
Effect of COVID-19-Related Lockdown οn Hospital Admissions for Asthma and COPD Exacerbations: Associations with Air Pollution and Patient Characteristics

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Patient Population
2.2. Study Periods
- (1)
- Lockdown: 9 March–3 May 2020 (8 weeks, Monday to Sunday)
- (2)
- Control: 11 March–5 May 2019 (8 weeks, Monday to Sunday)
- (3)
- Pre-lockdown: 3 February–8 March 2020 (5 weeks, Monday to Sunday)
- (4)
- Pre-Control: 4 February–10 March 2019 (5 weeks, Monday to Sunday)
- (5)
- Post-lockdown: 4 May–31 May 2020 (4 weeks, Monday to Sunday)
- (6)
- Post-Control: 6 May–2 June 2019 (4 weeks, Monday to Sunday)
2.3. Data Collection
2.4. Primary and Secondary Outcomes
2.5. Statistical Analysis
3. Results
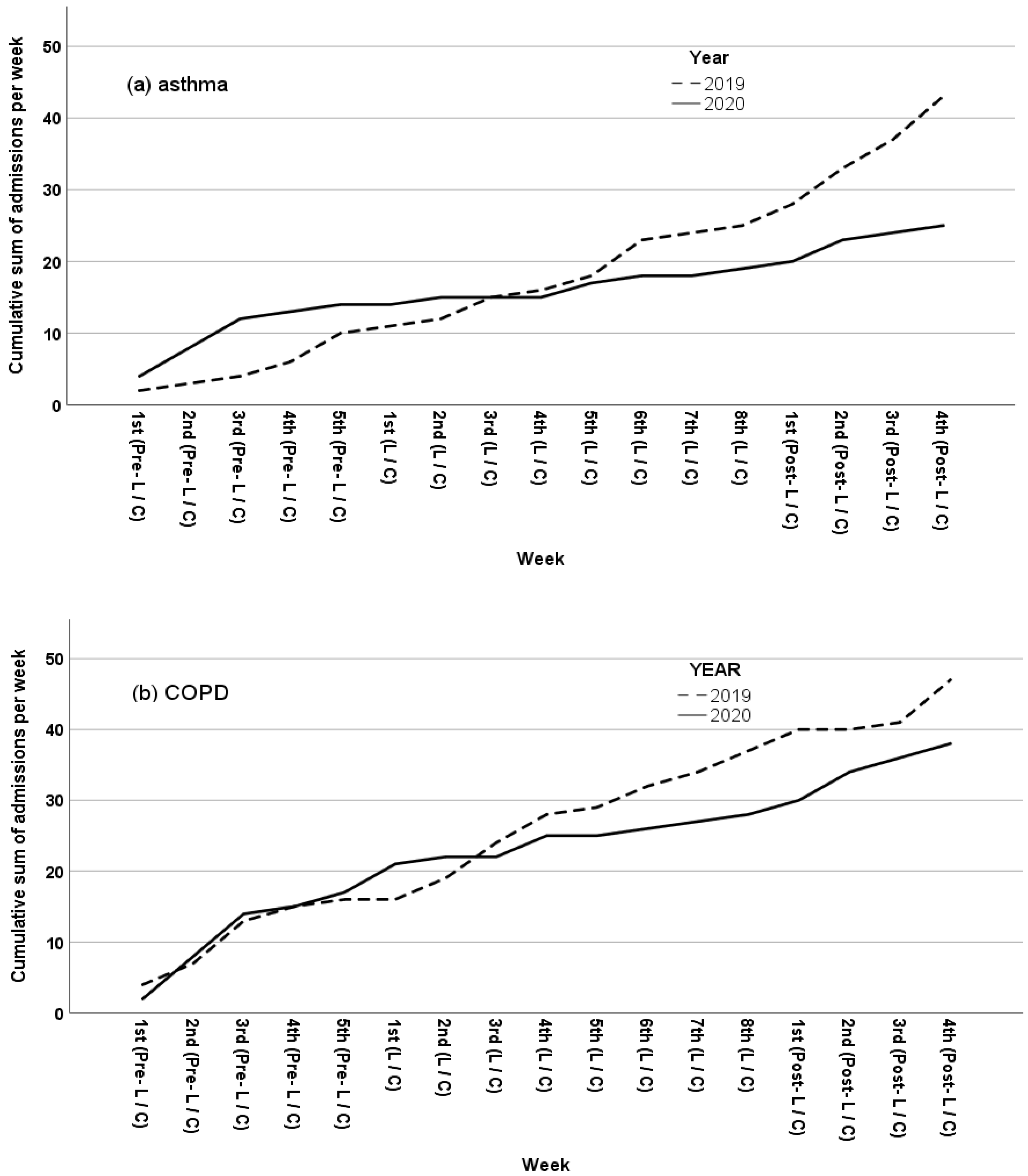
3.1. Primary Outcome
3.1.1. IR of Asthma and COPD Exacerbations
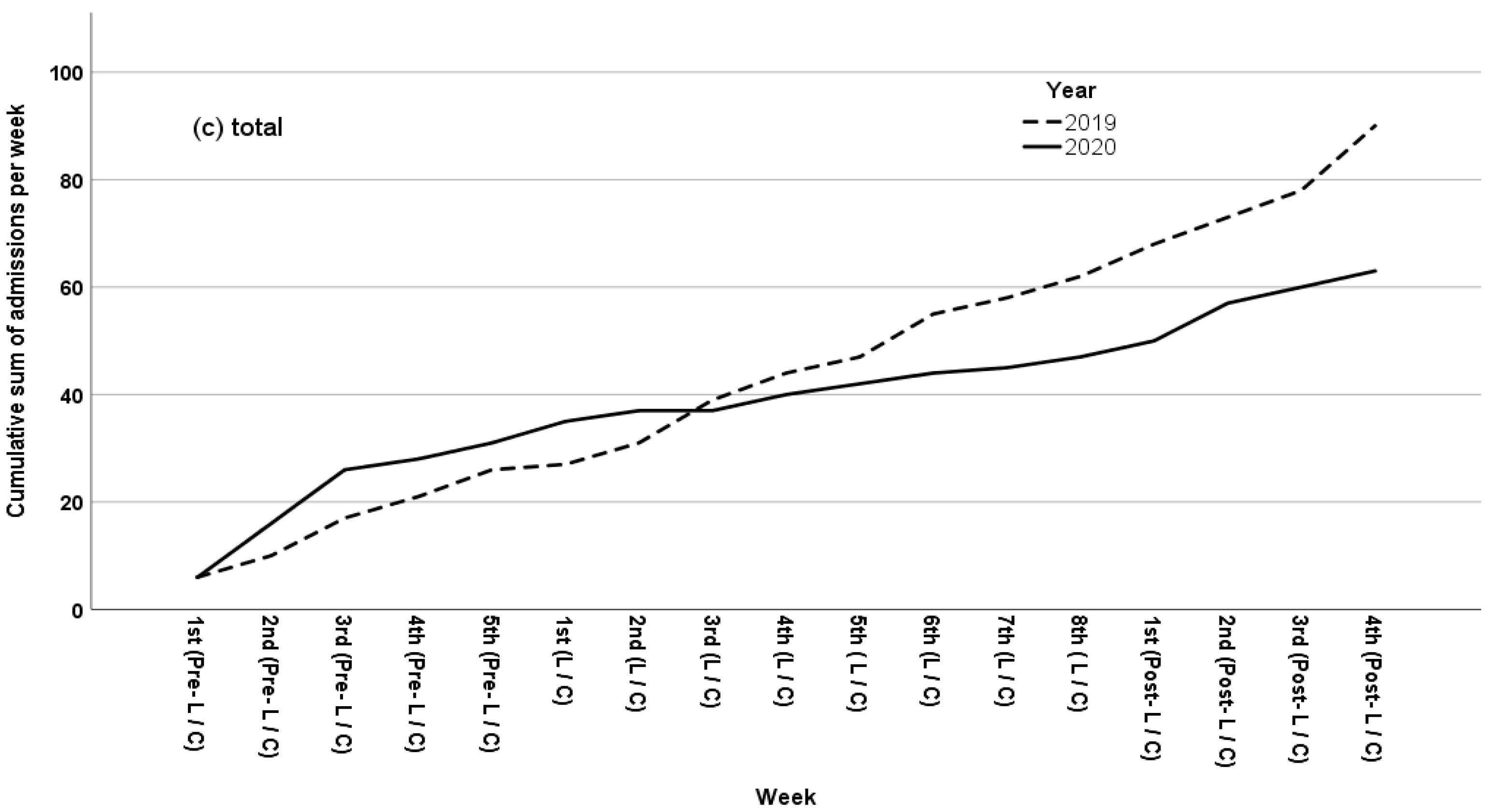
3.1.2. IR of Total Hospital Admission Rates
3.2. Secondary Outcomes
Patient Population Characteristics: Lockdown versus Pre-Lockdown
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Price, D.; Dale, P.; Elder, E.; Chapman, K.R. Types, frequency and impact of asthma triggers on patients’ lives: A quantitative study in five European countries. J. Asthma 2013, 51, 127–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, E.; Miller, G.E. Stress and inflammation in exacerbations of asthma. Brain Behav. Immun. 2007, 21, 993–999. [Google Scholar] [CrossRef] [Green Version]
- Liccardi, G.; Calzetta, L.; Milanese, M.; Salzillo, A.; Manzi, F.; Ferrari, M.; Rogliani, P. Psychological Stress, Lung Function and Exacerbation Risk in COPD: Is an Increase of Cholinergic Tone a Possible Link? COPD J. Chronic Obstr. Pulm. Dis. 2018, 15, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jung, H.M.; Kim, S.K.; Yoo, K.H.; Jung, K.-S.; Lee, S.H.; Rhee, C.K. Factors associated with chronic obstructive pulmonary disease exacerbation, based on big data analysis. Sci. Rep. 2019, 9, 6679. [Google Scholar] [CrossRef] [Green Version]
- Qureshi, H.; Sharafkhaneh, A.; Hanania, N.A. Chronic obstructive pulmonary disease exacerbations: Latest evidence and clinical implications. Ther. Adv. Chronic Dis. 2014, 5, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Sin, D.D. COVID-19 in COPD: A growing concern. EClinicalMedicine 2020, 26, 100546. [Google Scholar] [CrossRef]
