
Dynamics and Predictors of Cognitive Impairment along the Disease Course in Multiple Sclerosis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants, Clinical, and Cognitive Assessment
2.2. Magnetic Resonance Imaging (MRI)
2.2.1. MRI Acquisition and Processing
2.2.2. Structural MRI Processing for Volumetric Analysis
2.3. Statistical Analysis
3. Results
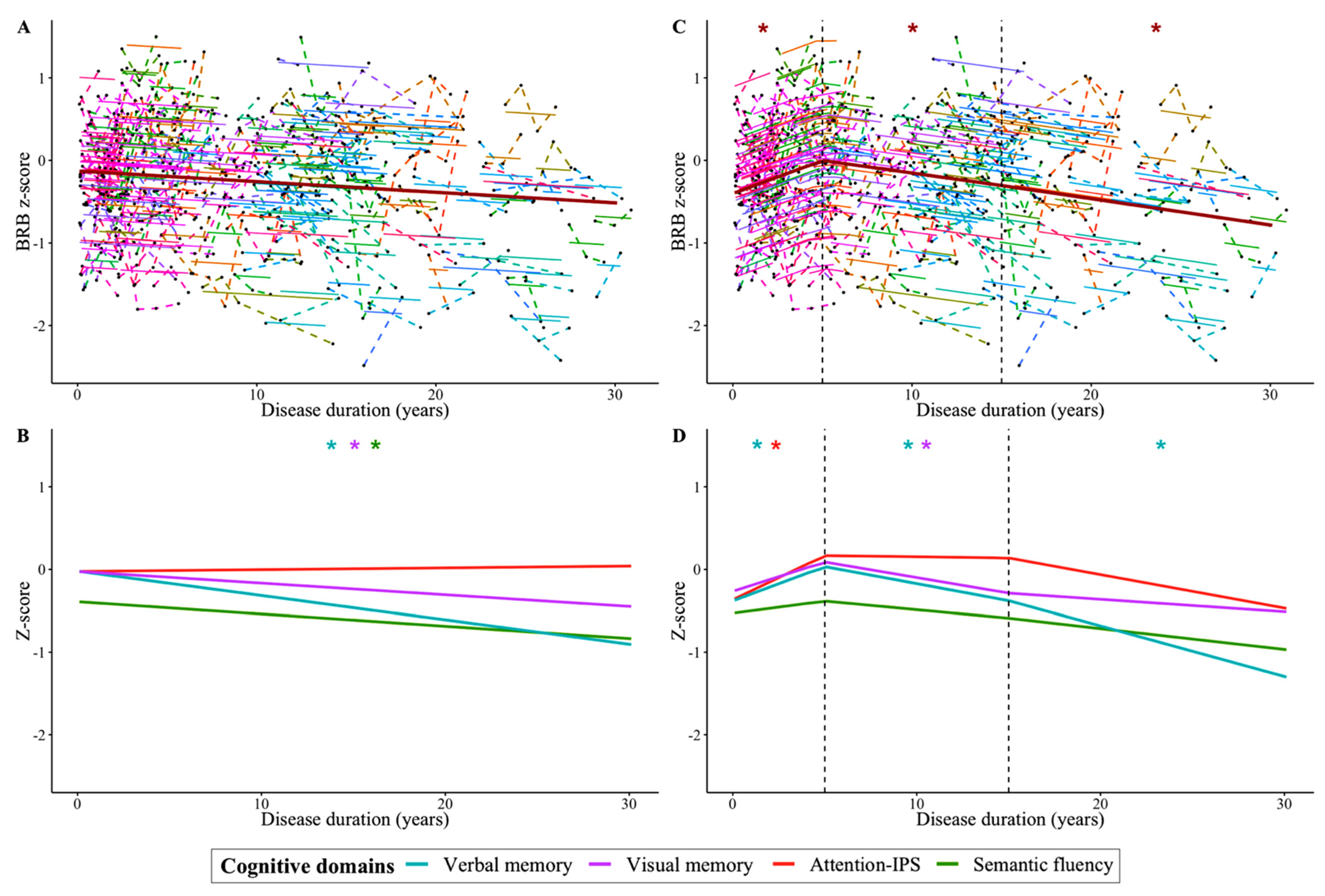
3.1. Cognitive Trajectory throughout Disease Course
3.2. Demographic, Clinical, and MRI Baseline Predictors of Future CI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chiaravalloti, N.D.; DeLuca, J. Cognitive Impairment in Multiple Sclerosis. Lancet Neurol. 2008, 7, 1139–1151. [Google Scholar] [CrossRef]
- Højsgaard Chow, H.; Schreiber, K.; Magyari, M.; Ammitzbøll, C.; Börnsen, L.; Romme Christensen, J.; Ratzer, R.; Soelberg Sørensen, P.; Sellebjerg, F. Progressive Multiple Sclerosis, Cognitive Function, and Quality of Life. Brain Behav. 2018, 8, e00875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, M.P.; Portaccio, E.; Goretti, B.; Zipoli, V.; Hakiki, B.; Giannini, M.; Pastò, L.; Razzolini, L. Cognitive Impairment in Early Stages of Multiple Sclerosis. Neurol. Sci. 2010, 31, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Sumowski, J.F.; Benedict, R.; Enzinger, C.; Filippi, M.; Geurts, J.J.; Hamalainen, P.; Hulst, H.; Inglese, M.; Leavitt, V.M.; Rocca, M.A.; et al. Cognition in Multiple Sclerosis: State of the Field and Priorities for the Future. Neurology 2018, 90, 278–288. [Google Scholar] [CrossRef] [Green Version]
- Damasceno, A.; Pimentel-Silva, L.R.; Damasceno, B.P.; Cendes, F. Cognitive Trajectories in Relapsing–remitting Multiple Sclerosis: A Longitudinal 6-Year Study. Mult. Scler. 2020, 26, 1740–1751. [Google Scholar] [CrossRef]
- Heled, E.; Aloni, R.; Achiron, A. Cognitive Functions and Disability Progression in Relapsing-Remitting Multiple Sclerosis: A Longitudinal Study. Appl. Neuropsychol. Adult 2021, 28, 210–219. [Google Scholar] [CrossRef]
- Eijlers, A.J.C.; Meijer, K.A.; van Geest, Q.; Geurts, J.J.G.; Schoonheim, M.M. Determinants of Cognitive Impairment in Patients with Multiple Sclerosis with and without Atrophy. Radiology 2018, 288, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Di Filippo, M.; Portaccio, E.; Mancini, A.; Calabresi, P. Multiple Sclerosis and Cognition: Synaptic Failure and Network Dysfunction. Nat. Rev. Neurosci. 2018, 19, 599–609. [Google Scholar] [CrossRef]
