
Influential Factors and Personalized Prediction Model of Acute Pain Trajectories after Surgery for Renal Cell Carcinoma


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Patient Selection
2.2. Anesthesia and Analgesia Management
2.3. Pain Assessment and Data Acquisition
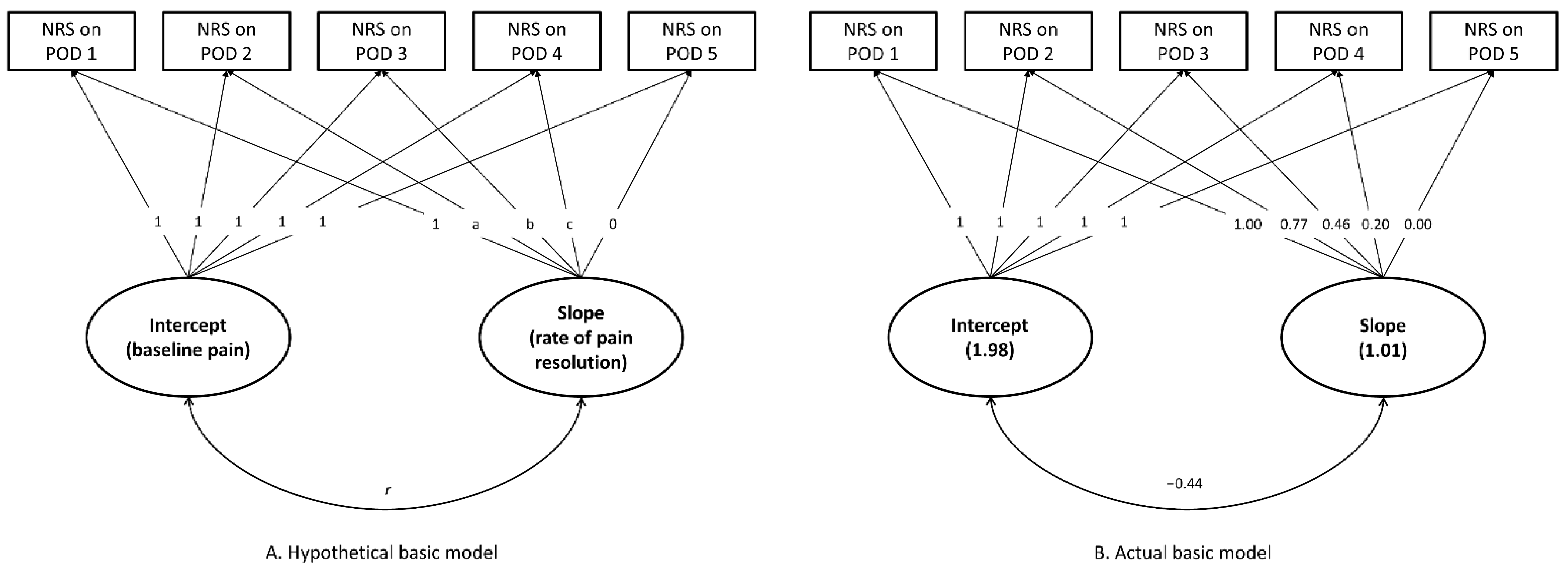
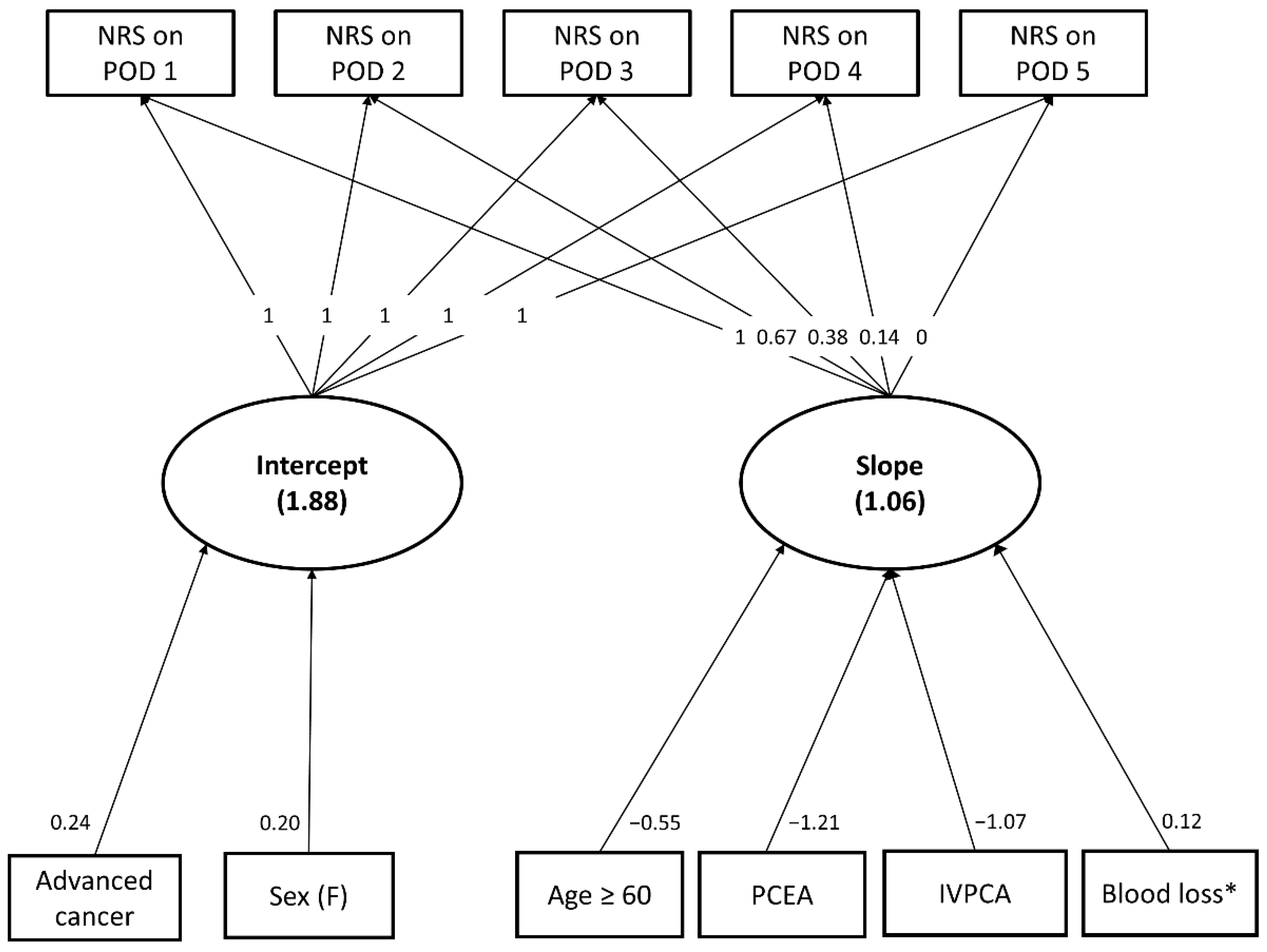
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hsieh, J.J.; Purdue, M.P.; Signoretti, S.; Swanton, C.; Albiges, L.; Schmidinger, M.; Heng, D.Y.; Larkin, J.; Ficarra, V. Renal cell carcinoma. Nat. Rev. Dis. Primers 2017, 3, 17009. [Google Scholar] [CrossRef]
- Nicholson, M.; Kaushik, M.; Lewis, G.; Brook, N.; Bagul, A.; Kay, M.; Harper, S.; Elwell, R.; Veitch, P. Randomized clinical trial of laparoscopic versus open donor nephrectomy. Br. J. Surg. 2010, 97, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Shahzad, M.M.; Lin, Y.G.; Armaiz-Pena, G.; Mangala, L.S.; Han, H.D.; Kim, H.S.; Nam, E.J.; Jennings, N.B.; Halder, J. Surgical stress promotes tumor growth in ovarian carcinoma. Clin. Cancer Res. 2009, 15, 2695–2702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cata, J.P.; Bauer, M.; Sokari, T.; Ramirez, M.F.; Mason, D.; Plautz, G.; Kurz, A. Effects of surgery, general anesthesia, and perioperative epidural analgesia on the immune function of patients with non-small cell lung cancer. J. Clin. Anesth. 2013, 25, 255–262. [Google Scholar] [CrossRef]
- Beattie, W.S.; Badner, N.H.; Choi, P.T. Meta-analysis demonstrates statistically significant reduction in postoperative myocardial infarction with the use of thoracic epidural analgesia. Anesth. Analg. 2003, 97, 919–920. [Google Scholar] [CrossRef]
- Pöpping, D.M.; Elia, N.; Marret, E.; Remy, C.; Tramer, M.R. Protective effects of epidural analgesia on pulmonary complications after abdominal and thoracic surgery: A meta-analysis. Arch. Surg. 2008, 143, 990–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, J.; Seltzer, Z. Transition from acute to chronic postsurgical pain: Risk factors and protective factors. Expert Rev. Neurother. 2009, 9, 723–744. [Google Scholar] [CrossRef] [Green Version]