- Abrams, E.M.; Jong, G.W.T.; Yang, C. Asthma and COVID-19. Can. Med Assoc. J. 2020, 192, E551. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.; Wang, M.; Huang, C.; Kinney, P.L.; Anastas, P.T. Air pollution reduction and mortality benefit during the COVID-19 outbreak in China. Lancet Planet. Health 2020, 4, e210–e212. [Google Scholar] [CrossRef]
- Barach, P.; Fisher, S.D.; Adams, M.J.; Burstein, G.R.; Brophy, P.D.; Kuo, D.Z.; Lipshultz, S.E. Disruption of healthcare: Will the COVID pandemic worsen non-COVID outcomes and disease outbreaks? Prog. Pediatric Cardiol. 2020, 59, 101254. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact Of The COVID-19 Pandemic on Hospital Admissions in the United States. Health Aff. 2020, 39, 2010–2017. [Google Scholar] [CrossRef] [PubMed]
- Nourazari, S.; Davis, S.R.; Granovsky, R.; Austin, R.; Straff, D.J.; Joseph, J.W.; Sanchez, L.D. Decreased hospital admissions through emergency departments during the COVID-19 pandemic. Am. J. Emerg. Med. 2021, 42, 203–210. [Google Scholar] [CrossRef]
- Baeza-Martínez, C.; Zamora-Molina, L.; Olea-Soto, J.; Soler-Sempere, M.J.; García-Pachón, E. Disproportionate decline in admissions for exacerbated COPD during the COVID-19 pandemic. Respir. Med. 2020, 106120. [Google Scholar] [CrossRef]
- Baeza-Martínez, C.; Zamora-Molina, L.; Olea-Soto, J.; Soler-Sempere, M.J.; García-Pachón, E. Reduction in Hospital Admissions for COPD Exacerbation During the Covid-19 Pandemic. Open Respir. Arch. 2020, 2, 201–202. [Google Scholar] [CrossRef]
- Chan, K.P.F.; Ma, T.F.; Kwok, W.C.; Leung, J.K.C.; Chiang, K.Y.; Ho, J.C.M.; Lam, D.C.L.; Tam, T.C.C.; Ip, M.S.M.; Ho, P.L. Significant reduction in hospital admissions for acute exacerbation of chronic obstructive pulmonary disease in Hong Kong during coronavirus disease 2019 pandemic. Respir. Med. 2020, 171, 106085. [Google Scholar] [CrossRef]
- Tan, J.Y.; Conceicao, E.P.; Wee, L.E.; Sim, X.Y.J.; Venkatachalam, I. COVID-19 public health measures: A reduction in hospital admissions for COPD exacerbations. Thorax 2021, 76, 512–513. [Google Scholar] [CrossRef] [PubMed]