- Martínez-Lapiscina, E.H.; Fraga-Pumar, E.; Gabilondo, I.; Martínez-Heras, E.; Torres-Torres, R.; Ortiz-Pérez, S.; Llufriu, S.; Tercero, A.; Andorra, M.; Roca, M.F.; et al. The Multiple Sclerosis Visual Pathway Cohort: Understanding Neurodegeneration in MS. BMC Res. Notes 2014, 7, 910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llufriu, S.; Martinez-Heras, E.; Solana, E.; Sola-Valls, N.; Sepulveda, M.; Blanco, Y.; Martinez-Lapiscina, E.H.; Andorra, M.; Villoslada, P.; Prats-Galino, A.; et al. Structural Networks Involved in Attention and Executive Functions in Multiple Sclerosis. NeuroImage Clin. 2017, 13, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating Neurologic Impairment in Multiple Sclerosis: An Expanded Disability Status Scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.M.; Leo, G.J.; Bernardin, L.; Unverzagt, F. Cognitive Dysfunction in Multiple Sclerosis. I. Frequency, Patterns, and Prediction. Neurology 1991, 41, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Sepulcre, J.; Vanotti, S.; Hernández, R.; Sandoval, G.; Cáceres, F.; Garcea, O.; Villoslada, P. Cognitive Impairment in Patients with Multiple Sclerosis Using the Brief Repeatable Battery-Neuropsychology Test. Mult. Scler. 2006, 12, 187–195. [Google Scholar] [CrossRef]
- Klein, A.; Ghosh, S.S.; Bao, F.S.; Giard, J.; Häme, Y.; Stavsky, E.; Lee, N.; Rossa, B.; Reuter, M.; Chaibub Neto, E.; et al. Mindboggling Morphometry of Human Brains. PLoS Comput. Biol. 2017, 13, e1005350. [Google Scholar] [CrossRef] [PubMed]
- Desikan, R.S.; Ségonne, F.; Fischl, B.; Quinn, B.T.; Dickerson, B.C.; Blacker, D.; Buckner, R.L.; Dale, A.M.; Maguire, R.P.; Hyman, B.T.; et al. An Automated Labeling System for Subdividing the Human Cerebral Cortex on MRI Scans into Gyral Based Regions of Interest. Neuroimage 2006, 31, 968–980. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.J.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in Functional and Structural MR Image Analysis and Implementation as FSL. Neuroimage 2004, 23 (Suppl. S1), S208–S219. [Google Scholar] [CrossRef] [Green Version]
- Fortin, J.-P.; Parker, D.; Tunç, B.; Watanabe, T.; Elliott, M.A.; Ruparel, K.; Roalf, D.R.; Satterthwaite, T.D.; Gur, R.C.; Gur, R.E.; et al. Harmonization of Multi-Site Diffusion Tensor Imaging Data. Neuroimage 2017, 161, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Radua, J.; Vieta, E.; Shinohara, R.; Kochunov, P.; Quidé, Y.; Green, M.J.; Weickert, C.S.; Weickert, T.; Bruggemann, J.; Kircher, T.; et al. Increased Power by Harmonizing Structural MRI Site Differences with the ComBat Batch Adjustment Method in ENIGMA. Neuroimage 2020, 218, 116956. [Google Scholar] [CrossRef]
- Scalfari, A.; Neuhaus, A.; Daumer, M.; Muraro, P.A.; Ebers, G.C. Onset of Secondary Progressive Phase and Long-Term Evolution of Multiple Sclerosis. J. Neurol. Neurosurg. Psychiatry 2014, 85, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Akaike, H. A New Look at the Statistical Model Identification. Springer Ser. Stat. 1974, 215–222. [Google Scholar]
