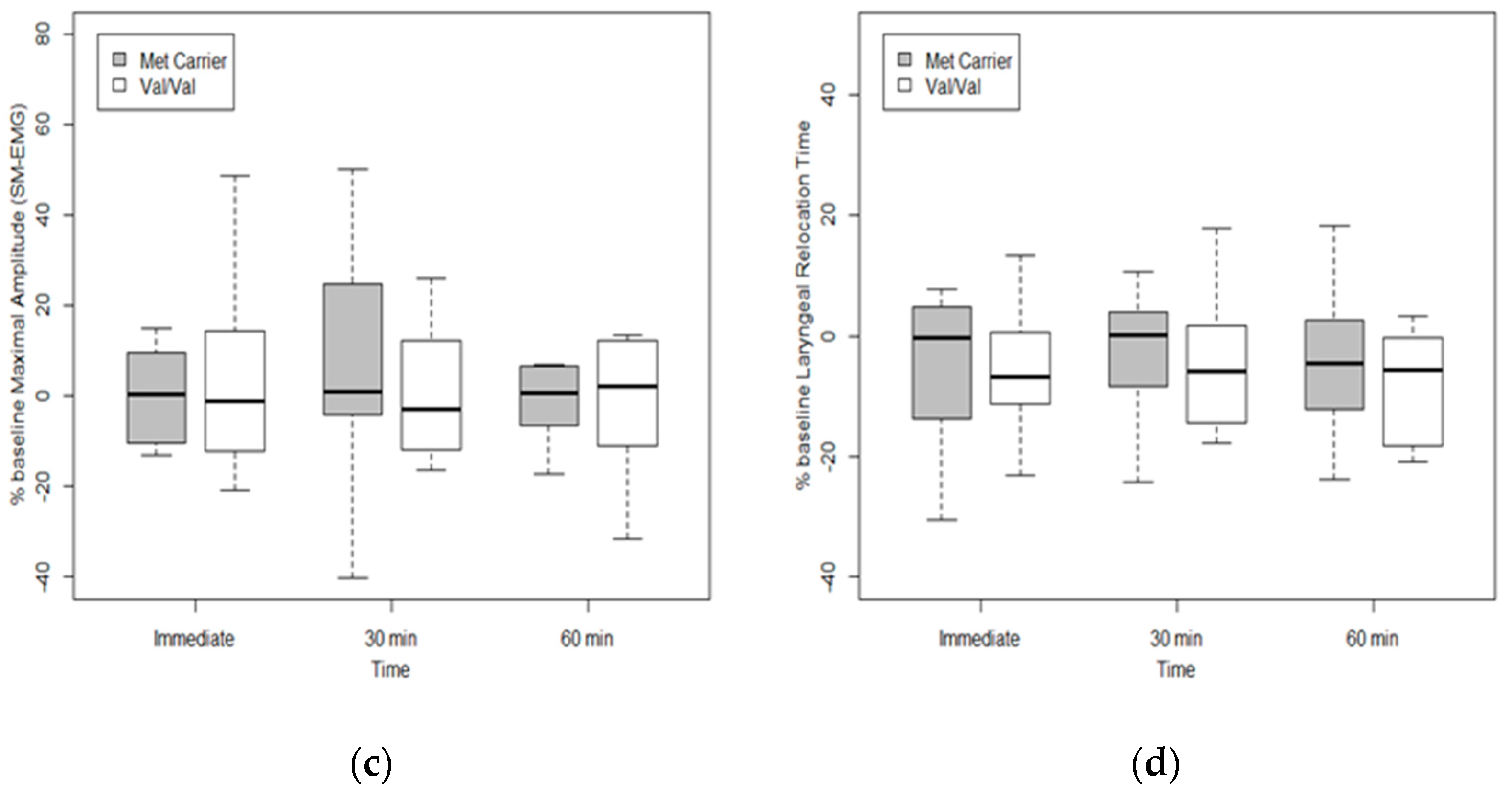
3.5. Effects of Genetic Polymorphism on Swallowing Function after tDCS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| tDCS | Transcranial direct current stimulation |
| rTMS | Repetitive transcranial magnetic stimulation |
| SNP | Single nucleotide polymorphism |
| COMT | Catechol-O-methyltransferase |
| BDNF | Brain-derived neurotrophic factor |
| MEP | Motor-evoked potential |
| rMT | Resting motor threshold |
| MH-MEP | Mylohyoid MEP |
| SM-EMG | Submental-electromyography |
References
- Martino, R.; Foley, N.; Bhogal, S.; Diamant, N.; Speechley, M.; Teasell, R. Dysphagia after stroke: Incidence, diagnosis, and pulmonary complications. Stroke 2005, 36, 2756–2763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cichero, J.A.; Lam, P.; Steele, C.M.; Hanson, B.; Chen, J.; Dantas, R.O.; Duivestein, J.; Kayashita, J.; Lecko, C.; Murray, J.; et al. Development of International Terminology and Definitions for Texture-Modified Foods and Thickened Fluids Used in Dysphagia Management: The IDDSI Framework. Dysphagia 2017, 32, 293–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.S.; Oh, D.H.; Hwang, N.K.; Lee, J.H. Effects of neuromuscular electrical stimulation combined with effortful swallowing on post-stroke oropharyngeal dysphagia: A randomised controlled trial. J. Oral Rehabil. 2016, 43, 426–434. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Lazzaro, V.D.; Filipović, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.-P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; Ridder, D.D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.L.; Roffe, C.; Beavan, J.; Blackett, B.; Fairfield, C.A.; Hamdy, S.; Havard, D.; McFarlane, M.; McLauglin, C.; Randall, M.; et al. Post-stroke dysphagia: A review and design considerations for future trials. Int. J. Stroke 2016, 11, 399–411. [Google Scholar] [CrossRef]
- Simons, A.; Hamdy, S. The Use of Brain Stimulation in Dysphagia Management. Dysphagia 2017, 32, 209–215. [Google Scholar] [CrossRef]
- Zhong, L.; Rao, J.; Wang, J.; Li, F.; Peng, Y.; Liu, H.; Zhang, Y.; Wang, P. Repetitive transcranial magnetic stimulation at different sites for dysphagia after stroke: A randomized, observer-blind clinical trial. Front. Neurol. 2021, 12, 625683. [Google Scholar] [CrossRef]
- Hamdy, S.; Aziz, Q.; Rothwell, J.C.; Singh, K.D.; Barlow, J.; Hughes, D.G.; Tallis, R.C.; Thompson, D.G. The cortical topography of human swallowing musculature in health and disease. Nat. Med. 1996, 2, 1217–1224. [Google Scholar] [CrossRef]
- Lin, Q.; Lin, S.-F.; Ke, X.-H.; Jia, X.-F.; Huang, D.-B. A systematic review and meta-analysis on the effectiveness of transcranial direct current stimulation (tDCS) on swallowing function of post-stroke patients. Am. J. Phys. Med. Rehabil. 2021. publish ahead of print. [Google Scholar] [CrossRef]