- Joshi, G.P.; Ogunnaike, B.O. Consequences of inadequate postoperative pain relief and chronic persistent postoperative pain. Anesthesiol. Clin. N. Am. 2005, 23, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Peuckmann, V.; Ekholm, O.; Rasmussen, N.K.; Groenvold, M.; Christiansen, P.; Møller, S.; Eriksen, J.; Sjøgren, P. Chronic pain and other sequelae in long-term breast cancer survivors: Nationwide survey in Denmark. Eur. J. Pain 2009, 13, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Feddern, M.L.; Jensen, T.S.; Laurberg, S. Chronic pain in the pelvic area or lower extremities after rectal cancer treatment and its impact on quality of life: A population-based cross-sectional study. Pain 2015, 156, 1765–1771. [Google Scholar] [CrossRef]
- Hinrichs-Rocker, A.; Schulz, K.; Järvinen, I.; Lefering, R.; Simanski, C.; Neugebauer, E.A. Psychosocial predictors and correlates for chronic post-surgical pain (CPSP)–a systematic review. Eur. J. Pain 2009, 13, 719–730. [Google Scholar] [CrossRef]
- Small, C.; Laycock, H. Acute postoperative pain management. Br. J. Surg. 2020, 107, e70–e80. [Google Scholar] [CrossRef]
- Tighe, P.J.; Le-Wendling, L.T.; Patel, A.; Zou, B.; Fillingim, R.B. Clinically derived early postoperative pain trajectories differ by age, sex, and type of surgery. Pain 2015, 156, 609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerbershagen, H.J.; Pogatzki-Zahn, E.; Aduckathil, S.; Peelen, L.M.; Kappen, T.H.; van Wijck, A.J.; Kalkman, C.J.; Meissner, W. Procedure-specific risk factor analysis for the development of severe postoperative pain. Anesthesiology 2014, 120, 1237–1245. [Google Scholar] [CrossRef]
- Chapman, C.R.; Donaldson, G.W.; Davis, J.J.; Bradshaw, D.H. Improving individual measurement of postoperative pain: The pain trajectory. J. Pain 2011, 12, 257–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannampallil, T.; Galanter, W.L.; Falck, S.; Gaunt, M.J.; Gibbons, R.D.; McNutt, R.; Odwazny, R.; Schiff, G.; Vaida, A.J.; Wilkie, D.J. Characterizing the pain score trajectories of hospitalized adult medical and surgical patients: A retrospective cohort study. Pain 2016, 157, 2739. [Google Scholar] [CrossRef] [Green Version]
