
Microporous Implants Modified by Bifunctional Hydrogel with Antibacterial and Osteogenic Properties Promote Bone Integration in Infected Bone Defects
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Hydrogel Preparation and Characterization
2.3. H2O2 Scavenging Capacity of the Hydrogel
2.4. Drug Loading and Release
2.5. Cytocompatibility
2.6. In Vitro Osteogenic Induction of the Drug-Loaded Hydrogel
2.7. In Vitro Antimicrobial Evaluation
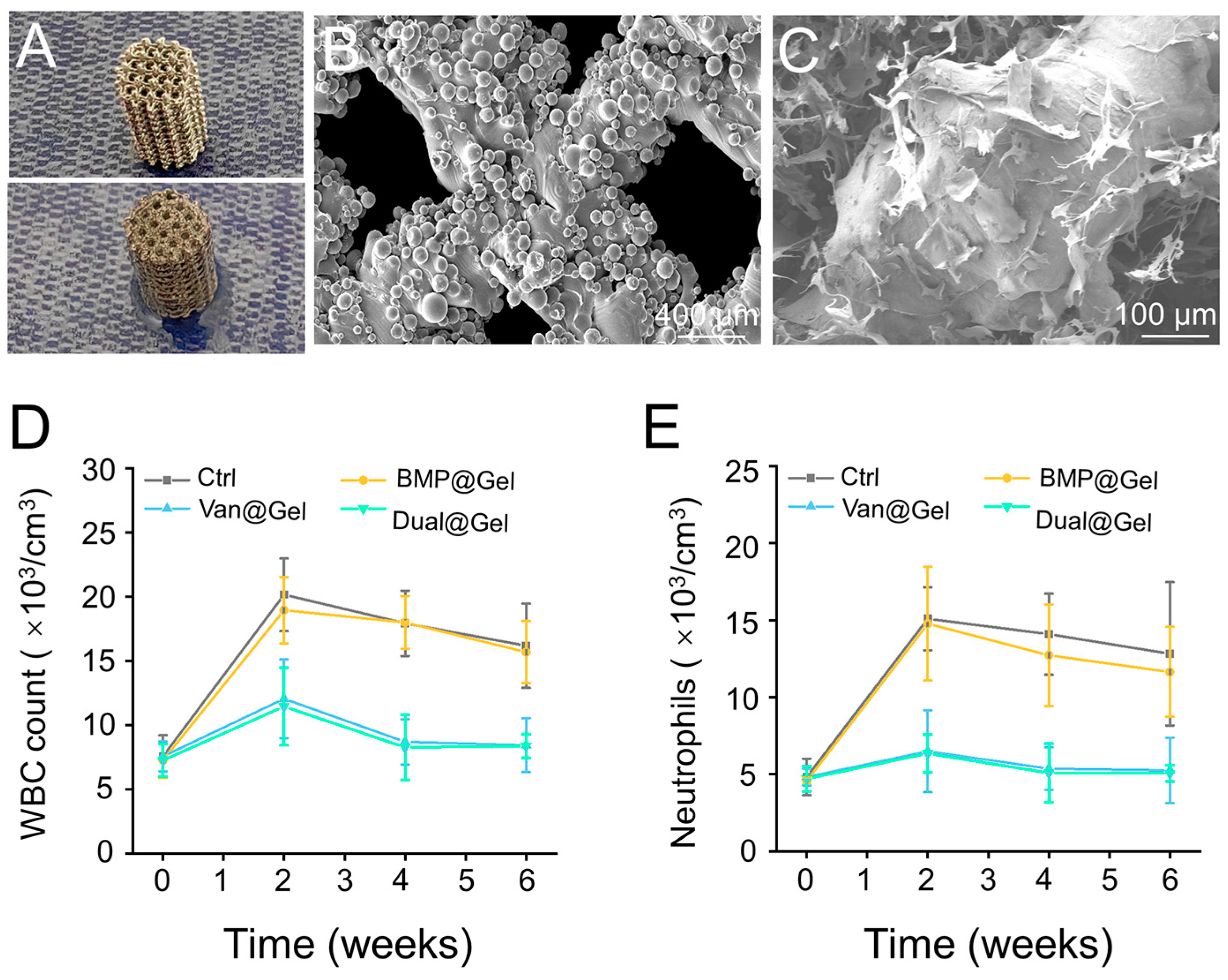
2.8. Preparation of 3D-Printed Implants
2.9. Animal Procedures
2.10. Micro-Computed Tomography (Micro-CT)
2.11. Histological Evaluation
2.12. Push-Out Test
2.13. Immunofluorescence
2.14. Statistical Analysis
3. Results
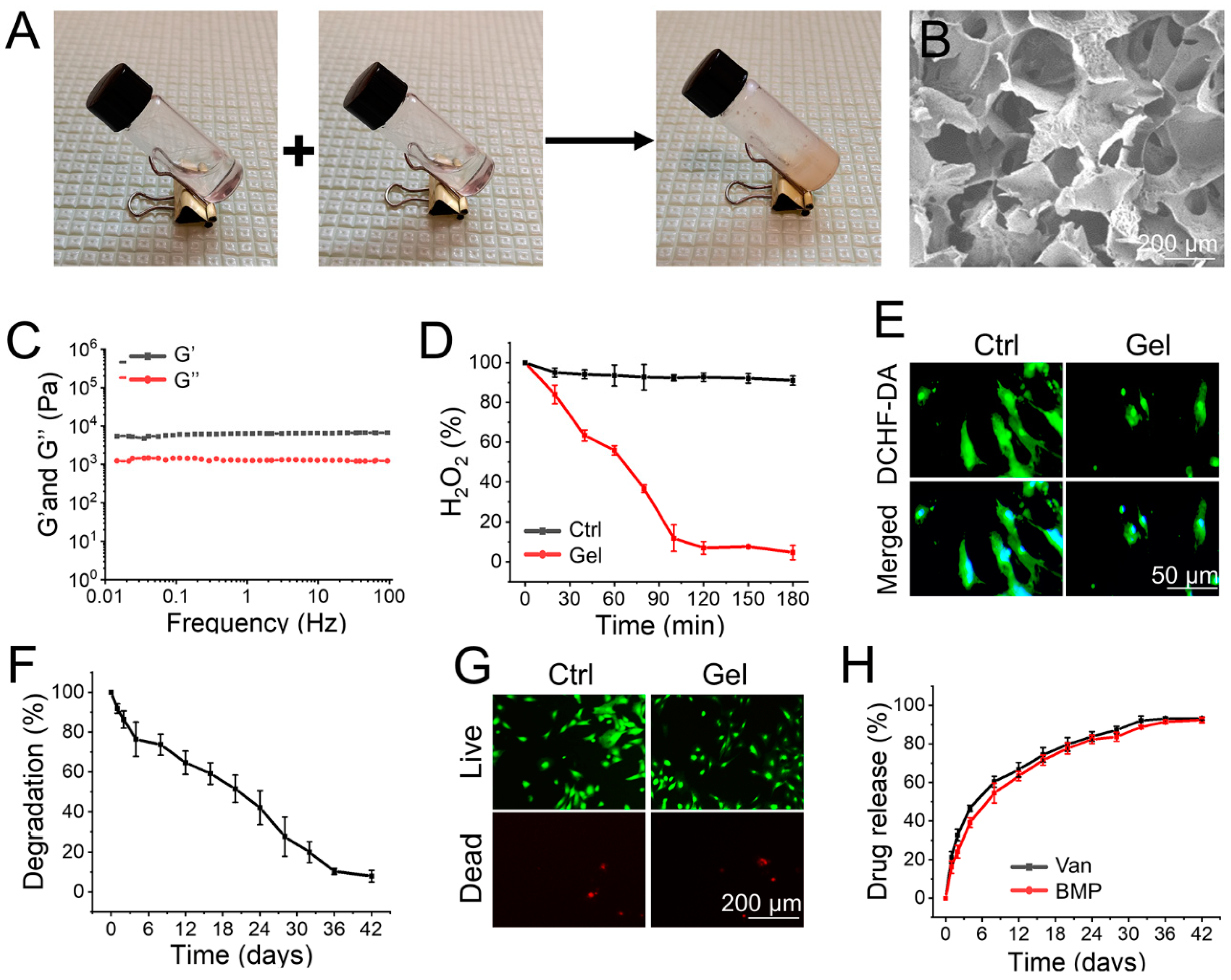
3.1. Preparation and Characterization of the Hydrogel
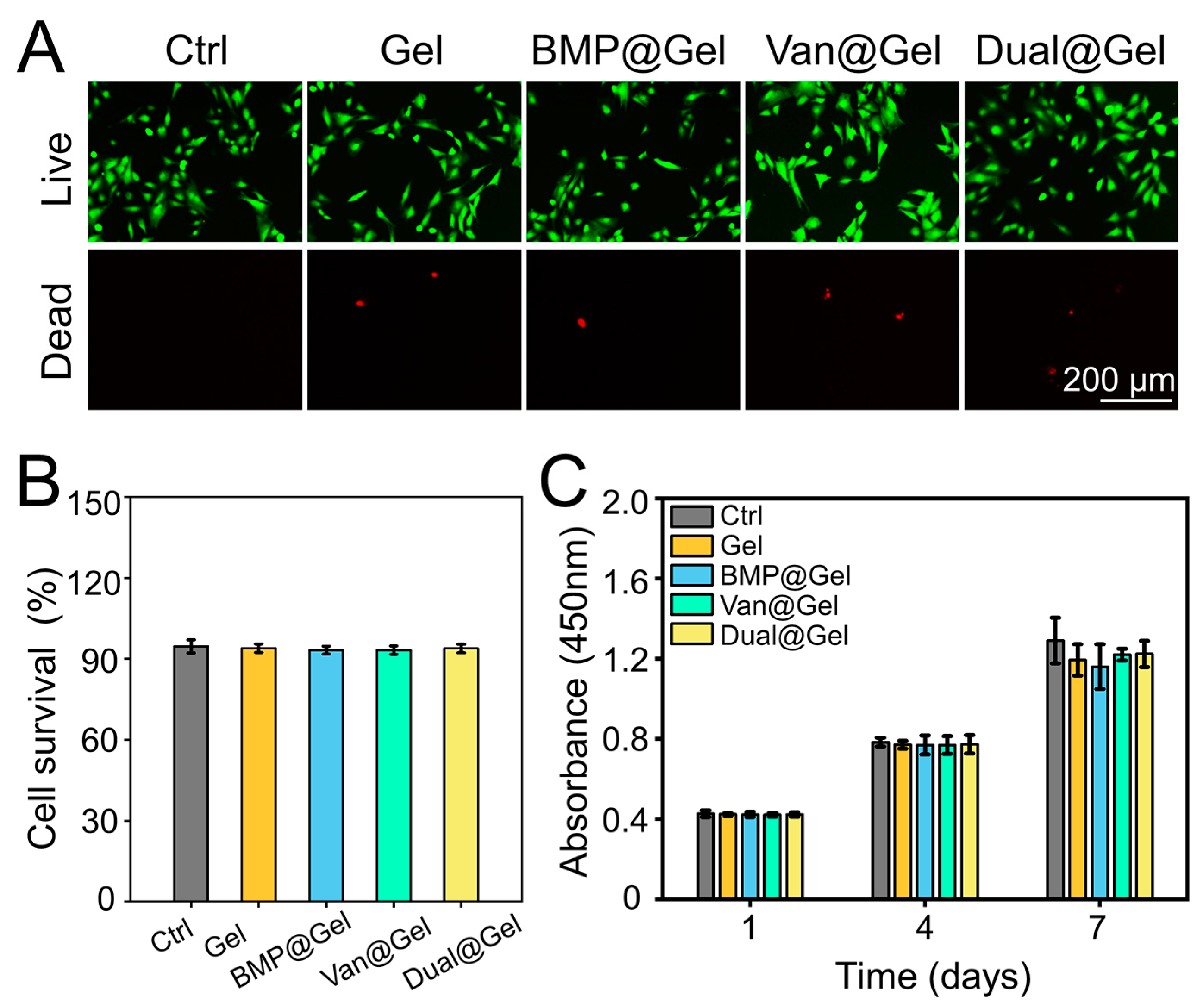
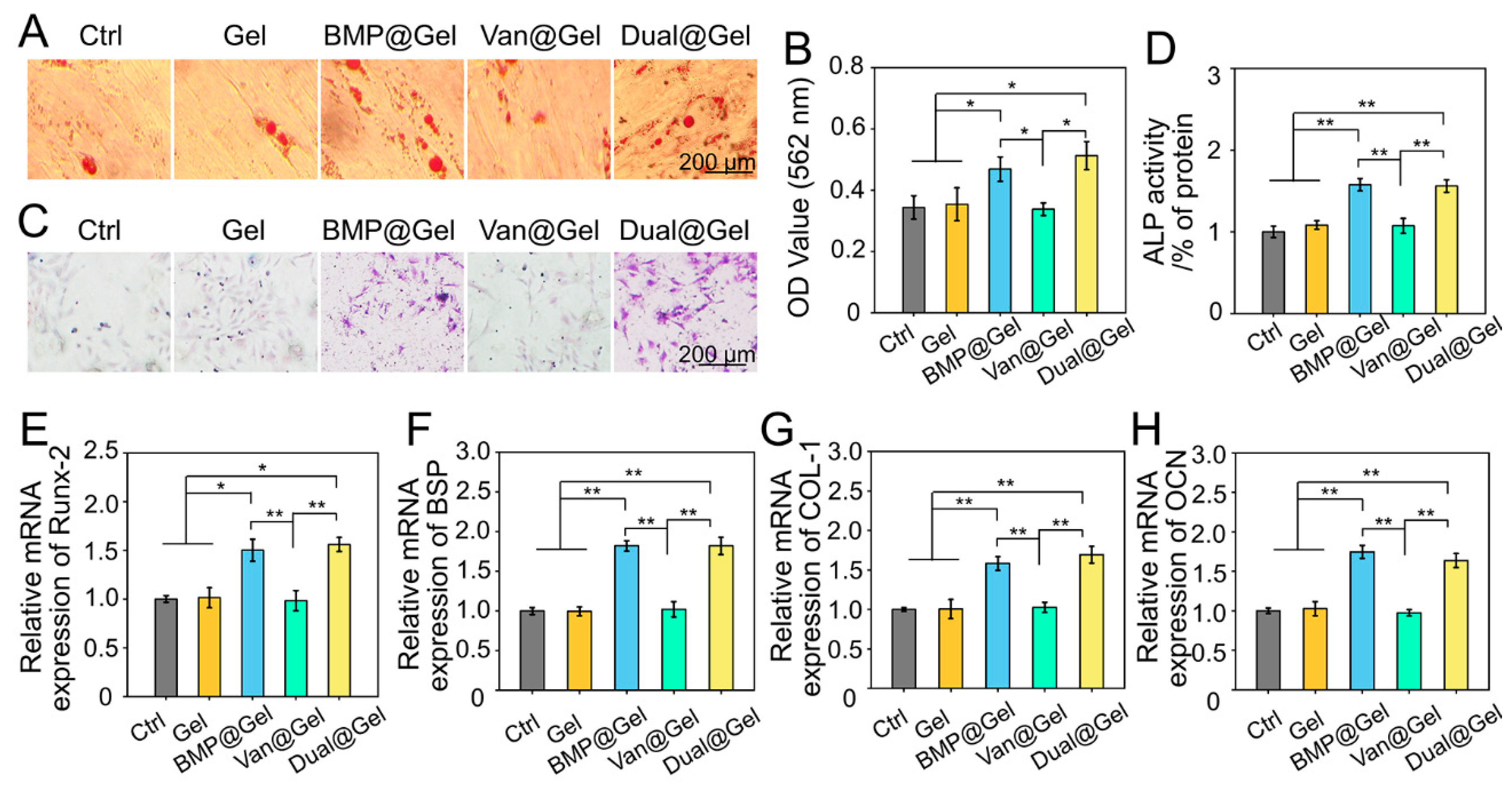
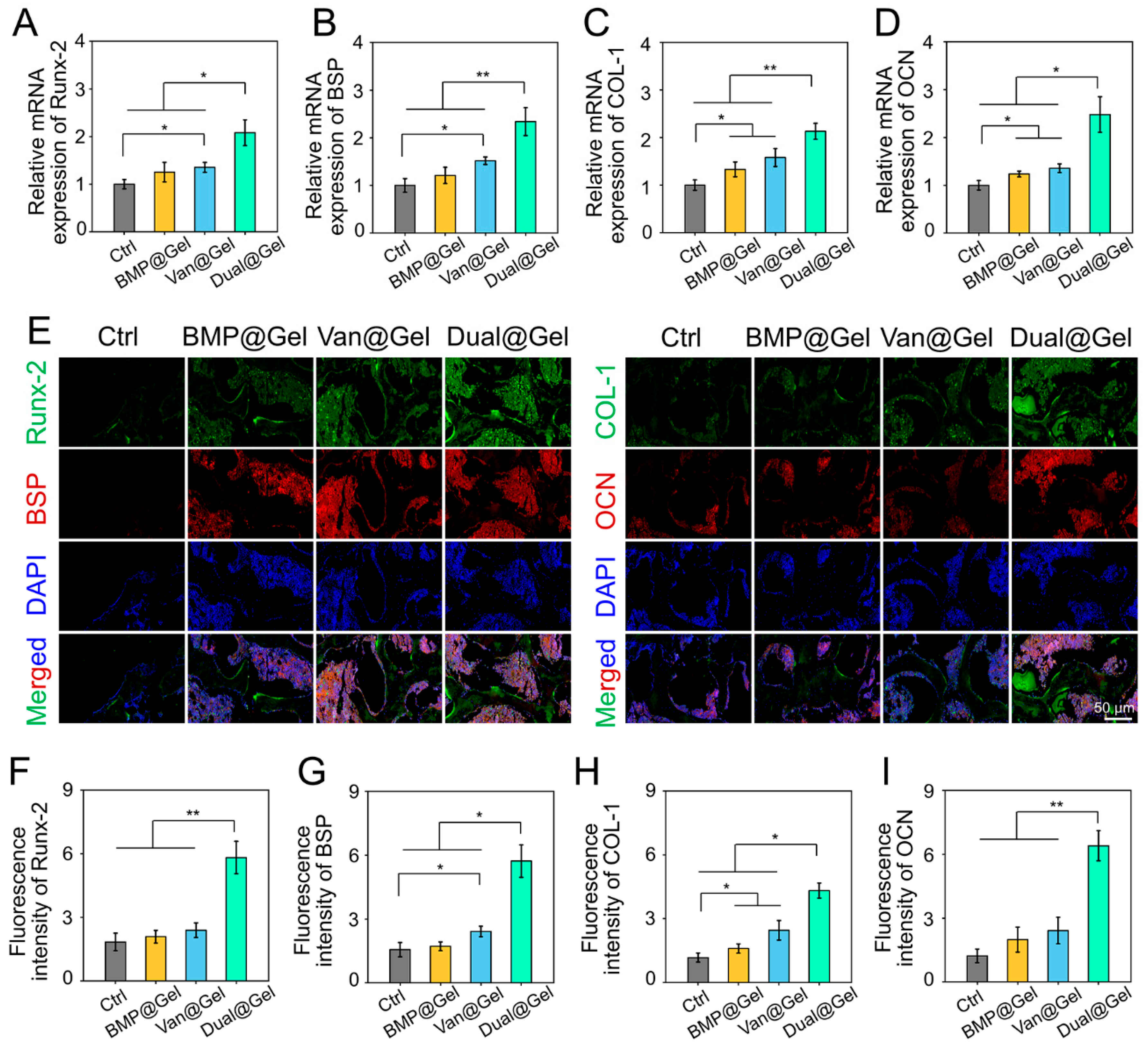
3.2. Biocompatibility and Osteogenic Differentiation of BMSCs in Drug-Loaded Hydrogel
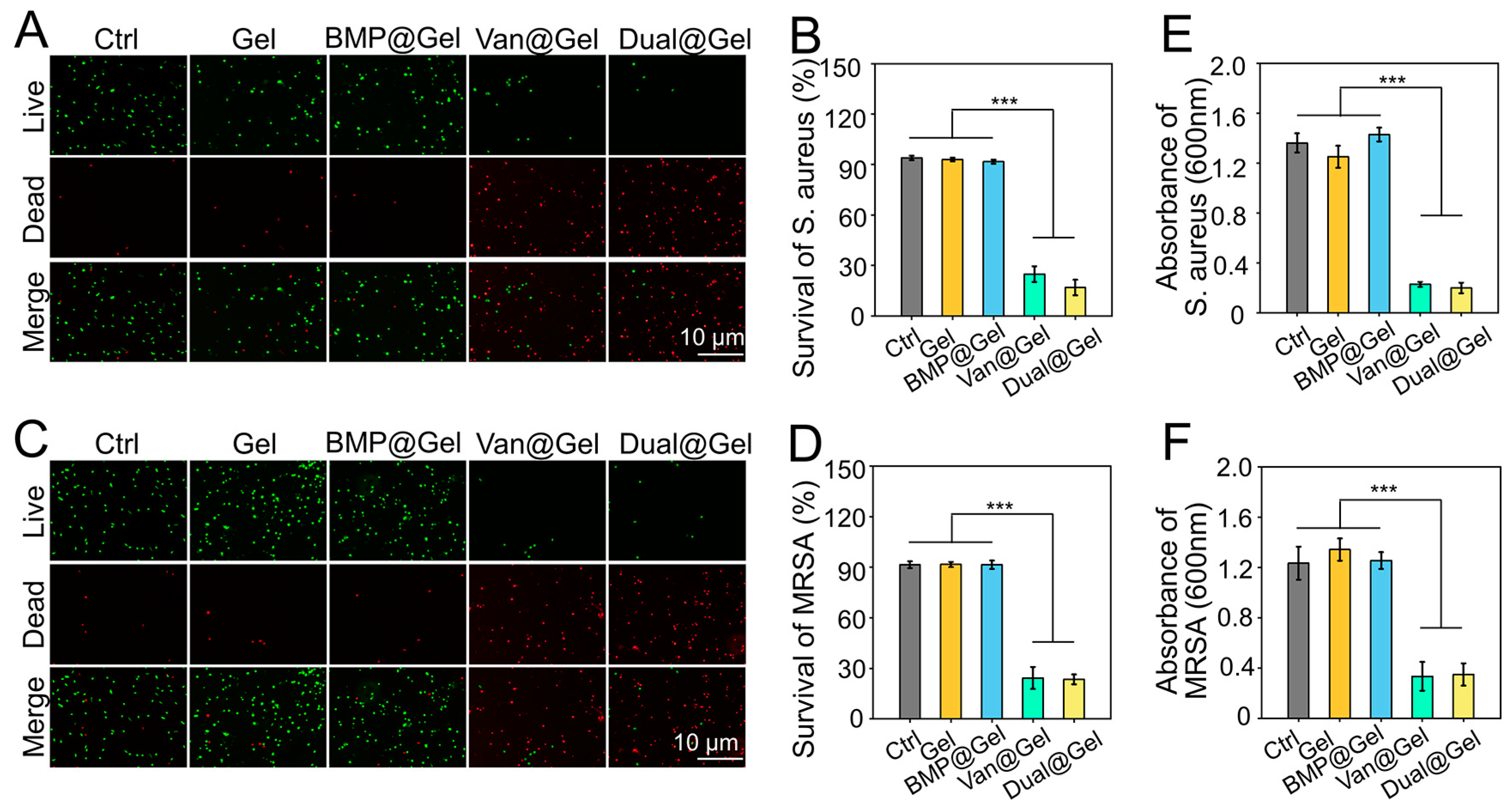
3.3. Antibacterial Assessment
3.4. In Vivo Anti-Infection Effects of the Drug-Loaded Hydrogel
3.5. Bone Regeneration and Integration in Contaminated Bone Defect
4. Conclusions
Ethical Statement
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Nair, M.B.; Kretlow, J.D.; Mikos, A.G.; Kasper, F.K. Infection and tissue engineering in segmental bone defects—A mini review. Curr. Opin. Biotechnol. 2011, 22, 721–725. [Google Scholar] [CrossRef]
- Mouriño, V.; Boccaccini, A.R. Bone tissue engineering therapeutics: Controlled drug delivery in three-dimensional scaffolds. J. R. Soc. Interface 2010, 7, 209–227. [Google Scholar] [CrossRef] [PubMed]
- Inzana, J.A.; Schwarz, E.M.; Kates, S.L.; Awad, H.A. Biomaterials approaches to treating implant-associated osteomyelitis. Biomaterials 2016, 81, 58–71. [Google Scholar]
- Li, Z.; Bai, H.; Wang, Z.; Liu, Y.; Ren, M.; Wang, X.; Gao, W.; Li, Q.; Wu, M.; Liu, H.; et al. Ultrasound-mediated rapamycin delivery for promoting osseointegration of 3D printed prosthetic interfaces via autophagy regulation in osteoporosis. Mater. Des. 2022, 216, 110586. [Google Scholar] [CrossRef]