- Kaye, L.; Theye, B.; Smeenk, I.; Gondalia, R.; Barrett, M.A.; Stempel, D.A. Changes in medication adherence among patients with asthma and COPD during the COVID-19 pandemic. J. Allergy Clin. Immunol. Pract. 2020, 8, 2384–2385. [Google Scholar] [CrossRef]
- Pleguezuelos, E.; Del Carmen, A.; Moreno, E.; Ortega, P.; Vila, X.; Ovejero, L.; Serra-Prat, M.; Palomera, E.; Garnacho-Castaño, M.V.; Loeb, E.; et al. The Experience of COPD Patients in Lockdown Due to the COVID-19 Pandemic. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 2621–2627. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.; Gogali, A.; Exarchos, K.; Potonos, D.; Tatsis, K.; Apollonatou, V.; Loukides, S.; Papiris, S.; Sigala, I.; Katsaounou, P.; et al. Reduction in Hospitalizations for Respiratory Diseases during the First COVID-19 Wave in Greece. Respiration 2021, 100, 588–593. [Google Scholar] [CrossRef]
- Bafadhel, M.; Greening, N.; Harvey-Dunstan, T.C.; Williams, J.E.; Morgan, M.D.; Brightling, C.; Hussain, S.F.; Pavord, I.; Singh, S.J.; Steiner, M. Blood Eosinophils and Outcomes in Severe Hospitalized Exacerbations of COPD. Chest 2016, 150, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Prins, H.J.; Duijkers, R.; Lutter, R.; Daniels, J.; van der Valk, P.; Schoorl, M.; Kerstjens, H.; van der Werf, T.; Boersma, W.G. Blood eosinophilia as a marker of early and late treatment failure in severe acute exacerbations of COPD. Respir. Med. 2017, 131, 118–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, M.I.; Osadnik, C.R.; Bulfin, L.; Hamza, K.; Leong, P.; Wong, A.; King, P.T.; Bardin, P.G. Low and High Blood Eosinophil Counts as Biomarkers in Hospitalized Acute Exacerbations of COPD. Chest 2019, 156, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Jabarkhil, A.; Moberg, M.; Janner, J.; Petersen, M.N.; Jensen, C.B.; Henrik Ängquist, L.; Vestbo, J.; Jess, T.; Porsbjerg, C. Elevated blood eosinophils in acute COPD exacerbations: Better short- and long-term prognosis. Eur. Clin. Respir. J. 2020, 7, 1757274. [Google Scholar] [CrossRef] [PubMed]
- Sivapalan, P.; Jensen, J.U. Non-eosinophilic severe exacerbations of COPD: What about antibiotics?—Authors’ reply. Lancet Respir. Med. 2019, 7, e34. [Google Scholar] [CrossRef]
- Miravitlles, M.; Llor, C. Non-eosinophilic severe exacerbations of COPD: What about antibiotics? Lancet Respir. Med. 2019, 7, e33. [Google Scholar] [CrossRef]