- Lavand’homme, P.M.; Grosu, I.; France, M.N.; Thienpont, E. Pain trajectories identify patients at risk of persistent pain after knee arthroplasty: An observational study. Clin. Orthop. Relat. Res. 2014, 472, 1409–1415. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, A.; Yamasaki, M.; Yokota, I.; Mori, M.; Matsuda, M.; Yamaguchi, Y.; Yamakita, S.; Ueno, H.; Sawa, T.; Taguchi, T. Classification of acute pain trajectory after breast cancer surgery identifies patients at risk for persistent pain: A prospective observational study. J. Pain Res. 2018, 11, 2197. [Google Scholar] [CrossRef] [Green Version]
- Althaus, A.; Arránz Becker, O.; Moser, K.H.; Lux, E.A.; Weber, F.; Neugebauer, E.; Simanski, C. Postoperative pain trajectories and pain Chronification—an empirical typology of pain patients. Pain Med. 2018, 19, 2536–2545. [Google Scholar] [CrossRef] [PubMed]
- Althaus, A.; Arránz Becker, O.; Neugebauer, E. Distinguishing between pain intensity and pain resolution: Using acute post-surgical pain trajectories to predict chronic post-surgical pain. Eur. J. Pain 2014, 18, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Boussard, T.; Graham, L.A.; Desai, K.; Wahl, T.S.; Aucoin, E.; Richman, J.S.; Morris, M.S.; Itani, K.M.; Telford, G.L.; Hawn, M.T. The fifth vital sign postoperative pain predicts 30-day readmissions and subsequent emergency department visits. Ann. Surg. 2017, 266, 516. [Google Scholar] [CrossRef] [PubMed]
- James, R.J.; Walsh, D.A.; Ferguson, E. Trajectories of pain predict disabilities affecting daily living in arthritis. Br. J. Health Psychol. 2019, 24, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.K.; Tai, Y.H.; Lin, S.P.; Wu, H.L.; Tsou, M.Y.; Chang, K.Y. An investigation of the relationships between postoperative pain trajectories and outcomes after surgery for colorectal cancer. J. Chin. Med. Assoc. 2019, 82, 865–871. [Google Scholar] [CrossRef]
- Hah, J.M.; Cramer, E.; Hilmoe, H.; Schmidt, P.; McCue, R.; Trafton, J.; Clay, D.; Sharifzadeh, Y.; Ruchelli, G.; Goodman, S. Factors associated with acute pain estimation, postoperative pain resolution, opioid cessation, and recovery: Secondary analysis of a randomized clinical trial. JAMA Netw. Open 2019, 2, e190168. [Google Scholar] [CrossRef] [Green Version]