- Wu, H.; Li, F.; Shao, W.; Gao, J.; Ling, D. Promoting Angiogenesis in Oxidative Diabetic Wound Microenvironment Using a Nanozyme-Reinforced Self-Protecting Hydrogel. ACS Cent. Sci. 2019, 5, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Han, F.; Ma, J.; Wang, H.; Pan, J.; Yang, G.; Zhao, H.; Zhao, J.; Liu, J.; Liu, Z.; et al. Targeting Endogenous Hydrogen Peroxide at Bone Defects Promotes Bone Repair. Adv. Funct. Mater. 2021, 32, 2111208. [Google Scholar] [CrossRef]
- Zhu, M.; Fang, J.; Li, Y.; Zhong, C.; Feng, S.; Ge, X.; Ye, H.; Wang, X.; Zhu, W.; Lu, X.; et al. The Synergy of Topographical Micropatterning and Ta|TaCu Bilayered Thin Film on Titanium Implants Enables Dual-Functions of Enhanced Osteogenesis and Anti-Infection. Adv. Health Mater. 2021, 10, e2002020. [Google Scholar] [CrossRef]
- Lebaudy, E.; Fournel, S.; Lavalle, P.; Vrana, N.E.; Gribova, V. Recent Advances in Antiinflammatory Material Design. Adv. Health Mater. 2021, 10, e2001373. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, X.; Yang, K.; Fu, Y.V.; Xu, T.; Li, S.; Zhang, D.; Wang, L.-N.; Lee, C.-S. A Novel Double-Crosslinking-Double-Network Design for Injectable Hydrogels with Enhanced Tissue Adhesion and Antibacterial Capability for Wound Treatment. Adv. Funct. Mater. 2020, 30, 1904156. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, J.; Song, J.; Yang, J.; Du, Z.; Zhao, W.; Guo, H.; Wen, C.; Li, Q.; Sui, X.; et al. A Multifunctional Pro-Healing Zwitterionic Hydrogel for Simultaneous Optical Monitoring of pH and Glucose in Diabetic Wound Treatment. Adv. Funct. Mater. 2020, 30, 1905493. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, Z.H.; Jiang, Y.N.; Liu, H.; Song, S.L.; Wang, C.Y.; Li, Z.H.; Yang, Z.; Liu, H.; Wang, J.C.; et al. Biomimetic Composite Scaffolds to Manipulate Stem Cells for Aiding Rheumatoid Arthritis Management. Adv. Funct. Mater. 2019, 29, 1807860. [Google Scholar] [CrossRef]
- Noddeland, H.K.; Lind, M.; Jensen, L.B.; Petersson, K.; Skak-Nielsen, T.; Larsen, F.H.; Malmsten, M.; Heinz, A. Design and characterization of matrix metalloproteinase-responsive hydrogels for the treatment of inflammatory skin diseases. Acta Biomater. 2022, 157, 149–161. [Google Scholar] [CrossRef]