- Mahad, D.H.; Trapp, B.D.; Lassmann, H. Pathological Mechanisms in Progressive Multiple Sclerosis. Lancet Neurol. 2015, 14, 183–193. [Google Scholar] [CrossRef]
- Achiron, A.; Chapman, J.; Magalashvili, D.; Dolev, M.; Lavie, M.; Bercovich, E.; Polliack, M.; Doniger, G.M.; Stern, Y.; Khilkevich, O.; et al. Modeling of Cognitive Impairment by Disease Duration in Multiple Sclerosis: A Cross-Sectional Study. PLoS ONE 2013, 8, e71058. [Google Scholar]
- Leavitt, V.M.; Brandstadter, R.; Fabian, M.; Sand, I.K.; Klineova, S.; Krieger, S.; Lewis, C.; Lublin, F.; Miller, A.; Pelle, G.; et al. Dissociable Cognitive Patterns Related to Depression and Anxiety in Multiple Sclerosis. Mult. Scler. J. 2020, 26, 1247–1255. [Google Scholar] [CrossRef]
- Wojcik, C.; Fuchs, T.A.; Tran, H.; Dwyer, M.G.; Jakimovski, D.; Unverdi, M.; Weinstock-Guttman, B.; Zivadinov, R.; Eshaghi, A.; Benedict, R.H. Staging and Stratifying Cognitive Dysfunction in Multiple Sclerosis. Mult. Scler. 2021, 13524585211011390. [Google Scholar]
- De Meo, E.; Portaccio, E.; Giorgio, A.; Ruano, L.; Goretti, B.; Niccolai, C.; Patti, F.; Chisari, C.G.; Gallo, P.; Grossi, P.; et al. Identifying the Distinct Cognitive Phenotypes in Multiple Sclerosis. JAMA Neurol. 2021, 78, 414–425. [Google Scholar] [CrossRef]
- Sumowski, J.F.; Chiaravalloti, N.; DeLuca, J. Cognitive Reserve Protects against Cognitive Dysfunction in Multiple Sclerosis. J. Clin. Exp. Neuropsychol. 2009, 31, 913–926. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Soley, E.; Solana, E.; Martínez-Heras, E.; Andorra, M.; Radua, J.; Prats-Uribe, A.; Montejo, C.; Sola-Valls, N.; Sepulveda, M.; Pulido-Valdeolivas, I.; et al. Impact of Cognitive Reserve and Structural Connectivity on Cognitive Performance in Multiple Sclerosis. Front. Neurol. 2020, 11, 581700. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, A.; Müller-Lenke, N.; Naegelin, Y.; Kalt, G.; Bendfeldt, K.; Kuster, P.; Stoecklin, M.; Gass, A.; Sprenger, T.; Radue, E.W.; et al. Contribution of Cortical and White Matter Lesions to Cognitive Impairment in Multiple Sclerosis. Mult. Scler. 2013, 19, 1290–1296. [Google Scholar] [CrossRef]
- Glikmann-Johnston, Y.; Oren, N.; Hendler, T.; Shapira-Lichter, I. Distinct Functional Connectivity of the Hippocampus during Semantic and Phonemic Fluency. Neuropsychologia 2015, 69, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Llufriu, S.; Rocca, M.A.; Pagani, E.; Riccitelli, G.C.; Solana, E.; Colombo, B.; Rodegher, M.; Falini, A.; Comi, G.; Filippi, M. Hippocampal-Related Memory Network in Multiple Sclerosis: A Structural Connectivity Analysis. Mult. Scler. 2019, 25, 801–810. [Google Scholar] [CrossRef]