- Rudroff, T.; Workman, C.D.; Fietsam, A.C.; Kamholz, J. Response variability in transcranial direct current stimulation: Why sex matters. Front. Psychiatry 2020, 11, 585. [Google Scholar] [CrossRef] [PubMed]
- Wiethoff, S.; Hamada, M.; Rothwell, J.C. Variability in response to transcranial direct current stimulation of the motor cortex. Brain Stimul. 2014, 7, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Hayek, D.; Antonenko, D.; Witte, A.V.; Lehnerer, S.M.; Meinzer, M.; Külzow, N.; Prehn, K.; Rujescu, D.; Schneider, A.; Grittner, U.; et al. Impact of COMT val158met on tDCS-induced cognitive enhancement in older adults. Behav. Brain Res. 2021, 401, 113081. [Google Scholar] [CrossRef]
- McClintock, S.M.; Martin, D.M.; Lisanby, S.H.; Alonzo, A.; McDonald, W.M.; Aaronson, S.T.; Husain, M.M.; O’Reardon, J.P.; Weickert, C.S.; Mohan, A.; et al. Neurocognitive effects of transcranial direct current stimulation (tDCS) in unipolar and bipolar depression: Findings from an international randomized controlled trial. Depress. Anxiety 2020, 37, 261–272. [Google Scholar] [CrossRef]
- Kim, D.Y.; Quinlan, E.B.; Gramer, R.; Cramer, S.C. BDNF Val66Met polymorphism is Related to motor system function after stroke. Phys. Ther. 2016, 96, 533–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, S.C.; Procaccio, V.; Americas, G.; Investigators, G.I.S. Correlation between genetic polymorphisms and stroke recovery: Analysis of the GAIN Americas and GAIN International Studies. Eur. J. Neurol. 2012, 19, 718–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, H.M.; Kim, T.W.; Park, H.Y.; Kim, Y.; Park, G.Y.; Im, S. Role of rs6265 BDNF polymorphisms and post-stroke dysphagia recovery-A prospective cohort study. Neurogastroenterol. Motil. 2021, 33, e13953. [Google Scholar] [CrossRef]
- Chang, W.H.; Bang, O.Y.; Shin, Y.I.; Lee, A.; Pascual-Leone, A.; Kim, Y.H. BDNF polymorphism and differential rTMS effects on motor recovery of stroke patients. Brain Stimul. 2014, 7, 553–558. [Google Scholar] [CrossRef]
- Jayasekeran, V.; Pendleton, N.; Holland, G.; Payton, A.; Jefferson, S.; Michou, E.; Vasant, D.; Ollier, B.; Horan, M.; Rothwell, J.; et al. Val66Met in brain-derived neurotrophic factor affects stimulus-induced plasticity in the human pharyngeal motor cortex. Gastroenterology 2011, 141, 827–836.e3. [Google Scholar] [CrossRef]
- Fridriksson, J.; Elm, J.; Stark, B.C.; Basilakos, A.; Rorden, C.; Sen, S.; George, M.S.; Gottfried, M.; Bonilha, L. BDNF genotype and tDCS interaction in aphasia treatment. Brain Stimul. 2018, 11, 1276–1281. [Google Scholar] [CrossRef] [Green Version]
- Cocco, S.; Podda, M.V.; Grassi, C. Role of BDNF Signaling in Memory Enhancement Induced by Transcranial Direct Current Stimulation. Front. Neurosci. 2018, 12, 427. [Google Scholar] [CrossRef] [PubMed]