- Man, K.; Brunet, M.Y.; Federici, A.S.; Hoey, D.A.; Cox, S.C. An ECM-Mimetic Hydrogel to Promote the Therapeutic Efficacy of Osteoblast-Derived Extracellular Vesicles for Bone Regeneration. Front. Bioeng. Biotechnol. 2022, 10, 829969. [Google Scholar] [CrossRef]
- Do, N.H.N.; Truong, Q.T.; Le, P.K.; Ha, A.C. Recent developments in chitosan hydrogels carrying natural bioactive compounds. Carbohydr. Polym. 2022, 294, 119726. [Google Scholar] [CrossRef]
- Cheng, X.; Li, L.; Yang, L.; Huang, Q.; Li, Y.; Cheng, Y. All-Small-Molecule Dynamic Covalent Hydrogels with Heat-Triggered Release Behavior for the Treatment of Bacterial Infections. Adv. Funct. Mater. 2022, 32, 2206201. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Z.; Guan, J.; Mao, Y.; Zhou, P. Hydrogel: A potential therapeutic material for bone tissue engineering. Aip Adv. 2021, 11, 010701. [Google Scholar] [CrossRef]
- Qi, M.; Zhou, Q.; Zeng, W.; Wu, L.; Zhao, S.; Chen, W.; Luo, C.; Shen, M.; Zhang, J.; Tang, C.E. Growth factors in the pathogenesis of diabetic foot ulcers. Front. Biosci. 2018, 23, 310–317. [Google Scholar]
- Alvand, A.; Rezapoor, M.; Parvizi, J. The Role of Biomarkers for the Diagnosis of Implant-Related Infections in Orthopaedics and Trauma. Adv. Exp. Med. Biol. 2017, 971, 69–79. [Google Scholar]
- Srinivasan, S.; Kumar, P.T.; Nair, S.V.; Nair, S.V.; Chennazhi, K.P.; Jayakumar, R. Antibacterial and bioactive alpha- and beta-chitin hydrogel/nanobioactive glass ceramic/nano silver composite scaffolds for periodontal regeneration. J. Biomed. Nanotechnol. 2013, 9, 1803–1816. [Google Scholar] [CrossRef]
- Mieszawska, A.J.; Fourligas, N.; Georgakoudi, I.; Ouhib, N.M.; Belton, D.J.; Perry, C.C.; Kaplan, D.L. Osteoinductive silk-silica composite biomaterials for bone regeneration. Biomaterials 2010, 31, 8902–8910. [Google Scholar] [CrossRef]
- Qiao, S.; Wu, D.; Li, Z.; Zhu, Y.; Zhan, F.; Lai, H.; Gu, Y. The combination of multi-functional ingredients-loaded hydrogels and three-dimensional printed porous titanium alloys for infective bone defect treatment. J. Tissue Eng. 2020, 11, 2041731420965797. [Google Scholar] [CrossRef]
