
Treatment Adherence in Chronic Conditions during Ageing: Uses, Functionalities, and Cultural Adaptation of the Assistant on Care and Health Offline (ACHO) in Rural Areas

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Chronicity and Treatment Adherence in Ageing
2. Materials and Methods
2.1. Study Design
2.2. Ethics Approval
2.3. Participants
- Over 65 years of age.
- Non-institutionalised (in care homes, day-care centres, or any other kind of facility).
- Not subject to cognitive decline of any kind.
- To have been prescribed at least one chronic illness medication by a doctor.
- To have voluntarily accepted participation in the study and provided informed consent.
2.4. Data Collection and Measures
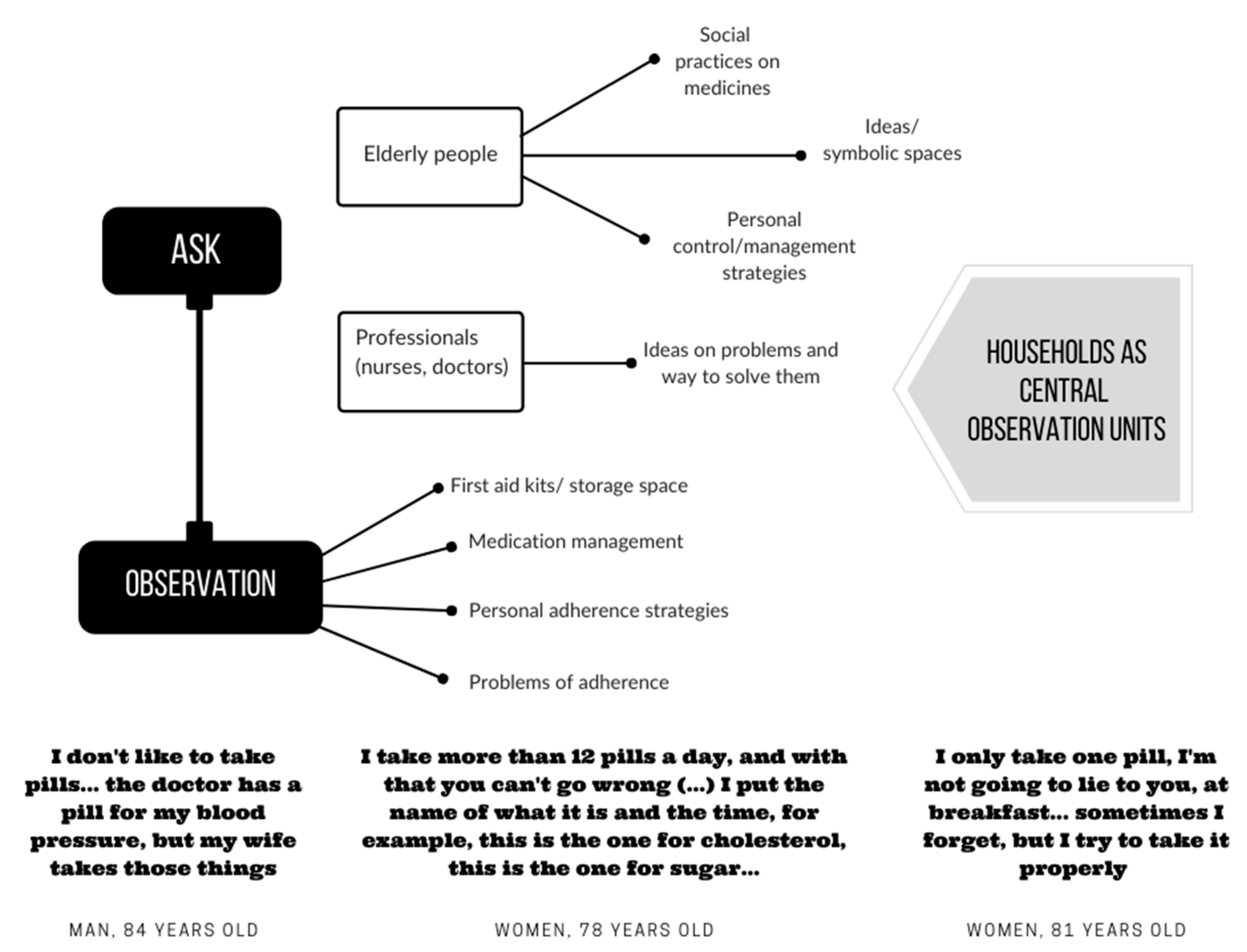
2.4.1. Participant Observation