- McAllister, T.W. Polymorphisms in genes modulating the dopamine system: Do they influence outcome and response to medication after traumatic brain injury? J. Head Trauma Rehabil. 2009, 24, 65–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baetu, I.; Burns, N.R.; Urry, K.; Barbante, G.G.; Pitcher, J.B. Commonly-occurring polymorphisms in the COMT, DRD1 and DRD2 genes influence different aspects of motor sequence learning in humans. Neurobiol. Learn. Mem. 2015, 125, 176–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.R.; Kim, H.Y.; Chun, Y.I.; Yun, Y.M.; Kim, H.; Choi, D.H.; Lee, J. Association between genetic variation in the dopamine system and motor recovery after stroke. Restor. Neurol. Neurosci. 2016, 34, 925–934. [Google Scholar] [CrossRef]
- Nimmons, D.; Pendleton, N.; Payton, A.; Ollier, W.; Horan, M.; Wilkinson, J.; Hamdy, S. A novel association between COMT and BDNF gene polymorphisms and likelihood of symptomatic dysphagia in older people. Neurogastroenterol. Motil. 2015, 27, 1223–1231. [Google Scholar] [CrossRef]
- Park, H.Y.; Kim, Y.; Oh, H.M.; Kim, T.W.; Park, G.Y.; Im, S. Potential prognostic impact of dopamine receptor D1 (rs4532) polymorphism in post-stroke outcome in the elderly. Front. Neurol. 2021, 12, 675060. [Google Scholar] [CrossRef]
- Koshiishi, T.; Koinuma, M.; Takagi, A.; Nakamura, H. Pharmacological considerations in antipsychotic drug selection for prevention of drug-induced dysphagia. Pharmazie 2020, 75, 595–598. [Google Scholar] [CrossRef]
- O’Neill, J.L.; Remington, T.L. Drug-induced esophageal injuries and dysphagia. Ann. Pharmacother. 2003, 37, 1675–1684. [Google Scholar] [CrossRef]
- Lim, J.; Ebstein, R.; Tse, C.Y.; Monakhov, M.; Lai, P.S.; Dinges, D.F.; Kwok, K. Dopaminergic polymorphisms associated with time-on-task declines and fatigue in the Psychomotor Vigilance Test. PLoS ONE 2012, 7, e33767. [Google Scholar] [CrossRef]
- Plewnia, C.; Zwissler, B.; Längst, I.; Maurer, B.; Giel, K.; Krüger, R. Effects of transcranial direct current stimulation (tDCS) on executive functions: Influence of COMT Val/Met polymorphism. Cortex 2013, 49, 1801–1807. [Google Scholar] [CrossRef]
- Shivakumar, V.; Chhabra, H.; Subbanna, M.; Agarwal, S.M.; Bose, A.; Kalmady, S.V.; Narayanaswamy, J.C.; Debnath, M.; Venkatasubramanian, G. Effect of tDCS on auditory hallucinations in schizophrenia: Influence of catechol-O-methyltransferase (COMT) Val158Met polymorphism. Asian J. Psychiatr. 2015, 16, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Stephens, J.A.; Jones, K.T.; Berryhill, M.E. Task demands, tDCS intensity, and the COMT val(158)met polymorphism impact tDCS-linked working memory training gains. Sci. Rep. 2017, 7, 13463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, W.; Huang, L.; Li, Y.; Zhang, Q.; Chen, X.; Fu, W.; Du, B.; Deng, X.; Ji, F.; Xiang, Y.T.; et al. Evidence for the contribution of COMT gene Val158/108Met polymorphism (rs4680) to working memory training-related prefrontal plasticity. Brain Behav. 2020, 10, e01523. [Google Scholar] [CrossRef]