- Sepulcre, J.; Masdeu, J.C.; Sastre-Garriga, J.; Goñi, J.; Vélez-de-Mendizábal, N.; Duque, B.; Pastor, M.A.; Bejarano, B.; Villoslada, P. Mapping the Brain Pathways of Declarative Verbal Memory: Evidence from White Matter Lesions in the Living Human Brain. Neuroimage 2008, 42, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Weygandt, M.; Wakonig, K.; Behrens, J.; Meyer-Arndt, L.; Söder, E.; Brandt, A.U.; Bellmann-Strobl, J.; Ruprecht, K.; Gold, S.M.; Haynes, J.-D.; et al. Brain Activity, Regional Gray Matter Loss, and Decision-Making in Multiple Sclerosis. Mult. Scler. 2018, 24, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Sepulcre, J.; Masdeu, J.C.; Pastor, M.A.; Goñi, J.; Barbosa, C.; Bejarano, B.; Villoslada, P. Brain Pathways of Verbal Working Memory: A Lesion-Function Correlation Study. Neuroimage 2009, 47, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Ontaneda, D. Thalamic Injury and Cognition in Multiple Sclerosis. Front. Neurol. 2020, 11, 623914. [Google Scholar] [CrossRef]
- Keser, Z.; Hasan, K.M.; Mwangi, B.; Younes, K.; Khayat-Khoei, M.; Kamali, A.; Lincoln, J.A.; Nelson, F.M. Quantitative Limbic System Mapping of Main Cognitive Domains in Multiple Sclerosis. Front. Neurol. 2018, 9, 132. [Google Scholar] [CrossRef]


{kind=link}
| Entire Cohort (n = 212) | |
|---|---|
| Female, n (%) | 145 (68) |
| Age, mean (SD) | 41 (9.47) |
| Educational level, n (%) | |
| Basic (0–8 years) | 16 (8) |
| Primary (9–12 years) | 85 (40) |
| Secondary (13–16 years) | 75 (35) |
| Higher (>17 years) | 36 (17) |
| Disease duration, median (range) | 8.20 (0.1–29.0) |
| Disease type, n (%) | |
| Clinically isolated syndrome | 19 (9) |
| Relapsing-remitting MS | 176 (83) |
| Secondary progressive MS | 13 (6) |
| Primary progressive MS | 4 (2) |
| EDSS score, median (range) | 2.0 (0–7.0) |
| Use of DMTs, n (%) | 111 (52) |
| Number of previous relapses, median [IQR] | 3 (2–4) |
| Lesion volume (cm3), median [IQR] | 5.16 (2.37–12.15) |
| Cognitive Domain | N | Balanced Accuracy (%) | Sensitivity (%, 95% CI) | Specificity (%, 95% CI) | PPV (%, 95% CI) | NPV (%, 95% CI) |
|---|---|---|---|---|---|---|
| Global cognition | 212 | 71 | 70 (59–80) | 71 (63–79) | 58 (47–68) | 81 (72–87) |
| Verbal memory | 212 | 79 | 76 (63–86) | 82 (76–88) | 62 (50–73) | 90 (84–94) |
| Visual memory | 212 | 62 | 71 (56–82) | 54 (46–62) | 33 (24–42) | 85 (77–91) |
| Attention-IPS | 212 | 73 | 71 (54–85) | 75 (68–81) | 38 (27–50) | 92 (86–96) |
| Semantic fluency | 210 | 62 | 51 (44–59) | 73 (57–86) | 89 (81–94) | 29 (19–36) |
| Cognitive Domain | N | Predictors | β | Predictors Selection Rates (Frequency *, %) |