- Tai, Y.H.; Wu, H.L.; Lin, S.P.; Tsou, M.Y.; Chang, K.Y. Influential factors of postoperative pain trajectories in patients receiving intravenous patient-controlled analgesia: A single-centre cohort study in Taiwan. BMJ Open 2019, 9, e031936. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.Y.; Chang, W.K.; Wu, H.L.; Lin, S.P.; Tsou, M.Y.; Chang, K.Y. Dynamic analysis of variations in postoperative pain trajectories over time in patients receiving epidural analgesia using latent curve models. J. Chin. Med. Assoc. 2020, 83, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Chao, P.W.; Lin, S.P.; Tsou, M.Y.; Kuo, I.T.; Chang, K.Y. Assessing the impact of renal function on trajectory of intravenous patient-controlled analgesic demands over time after open and laparoscopic colorectal surgery using latent curve analysis. Clin. J. Pain 2016, 32, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Wichman, A.L.; MacCallum, R.C.; Briggs, N.E. Latent Growth Curve Modeling; Sage: Los Angeles, CA, USA, 2008; pp. 22–52. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with Amos: Basic Concepts, Applications, and Programming, 3rd ed.; Routledge: New York, NY, USA, 2016; pp. 339–363. [Google Scholar]
- Hair, J.F.; Black, B.; Babin, B.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 6th ed.; Pearson Education Inc.: Upper Saddle River, NJ, USA, 2006; pp. 740–742. [Google Scholar]
- Kim, H.C.; Bae, J.Y.; Kim, T.K.; Jeon, Y.; Min, J.J.; Goo, E.K.; Hong, D.M. Efficacy of intrathecal morphine for postoperative pain management following open nephrectomy. J. Int. Med. Res. 2016, 44, 42–53. [Google Scholar] [CrossRef] [Green Version]
- Gerbershagen, H.J.; Dagtekin, O.; Rothe, T.; Heidenreich, A.; Gerbershagen, K.; Sabatowski, R.; Petzke, F.; Özgür, E. Risk factors for acute and chronic postoperative pain in patients with benign and malignant renal disease after nephrectomy. Eur. J. Pain 2009, 13, 853–860. [Google Scholar] [CrossRef]
- Dillenburg, W.; Poulakis, V.; Skriapas, K.; de Vries, R.; Ferakis, N.; Witzsch, U.; Melekos, M.; Becht, E. Retroperitoneoscopic versus open surgical radical nephrectomy for large renal cell carcinoma in clinical stage cT2 or cT3a: Quality of life, pain and reconvalescence. Eur. Urol. 2006, 49, 314–323. [Google Scholar] [CrossRef]
- Hemal, A.; Kumar, A.; Kumar, R.; Wadhwa, P.; Seth, A.; Gupta, N. Laparoscopic versus open radical nephrectomy for large renal tumors: A long-term prospective comparison. J. Urol. 2007, 177, 862–866. [Google Scholar] [CrossRef]
- Isik Alper, E.Y. Comparison of acute and chronic pain after open nephrectomy versus laparoscopic nephrectomy: A prospective clinical trial. Medicine 2016, 95, e3433. [Google Scholar] [CrossRef]