2.4.2. Semi-Structured Interviews
2.4.3. Field Diary
2.5. Data Analysis
3. Results
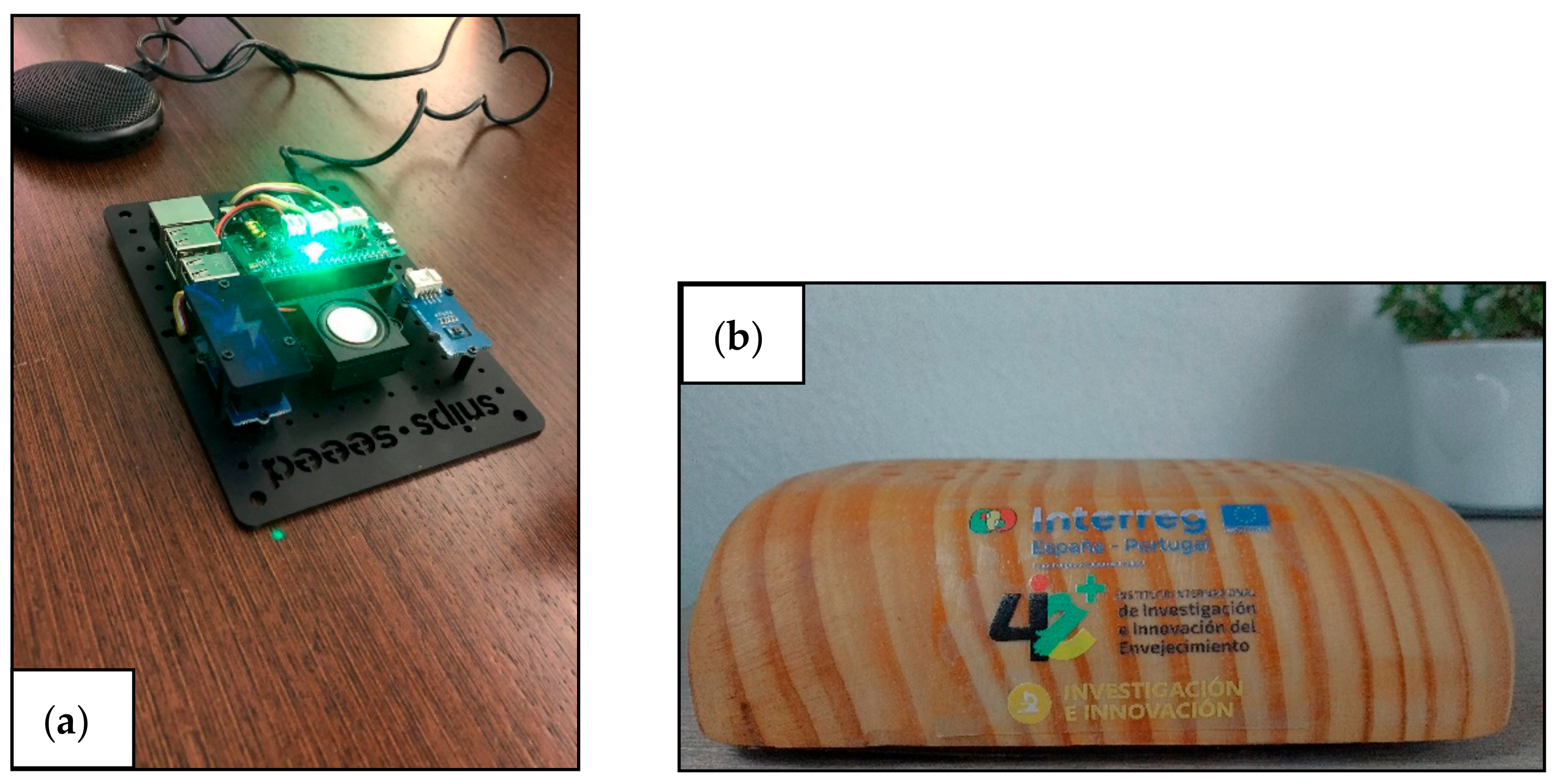
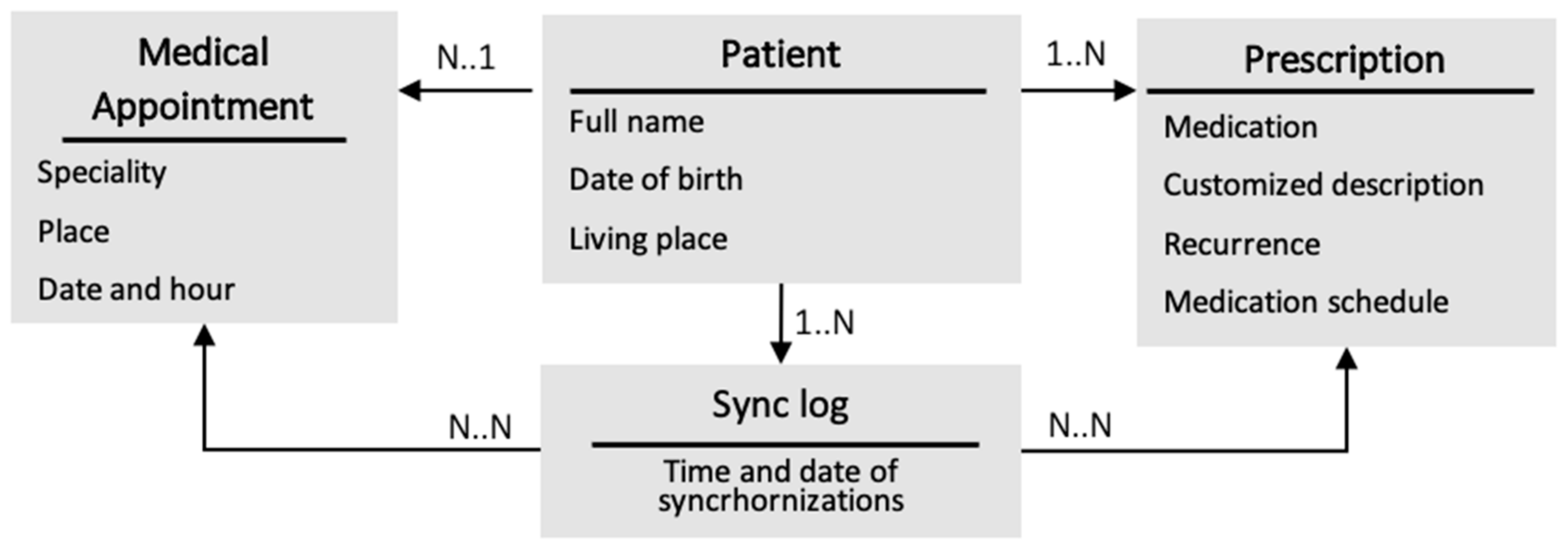
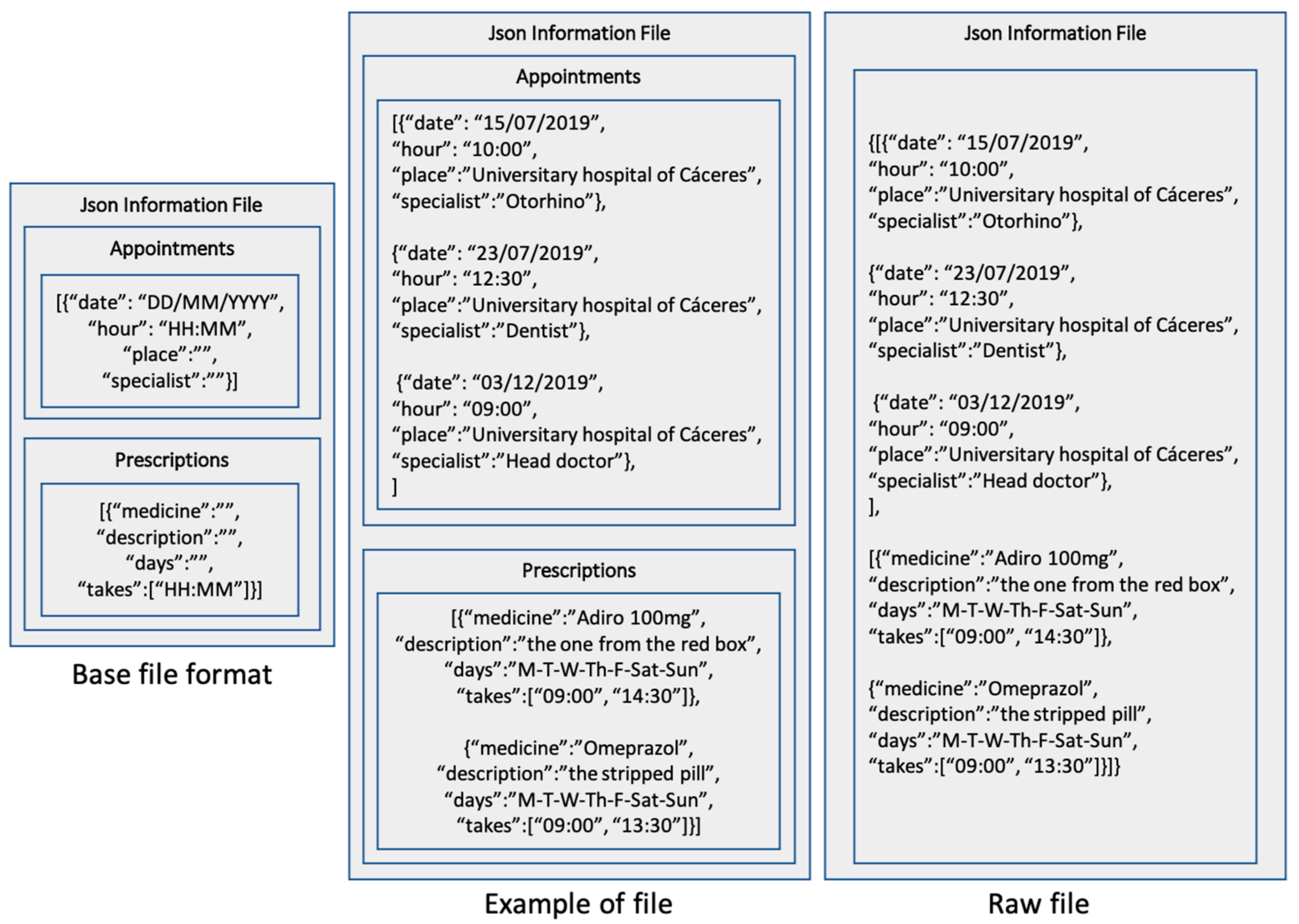
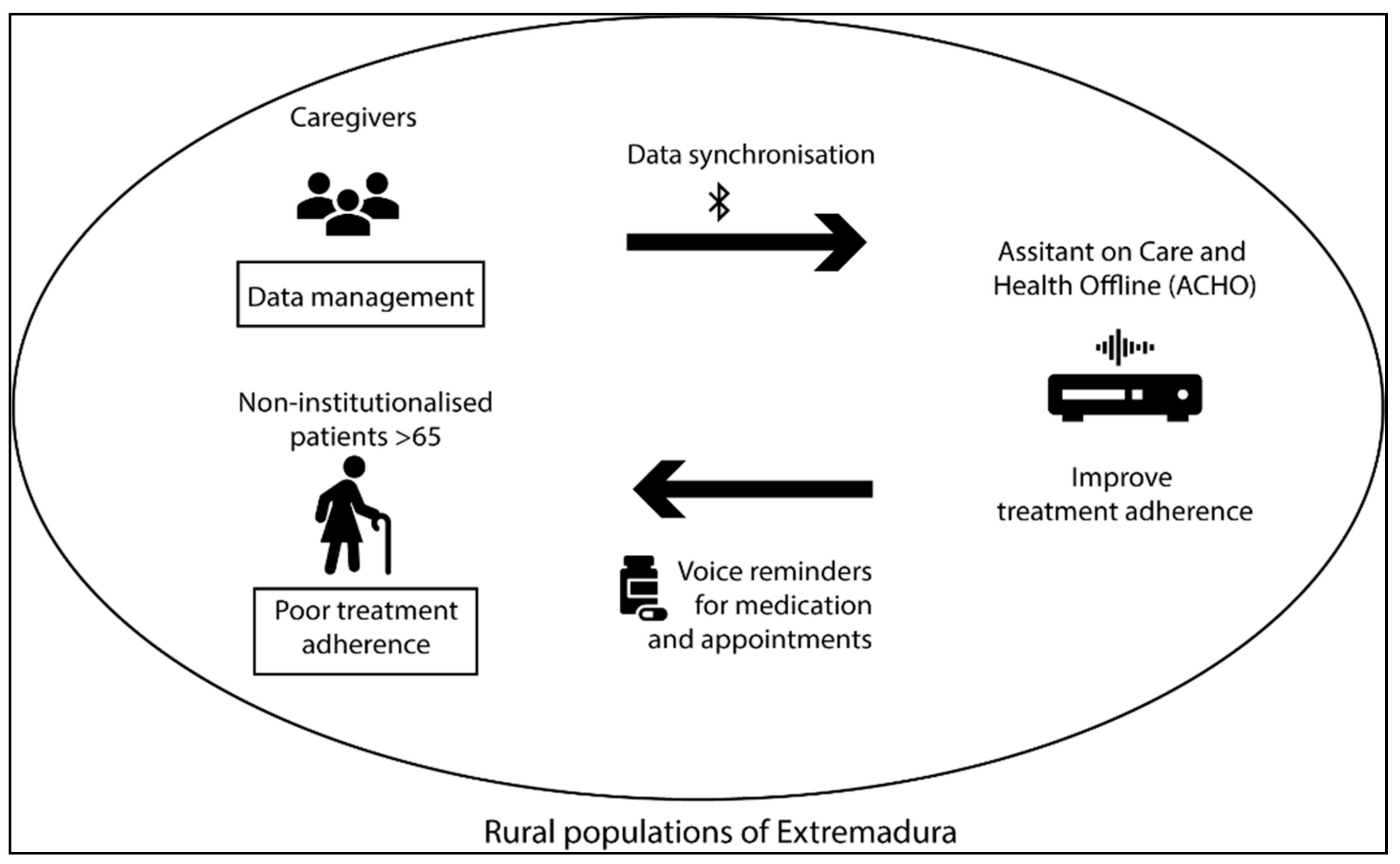
3.1. ACHO Design
3.2. Operation
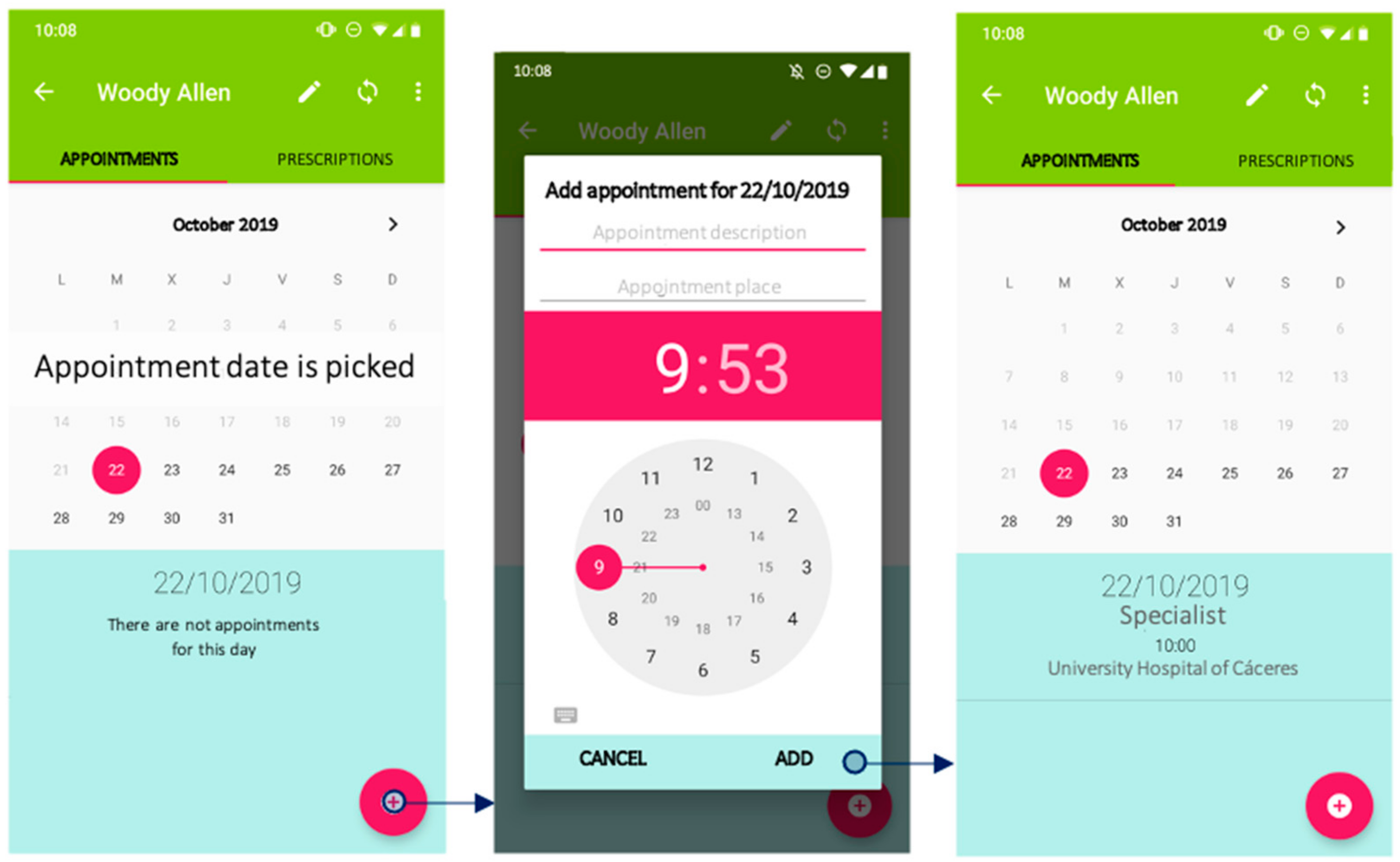
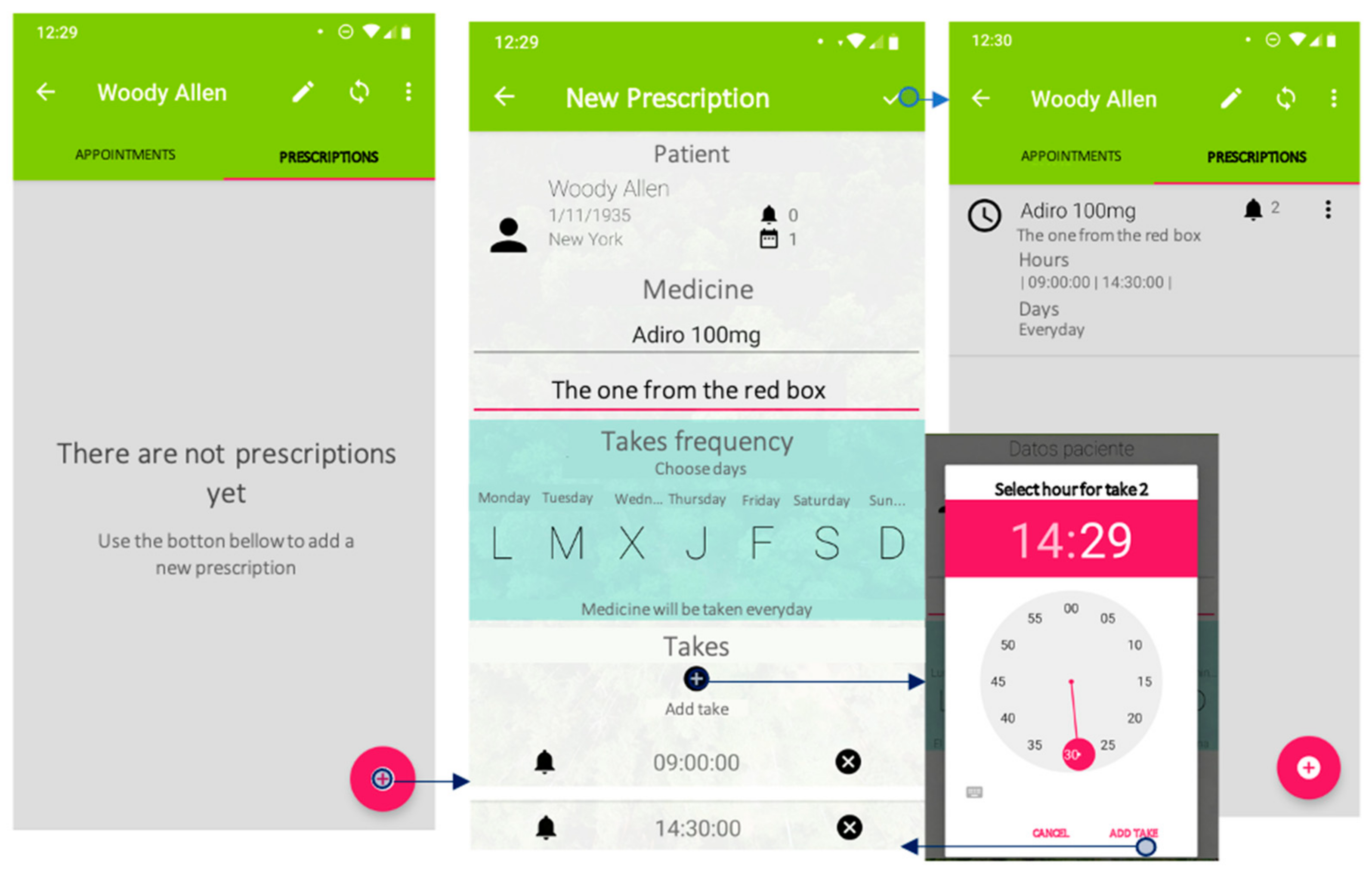
3.2.1. Mobile Application
