The Effects of Haemophilia on the Postural Control of Adolescents


Groupe de Recherche sur les Affections Neuro-musculo-squelettiques (GRAN), Department of Science and Physical Activity, University of Québec at Trois-Rivières, 3351 Boulevard des Forges, CP 500, Trois-Rivières, QC G9A 5H7, Canada
*
Author to whom correspondence should be addressed.
J. Funct. Morphol. Kinesiol. 2017, 2(3), 24; https://doi.org/10.3390/jfmk2030024
Submission received: 23 June 2017
/
Revised: 10 July 2017
/
Accepted: 10 July 2017
/
Published: 12 July 2017
(This article belongs to the Special Issue New Advances in Human Posture and Movement)
Abstract
:A small number of studies have reported that children and adults with haemophilia have impaired balance control and show faster body sway during upright stance than healthy individuals. A decrease of somatosensory information due to multiple bleedings has been suggested to explain this difference. Therefore, the objective of this study was to examine if haemophilia is related to a decreased balance control under altered visual and proprioceptive conditions in male adolescents. Postural sway of healthy (n = 12, Age = 14.8 ± 1.4 years; BMI = 19.8 ± 1.8 kg/m2) and haemophiliac (n = 8, Age = 15.0 ± 1.4 years; BMI = 20.4 ± 3.2 kg/m2) male adolescents was measured with a force platform for normal quiet stance lasting 30 s with open and closed eyes on hard and foam floor conditions. The ANOVA revealed a significant Group × Vision × Proprioception (F(1,18) = 5.861, p < 0.05) interaction. Both groups showed an increased centre of pressure (COP) speed when vision and proprioception are challenged. Planned comparisons revealed that the haemophiliac group oscillated at a faster COP speed than the healthy group when vision is altered in hard floor (1.11 ± 0.27 versus 0.76 ± 0.19 cm/s; p < 0.05) and foam floor (6.83 ± 1.68 versus 4.89 ± 1.05 cm/s; p < 0.01) conditions. More important, haemophiliac adolescents were more disturbed by the proprioceptive condition and had a significantly higher COP speed on the foam even if vision is available (3.02 ± 0.47 versus 2.34 ± 0.45 cm/s; p < 0.05) compared to the healthy adolescents. In conclusion, haemophilia clearly affects postural control in altered sensory conditions. Our results suggest that haemophilia has a negative impact on the capacity of male adolescents to adequately use proprioceptive information for posture control.
1. Introduction
Human standing is a fundamental part of the activities of daily living and is essentially characterized by sway of the whole body about the ankle joints [1]. Maintaining upright balance is controlled primarily by the calf muscle, which counteracts the destabilizing effect of gravity [2]. It has been reported that passive stiffness and open loop mechanisms contribute to the generation of the muscle activity required for stance control [3], which depends on a coordinated effort of the sensory systems (visual, vestibular, and proprioceptive systems). Consequently, sensory integration from vision, proprioception, and vestibular organ plays an essential role in quasi-static and dynamic postural control, contributing to the organization and selection of an appropriate motor response when balance is challenged [4]. Deficits in these systems result in impaired balance control and have been clearly identified as a risk factor for falls [5,6,7].
Haemophilia is a medical condition caused by a hereditary lack of a coagulation factor (Haemophilia A/factor VIII and Haemophilia B/factor IX), and haemophiliac individuals present a severely reduced ability of the blood to clot, which results in a longer bleeding time after an injury [8]. Common physical problems have been identified for individuals with haemophilia, and include intra-articular and intramuscular bleeding, which can cause joint arthritis, limb pain, muscle weakness, muscle atrophy, loss of proprioception, and lack of joint flexibility [9,10,11]. It has been suggested that these impairments—especially those related to the lower limbs—may alter the postural control, leading to balance dysfunction [9,12,13]. To our knowledge, only four studies have investigated the effects of haemophilia on postural control [9,10,13,14]. All of these studies reported that postural stability is affected by haemophilia in adults [9,10,13] and in children [14]. The authors of these studies have hypothesized that the alteration of the postural control observed in their haemophiliac subjects could be related to a deficit in the proprioceptive inputs involved in the organization of the balance control.