- Wang, J.; Fu, Y.; Yuan, T.; Wang, N. Comparison of postoperative analgesic requirements in living donors and patients undergoing similar surgical procedures. Transplant. Proc. 2015, 47, 1896–1900. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.M.; Hartley, R.L.; Leung, A.A.; Ronksley, P.E.; Jetté, N.; Casha, S.; Riva-Cambrin, J. Preoperative predictors of poor acute postoperative pain control: A systematic review and meta-analysis. BMJ open 2019, 9, e025091. [Google Scholar] [CrossRef]
- Kaye, A.D.; Baluch, A.; Scott, J.T. Pain management in the elderly population: A review. Ochsner J. 2010, 10, 179–187. [Google Scholar]
- Chakour, M.; Gibson, S.; Bradbeer, M.; Helme, R. The effect of age on Aδ-and C-fibre thermal pain perception. Pain 1996, 64, 143–152. [Google Scholar] [CrossRef]
- Barsky, A.J.; Peekna, H.M.; Borus, J.F. Somatic symptom reporting in women and men. J. Gen. Intern. Med. 2001, 16, 266–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ip, H.Y.V.; Abrishami, A.; Peng, P.W.; Wong, J.; Chung, F. Predictors of postoperative pain and analgesic consumption: A qualitative systematic review. Anesthesiology 2009, 111, 657–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, M.J.; Ventham, N.T.; McNally, S.; Harrison, E.; Wigmore, S. Analgesia after open abdominal surgery in the setting of enhanced recovery surgery: A systematic review and meta-analysis. JAMA Surg. 2014, 149, 1224–1230. [Google Scholar] [CrossRef]
- Deyo, R.; Cherkin, D.; Loeser, J.; Bigos, S.; Ciol, M. Morbidity and mortality in association with operations on the lumbar spine. The influence of age, diagnosis, and procedure. J. Bone Joint Surg. Am. 1992, 74, 536–543. [Google Scholar] [CrossRef]
- Pagé, M.G.; Karanicolas, P.J.; Cleary, S.; Wei, A.C.; McHardy, P.; Ladak, S.S.; Ayach, N.; Sawyer, J.; McCluskey, S.A.; Srinivas, C. In-hospital opioid consumption, but not pain intensity scores, predicts 6-month levels of pain catastrophizing following hepatic resection: A trajectory analysis. Eur. J. Pain 2019, 23, 503–514. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No PCA (n = 362) | PCEA (n = 148) | IVPCA (n = 351) | p | |
|---|---|---|---|---|
| Age ≥ 60 years | 173 (47.8%) | 64 (43.2%) | 178 (50.7%) | 0.306 |