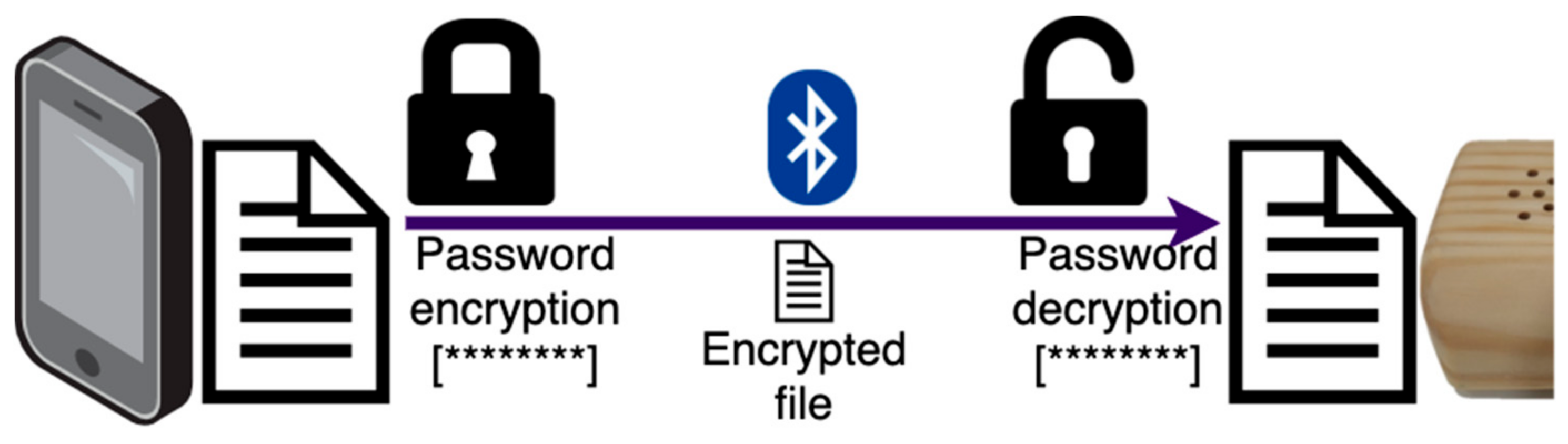
3.2.2. Voice Assistant
3.3. Originality of the Proposal
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eurostats. Estructura Demográfica y Envejecimiento de la Población. 2020. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing/es#:~:text=En%202018%2C%20casi%20la%20quinta,6%20%25%20de%20la%20poblaci%C3%B3n%20total (accessed on 8 January 2021).