- Abe, K.; Miyawaki, A.; Nakamura, M.; Ninomiya, H.; Kobayashi, Y. Trends in Hospitalizations for Asthma During the COVID-19 Outbreak in Japan. J. Allergy Clin. Immunol. Pract. 2021, 9, 494–496.e1. [Google Scholar] [CrossRef]
- Pignatti, P.; Visca, D.; Cherubino, F.; Zampogna, E.; Spanevello, A. Impact of COVID-19 on patients with asthma. Int. J. Tuberc. Lung Dis. 2020, 24, 1217–1219. [Google Scholar] [CrossRef]
- Khan, M.; Rajendram, R.; Al-Jahdali, H.; Alhamadi, M.; Alabdulaali, S.; Al-Ghamdi, B. P119 The effects of the COVID-19 lockdown on severe asthma in patients taking biologic therapy and air pollution. Thorax 2021, 76, A153. [Google Scholar]
- Taquechel, K.; Diwadkar, A.R.; Sayed, S.; Dudley, J.W.; Grundmeier, R.W.; Kenyon, C.C.; Henrickson, S.E.; Himes, B.E.; Hill, D.A. Pediatric Asthma Health Care Utilization, Viral Testing, and Air Pollution Changes During the COVID-19 Pandemic. J. Allergy Clin. Immunol. Pract. 2020, 8, 3378–3387.e11. [Google Scholar] [CrossRef]
- Krivec, U.; Seliger, A.K.; Tursic, J. COVID-19 lockdown dropped the rate of paediatric asthma admissions. Arch. Dis. Child. 2020, 105, 809–810. [Google Scholar] [CrossRef]
- Kenyon, C.C.; Hill, D.; Henrickson, S.E.; Bryant-Stephens, T.C.; Zorc, J.J. Initial effects of the COVID-19 pandemic on pediatric asthma emergency department utilization. J. Allergy Clin. Immunol. Pract. 2020, 8, 2774–2776.e1. [Google Scholar] [CrossRef]
- Simoneau, T.; Greco, K.F.; Hammond, A.; Nelson, K.; Gaffin, J.M. Impact of the COVID-19 pandemic on pediatric emergency department use for asthma. Ann. Am. Thorac. Soc. 2021, 18, 717–719. [Google Scholar] [CrossRef]
- Connerton, P.; De Assunção, J.V.; De Miranda, R.M.; Slovic, A.D.; Pérez-Martínez, P.J.; Ribeiro, H. Air quality during covid-19 in four megacities: Lessons and challenges for public health. Int. J. Environ. Res. Public Health 2020, 17, 5067. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, M.; Yu, S.; Chen, X.; Li, Z.; Zhang, Y.; Jiang, L.; Xia, Y.; Li, J.; Liu, W.; et al. Unexpected rise of ozone in urban and rural areas, and sulfur dioxide in rural areas during the coronavirus city lockdown in Hangzhou, China: Implications for air quality. Environ. Chem. Lett. 2020, 18, 1713–1723. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Sun, S.; Tang, R.; Qiu, H.; Huang, Q.; Mason, T.G.; Tian, L. Major air pollutants and risk of COPD exacerbations: A systematic review and meta-analysis. Int. J. COPD 2016, 11, 3079–3091. [Google Scholar] [CrossRef] [Green Version]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Kutralam-Muniasamy, G.; Pérez-Guevara, F.; Roy, P.D.; Elizalde-Martínez, I.; Shruti, V. Impacts of the COVID-19 lockdown on air quality and its association with human mortality trends in megapolis Mexico City. Air Qual. Atmos. Health 2021, 14, 553–562. [Google Scholar] [CrossRef]
- Xiang, J.; Austin, E.; Gould, T.; Larson, T.; Shirai, J.; Liu, Y.; Marshall, J.; Seto, E. Impacts of the COVID-19 responses on traffic-related air pollution in a Northwestern US city. Sci Total Environ. Sci. Total Environ. 2020, 747, 141325. [Google Scholar] [CrossRef]
- Hudda, N.; Simon, M.C.; Patton, A.P.; Durant, J.L. Reductions in traffic-related black carbon and ultrafine particle number concentrations in an urban neighborhood during the COVID-19 pandemic. Sci. Total Environ. 2020, 742, 140931. [Google Scholar] [CrossRef]
- Liu, N.; Lin, W.; Ma, J.; Xu, W.; Xu, X. Seasonal variation in surface ozone and its regional characteristics at global atmosphere watch stations in China. J. Environ. Sci. (China) 2019, 77, 291–302. [Google Scholar] [CrossRef]
- Selvaraj, R.S.; Padma, K.; Boaz, B.M. Seasonal variation of surface ozone and its association with meteorological parameters, UV-radiation, rainfall and cloud cover over Chennai, India. Curr. Sci. 2013, 105, 676–684. [Google Scholar]
- Krmpotic, D.; Luzar-Stiffler, V.; Herzog, P. Effects of urban ozone pollution on hospitalizations for exacerbation of chronic obstructive pulmonary disease. Eur. Respir. J. 2015, 46, PA3411. [Google Scholar]
- Li, X.; Chen, Q.; Zheng, X.; Li, Y.; Han, M.; Liu, T.; Xiao, J.; Guo, L.; Zeng, W.; Zhang, J.; et al. Effects of ambient ozone concentrations with different averaging times on asthma exacerbations: A meta-analysis. Sci. Total Environ. 2019, 691, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Paulin, L.M.; Gassett, A.J.; Alexis, N.E.; Kirwa, K.; Kanner, R.E.; Peters, S.; Krishnan, J.A.; Paine, R.; Dransfield, M.; Woodruff, P.G.; et al. Association of Long-term Ambient Ozone Exposure with Respiratory Morbidity in Smokers. JAMA Intern. Med. 2020, 180, 106–115. [Google Scholar] [CrossRef]