- Zhao, H.; Huang, J.; Li, Y.; Lv, X.; Zhou, H.; Wang, H.; Xu, Y.; Wang, C.; Wang, J.; Liu, Z. ROS-scavenging hydrogel to promote healing of bacteria infected diabetic wounds. Biomaterials 2020, 258, 120286. [Google Scholar] [CrossRef] [PubMed]
- Cheng, G.; Yin, C.; Tu, H.; Jiang, S.; Wang, Q.; Zhou, X.; Xing, X.; Xie, C.; Shi, X.; Du, Y.; et al. Controlled Co-delivery of Growth Factors through Layer-by-Layer Assembly of Core-Shell Nanofibers for Improving Bone Regeneration. ACS Nano 2019, 13, 6372–6382. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Wang, S.; He, Q.; Li, D.; Xin, L.; Xu, C.; Zhu, X.; Mei, L.; Cannon, R.D.; Ji, P.; et al. A Mechanically Reinforced Super Bone Glue Makes a Leap in Hard Tissue Strong Adhesion and Augmented Bone Regeneration. Adv. Sci. 2023, 10, e2206450. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, J.; Zhang, X.; Yu, S.; Wen, D.; Hu, Q.; Ye, Y.; Bomba, H.; Hu, X.; Liu, Z.; et al. In situ formed reactive oxygen species-responsive scaffold with gemcitabine and checkpoint inhibitor for combination therapy. Sci. Transl. Med. 2018, 10, eaan3682. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, Y.; Huang, H.; Zhang, C.; Liu, H.; Wang, Z.; Yi, M.; Xie, N.; Shen, Y.; Ren, X.; et al. A Nanozyme-Immobilized Hydrogel with Endogenous ROS-Scavenging and Oxygen Generation Abilities for Significantly Promoting Oxidative Diabetic Wound Healing. Adv. Health Mater. 2022, 11, 2201524. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Song, S.; Wang, D.; Liu, H.; Zhang, J.; Li, Z.; Wang, J.; Ren, X.; Zhao, Y. Nanozyme-reinforced hydrogel as a H2O2-driven oxygenerator for enhancing prosthetic interface osseointegration in rheumatoid arthritis therapy. Nat. Commun. 2022, 13, 6758. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, Y.; Wang, Z.; Ren, M.; Wang, X.; Liu, H.; Lin, Q.; Wang, J. Engineering Multifunctional Hydrogel-Integrated 3D Printed Bioactive Prosthetic Interfaces for Osteoporotic Osseointegration. Adv. Health Mater. 2022, 11, 2102535. [Google Scholar] [CrossRef]
- Kumar, A.; Nune, K.C.; Misra, R.D.K. Design and biological functionality of a novel hybrid Ti-6Al-4V/hydrogel system for reconstruction of bone defects. J. Tissue Eng. Regen. Med. 2018, 12, 1133–1144. [Google Scholar] [CrossRef]