- INE. Instituto Nacional de Estadística. Estadística del Padrón Continuo. 2019. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177012&menu=ultiDatos&idp=1254734710990 (accessed on 11 January 2021).
- European Comission. The 2015 Ageing Report Economic and Budgetary Projections for the 28 EU Member States (2013–2060) [Internet]; Economic and Financial Affairs. 2015. Available online: http://ec.europa.eu/economy_finance/publications/european_economy/2015/ee3_en.htm (accessed on 9 January 2021).
- Ávila, M.M.H.; Romaguera, M.R.; Hechavarria, H.G.; Hechavarria, A.G. The aging. Social and individual repercussion. Rev. Inf. Cient. 2018, 97, 1173–1188. [Google Scholar]
- Van De Kaa, D.J. The Idea of a Second Demographic Transition in Industrialized Countries. In Proceedings of the Sixth Welfare Policy Seminar of the National Institute of Population and Social Security, Tokyo, Japan, 29 January 2002; p. 34. [Google Scholar]
- Abellán García, A.; Aceituno Nieto, P.; Pérez Díaz, J.; Ramiro Fariñas, D.; Ayala García, A.; Pujol Rodríguez, R. Un Perfil de las Personas Mayores en España, 2017. Indicadores Estadísticos Básicos [Internet]; Informes Envejecimiento en Red. Madrid. 2017. Available online: https://bit.ly/3dQZaja (accessed on 15 December 2020).
- World Health Organization. Informe Sobre el Envejecimiento y la Salud; WHO: Geneve, Switzerland, 2015. [Google Scholar]
- The Lancet Public Health Editorial. Ageing: A 21st century public health challenge? Lancet Public Health 2017, 2, e297. [Google Scholar] [CrossRef]
- Rivero Jiménez, B.; García Perales, N.M.; Conde Caballero, D.; Muñoz González, B.; Calderón García, J.F.; Mariano Juarez, L. Loneliness Among Rural Elderly: Present and Future Public Health Challenges. In Handbook of Research on Health Systems and Organizations for an Aging Society; IGI Global: Hershey, PA, USA, 2020; pp. 48–61. [Google Scholar]
- Marengoni, A.; Winblad, B.; Karp, A.; Fratiglioni, L. Prevalence of chronic diseases and multimorbidity among the elderly population in Sweden. Am. J. Public Health 2008, 98, 1198–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, L.; Breuer, J.; Kostev, K. Prevalence of chronic diseases among older patients in German general practices. GMS Ger. Med. Sci. 2016, 14. [Google Scholar] [CrossRef]
- Mwangi, J.; Kulane, A.; Van Hoi, L. Chronic diseases among the elderly in a rural Vietnam: Prevalence, associated socio-demographic factors and healthcare expenditures. Int. J. Equity Health 2015, 14, 134. [Google Scholar] [CrossRef] [Green Version]
- Rosted, E.; Schultz, M.; Sanders, S. Frailty and polypharmacy in elderly patients are associated with a high readmission risk. Dan. Med. J. 2016, 63, A5274. [Google Scholar] [PubMed]
- Pesante-Pinto, J.L. Clinical pharmacology and the risks of polypharmacy in the geriatric patient. Phys. Med. Rehabil. Clin. 2017, 28, 739–746. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- Paci, J.F.; Alfaro, M.G.; Alonso, F.J.R.; San-Martin, M.I.F.; Litoral, G.P. Prescripción inadecuada en pacientes polimedicados mayores de 64 años en atención primaria. Aten. Primaria 2015, 47, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Roncoroni, J.; Tucker, C.M.; Wall, W.; Wippold, G.; Ratchford, J. Associations of Health Self-efficacy With Engagement in Health-Promoting Behaviors and Treatment Adherence in Rural Patients. Fam. Community Health 2019, 42, 109–116. [Google Scholar] [CrossRef]
- Rahmawati, R.; Bajorek, B. Factors affecting self-reported medication adherence and hypertension knowledge: A cross-sectional study in rural villages, Yogyakarta Province, Indonesia. Chronic. Illn. 2018, 14, 212–227. [Google Scholar] [CrossRef]
- Tuesca-Molina, R.; Guallar-Castillón, P.; Banegas-Banegas, J.R.; Regadera, A.G.-P. Determinantes del cumplimiento terapéutico en personas mayores de 60 años en España. Gac. Sanit. 2006, 20, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Dham, P.; Gupta, N.; Alexander, J.; Black, W.; Rajji, T.; Skinner, E. Community based telepsychiatry service for older adults residing in a rural and remote region-utilization pattern and satisfaction among stakeholders. BMC Psychiatry 2018, 18, 316. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.M. Medication non-adherence in the elderly: How big is the problem? Drugs Aging 2004, 21, 793–811. [Google Scholar] [CrossRef]
- Smith, D.; Lovell, J.; Weller, C.; Kennedy, B.; Winbolt, M.; Young, C.; Ibrahim, J. A systematic review of medication non-adherence in persons with dementia or cognitive impairment. PLoS ONE 2017, 12, e0170651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwlaat, R.; Wilczynski, N.; Navarro, T.; Hobson, N.; Jeffery, R.; Keepanasseril, A.; Agoritsas, T.; Mistry, N.; Iorio, A.; Jack, S.; et al. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2014, 11. [Google Scholar] [CrossRef]
- Carrillo, J.A. Consideraciones sobre la prescripción y utilización de fármacos en personas mayores. Rev. ROL Enferm. 2020, 43, 8–15. [Google Scholar]
- Yilmaz, F.; Colak, M.Y. Evaluation of inappropriate medication use and compliance in elderly people. Curr. Drug Saf. 2018, 13, 122–127. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; WHO: Geneve, Switzerland, 2003. [Google Scholar]
- Montenegro, A.J.N.; Luque, A.M.; Aurioles, E.M.; Verdú, B.T.; Moreno, C.L.; Correa, J.A.G.; En representación del grupo Polipresact. Adherencia al tratamiento en pacientes polimedicados mayores de 65 años con prescripción por principio activo. Aten. Primaria 2014, 46, 238–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagnasco, A.; Petralia, P.; Furnari, S.; Ghio, S.; Calza, S.; Sasso, L. Paediatric nurses’ perception of the child-family dyad’s autonomy in managing a chronic disease situation: The experience of an Italian Paediatric Department. J. Prev. Med. Hyg. 2013, 54, 124. [Google Scholar]
- Peñarrieta, M.I.; Kendall, T.; Martinez, N.; Rivera, A.M.; Gonzales, N.; Flores, F.; Angel, E.D. Adherencia al tratamiento antirretroviral en personas con VIH en Tamaulipas, México. Rev. Peru. Med. Exp. Salud Publica 2009, 26, 333–337. [Google Scholar]
- Martins, A.I.; Queirós, A.; Cerqueira, M.; Rocha, N.; Teixeira, A. The international classification of functioning, disability and health as a conceptual model for the evaluation of environmental factors. In Procedia Computer Science; Elsevier B.V.: Amsterdam, The Netherlands, 2012; pp. 293–300. [Google Scholar]
- Checchi, K.D.; Huybrechts, K.F.; Avorn, J.; Kesselheim, A.S. Electronic medication packaging devices and medication adherence: A systematic review. JAMA 2014, 312, 1237–1247. [Google Scholar] [CrossRef] [Green Version]
- Hartman, L.; Lems, W.F.; Boers, M. Outcome measures for adherence data from a medication event monitoring system: A literature review. J. Clin. Pharm. Ther. 2019, 44, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Chamorro, R.; García-Jiménez, E.; Busquets Gil, A.; Rodríguez Chamorro, A.; Pérez Merino, E.; Dáder, F.; Martínez Martínez, F. Herramientas para identificar el incumplimiento farmacoterapéutico desde la farmacia comunitaria. Pharm. Care España 2009, 11, 183–191. [Google Scholar]