| Sex, female | 112 (30.9%) | 46 (31.1%) | 117 (33.3%) | 0.767 |
| Body height, cm | 165 ± 9 | 166 ± 8 | 164 ± 9 | 0.040 |
| Body weight, kg | 69.8 ± 14.0 | 70.2 ± 12.6 | 69.0 ± 13.5 | 0.591 |
| Body mass index, kg·m−2 | 25.6 ± 4.0 | 25.4 ± 3.9 | 25.7 ± 4.1 | 0.840 |
| ASA class ≥ 3 | 111 (30.7%) | 39 (26.4%) | 97 (27.6%) | 0.529 |
| Charlson comorbidity index | 4.1 ± 1.8 | 3.8 ± 1.8 | 4.0 ± 1.7 | 0.208 |
| Advanced cancer (stage III, IV) | 97 (26.8%) | 45 (30.4%) | 119 (33.9%) | 0.119 |
| Tumor side | 0.839 | |||
| Left | 172 (47.5%) | 64 (43.2%) | 169 (48.1%) | |
| Right | 183 (50.6%) | 80 (54.1%) | 173 (49.3%) | |
| Bilateral | 7 (1.9%) | 4 (2.7%) | 9 (2.6%) | |
| Anesthesia time, min * | 8.5 ± 0.4 | 8.5 ± 0.5 | 8.5 ± 0.5 | 0.172 |
| Surgical type | 0.330 | |||
| Radical nephrectomy | 230 (63.5%) | 87 (58.8%) | 205 (58.4%) | |
| Partial nephrectomy | 132 (36.5%) | 61 (41.2%) | 146 (41.6%) | |
| Surgical technique | <0.001 | |||
| Open | 109 (30.1%) | 134 (90.5%) | 210 (59.8%) | |
| Laparoscopic | 105 (29.0%) | 3 (2.0%) | 65 (18.5%) | |
| Robotic | 148 (40.9%) | 11 (7.4%) | 76 (21.7%) | |
| Surgical approach ** | <0.001 | |||
| Transperitoneal | 235 (64.9%) | 14 (9.4%) | 138 (39.3%) | |
| Retroperitoneal | 18 (5.0%) | 0 (0.0%) | 3 (0.9%) | |
| Surgical drain | 0.264 | |||
| 0 | 19 (5.2%) | 10 (6.8%) | 15 (4.3%) | |
| 1 | 332 (91.7%) | 128 (86.5%) | 322 (91.7%) | |
| ≥2 | 11 (3.0%) | 10 (6.8%) | 14 (4.0%) | |
| Surgical blood loss, mL * | 7.4 ± 1.9 | 8.0 ± 2.0 | 7.8 ± 1.9 | <0.001 |
| Perioperative transfusion | 69 (19.1%) | 42 (28.4%) | 95 (27.1%) | 0.106 |
| Mean NRS pain score | ||||
| POD 1 | 3.8 ± 2. | 2.8 ± 2.0 | 2.7 ± 2.0 | <0.001 |
| POD 2 | 3.1 ± 2.1 | 2.2 ± 1.3 | 2.5 ± 1.7 | <0.001 |
| POD 3 | 2.6 ± 1.7 | 2.2 ± 1.4 | 2.3 ± 1.4 | 0.012 |
| POD 4 | 2.3 ± 1.6 | 2.1 ± 1.4 | 2.3 ± 1.6 | 0.553 |
| POD 5 | 2.0 ± 1.5 | 2.0 ± 1.3 | 2.1 ± 1.4 | 0.920 |
| Intercept | Slope | |||||
|---|---|---|---|---|---|---|
| Estimate | SE | p | Estimate | SE | p | |
| Age ≥ 60 | 0.151 | 0.093 | 0.107 | −0.56 | 0.156 | <0.001 |
| Sex (female vs. male) | 0.204 | 0.1 | 0.04 | −0.162 | 0.165 | 0.326 |
| Body height | −0.004 | 0.005 | 0.468 | 0.004 | 0.009 | 0.633 |
| Body weight | −0.002 | 0.003 | 0.584 | 0.002 | 0.006 | 0.679 |
| Body mass index | −0.003 | 0.012 | 0.821 | 0.002 | 0.019 | 0.924 |