The manipulation of sensory information gives an estimation of the importance of this information for posture control, in addition to indicating how the central nervous system adapts and reorganizes information provided by the remaining sources of sensory information [15]. We hypothesized that haemophiliac adolescents would have even greater difficulty controlling balance than healthy adolescents under altered visual and proprioceptive conditions due to a deficit of proprioceptive information needed for postural control. Therefore, the objective of this study was to examine if haemophilia is associated with a decreased postural stability in male adolescents.
2. Materials and Methods
Twenty male adolescents aged between 13 and 17 years were separated into two groups: 12 healthy subjects and 8 haemophiliac subjects (2 subjects with severe haemophilia A/Factor VIII < 0.01 IU mL−1 and 6 subjects with moderate haemophilia A/Factor VIII 0.01–0.05 IU mL−1). All haemophiliac adolescents had at least four haemarthrosis in a 6-month interval in a joint of the lower limbs. Haemophiliac adolescents presenting neurologic deficits and chronic pain syndrome were excluded. Haemophiliac adolescents reporting bleeding in the joints or in the muscles the week prior to the postural assessment were not included. Healthy adolescents were recruited based on the absence of musculoskeletal or neurological disorders. Adolescents presenting diabetes, cancer, six-month post-operative condition, psychotropic medication use, and cognitive issues were also excluded. All adolescents participated in the physical education programme of their school twice a week and in a sports activity at least once a week, except for one adolescent of the haemophiliac group. All haemophiliac adolescents were involved in a home exercise programme targeting walking and running at least twice a week. All participants and their parents gave their written informed consent to participate in this study, which was approved by the University of Québec at Trois-Rivières Ethics Committee (CER-15-211-07.104, 17, February, 2016).
Balance control was evaluated with a force platform (model no. FP4060, Bertec Corporation, Columbus, OH, USA). Subjects stood barefoot on the platform with their feet 10 cm apart. The subjects were asked to maintain a stable posture while fixating on a reference point located at eye level (1.5 m in front of them). The arms were held alongside the body. They performed seven trials in four different conditions: (1) control vision (eyes opened) and normal surface (platform surface), referred to as vision/hard floor condition; (2) altered vision (without vision) and normal surface, referred to as no vision/hard floor condition; (3) normal vision and altered surface, referred to as vision/foam floor condition; and (4) altered vision and altered surface, referred to as no vision/foam floor condition. For the foam floor condition, a foam rubber BalancePad® (AlcanAirex, HerexC70.40®, Sins, Switzerland) was inserted between the platform surface and the soles of the subject’s feet, and was used to alter the compliance of the supporting surface [16,17]. The pad measured 500 × 410 mm2, with a thickness of 60 mm and a density of 57 kg/m3. The addition of a foam support surface alters the reliability of the somatosensory contributions to posture control. All trials lasted 30 s and were initiated with the eyes opened, representing a total of 28 trials per subject. Subjects were able to rest midway through the experiment. An assistant helped throughout the session to ensure that procedures were adequately followed and that foot position was constant across all trials.
Antero-posterior and medio-lateral coordinates of the centre of pressure (COP) were determined from the ground reaction forces recorded at 100 Hz (12-bit A/D conversion). Before computing the COP displacement, the force data were digitally filtered (Butterworth fourth-order, 7 Hz low-pass cut-off frequency with dual-pass to remove phase shift). To evaluate the ability of the participants to control their balance, the mean speed of the COP was calculated (COP speed). The COP speed corresponds to the cumulative distance over the sampling period and constitutes a good index of activity required to maintain stability [18,19], with a faster speed indicating a less-stable individual. It is considered as a sensitive and discriminative variable of stability [20,21]. All computations were performed using Matlab 7.0 (The MathWorks, Natick, MA, USA).
Statistica software 7.0 (Statsoft, Inc, Tulsa, OK, USA) was used for all analyses. The Kolmogorov–Smirnov test was used to verify if all data were normally distributed. Analyses of variance (ANOVAs) were used to compare groups for age, height, weight, and body mass index (BMI). Balance control measures were submitted to ANOVAs contrasting groups (healthy and haemophiliac groups) × vision conditions (vision and no vision) × proprioceptive conditions (hard floor and foam floor conditions) with repeated measures on the two last factors. The Wilks’ Lambda statistical test was used to assess the null hypothesis. A post hoc test, the Newman–Keuls method, was used to assess interactive effects of intra-subject and inter-subject factors. Significance level was set at p < 0.05.