- ROS-scavenging hydrogel as protective carrier to regulate stem cells activity and promote osteointegration of 3D printed porous titanium prosthesis in osteoporosis. Front. Bioeng. Biotechnol. 2023, 11, 1103611. [CrossRef] [PubMed]
- Bai, H.; Cui, Y.; Wang, C.; Wang, Z.; Luo, W.; Liu, Y.; Leng, Y.; Wang, J.; Li, Z.; Liu, H. 3D printed porous biomimetic composition sustained release zoledronate to promote osteointegration of osteoporotic defects. Mater. Des. 2020, 189, 108513. [Google Scholar] [CrossRef]
- Diomede, F.; Gugliandolo, A.; Cardelli, P.; Merciaro, I.; Ettorre, V.; Traini, T.; Bedini, R.; Scionti, D.; Bramanti, A.; Nanci, A.; et al. Three-dimensional printed PLA scaffold and human gingival stem cell-derived extracellular vesicles: A new tool for bone defect repair. Stem Cell. Res. Ther. 2018, 9, 104. [Google Scholar]
- Guo, Y.; Ren, L.; Xie, K.; Wang, L.; Yu, B.; Jiang, W.; Zhao, Y.; Hao, Y. Functionalized TiCu/Ti-Cu-N-Coated 3D-Printed Porous Ti6Al4V Scaffold Promotes Bone Regeneration through BMSC Recruitment. Adv. Mater. Interfaces 2020, 7, 1901632. [Google Scholar] [CrossRef]
- Rashdan, N.A.; Sim, A.M.; Cui, L.; Phadwal, K.; Roberts, F.L.; Carter, R.; Ozdemir, D.D.; Hohenstein, P.; Hung, J.; Kaczynski, J.; et al. Osteocalcin Regulates Arterial Calcification Via Altered Wnt Signaling and Glucose Metabolism. J. Bone Miner. Res. 2020, 35, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Sivashanmugam, A.; Charoenlarp, P.; Deepthi, S.; Rajendran, A.; Nair, S.V.; Iseki, S.; Jayakumar, R. Injectable Shear-Thinning CaSO(4)/FGF-18-Incorporated Chitin-PLGA Hydrogel Enhances Bone Regeneration in Mice Cranial Bone Defect Model. ACS Appl. Mater. Interfaces 2017, 9, 42639–42652. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, Z.; Jiang, Y.; Liu, H.; Feng, Y.; Wang, Z.; Liu, H.; Wang, J.; Yang, B.; Lin, Q. Bioinspired mineral hydrogels as nanocomposite scaffolds for the promotion of osteogenic marker expression and the induction of bone regeneration in osteoporosis. Acta Biomater. 2020, 113, 614–626. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Liu, X.; Zhou, X.; Zhang, H.; Zhang, W.; Xiao, W.; Pan, G.; Cui, W.; Santos, H.A.; Shi, Q. Gelatin Templated Polypeptide Co-Cross-Linked Hydrogel for Bone Regeneration. Adv. Healthc. Mater. 2020, 9, 1901239. [Google Scholar] [CrossRef]