- Rossini, P.M.; Barker, A.T.; Berardelli, A.; Caramia, M.D.; Caruso, G.; Cracco, R.Q.; Dimitrijević, M.R.; Hallett, M.; Katayama, Y.; Lücking, C.H.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord and roots: Basic principles and procedures for routine clinical application. Report of an IFCN committee. Electroencephalogr. Clin. Neurophysiol. 1994, 91, 79–92. [Google Scholar] [CrossRef]
- Gallas, S.; Moirot, P.; Debono, G.; Navarre, I.; Denis, P.; Marie, J.P.; Verin, E. Mylohyoid motor-evoked potentials relate to swallowing function after chronic stroke dysphagia. Neurogastroenterol. Motil. 2007, 19, 453–458. [Google Scholar] [CrossRef]
- Suntrup-Krueger, S.; Ringmaier, C.; Muhle, P.; Wollbrink, A.; Kemmling, A.; Hanning, U.; Claus, I.; Warnecke, T.; Teismann, I.; Pantev, C.; et al. Randomized trial of transcranial direct current stimulation for poststroke dysphagia. Ann. Neurol. 2018, 83, 328–340. [Google Scholar] [CrossRef]
- Vasant, D.H.; Mistry, S.; Michou, E.; Jefferson, S.; Rothwell, J.C.; Hamdy, S. Transcranial direct current stimulation reverses neurophysiological and behavioural effects of focal inhibition of human pharyngeal motor cortex on swallowing. J. Physiol. 2014, 592, 695–709. [Google Scholar] [CrossRef]
- Jefferson, S.; Mistry, S.; Singh, S.; Rothwell, J.; Hamdy, S. Characterizing the application of transcranial direct current stimulation in human pharyngeal motor cortex. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 297, G1035–G1040. [Google Scholar] [CrossRef] [Green Version]
- Gandiga, P.C.; Hummel, F.C.; Cohen, L.G. Transcranial DC stimulation (tDCS): A tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 2006, 117, 845–850. [Google Scholar] [CrossRef]
- Ertekin, C. Electrophysiological evaluation of oropharyngeal Dysphagia in Parkinson’s disease. J. Mov. Disord. 2014, 7, 31–56. [Google Scholar] [CrossRef]
- Ertekin, C.; Tarlaci, S.; Aydogdu, I.; Kiylioglu, N.; Yuceyar, N.; Turman, A.B.; Secil, Y.; Esmeli, F. Electrophysiological evaluation of pharyngeal phase of swallowing in patients with Parkinson’s disease. Mov. Disord. 2002, 17, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Ertekin, C.; Yüceyar, N.; Aydoğdu, I.; Karasoy, H. Electrophysiological evaluation of oropharyngeal swallowing in myotonic dystrophy. J. Neurol. Neurosurg. Psychiatry 2001, 70, 363–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayasekeran, V.; Singh, S.; Tyrrell, P.; Michou, E.; Jefferson, S.; Mistry, S.; Gamble, E.; Rothwell, J.; Thompson, D.; Hamdy, S. Adjunctive functional pharyngeal electrical stimulation reverses swallowing disability after brain lesions. Gastroenterology 2010, 138, 1737–1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michou, E.; Mistry, S.; Jefferson, S.; Singh, S.; Rothwell, J.; Hamdy, S. Targeting unlesioned pharyngeal motor cortex improves swallowing in healthy individuals and after dysphagic stroke. Gastroenterology 2012, 142, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Dou, Z.; Wei, X.; Li, J.; Dai, M.; Wang, Y.; Yang, Q.; He, H. Task-concurrent anodal tDCS modulates bilateral plasticity in the human suprahyoid motor cortex. Front. Hum. Neurosci. 2015, 9, 370. [Google Scholar] [CrossRef] [Green Version]