3. Results
3.1. Anthropometric Characteristics
The anthropometric characteristics of the two participant groups are presented in Table 1. There is no significant difference between groups for Age (F(1,18) = 0.067; p = 0.798), Height (F(1,18) = 0.343; p = 0.565), Weight (F(1,18) = 0.024; p = 0.879), or BMI (F(1,18) = 0.354; p = 0.560).
3.2. COP Speed
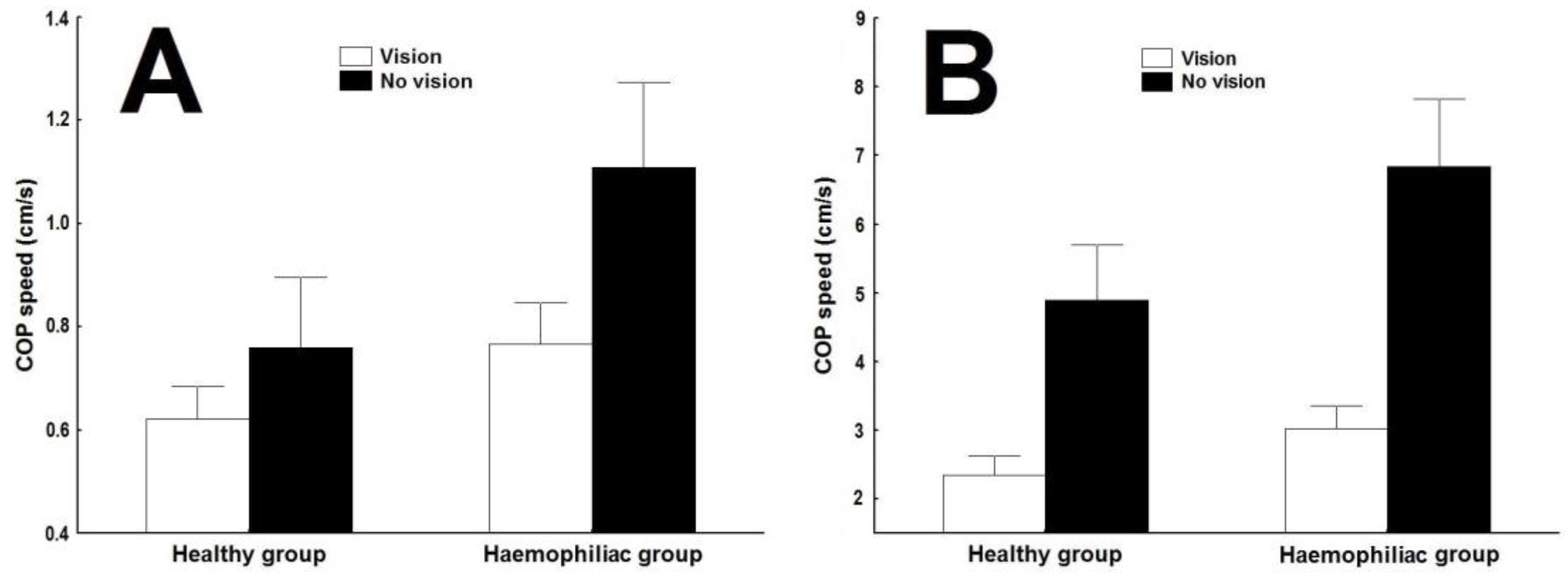
The main objective of this study was to determine if haemophilia is associated with a decreased postural stability in male adolescents. Figure 1 illustrates the effect of haemophilia on the mean speed of the postural sway (COP Speed) for visual (vision/no vision) and proprioceptive (hard floor/foam floor) conditions. The ANOVA revealed a significant main effect of Group (F(1,18) = 14.425, p < 0.01), Vision (F(1,18) = 236.67, p < 0.001), and Proprioception (F(1,18) = 296.19, p < 0.001), as well as significant Vision × Proprioception (F(1,18) = 18.506, p < 0.001), Group × Vision (F(1,18) = 10.723, p < 0.01), Group × Proprioception (F(1,18) = 6.870, p < 0.05), and Group × Vision × Proprioception (F(1,18) = 5.861, p < 0.05) interactions. For both groups, COP speed clearly increased when vision and proprioception were challenged. The decomposition of the interaction showed that haemophiliac adolescents had significantly higher average speed of COP displacement for all visual and proprioceptive conditions compared to healthy adolescents, except for the vision/hard floor condition (reaching significance failed at p < 0.07). COP speed values obtained were 0.77 ± 0.08 versus 0.62 ± 0.12 cm/s in vision/hard floor condition (p < 0.07) (Figure 1A), 1.11 ± 0.27 versus 0.76 ± 0.19 cm/s in no vision/hard floor condition (p < 0.05) (Figure 1A), 3.02 ± 0.47 versus 2.34 ± 0.45 cm/s in vision/foam floor condition (p < 0.05) (Figure 1B), and 6.83 ± 1.68 versus 4.89 ± 1.05 cm/s in no vision/foam floor condition (p < 0.01) (Figure 1B).