|---|---|---|---|---|
| Global cognition | 212 | Educational level | −0.060 | 1253 (63) |
| Disease duration | 0.034 | 936 (47) | ||
| EDSS score | 0.325 | 2000 (100) | ||
| Number of previous relapses | 0.069 | 1635 (82) | ||
| Lesion volume | 0.388 | 2000 (100) | ||
| LH parahippocampal | 0.127 | 1793 (90) | ||
| Left hippocampus | 0.070 | 1595 (80) | ||
| Right caudate | −0.057 | 1133 (57) | ||
| RH entorhinal | 0.044 | 1087 (54) | ||
| RH parahippocampal | 0.085 | 1836 (92) | ||
| RH rostral anterior cingulate | 0.195 | 1984 (99) | ||
| Verbal memory | 212 | Educational level | −0.386 | 1983 (99) |
| Disease type | 0.229 | 1557 (78) | ||
| EDSS score | 0.458 | 2000 (100) | ||
| Number of previous relapses | 0.115 | 1935 (97) | ||
| Lesion volume | 0.309 | 1998 (100) | ||
| LH parsopercularis | −0.101 | 1046 (52) | ||
| LH pericalcarine | 0.226 | 1894 (95) | ||
| Left thalamus proper | −0.096 | 1536 (77) | ||
| Left accumbens area | 0.038 | 1102 (55) | ||
| RH parahippocampal | 0.680 | 2000 (100) | ||
| RH rostral anterior cingulate | 0.040 | 1407 (70) | ||
| Visual memory | 212 | Lesion volume | 0.054 | 1949 (97) |
| Attention-IPS | 212 | EDSS score | 0.654 | 2000 (100) |
| Lesion volume | 0.199 | 1975 (99) | ||
| LH pericalcarine | 0.103 | 1838 (92) | ||
| Right hippocampus | 0.078 | 0.919 (83) | ||
| RH caudal anterior cingulate | 0.035 | 881 (44) | ||
| RH entorhinal | 0.111 | 1275 (64) | ||
| Semantic fluency | 210 | Lesion volume | −0.019 | 1005 (50) |
| Left hippocampus | −0.017 | 1071 (53) | ||
| RH rostral anterior cingulate | −0.021 | 658 (33) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Soley, E.; Martinez-Heras, E.; Andorra, M.; Solanes, A.; Radua, J.; Montejo, C.; Alba-Arbalat, S.; Sola-Valls, N.; Pulido-Valdeolivas, I.; Sepulveda, M.; et al. Dynamics and Predictors of Cognitive Impairment along the Disease Course in Multiple Sclerosis. J. Pers. Med. 2021, 11, 1107. https://doi.org/10.3390/jpm11111107
Lopez-Soley E, Martinez-Heras E, Andorra M, Solanes A, Radua J, Montejo C, Alba-Arbalat S, Sola-Valls N, Pulido-Valdeolivas I, Sepulveda M, et al. Dynamics and Predictors of Cognitive Impairment along the Disease Course in Multiple Sclerosis. Journal of Personalized Medicine. 2021; 11(11):1107. https://doi.org/10.3390/jpm11111107
Chicago/Turabian StyleLopez-Soley, Elisabet, Eloy Martinez-Heras, Magi Andorra, Aleix Solanes, Joaquim Radua, Carmen Montejo, Salut Alba-Arbalat, Nuria Sola-Valls, Irene Pulido-Valdeolivas, Maria Sepulveda, and et al. 2021. "Dynamics and Predictors of Cognitive Impairment along the Disease Course in Multiple Sclerosis" Journal of Personalized Medicine 11, no. 11: 1107. https://doi.org/10.3390/jpm11111107