- Tobías, A.; Carnerero, C.; Reche, C.; Massagué, J.; Via, M.; Minguillón, M.C.; Alastuey, A.; Querol, X. Changes in air quality during the lockdown in Barcelona (Spain) one month into the SARS-CoV-2 epidemic. Sci. Total Environ. 2020, 726, 138540. [Google Scholar] [CrossRef]
- Li, L.; Li, Q.; Huang, L.; Wang, Q.; Zhu, A.; Xu, J.; Liu, Z.; Li, H.; Shi, L.; Li, R.; et al. Air quality changes during the COVID-19 lockdown over the Yangtze River Delta Region: An insight into the impact of human activity pattern changes on air pollution variation. Sci. Total Environ. 2020, 732, 139282. [Google Scholar] [CrossRef] [PubMed]
- McAuley, H.; Hadley, K.; Elneima, O.; Brightling, C.E.; Evans, R.A.; Steiner, M.C.; Greening, N.J. COPD in the time of COVID-19: An analysis of acute exacerbations and reported behavioural changes in patients with COPD. ERJ Open Res. 2021, 7. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Missing (Total) | Asthma (68 Admissions) | COPD (85 Admissions) | p-Value | |
|---|---|---|---|---|
| Age (years) | 1 | 57 (44.25–72) | 70 (63–78.75) | <0.001 |
| Females (%) | 0 | 55.9 | 37.6 | 0.024 |
| Hospitalization (days) | 0 | 5 (3–8) | 7 (5–12) | <0.001 |
| Symptom duration before admission (days) | 3 | 4.5 (2–7) | 5 (2–7) | 0.986 |
| Current Smoker (%) | 4 | 35.8 | 62.2 | 0.001 |
| Dyspnea (%) | 1 | 86.8 | 95.2 | 0.063 |
| Cough (%) | 1 | 70.6 | 70.2 | 0.962 |
| Sputum (%) | 1 | 47.1 | 64.3 | 0.033 |
| Fever (%) | 2 | 27.9 | 37.3 | 0.222 |
| Lethargy/Coma (%) | 2 | 8.8 | 20.5 | 0.047 |
| Respiratory Failure (%) | 2 | 63.2 | 94 | <0.001 |
| Hypercapnia (%) | 2 | 20.6 | 51.8 | <0.001 |
| Abnormal X-RAY (%) | 1 | 35.3 | 36.9 | 0.837 |
| White Blood Cells (admission) | 0 | 10,090 (7537.5–12,532.5) | 10,460 (7920–12,550) | 0.645 |
| Neutrophiles (%) | 0 | 72.25 (61.275–86) | 77.6 (69–87) | 0.047 |
| Lymphocytes (%) | 0 | 17 (9.075–25.825) | 14 (7.5–18.65) | 0.032 |
| Eosinophiles (%) | 0 | 1.2277 (0.1945–3.4631) | 0.4564 (0.0838–1.9037) | 0.010 |
| Eosinophile (n) | 0 | 120 (20–277.5) | 40 (10–175) | 0.008 |
| Serum CRP (mg/dL) | 0 | 1.7 (0.4–5.175) | 2.6 (0.8–11.1) | 0.025 |