4. Discussion
The objective of this study was to assess if haemophilia negatively affects balance control in male adolescents. Our results show that haemophiliac subjects had increased COP speed, which could be interpreted as decreased postural stability, especially when vision and proprioception were altered.
4.1. Haemophilia, Postural Control, and Altered Vision Condition
Even during quiet stance, continuous adjustments of muscle activity and joint position occur in anticipation and response to the integration of sensory information from visual, vestibular, and somatosensory inputs, all of which contribute to postural balance [5,22,23]. For balance control in the current study, an effect of interaction between group and vision conditions was observed, and planned comparisons revealed that the haemophiliac group was significantly more affected by the altered vision condition than the healthy group. All haemophiliac adolescents had systematically higher COP speed values while standing upright with eyes closed versus eyes open, indicating that the removal of vision had a more pronounced effect on postural balance performance. Returning to our hypotheses, this result supports the notion that there is a sensorial component to balance control that is important in maintaining stability in haemophiliac individuals. It is well known that when vision is removed during the maintenance of normal quiet stance, there is a sensorial reweighting that occurs and somatosensory inputs (proprioception) are tuned in order to compensate and maintain postural stability [22,24]. Our results in altered vision condition suggest that the proprioception of haemophiliac adolescents did not adequately compensate for the lack of visual information in posture control.
The effect of haemophilia on balance control has been previously observed and reported elsewhere [9,10,13,14], and the original contribution of this study is the demonstration of the effect of haemophilia on balance control in male adolescents when vision and proprioception are challenged. Our haemophiliac subjects swayed at a faster speed compared to our healthy group, as shown by the effect of group × vision interaction for COP speed. Our findings are in accordance with a previous study realized in haemophiliac adults, where this particular effect has been previously investigated and reported [9]. Effectively, Hilberg et al. [9] investigated proprioception and leg muscle strength in participants with haemophilia and age-matched control participants without haemophilia. Their haemophiliac subjects had significantly impaired proprioceptive function when measured on the one-leg-stand test with and without vision compared to the control group. However, our results are not in accordance with those reported in haemophiliac children when vision and proprioception are both altered [14]. The authors reported no differences between haemophiliac children compared to healthy children in visual and vestibular quotients variables between groups, and mentioned that their results from vestibular quotient were expected, as their participants were known to have no vestibular pathology. On the other hand, their results obtained for the visual quotient went counter to the hypothesis that haemophiliac children may have impairment in sensory information from joints and muscles. Consequently, our results confirm the hypothesis that in the absence of vision, haemophilia alters postural control due to a deficit in proprioceptive inputs induced by repetitive joint or muscle bleeds. Furthermore, Souza et al. [14] suggest that joint distention due to haemarthrosis can lead to the inhibition of the reflex of extensor muscles and to increased activation of flexors, which in turn could lead to inaccurate information about limb position and movement. Their hypothesis is that most joint bleeds in haemophiliac subjects occur in lower limbs (especially knee and ankle [25]), and that these anatomical locations are important for postural synergies [26]; thus, alterations in postural balance are expected after repetitive haemarthrosis.
4.2. Haemophilia, Postural Control, and Altered Proprioception Condition
Regarding the proprioceptive condition, our results show an effect of interaction between group and proprioceptive condition, with planned comparisons revealing that the haemophiliac group was significantly more affected by the altered proprioceptive condition than the healthy group. All haemophiliac adolescents had systematically greater COP speed value while standing upright with eyes open or closed on the foam floor versus on the hard floor, revealing that an alteration of the standing surface of the support had a more pronounced effect on the regulation of postural control.