- Guber, R. La Etnografía: Método, Campo y Reflexividad; Siglo XXI: Buenos Aires, Argentina, 2011. [Google Scholar]
- Hammersley, M.; Atkinson, P. Etnografía. In Métodos de Investigación; Paidós: Barcelona, Spain, 1994; p. 297. [Google Scholar]
- Velasco, H.; Díaz de Rada, Á. La Lógica de la Investigación Etnográfica; Trotta: Madrid, Spain, 2006; p. 303. [Google Scholar]
- Fadrique, L.X.; Rahman, D.; Vaillancourt, H.; Boissonneault, P.; Donovska, T.; Morita, P.P. Overview of Policies, Guidelines, and Standards for Active Assisted Living Data Exchange: Thematic Analysis. JMIR mHealth uHealth 2020, 8, e15923. [Google Scholar] [CrossRef]
- Asociación Médica Mundial. Declaración de Helsinki. In Principios Éticos Para Las Investigaciones Médicas en Seres Humanos; Asociación Médica Mundial: Seúl, Korea, 2008. [Google Scholar]
- National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. Belmont Report: Ethical Principles and Guidelines for Research Involving Human Subjects; U.S. Government Department of Health, Education and Welfare: Washington, DC, USA, 1979. [Google Scholar]
- Instituto Nacional de Estadística de España (INE). Estadística del Padrón Continuo. Datos Provisionales a 1 de Enero de 2020 [Internet]. 2020. Available online: https://www.ine.es/dynt3/inebase/index.htm?type=pcaxis&path=/t20/e245/p04/provi&file=pcaxis&dh=0&capsel=0 (accessed on 11 January 2021).
- Creswell, J.W. Qualitative Inquiry & Research Design; Sage Publications: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Strauss, A.; Corbin, J. Bases de la investigación cualitativa. In Técnicas y Procedimientos Para Desarrollar la Teoría Fundamentada; Sage Publications: Antioquia, Colombia, 2004; p. 340. [Google Scholar]
- Shopes, L. Formas de entrevistar. Hist. Antropol. Fuentes Orales 2001, 25, 132–142. [Google Scholar]
- Rivero-Jiménez, B.; Conde-Caballero, D.; Mariano-Juárez, L. Health and Nutritional Beliefs and Practices among Rural Elderly Population: An Ethnographic Study in Western Spain. Int. J. Environ. Res. Public Health 2020, 17, 5923. [Google Scholar] [CrossRef]
- Shah, A. Ethnography? Participant observation, a potentially revolutionary praxis. HAU J. Ethnogr. Theory 2017, 7, 45–59. [Google Scholar] [CrossRef]
- Denzin, N.K.; Lincoln, Y.S. Handbook of Qualitative Research; SAGE Publications: London, UK, 1994. [Google Scholar]
- Brinkman, S.; Kvale, S. Interviews: Learning the Craft of Qualitative Research Interviewing; SAGE: London, UK, 2015. [Google Scholar]
- Neumann, C.B.B.; Neumann, I.B. Interview Techniques. In Power, Culture and Situated Research Methodology; Palgrave MacMillan: London, UK, 2018. [Google Scholar]
- Casado i Aijón, I. Itinerarios terapéuticos. Propuesta para la aplicabilidad en la etnografía. GRAFO Work Pap. 2016, 5, 1–30. [Google Scholar]
- Guerin, G.D.; Rossoni, E.; Bueno, D. Itinerários terapêuticos de usuários de medicamentos de uma unidade de Estratégia de Saúde da Família. Cien Saude Colet 2012, 17, 3003–3010. [Google Scholar] [CrossRef] [Green Version]
- Venturiello, M.P. Itinerario terapéutico de las personas con discapacidad y mediaciones en el cuidado de la salud: La mirada de los familiares. Physis. Rev. Saúde Coletiva 2012, 22, 1063–1083. [Google Scholar] [CrossRef] [Green Version]
- Peacock, J.L. Method. In The Anthropological Lens; Cambridge University Press: London, UK, 1986. [Google Scholar]
- Pope, C. Qualitative research in health care: Analysing qualitative data. BMJ 2000. [Google Scholar] [CrossRef]
- Queirós, A.; Silva, A.; Alvarelhão, J.; Rocha, N.P.; Teixeira, A. Usability, accessibility and ambient-assisted living: A systematic literature review. Univ. Access. Inf. Soc. 2015, 14, 57–66. [Google Scholar] [CrossRef]
- Mills, C.W. La Imaginación Sociológica; Oxford University Press: Nueva York, NY, USA, 1959. [Google Scholar]
- Szanton, S.L.; Leff, B.; Wolff, J.L.; Roberts, L.; Gitlin, L.N. Home-based care program reduces disability and promotes aging in place. Health Aff. 2016, 35, 1558–1563. [Google Scholar] [CrossRef] [PubMed]
- Ruanova, B.F.; Tenorio-Laranga, J.; Jurado, A.A.; Hernaiz, J.X.L.; Justo, R.; Barañano, M.I.T. Innovation on home-based care services. Int. J. Integr. Care 2019. [Google Scholar] [CrossRef] [Green Version]
- Woods, O.; Kong, L. New cultures of care? The spatio-temporal modalities of home-based smart eldercare technologies in Singapore. Soc. Cult. Geogr. 2020, 21, 1307–1327. [Google Scholar] [CrossRef]
- Jiménez Buñuales, M.; González Diego, P.; Martín Moreno, J.M. La clasificación internacional del funcionamiento de la discapacidad y de la salud (CIF) 2001. Rev. Esp. Salud Publica 2002, 76, 271–279. [Google Scholar] [PubMed]
- Coucke, A.; Saade, A.; Ball, A.; Bluche, T.; Caulier, A.; Leroy, D.; Doumouro, C.; Gisselbrecht, T.; Caltagirone, F.; Lavril, T.; et al. Snips Voice Platform: An embedded Spoken Language Understanding system for private-by-design voice interfaces. arXiv 2018, arXiv:1805.10190. [Google Scholar]
- Jesús-Azabal, M.; Rojo, J.; Moguel, E.; Flores-Martin, D.; Berrocal, J.; Garcia-Alonso, J.; Murillo, J.M. Voice Assistant to Remind Pharmacologic Treatment in Elders. In International Workshop on Gerontechnology; Springer: Cham, Switzerland, 2019; pp. 123–133. [Google Scholar]
- Granger, B.B.; Bosworth, H. Medication adherence: Emerging use of technology. Curr. Opin. Cardiol. 2011, 26, 279. [Google Scholar] [CrossRef] [Green Version]
- Reach, G. Can technology improve adherence to long-term therapies? J. Diabetes Sci. Technol. 2009, 3, 492–499. [Google Scholar] [CrossRef] [Green Version]
- Mateo, M.M.; Herrera, D.G. Adherencia terapéutica en pacientes con diabetes mellitus tipo II y el uso de la tecnologia móvil básica: Una revisión sistemática. Rev. Esp. Commun. Salud 2019, 10, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Minaam, D.S.A.; Abd-ELfattah, M. Smart drugs: Improving healthcare using smart pill box for medicine reminder and monitoring system. Futur. Comput. Inform. J. 2018, 3, 443–456. [Google Scholar] [CrossRef]
- Kannisto, K.A.; Koivunen, M.H.; Välimäki, M.A. Use of mobile phone text message reminders in health care services: A narrative literature review. J. Med. Internet. Res. 2014, 16, e222. [Google Scholar] [CrossRef]