- Kim, H.D.; Hong, X.; An, Y.-H.; Park, M.J.; Kim, D.-G.; Greene, A.K.; Padwa, B.L.; Hwang, N.S.; Lin, R.-Z.; Melero-Martin, J.M. A Biphasic Osteovascular Biomimetic Scaffold for Rapid and Self-Sustained Endochondral Ossification. Adv. Health Mater. 2021, 10, e2100070. [Google Scholar] [CrossRef]
- Yang, Z.; Xie, L.; Zhang, B.; Zhang, G.; Huo, F.; Zhou, C.; Liang, X.; Fan, Y.; Tian, W.; Tan, Y. Preparation of BMP-2/PDA-BCP Bioceramic Scaffold by DLP 3D Printing and its Ability for Inducing Continuous Bone Formation. Front. Bioeng. Biotechnol. 2022, 10, 854693. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Wang, J.; Cao, Q.; Chen, F.; Wang, M.; Wu, Y.; Chen, X.; Zhu, X.; Zhang, X. Dopamine/DOPAC-assisted immobilization of bone morphogenetic protein-2 loaded Heparin/PEI nanogels onto three-dimentional printed calcium phosphate ceramics for enhanced osteoinductivity and osteogenicity. Biomater. Adv. 2022, 140, 854693. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Cheng, S.; Li, A.; Song, C.; Jiang, A.; Xu, F.; Chi, H.; Yan, J.; Chen, G. Fabrication of BMP-2-peptide-Deferoxamine- and QK-peptide-functionalized nanoscaffolds and their application for bone defect treatment. J. Tissue Eng. Regen. Med. 2022, 16, 1223–1237. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, S.; Wang, Y.; Yu, Z.; Ao, H.; Zhang, H.; Qin, L.; Guillaume, O.; Eglin, D.; Richards, R.G.; et al. Anti-infective efficacy, cytocompatibility and biocompatibility of a 3D-printed osteoconductive composite scaffold functionalized with quaternized chitosan. Acta Biomater. 2016, 46, 112–128. [Google Scholar] [PubMed]
- Yang, Y.; Chu, L.; Yang, S.; Zhang, H.; Qin, L.; Guillaume, O.; Eglin, D.; Richards, R.G.; Tang, T. Dual-functional 3D-printed composite scaffold for inhibiting bacterial infection and promoting bone regeneration in infected bone defect models. Acta Biomater. 2018, 79, 265–275. [Google Scholar] [CrossRef]
- Romanò, C.L.; Manzi, G.; Logoluso, N.; Romanò, D. Value of debridement and irrigation for the treatment of peri-prosthetic infections. A systematic review. Hip Int. 2012, 22 (Suppl. S8), S19–S24. [Google Scholar] [CrossRef]