Our results are in accordance with those of Souza et al. [14]. In their study, their haemophiliac children exhibited a more important value in the sway area of the COP displacement for the proprioceptive quotient when their participants were standing on a foam floor compared to on a hard floor. The authors mentioned that this unstable condition on the foam floor (altered surface) occurs due to altered information about the surface, leading to a more difficult adaptation of the foot on the floor and consequently a lesser ability to apply force on the floor. Effectively, the use of a foam surface challenges balance control and produces a multidirectional balance perturbation [27]. Upright stance in static balance condition on a foam surface changes the biomechanics of the foot, resulting in an alteration of the distribution of the plantar pressures [17] and an increase of the activation of the ankle muscles related to the location of the COP under the foot [23]. Interestingly, Kurz et al. [11] investigated the ankle muscle activation in adult individuals with haemophilia in upright stance. The authors found that superficial flexors of the ankle joint are less active in people with haemophilia compared to healthy controls. Usually, human upright posture is especially ensured through activity of ankle joint muscles [28]. It is well known that due to an anterior position of the centre of gravity, calf muscles of normal individuals during control condition in upright stance demonstrate an elevated activity to preserve a constant balance and prevent falls [29]. This may explain the increased COP speed observed in our haemophiliac group in altered surface with and without vision, as well as observed in previous studies [7,14].
Finally, our results showed no differences between haemophiliac group and healthy group in normal condition (vision available on stable surface—i.e., hard floor); only a tendency was observed (reaching significance failed at p < 0.07). This confirms previous results obtained in haemophiliac children [14], and is not in accordance with results reported in haemophiliac adults [10,13]. On the other hand, results obtained in haemophiliac adults were found in dynamic postural conditions, contrary to ours realized in static conditions. The limitations of our study concern the small sample of subjects of our experimental group (n = 8) and also that our adolescents were not evaluated by an adolescent activity level questionnaire (i.e., International Physical Activity Questionnaire). However, our results should not be minimized, and it is difficult to conclude if haemophilia actually affects postural control in normal condition—especially since several factors have not been controlled in our study and in other studies. These factors are well documented, and could be directly related to the haemophiliac condition. Factors present in lower limbs in haemophiliac individuals has been identified to affect postural control in normal individuals; e.g., pain [30] or muscular fatigue [31]. These factors combined together with an altered proprioception in haemophiliac individuals may have a confounding effect, resulting in a decreased postural stability as observed in altered visual and proprioceptive conditions.
In conclusion, balance control is an essential prerequisite in daily life. Even though it is often considered as a simple task, it is the basis for most movements we perform. The results of this present study indicate an association between haemophilia and balance control in male adolescents. Haemophiliac adolescents showed more postural instability when compared to healthy individuals. A deficit in somatosensory inputs modifies the ability of the central nervous system to adequately use these proprioceptive inputs for postural control, and this influences the performances to realize with accuracy the activities of daily living, causing functional limitations and possibly predisposing to potential injuries. As postural instability or balance control deficits are identified as a risk factor for falling [5,6], our results also suggest that haemophilia in individuals could be considered as a potential contributing factor for falling. Further studies are needed to investigate if postural alterations in haemophiliac individuals are related to the severity of the haemophiliac factor and could contribute to potential injuries. From a clinical perspective, and since it has been shown that postural control can be increased by specific training in haemophiliac adults [32], our results underline the real need of developing a specific and safe training programme adapted for haemophiliac subjects to improve proprioceptive performance. Therefore, physical therapy and kinesiology should focus their intervention on adapted proprioceptive integration exercises to improve balance control related to situations encountered in the activities of daily life. Moreover, specific and adapted muscular exercises should be specifically oriented to increase muscle strength, conserve the pattern of muscle contraction, and increase the range of motion at the ankle to maintain its role in balance function. This should be done in addition to the improvement of the muscle function targeting the protection of the joints from progressive degeneration in haemophiliac individuals.
Acknowledgments
All participants are gratefully acknowledged. Special thanks to Marcel Kazsap for programming expertise and technical support and to Mathieu Germain-Robitaille during testing sessions. Finally, this research has been realized with the precious implication of two external collaborators: Philippe Nadeau who coordinated the feasibility of this study at the Enfant-Jésus Hospital of Québec city and Stéphanie Cloutier who kindly authorized her patients to participate to this research project.