| Intubation/Death(%) | 0 | 5.9 | 16.5 | 0.043 |
| Flu positive (%) | 0 | 4.4 | 3.5 | 1.000 |
| Asthma | COPD | Total Admissions | |||||||
|---|---|---|---|---|---|---|---|---|---|
| IR | IRR with 95% CI | p | IR | IRR with 95% CI | p | IR | IRR with 95% CI | p-Value | |
| Lockdown 2020 (Reference) | 0.625 | 1 | - | 1.375 | 1 | - | 2 | 1 | - |
| Pre-lockdown | 2.8 | 4.48 (1.6–12.4) | p = 0.004 | 3.4 | 2.5 (1.2–5.3) | p = 0.019 | 6.2 | 3.1 (1.7–5.7) | p < 0.001 |
| Post-lockdown | 1.5 | 2.4 (0.7–7.9) | p = 0.148 | 2.5 | 1.8 (0.8–4.3) | p = 0.171 | 4 | 2.0 (1.0–4.0) | p = 0.05 |
| Pre-Control | 2 | 3.2 (1.1–9.4) | p = 0.034 | 3.2 | 2.3 (1.1–5.0) | p = 0.031 | 5.2 | 2.6 (1.4–4.8) | p = 0.003 |
| Control 2019 | 1.875 | 3 (1.1–8.3) | p = 0.033 | 2.625 | 1.9 (0.9–4.0) | p = 0.082 | 4.5 | 2.3 (1.2–4.1) | p = 0.007 |
| Post-Control | 4.5 | 7.2 (2.7–19.4) | p < 0.001 | 2.5 | 1.8 (0.8–4.3) | p = 0.171 | 7 | 3.5 (1.9–6.5) | p < 0.001 |
| Asthma | COPD | |||||
|---|---|---|---|---|---|---|
| Pre-Lockdown (n = 14) | Lockdown (n = 5) | p-Value | Pre-Lockdown (n = 17) | Lockdown (n = 11) | p-Value | |
| Age (years) | 63.5 (55.5–81.5) | 50 (38–59.5) | 0.046 | 68 (63.5–75) | 76 (60–83) | 0.621 |
| Females (%) | 71.4 | 60 | 1.000 | 29.4 | 18.2 | 0.668 |
| Hospitalization (days) | 6 (2–8) | 4 (2.5–13.5) | 0.852 | 7 (5.5–13) | 9 (6–14) | 0.569 |
| Symptom duration before admission (days) | 4 (2–7) | 7 (4–10.5) | 0.138 | 7 (4–9.25) | 5 (2–7) | 0.278 |
| Current Smoker (%) | 57.1 | 20 | 0.303 | 68.8 | 45.5 | 0.264 |
| Dyspnea (%) | 85.7 | 80 | 1.000 | 100 | 100 | - |
| Cough (%) | 71.4 | 60 | 1.000 | 88.2 | 72.7 | 0.353 |
| Sputum (%) | 57.1 | 40 | 0.628 | 88.2 | 63.6 | 0.174 |
| Fever (%) | 35.7 | 20 | 1.000 | 43.8 | 27.3 | 0.448 |
| Lethargy/Coma (%) | 14.3 | 0 | 1.000 | 18.8 | 36.4 | 0.391 |
| Respiratory Failure (%) | 78.6 | 20 | 0.038 | 87.5 | 100 | 0.499 |
| Hypercapnia(%) | 28.6 | 0 | 0.530 | 56.3 | 63.6 | 1.000 |
| Abnormal X-RAY (%) | 42.9 | 20 | 0.603 | 41.2 | 36.4 | 1.000 |
| White Blood Cells | 9145 (7010–13,242.5) | 12,640 (8225–16,485) | 0.267 | 10,500 (8745–15,270) | 9270 (7090–14,800) | 0.290 |
| Neutrophiles (%) | 73.4 (57.8–77.1) | 72 (57.9–85.3) | 0.853 | 79 (74.3–85.5) | 75 (61–87) | 0.451 |
| Lymphocytes (%) | 17.2 (12.9–31.3) | 13.1 (8.6–19.6) | 0.195 | 10.7 (7–16.1) | 15 (8–25) | 0.437 |