- Ertekin, C.; Aydogdu, I.; Yuceyar, N.; Tarlaci, S.; Kiylioglu, N.; Pehlivan, M.; Celebi, G. Electrodiagnostic methods for neurogenic dysphagia. Electroencephalogr. Clin. Neurophysiol. 1998, 109, 331–340. [Google Scholar] [CrossRef]
- Campbell, D.; Bick, J.; Yrigollen, C.M.; Lee, M.; Joseph, A.; Chang, J.T.; Grigorenko, E.L.; Learning Disabilities Project Zambia. Schooling and variation in the COMT gene: The devil is in the details. J. Child Psychol. Psychiatry 2013, 54, 1056–1065. [Google Scholar] [CrossRef]
- Nolan, K.A.; Bilder, R.M.; Lachman, H.M.; Volavka, J. Catechol O-methyltransferase Val158Met polymorphism in schizophrenia: Differential effects of Val and Met alleles on cognitive stability and flexibility. Am. J. Psychiatry 2004, 161, 359–361. [Google Scholar] [CrossRef] [Green Version]
- Lotta, T.; Vidgren, J.; Tilgmann, C.; Ulmanen, I.; Melén, K.; Julkunen, I.; Taskinen, J. Kinetics of human soluble and membrane-bound catechol O-methyltransferase: A revised mechanism and description of the thermolabile variant of the enzyme. Biochemistry 1995, 34, 4202–4210. [Google Scholar] [CrossRef]
- Ren, J.; Wu, Y.D.; Chan, J.S.; Yan, J.H. Cognitive aging affects motor performance and learning. Geriatr. Gerontol. Int. 2013, 13, 19–27. [Google Scholar] [CrossRef]
- Liepert, J.; Heller, A.; Behnisch, G.; Schoenfeld, A. Catechol-O-methyltransferase polymorphism influences outcome after ischemic stroke: A prospective double-blind study. Neurorehabil. Neural. Repair 2013, 27, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Arnsten, A.F.T. Catecholamine modulation of prefrontal cortical cognitive function. Trends Cogn. Sci. 1998, 2, 436–447. [Google Scholar] [CrossRef]
- Lindenberger, U.; Nagel, I.E.; Chicherio, C.; Li, S.C.; Heekeren, H.R.; Backman, L. Age-related decline in brain resources modulates genetic effects on cognitive functioning. Front. Neurosci. 2008, 2, 234–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukai, M.; Bunai, T.; Hirosawa, T.; Kikuchi, M.; Ito, S.; Minabe, Y.; Ouchi, Y. Endogenous dopamine release under transcranial direct-current stimulation governs enhanced attention: A study with positron emission tomography. Transl. Psychiatry 2019, 9, 115. [Google Scholar] [CrossRef]
- Bilder, R.M.; Volavka, J.; Lachman, H.M.; Grace, A.A. The catechol-O-methyltransferase polymorphism: Relations to the tonic-phasic dopamine hypothesis and neuropsychiatric phenotypes. Neuropsychopharmacology 2004, 29, 1943–1961. [Google Scholar] [CrossRef] [Green Version]
- Rosa, E.C.; Dickinson, D.; Apud, J.; Weinberger, D.R.; Elvevåg, B. COMT Val158Met polymorphism, cognitive stability and cognitive flexibility: An experimental examination. Behav. Brain Funct. 2010, 6, 53. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Val/Val | Met Carriers | p-Value | |