Author Contributions
Olivier Hue conceived and designed the experiment and obtained the approval of the University of Québec at Trois-Rivières ethics committee. Hafedh Alaeddine Thabti, Sarah Beausoleil and Olivier Hue participated in the acquisition of data and in data analyses. Sarah Beausoleil made bibliographic research concerning the specific literature used (haemophilia and postural control related to her winter session student’s project). Hafedh Alaeddine Thabti and Olivier Hue wrote the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Loram, I.D.; Kelly, S.M.; Lakie, M. Human balancing of an inverted pendulum: Is sway size controlled by ankle impedance? J. Physiol. 2001, 532, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Johansson, R.; Magnusson, M.; Akesson, M. Identification of human postural dynamics. IEEE Trans. Biomed. Eng. 1988, 35, 858–869. [Google Scholar] [CrossRef] [PubMed]
- Loram, I.D.; Lakie, M. Direct measurement of human ankle stiffness during quiet standing: The intrinsic mechanical stiffness is insufficient for stability. J. Physiol. 2002, 545, 1041–1053. [Google Scholar] [CrossRef] [PubMed]
- Massion, J. Postural control system. Curr. Opin. Neurobiol. 1994, 4, 877–887. [Google Scholar] [CrossRef]
- Horak, F.B.; Shupert, C.L.; Mirka, A. Components of postural dyscontrol in the elderly: A review. Neurobiol. Aging 1989, 10, 727–738. [Google Scholar] [CrossRef]
- Maki, B.E.; Holliday, P.J.; Topper, A.K. A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. J. Gerontol. 1994, 49, M72–M84. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Berg, K.; Chesworth, B.; Klar, N.; Speechley, M. Quantifying the magnitude of risk for balance impairment on falls in community-dwelling older adults: A systematic review and meta-analysis. J. Clin. Epidemiol. 2010, 63, 389–406. [Google Scholar] [CrossRef] [PubMed]
- Cahill, M.R.; Colvin, B.T. Haemophilia. Postgrad. Med. J. 1997, 73, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Hilberg, T.; Herbsleb, M.; Gabriel, H.H.; Jeschke, D.; Schramm, W. Proprioception and isometric muscular strength in haemophiliac subjects. Haemophilia 2001, 7, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Fearn, M.; Hill, K.; Williams, S.; Mudge, L.; Walsh, C.; McCarthy, P.; Walsh, M.; Street, A. Balance dysfunction in adults with haemophilia. Haemophilia 2010, 16, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Kurz, E.; Anders, C.; Herbsleb, M.; Puta, C.; Czepa, D.; Hilberg, T. Ankle muscle activation in people with haemophilia. Haemophilia 2012, 18, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Buzzard, B.M. Proprioceptive training in haemophilia. Haemophilia 1998, 4, 528–531. [Google Scholar] [PubMed]
- Gallach, J.E.; Querol, F.; González, L.M.; Pardo, A.; Aznar, J.A. Posturographic analysis of balance control in patients with haemophiliac arthropathy. Haemophilia 2008, 14, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Souza, F.M.; McLaughlin, P.; Pereira, R.P.; Minuque, N.P.; Mello, M.H.; Siqueira, C.; Villaça, P.; Tanaka, C. The effects of repetitive haemarthrosis on postural balance in children with haemophilia. Haemophilia 2013, 19, e212–e217. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, N.; Stelmach, G.E.; Breunig, A. Postural sway characteristics of the elderly under normal and altered visual and support surface conditions. J. Gerontol. 1991, 46, B238–B244. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Chiang, J.H. The effects of surface compliance on foot pressure in stance. Gait Posture 1996, 4, 122–129. [Google Scholar] [CrossRef]
- Chiang, J.H.; Wu, G. The influence of foam surfaces on biomechanical variables contributing to postural control. Gait Posture 1997, 5, 239–245. [Google Scholar] [CrossRef]
- Maki, B.E.; Holliday, P.J.; Fernie, G.R. A comparison of spontaneous-and induced sway balance tests. J. Am. Geriatr. Soc. 1990, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Geurts, A.C.; Nienhuis, B.; Mulder, T.W. Intrasubject variability of selected force-platform parameters in the quantification of postural control. Arch. Phys. Med. Rehabil. 1993, 74, 1144–1150. [Google Scholar] [PubMed]