| Eosinophiles (%) | 0.4 (0.1–1.7) | 2.8 (1–20.1) | 0.052 | 0.1 (0–0.8) | 2.2 (0.5–4.2) | 0.017 |
| Eosinophile (n) | 30 (10–205) | 220 (95–3225) | 0.070 | 10 (0–105) | 170 (30–300) | 0.012 |
| Serum CRP (mg/dL) | 3.1 (0.9–7.4) | 0.3 (0–13.5) | 0.115 | 3.8 (0.8–16.6) | 1.5 (0.2–8.8) | 0.110 |
| Intubation/Death (%) | 7.1 | 0 | 1.000 | 23.5 | 18.2 | 1.000 |
| Flu positive (%) | 14.3 | 0 | 1.000 | 5.9 | 0 | 1.000 |
| NO | NO2 | PM2.5 | PM10 | O3 | CO | SO2 | BENZENE | ||
|---|---|---|---|---|---|---|---|---|---|
| Total admissions | r | +0.694 | +0.601 | +0.526 | +0.435 | −0.635 | +0.707 | +0.373 | +0.721 |
| p | 0.002 | 0.011 | 0.030 | 0.081 | 0.006 | 0.002 | 0.140 | 0.001 | |
| Asthma admissions | r | +0.401 | +0.311 | +0.543 | +0.358 | −0.368 | +0.526 | +0.516 | +0.546 |
| p | 0.111 | 0.224 | 0.024 | 0.158 | 0.146 | 0.030 | 0.034 | 0.023 | |
| COPD admissions | r | +0.642 | +0.554 | +0.492 | +0.439 | −0.56 | +0.616 | +0.246 | +0.621 |
| p | 0.005 | 0.021 | 0.045 | 0.078 | 0.019 | 0.009 | 0.342 | 0.008 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sigala, I.; Giannakas, T.; Giannakoulis, V.G.; Zervas, E.; Brinia, A.; Gianiou, N.; Asimakos, A.; Dima, E.; Kalomenidis, I.; Katsaounou, P. Effect of COVID-19-Related Lockdown οn Hospital Admissions for Asthma and COPD Exacerbations: Associations with Air Pollution and Patient Characteristics. J. Pers. Med. 2021, 11, 867. https://doi.org/10.3390/jpm11090867
Sigala I, Giannakas T, Giannakoulis VG, Zervas E, Brinia A, Gianiou N, Asimakos A, Dima E, Kalomenidis I, Katsaounou P. Effect of COVID-19-Related Lockdown οn Hospital Admissions for Asthma and COPD Exacerbations: Associations with Air Pollution and Patient Characteristics. Journal of Personalized Medicine. 2021; 11(9):867. https://doi.org/10.3390/jpm11090867
Chicago/Turabian StyleSigala, Ioanna, Timoleon Giannakas, Vassilis G. Giannakoulis, Efthimios Zervas, Aikaterini Brinia, Niki Gianiou, Andreas Asimakos, Efi Dima, Ioannis Kalomenidis, and Paraskevi Katsaounou. 2021. "Effect of COVID-19-Related Lockdown οn Hospital Admissions for Asthma and COPD Exacerbations: Associations with Air Pollution and Patient Characteristics" Journal of Personalized Medicine 11, no. 9: 867. https://doi.org/10.3390/jpm11090867