- Yao, Q.-Q.; Zhou, J.; Jiang, C.-Z.; Sui, J.-S.; Li, J.-Y.; Xu, Y.; Wu, X.-L.; Liu, N.Q.; Buser, Z.; Wang, L.-M. Mechanical and In Vitro Antibacterial Properties of a Porous Ti-6Al-4V Scaffold Combined with Vancomycin-Loaded Polymethyl Methacrylate by Three-Dimensional Printing. J. Biomater. Tissue Eng. 2018, 8, 740–749. [Google Scholar] [CrossRef]
- Penn-Barwell, J.G.; Murray, C.K.; Wenke, J.C. Local antibiotic delivery by a bioabsorbable gel is superior to PMMA bead depot in reducing infection in an open fracture model. J. Orthop. Trauma. 2014, 28, 370–375. [Google Scholar]
- Arcos, D.; Vallet-Regi, M. Bioceramics for drug delivery. Acta Mater. 2013, 61, 890–911. [Google Scholar]
- Campoccia, D.; Montanaro, L.; Speziale, P.; Arciola, C.R. Antibiotic-loaded biomaterials and the risks for the spread of antibiotic resistance following their prophylactic and therapeutic clinical use. Biomaterials 2010, 31, 6363–6377. [Google Scholar] [PubMed]
- Chen, W.L.; Chang, W.N.; Chen, Y.S.; Hsieh, K.S.; Chen, C.K.; Peng, N.J.; Wu, K.S.; Cheng, M.F. Acute community-acquired osteoarticular infections in children: High incidence of concomitant bone and joint involvement. J. Microbiol. Immunol. Infect. 2010, 43, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.Y.; Davis, J.S.; Eichenberger, E.; Holland, T.L.; Fowler, V.G., Jr. Staphylococcus aureus infections: Epidemiology, pathophysiology, clinical manifestations, and management. Clin. Microbiol. Rev. 2015, 28, 603–661. [Google Scholar]
- Rodríguez-Pardo, D.; Pigrau, C.; Lora-Tamayo, J.; Soriano, A.; del Toro, M.D.; Cobo, J.; Palomino, J.; Euba, G.; Riera, M.; Sánchez-Somolinos, M.; et al. Gram-negative prosthetic joint infection: Outcome of a debridement, antibiotics and implant retention approach. A large multicentre study. Clin. Microbiol. Infect. 2014, 20, O911-9. [Google Scholar] [CrossRef] [PubMed]