| ASA class (≥ 3 vs. < 3) | 0.211 | 0.103 | 0.04 | −0.052 | 0.17 | 0.758 |
| Charlson comorbidity index | 0.002 | 0.026 | 0.953 | −0.055 | 0.044 | 0.210 |
| Cancer (stage III, IV vs. I, II) | 0.243 | 0.101 | 0.016 | −0.145 | 0.167 | 0.386 |
| PCA use | ||||||
| PCEA vs. nil | −0.006 | 0.134 | 0.962 | −1.081 | 0.22 | <0.001 |
| IVPCA vs. nil | 0.122 | 0.104 | 0.238 | −1.065 | 0.17 | <0.001 |
| Tumor side (left vs. right) | −0.036 | 0.094 | 0.699 | −0.133 | 0.156 | 0.395 |
| Anesthesia time * | 0.083 | 0.102 | 0.416 | 0.116 | 0.169 | 0.493 |
| Surgical type (radical vs. partial) | 0.238 | 0.095 | 0.012 | −0.113 | 0.157 | 0.475 |
| Surgical technique | ||||||
| Laparoscopic vs. open | 0.081 | 0.122 | 0.504 | 0.623 | 0.202 | 0.002 |
| Robot vs. open | −0.248 | 0.109 | 0.023 | 0.154 | 0.181 | 0.394 |
| Surgical drain | −0.079 | 0.120 | 0.511 | 0.074 | 0.198 | 0.711 |
| Surgical blood loss * | 0.027 | 0.024 | 0.27 | 0.055 | 0.041 | 0.172 |
| Perioperative transfusion | 0.282 | 0.108 | 0.009 | 0.012 | 0.18 | 0.949 |
| Estimate | SE | p | |
|---|---|---|---|
| Intercept | |||
| Sex (female vs. male) | 0.236 | 0.094 | 0.028 |
| Cancer (stage III, IV vs. I, II) | 0.204 | 0.093 | 0.012 |
| Slope | |||
| Age ≥ 60 | −1.214 | 0.207 | <0.001 |
| PCA use | |||
| PCEA vs. nil | −1.068 | 0.159 | <0.001 |
| IVPCA vs. nil | 0.122 | 0.038 | <0.001 |
| Surgical blood loss * | 0.068 | 0.013 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, H.-J.; Chang, W.-K.; Yen, F.-Y.; Lin, S.-P.; Lin, T.-P.; Chang, K.-Y. Influential Factors and Personalized Prediction Model of Acute Pain Trajectories after Surgery for Renal Cell Carcinoma. J. Pers. Med. 2022, 12, 360. https://doi.org/10.3390/jpm12030360
Tsai H-J, Chang W-K, Yen F-Y, Lin S-P, Lin T-P, Chang K-Y. Influential Factors and Personalized Prediction Model of Acute Pain Trajectories after Surgery for Renal Cell Carcinoma. Journal of Personalized Medicine. 2022; 12(3):360. https://doi.org/10.3390/jpm12030360
Chicago/Turabian StyleTsai, Hsin-Jung, Wen-Kuei Chang, Fang-Yu Yen, Shih-Pin Lin, Tzu-Ping Lin, and Kuang-Yi Chang. 2022. "Influential Factors and Personalized Prediction Model of Acute Pain Trajectories after Surgery for Renal Cell Carcinoma" Journal of Personalized Medicine 12, no. 3: 360. https://doi.org/10.3390/jpm12030360