|---|---|---|---|
| No. of subjects | 12 | 12 | |
| Male (%) | 7 (58.3%) | 6 (50.0%) | 1.000 |
| APB rMT (mV) | 20.4 ± 6.9 | 19.3 ± 3.2 | 0.628 |
| tDCS session | |||
| MH-MEP latency (ms) | 4.7 ± 0.3 | 5.5 ± 0.5 | 0.209 |
| MH-MEP amplitude (mV) | 89.6 ± 21.9 | 98.8 ± 29.1 | 0.843 |
| Triggering time (ms) | 392.1 ± 47.0 | 406.9 ± 40.4 | 0.814 |
| Total duration of SM-EMG (ms) | 914.8 ± 69.4 | 953.6 ± 93.1 | 0.742 |
| Maximal amplitude of SM-EMG (uV) | 104.4 ± 5.7 | 117.5 ± 19.1 | 0.977 |
| Laryngeal relocation time (ms) | 712.7 ± 35.6 | 708.9 ± 38.3 | 0.944 |
| Sham mode session | |||
| MH-MEP latency (ms) | 5.1 ± 0.3 | 5.7 ± 0.5 | 0.361 |
| MH-MEP amplitude (mV) | 89.5 ± 24.6 | 119.6 ± 30.0 | 0.478 |
| Triggering time (ms) | 391.6 ± 46.1 | 406.9 ± 40.4 | 0.805 |
| Total duration of SM-EMG (ms) | 915.6 ± 70.3 | 953.6 ± 93.1 | 0.748 |
| Maximal amplitude of SM-EMG (uV) | 103.9 ± 5.5 | 117.5 ± 19.1 | 0.977 |
| Laryngeal relocation time (ms) | 716.0 ± 35.1 | 708.9 ± 38.3 | 0.893 |
| Baseline | 60 min | p-Value (Baseline vs. 60 min) | p-Value (tDCS vs. Sham Mode) | ||
|---|---|---|---|---|---|
| Cortical Excitability | |||||
| MH-MEP Latencies (ms) | tDCS | 5.4 ± 0.3 | 5.3 ± 0.3 | 0.415 | 0.855 |
| Sham | 5.6 ± 0.3 | 6.4 ± 0.9 | 0.376 | ||
| MH-MEP Amplitudes (mV) | tDCS | 80.9 ± 17.6 | 152.6 ± 32.1 | <0.001 * | 0.014 * |
| Sham | 71.1 ± 14.6 | 86.2 ± 14.5 | 0.007 * | ||
| Swallowing Function | |||||
| Triggering time (ms) | tDCS | 453.0 ± 32.7 | 367.3 ± 24.7 | <0.001 * | 0.002 * |
| Sham | 426.3 ± 23.0 | 441.1 ± 31.2 | 0.627 | ||
| Total duration of SM-EMG (ms) | tDCS | 1029.7 ± 62.0 | 992.4 ± 57.8 | 0.162 | 0.137 |
| Sham | 981.8 ± 58.5 | 981.6 ± 55.0 | 0.52 | ||
| Maximal amplitude of SM-EMG (uV) | tDCS | 110.7 ± 8.1 | 112.8 ± 10.8 | 0.617 | 0.440 |
| Sham | 95.9 ± 6.6 | 104.6 ± 8.5 | 0.648 | ||
| Laryngeal relocation time (ms) | tDCS | 813.0 ± 56.1 | 738.1 ± 44.1 | 0.032 * | 0.074 |
| Sham | 729.1 ± 30.1 | 741.6 ± 24.2 | 0.511 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, H.; Han, Y.; Park, G.-Y.; Lee, S.; Park, H.-Y.; Im, S. Role of Catechol-O-methyltransferase Val158Met Polymorphism on Transcranial Direct Current Stimulation in Swallowing. J. Pers. Med. 2022, 12, 488. https://doi.org/10.3390/jpm12030488
Hwang H, Han Y, Park G-Y, Lee S, Park H-Y, Im S. Role of Catechol-O-methyltransferase Val158Met Polymorphism on Transcranial Direct Current Stimulation in Swallowing. Journal of Personalized Medicine. 2022; 12(3):488. https://doi.org/10.3390/jpm12030488
Chicago/Turabian StyleHwang, Hyemi, Yeonjae Han, Geun-Young Park, Soohwan Lee, Hae-Yeon Park, and Sun Im. 2022. "Role of Catechol-O-methyltransferase Val158Met Polymorphism on Transcranial Direct Current Stimulation in Swallowing" Journal of Personalized Medicine 12, no. 3: 488. https://doi.org/10.3390/jpm12030488