- Lamagni, T.; Elgohari, S.; Harrington, P. Trends in surgical site infections following orthopaedic surgery. Curr. Opin. Infect. Dis. 2015, 28, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Hwang, J.S.; Lee, D.G. Periplanetasin-2 Enhances the Antibacterial Properties of Vancomycin or Chloramphenicol in Escherichia coli. J. Microbiol. Biotechnol. 2021, 31, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Hua, X.; Xue, Z.; Ma, J. Cajanin Stilbene Acid Inhibited Vancomycin-Resistant Enterococcus by Inhibiting Phosphotransferase System. Front. Pharmacol. 2020, 11, 473. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Guo, Y.; Dong, Y.; Wu, Y.; Cheng, L.; Wang, Y.; Xing, M.; Yuan, Q. A Novel Nanosilver/Nanosilica Hydrogel for Bone Regeneration in Infected Bone Defects. ACS Appl. Mater. & Inter. 2016, 8, 13242–13250. [Google Scholar]
- Pizzicannella, J.; Diomede, F.; Gugliandolo, A.; Chiricosta, L.; Bramanti, P.; Merciaro, I.; Orsini, T.; Mazzon, E.; Trubiani, O. 3D Printing PLA/Gingival Stem Cells/ EVs Upregulate miR-2861 and -210 during Osteoangiogenesis Commitment. Int. J. Mol. Sci. 2019, 20, 3256. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Genes | Primers |
|---|---|
| Runx-2 | F: 5′-AGAGTCAGATTACAGATCCCAGG-3′ |
| R: 5′-TGGCTCTTCTTACTGAGAGAGG-3′ | |
| COL-I | F:5′-GATGTTGAACTTGTTGTTGCTGAGGG-3′ |
| R:5′-GGCAGGCGAGATGGCTTATT-3′ | |
| BSP | F:5′-AAAAGTGAAGGAAAGCGACGAG-3′ |
| R:5′-CGTGGAGTTGGTGCTGGTG-3′ | |
| OCN | F:5′-GAACAGACAAGTCCCACACAGC-3′ |
| R:5′-TCAGCAGAGTGAGCAGAAAGAT-3′ | |
| GAPDH | F:5′-CTCGTCCCGTAGACAAAATGGT-3′ |
| R:5′-GAGGTCAATGAAGGGGTCGTT-3′ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pu, Y.; Lin, X.; Zhi, Q.; Qiao, S.; Yu, C. Microporous Implants Modified by Bifunctional Hydrogel with Antibacterial and Osteogenic Properties Promote Bone Integration in Infected Bone Defects. J. Funct. Biomater. 2023, 14, 226. https://doi.org/10.3390/jfb14040226
Pu Y, Lin X, Zhi Q, Qiao S, Yu C. Microporous Implants Modified by Bifunctional Hydrogel with Antibacterial and Osteogenic Properties Promote Bone Integration in Infected Bone Defects. Journal of Functional Biomaterials. 2023; 14(4):226. https://doi.org/10.3390/jfb14040226
Chicago/Turabian StylePu, Yiping, Xuecai Lin, Qiang Zhi, Shichong Qiao, and Chuangqi Yu. 2023. "Microporous Implants Modified by Bifunctional Hydrogel with Antibacterial and Osteogenic Properties Promote Bone Integration in Infected Bone Defects" Journal of Functional Biomaterials 14, no. 4: 226. https://doi.org/10.3390/jfb14040226