- Baratto, L.; Morasso, P.G.; Re, C.; Spada, G. A new look at posturographic analysis in the clinical context: Sway-density versus other parameterization techniques. Mot. Control 2002, 6, 246–270. [Google Scholar] [CrossRef]
- Raymakers, J.A.; Samson, M.M.; Verhaar, H.J.J. The assessment of body sway and the choice of the stability parameter(s). Gait Posture 2005, 21, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Peterka, R.J. Sensorimotor integration in human postural control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [PubMed]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Teasdale, N.; Simoneau, M. Attentional demands for postural control: The effects of aging and sensory reintegration. Gait Posture 2001, 14, 203–210. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C. Articular Bleeding in Hemophilia. Cardiovasc. Hematol. Disord. Drug Targets 2016, 16, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Runge, C.F.; Shupert, C.L.; Horak, F.B.; Zajac, F.E. Ankle and hip postural strategies defined by joint torques. Gait Posture 1999, 10, 161–170. [Google Scholar] [CrossRef]
- Patel, M.; Fransson, P.A.; Lush, D.; Petersen, H.; Magnusson, M.; Johansson, R.; Gomez, S. The effects of foam surface properties on standing body movement. Acta Otolaryngol. 2008, 128, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Gurfinkel, V.S.; Lipshits, M.I.; Mori, S.; Popov, K.E. Stabilization of body position as the main task of postural regulation. Hum. Physiol. 1981, 7, 155–165. [Google Scholar] [PubMed]
- Soames, R.W.; Atha, J. The role of the antigravity musculature during quiet standing in man. Eur. J. Appl. Physiol. Occup. Physiol. 1981, 47, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Corbeil, P.; Blouin, J.S.; Teasdale, N. Effects of intensity and locus of painful stimulation on postural stability. Pain 2004, 108, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Forestier, N.; Teasdale, N.; Nougier, V. Alteration of the position sense at the ankle induced by muscular fatigue in humans. Med. Sci. Sports Exerc. 2002, 34, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.; Fearn, M.; Williams, S.; Mudge, L.; Walsh, C.; McCarthy, P.; Walsh, M.; Street, A. Effectiveness of a balance training home exercise programme for adults with haemophilia: A pilot study. Haemophilia 2010, 16, 162–169. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mean speed of the centre of pressure (COP Speed) for healthy and haemophiliac groups in (A) hard floor and (B) foam floor conditions. Error bars are ±95% confidence intervals.
Figure 1.
Mean speed of the centre of pressure (COP Speed) for healthy and haemophiliac groups in (A) hard floor and (B) foam floor conditions. Error bars are ±95% confidence intervals.


{kind=link}
Table 1.
Group characteristics.
| Variables | Healthy Group n = 12 | Haemophiliac Group n = 8 |
|---|---|---|
| Age (years) | 14.8 ± 1.4 (13–17) | 15.0 ± 1.4 (14–17) |
| Height (m) | 1.69 ± 0.1 (1.54–1.82) | 1.66 ± 0.1 (1.52–1.79) |
| Weight (kg) | 56.7 ± 9.8 (40–69) | 56.1 ± 8.0 (40.8–65.7) |
| BMI (kg/m2) | 19.8 ± 1.8 (16.8–22.3) | 20.4 ± 3.2 (17.4–27.3) |
Values are means ± SD (min–max). BMI: body mass index.
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Thabti, H.A.; Beausoleil, S.; Hue, O. The Effects of Haemophilia on the Postural Control of Adolescents. J. Funct. Morphol. Kinesiol. 2017, 2, 24. https://doi.org/10.3390/jfmk2030024
AMA Style
Thabti HA, Beausoleil S, Hue O. The Effects of Haemophilia on the Postural Control of Adolescents. Journal of Functional Morphology and Kinesiology. 2017; 2(3):24. https://doi.org/10.3390/jfmk2030024
Chicago/Turabian StyleThabti, Hafedh Alaeddine, Sarah Beausoleil, and Olivier Hue. 2017. "The Effects of Haemophilia on the Postural Control of Adolescents" Journal of Functional Morphology and Kinesiology 2, no. 3: 24. https://doi.org/10.3390/jfmk2030024