- Strandbygaard, U.; Thomsen, S.F.; Backer, V. A daily SMS reminder increases adherence to asthma treatment: A three-month follow-up study. Respir. Med. 2010, 104, 166–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, H.; Kumar, V.; Doros, G.; Farmer, E.; Drainoni, M.L.; Rybin, D.; Myung, D.; Jackson, J.; Backman, E.; Stanic, A.; et al. Randomized controlled trial of a personalized cellular phone reminder system to enhance adherence to antiretroviral therapy. AIDS Patient Care STDS 2011, 25, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, A.; McGruder, H.F.; Wu, A.W.; Celano, S.A.; Skolasky, R.L.J.; Selnes, O.A.; Huang, I.C.; McArthur, J.C. A programmable prompting device improves adherence to highly active antiretroviral therapy in HIV-infected subjects with memory impairment. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2005, 41, 875–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Costa, F.A.; Guerreiro, J.P.; de Melo, M.N.; Miranda AD, C.; Martins, A.P.; Garçāo, J.; Madureira, B. Effect of reminder cards on compliance with antihypertensive medication. Int. J. Pharm. Pract. 2005, 13, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Christensen, A.; Christrup, L.L.; Fabricius, P.E.; Chrostowska, M.; Wronka, M.; Narkiewicz, K.; Hansen, E.H. The impact of an electronic monitoring and reminder device on patient compliance with antihypertensive therapy: A randomized controlled trial. J. Hypertens. 2010, 28, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Ho, L.Y.; Camejo, L.; Kahook, M.Y.; Noecker, R. Effect of audible and visual reminders on adherence in glaucoma patients using a commercially available dosing aid. Clin. Ophthalmol. 2008, 2, 769. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Diffusion of eHealth: Making Universal Health Coverage Achievable: Report of the Third Global Survey on eHealth; World Health Organization: Geneve, Switzerland, 2017. [Google Scholar]
- Lorca-Cabrera, J.; Marti-Arques, R.; Albacar-Riobóo, N.; Raigal-Aran, L.; Roldan-Merino, J.; Ferré-Grau, C. Mobile Applications for Caregivers of Individuals with Chronic Conditions and/or Diseases: Quantitative Content Analysis. Int. J. Med. Inform. 2020, 104310. [Google Scholar] [CrossRef]
- Franco Bonal, A.; Silva Valido, J.A.; Soto Martinez, O.; Franco Bonal, A. Evaluación de adherencia terapéutica antihipertensiva en el adulto mayor. Rev. Inf. Cient. 2018, 97, 1124–1134. [Google Scholar]
- Debon, R.; Coleone, J.D.; Bellei, E.A.; De Marchi, A.C.B. Mobile health applications for chronic diseases: A systematic review of features for lifestyle improvement. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2507–2512. [Google Scholar] [CrossRef]
- Krauskopf, P.B. Evaluation of CDC Opioid Prescribing and Medisafe Apps. J. Nurse Pract. 2017, 13, e293–e295. [Google Scholar] [CrossRef]
- Logan, A.G.; Jassal, S.V. Building a Stronger Care Loop Through mHealth Technology. JAMA Intern. Med. 2018, 178, 809–811. [Google Scholar] [CrossRef]
- Hara, H.; Mihara, M.; Iida, T.; Narushima, M.; Todokoro, T.; Yamamoto, T.; Koshima, I. Blood glucose measurement for flap monitoring to salvage flaps from venous thrombosis. J. Plast. Reconstr. Aesthetic. Surg. 2012, 65, 616–619. [Google Scholar] [CrossRef]
- Wagner, S.; Nielsen, C. OpenCare project: An open, flexible and easily extendible infrastructure for pervasive healthcare assisted living solutions. In Proceedings of the 2009 3rd International Conference on Pervasive Computing Technologies for Healthcare, London, UK, 1–3 April 2009; pp. 1–10. [Google Scholar]
- Sá, M.C.; Oliveira, A.; Nabais, A. The importance of Information and Communication Technologies (ICT) to promote information, self-care and empowerment in patients with chronic diseases. In Proceedings of the Edulearn 18 10th International Conference on Education and New Learning Technology, Palma, Spain, 2–4 July 2018; pp. 7993–7998. [Google Scholar]
- Oscalices, M.I.L.; Okuno, M.F.P.; Lopes, M.C.B.T.; Campanharo, C.R.V.; Batista, R.E.A. Discharge guidance and telephone follow-up in the therapeutic adherence of heart failure: Randomized clinical trial. Rev. Lat. Am. Enfermagem. 2019, 27. [Google Scholar] [CrossRef]
- Mitzner, T.L.; Boron, J.B.; Fausset, C.B.; Adams, A.E.; Charness, N.; Czaja, S.J.; Dijkstrae, K.; Fiska, A.D.; Rogersa, W.A.; Sharitf, J. Older adults talk technology: Technology usage and attitudes. Comput. Hum. Behav. 2010, 26, 1710–1721. [Google Scholar] [CrossRef] [Green Version]
- Harrefors, C.; Axelsson, K.; Sävenstedt, S. Using assistive technology services at differing levels of care: Healthy older couples’ perceptions. J. Adv. Nurs. 2010, 66, 1523–1532. [Google Scholar] [CrossRef]
- Ennis, A.; Rafferty, J.; Synnott, J.; Cleland, I.; Nugent, C.; Selby, A.; McIlroy, S.; Berthelot, A.; Masci, G. A Smart Cabinet and Voice Assistant to Support Independence in Older Adults. In Proceedings of the International Conference on Ubiquitous Computing and Ambient Intelligence, Philadelphia, PA, USA, 7–10 November 2017; pp. 466–472. [Google Scholar]
- Dojchinovski, D.; Ilievski, A.; Gusev, M. Interactive home healthcare system with integrated voice assistant. In Proceedings of the 2019 42nd International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 20–24 May 2019; pp. 284–288. [Google Scholar]
- Shalini, S.; Levins, T.; Robinson, E.L.; Lane, K.; Park, G.; Skubic, M. Development and Comparison of Customized Voice-Assistant Systems for Independent Living Older Adults. In Proceedings of the International Conference on Human-Computer Interaction, Paphos, Cyprus, 2–6 September 2019; pp. 464–479. [Google Scholar]
- Pradhan, A.; Mehta, K.; Findlater, L. “Accesibility Came by Accident”: Use of Voice-Controlled Intelligent Personal Assistans vy people with Dissabilities. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems—CHI ’18, New York, NY, USA, 8–13 May 2018; ACM Press: New York, NY, USA, 2018; pp. 1–13. [Google Scholar]
- Miner, A.S.; Milstein, A.; Schueller, S.; Hegde, R.; Mangurian, C.; Linos, E. Smartphone-Based Conversational Agents and Responses to Questions About Mental Health, Interpersonal Violence, and Physical Health. JAMA Intern. Med. 2016, 176, 619. [Google Scholar] [CrossRef]
- Pradhan, A.; Lazar, A.; Findlater, L. Use of intelligent voice assistants by older adults with low technology use. ACM Trans. Comput. Interact. 2020, 27, 1–27. [Google Scholar] [CrossRef]
- Vidal, E.; Acuña, J.; Rosas, D.; Castro, E. Asistente de voz autónomo: Un soporte de adherencia a tratamientos médicos. Rev. Ibérica Sist. Technol. Inf. 2020, 105–113. [Google Scholar]
- Jesús-Azabal, M.; Medina-Rodríguez, J.A.; Durán-García, J.; García-Pérez, D. Remembranza pills: Using alexa to remind the daily medicine doses to elderly. In Communications in Computer and Information Science; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Safi, S.; Thiessen, T.; Schmailzl, K.J.G. Acceptance and resistance of new digital technologies in medicine: Qualitative study. JMIR Res. Protoc. 2018, 7, e11072. [Google Scholar] [CrossRef]
- Kalimullah, K.; Sushmitha, D. Influence of Design Elements in Mobile Applications on User Experience of Elderly People. In Procedia Computer Science; Elsevier B.V.: Amsterdam, The Netherlands, 2017; pp. 352–359. [Google Scholar]
- Hoy, M.B. Alexa, Siri, Cortana, and More: An Introduction to Voice Assistants. Med. Ref. Serv. Q. 2018, 37, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística de España. Población Que Usa Internet de Manera Frecuente (al Menos Una Vez a la Semana). Available online: https://www.ine.es/ss/Satellite?L=es_ES&c=INESeccion_C&cid=1259925528559&p=%5C&pagename=ProductosYServicios%2FPYSLayout¶m1=PYSDetalle¶m3=1259924822888 (accessed on 8 January 2021).
- Romo, N.M. Escuela, medio rural e igualdad de oportunidades: ¿un trío imposible? Doc. Soc. 2007, 135–154. [Google Scholar]
- Kelker, K.A. Family Guide to Assistive Technology: Parents, Let’s Unite for Kids (PLUK); U.S. Department of Education: Billings, MT, USA, 1997. [Google Scholar]
- Nuance Healthcare. Will Virtual Assistants Propel the Future of Medicine. 2013. Available online: https://www.healthcareitnews.com/infographic/will-virutal-assistants-propel-future-medicine (accessed on 17 January 2021).
- Delgado, J.A.M.; Alonso, F.J.M.; Boquet, E.M.; de Tomás, J.F.Á.; Diez, J.M.C. Competencias digitales clave de los profesionales sanitarios. Educ. Méd. 2020, 21, 338–344. [Google Scholar] [CrossRef]
- Salman, H.; Wan Ahmad, W.; Sulaiman, S. Usability Evaluation of the Smartphone UserInterface in Supporting Elderly UsersFrom Experts’ Perspective. IEEE Access. 2018, 6, 22578–22591. [Google Scholar] [CrossRef]
- Bartlett Ellis, R.J.; Knisely, M.R.; Boyer, K.; Pike, C. Pillbox intervention fidelity in medication adherence research: A systematic review. Nurs. Outlook 2017. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, J.S.; Ramos, C.; Wünsche, B.C.; Lutteroth, C. Designing a web-based telehealth system for elderly people: An interview study in New Zealand. In Proceedings of the 2011 24th International Symposium on Computer-Based Medical Systems (CBMS), Bristol, UK, 27–30 June 2011; pp. 1–6. [Google Scholar]
- McCabe, R.; Healey, P.G.T. Miscommunication in Doctor–Patient Communication. Top. Cogn. Sci. 2018, 10, 409–424. [Google Scholar] [CrossRef] [Green Version]
- Wolf, M.S.; Davis, T.C.; Curtis, L.M.; Bailey, S.C.; Knox, J.A.P.; Bergeron, A.; Abbet, M.; Shrank, W.H.; Parker, R.M.; Wood, A.J. A Patient-Centered Prescription Drug Label to Promote Appropriate Medication Use and Adherence. J. Gen. Intern. Med. 2016, 31, 1482–1489. [Google Scholar] [CrossRef]
- Metcalf, D.; Milliard, S.T.J.; Gomez, M.; Schwartz, M. Wearables and the internet of things for health: Wearable, interconnected devices promise more efficient and comprehensive health care. IEEE Pulse 2016, 7, 35–39. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Technique | Empirical Material Obtained |
|---|---|
| Field diary | Notes taken during fieldwork. Information on context and on additional topics |
| Participant observation | Observation of everyday activities, particularly regarding medication management (intake schedule, storage, re-naming practices) |
| Informal conversations | Conducted independently from the interview guide, these can open alternative epistemological windows |
| Semi-structured interviews | Categories include issues regarding treatment adherence among chronically ill patients |
| Categories | Questions |
|---|---|
| Problems with therapeutic itineraries | Do you have problems when trying to make an appointment? What is the procedure? Is it easy? Why does it take so long/so little, and why do you think that is? Do you have any problems in accessing the doctor’s office? How would you describe your relationship with your doctor? |
| Treatment and different itineraries | Did you start treating your illness before you were diagnosed? How do you think your health problem can be treated? What previous health problems have you had, and how did you deal with them? How do you feel about the care you have received from your doctor? Tell us about your search for solutions or treatments. |
| Problems with medication | What medications do you take? Do you always take your medication? Why do you sometimes forget? Do you have any help to remember to take your medication? Do your relatives help you to remember? Does forgetting to take your medication result in health problems? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conde-Caballero, D.; Rivero-Jiménez, B.; Cipriano-Crespo, C.; Jesus-Azabal, M.; Garcia-Alonso, J.; Mariano-Juárez, L. Treatment Adherence in Chronic Conditions during Ageing: Uses, Functionalities, and Cultural Adaptation of the Assistant on Care and Health Offline (ACHO) in Rural Areas. J. Pers. Med. 2021, 11, 173. https://doi.org/10.3390/jpm11030173
Conde-Caballero D, Rivero-Jiménez B, Cipriano-Crespo C, Jesus-Azabal M, Garcia-Alonso J, Mariano-Juárez L. Treatment Adherence in Chronic Conditions during Ageing: Uses, Functionalities, and Cultural Adaptation of the Assistant on Care and Health Offline (ACHO) in Rural Areas. Journal of Personalized Medicine. 2021; 11(3):173. https://doi.org/10.3390/jpm11030173
Chicago/Turabian StyleConde-Caballero, David, Borja Rivero-Jiménez, Carmen Cipriano-Crespo, Manuel Jesus-Azabal, Jose Garcia-Alonso, and Lorenzo Mariano-Juárez. 2021. "Treatment Adherence in Chronic Conditions during Ageing: Uses, Functionalities, and Cultural Adaptation of the Assistant on Care and Health Offline (ACHO) in Rural Areas" Journal of Personalized Medicine 11, no. 3: 173. https://doi.org/10.3390/jpm11030173