Evidence of Mitochondrial Dysfunction in Fibromyalgia: Deviating Muscle Energy Metabolism Detected Using Microdialysis and Magnetic Resonance

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects
2.2. Procedures
2.3. Clinical Examinations
2.3.1. Pressure Pain Thresholds
2.3.2. Physical tests
Hand function
Aerobic fitness test
Lower extremity muscle performance
2.4. Questionnaire
2.4.1. Pain aspects
2.4.2. Psychological distress
2.4.3. Disability
2.4.4. Health aspects
2.5. Microdialysis and Sample Preparation
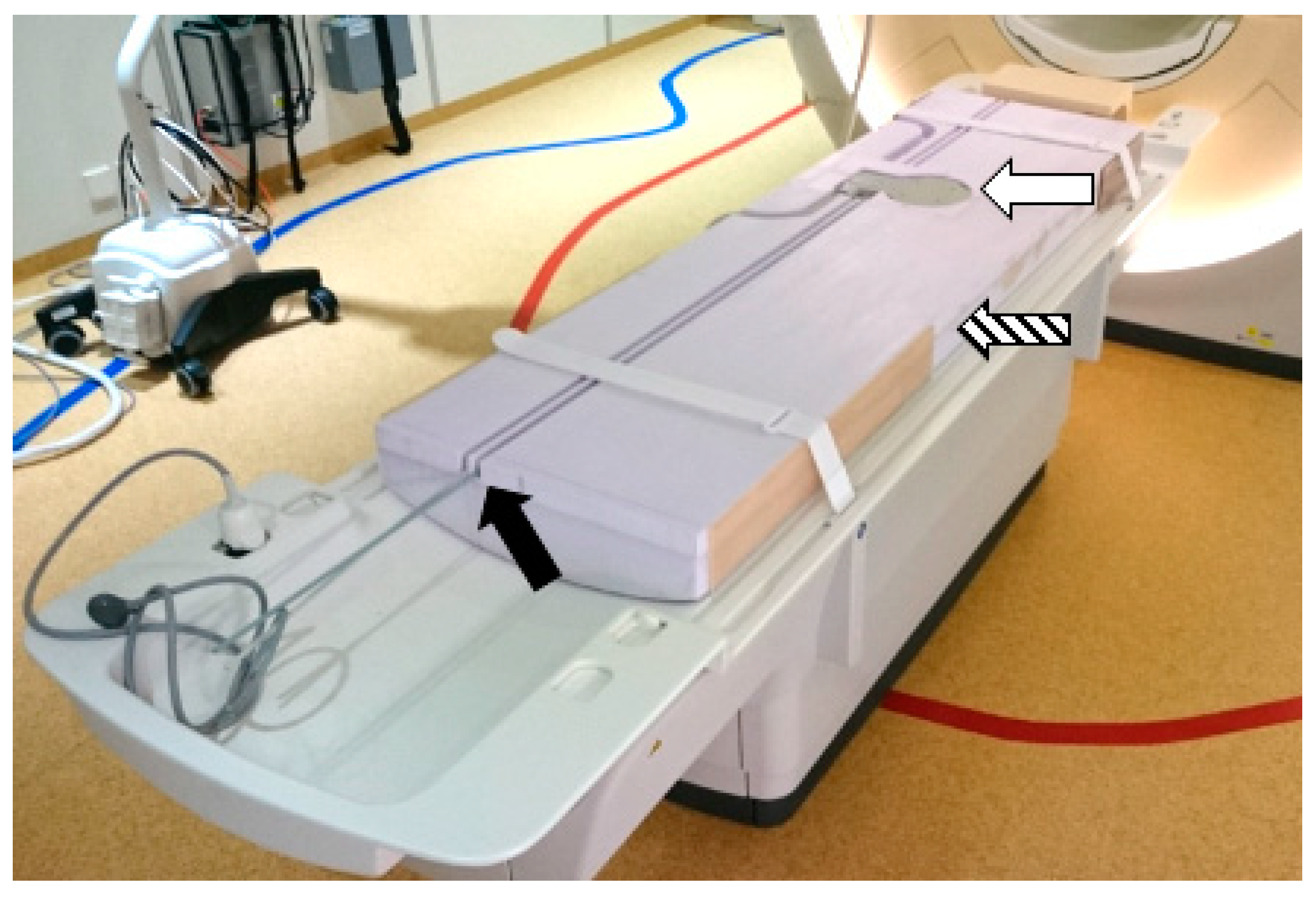
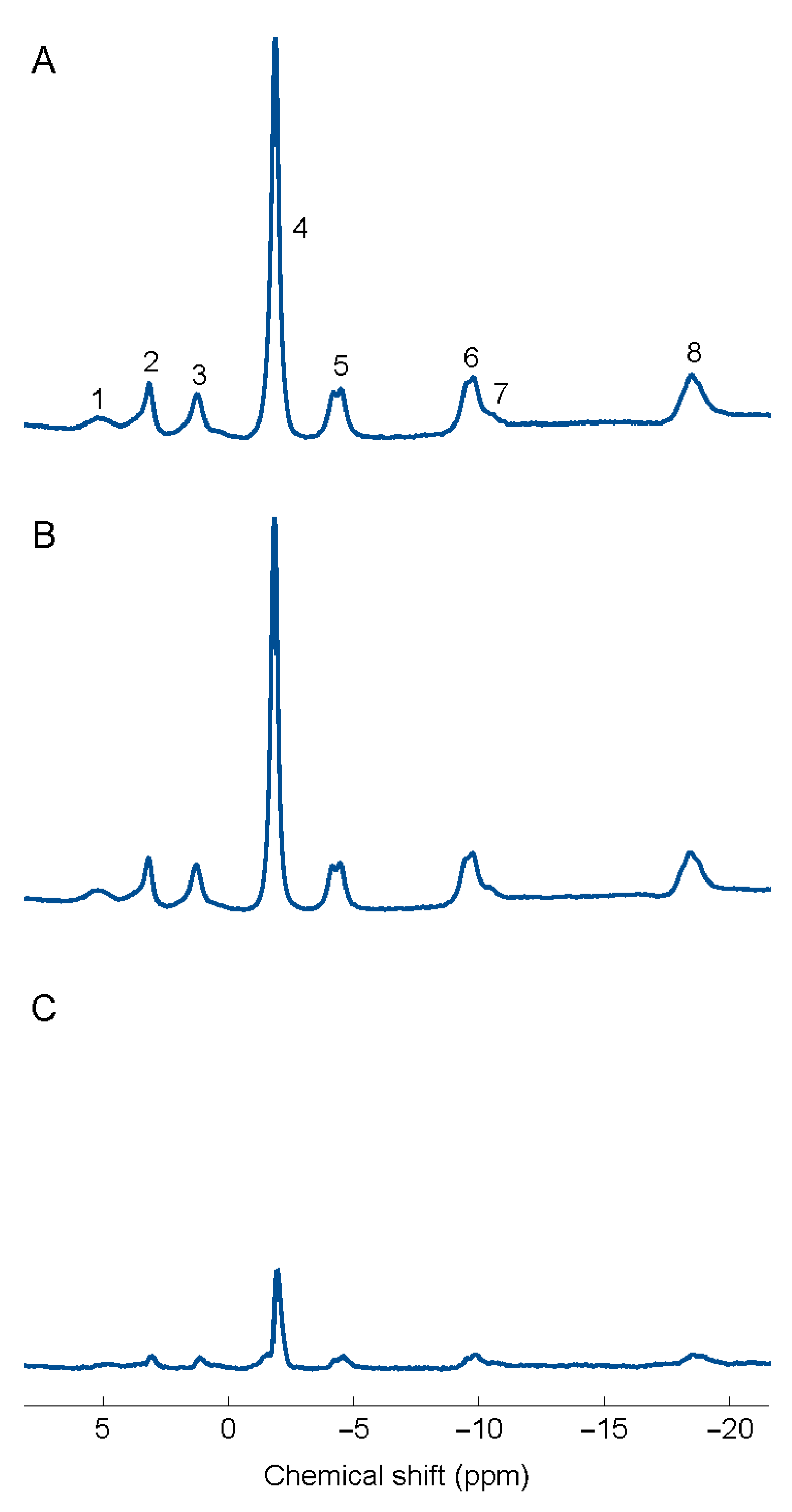
2.6. Magnetic Resonance Spectroscopy of Erector Spinae
2.7. Statistics
3. Results
3.1. Data from Questionnaires and Clinical Examinations
3.2. Microdialysis (MD)
3.3. Spectroscopy (31P-MRS)
3.4. Regression Analyses
3.4.1. Group Membership
3.4.2. Pain Intensity in FM
3.4.3. Pressure Pain Thresholds (PPT) for Trapezius and Erector Spinae
PPT of trapezius
PPT of Erector spinae
3.4.4. Blood Flow in Erector Spinae
3.4.5. Physical Tests
4. Discussion
4.1. Major Results
4.2. Significantly Higher Levels of Pyruvate in FM
4.3. Lower Absolute Concentrations of PCr and ATP of Erector Spinae in FM
4.4. What is the Explanation for Metabolic and Blood Flow Alterations?
4.5. What Is the Reason for Mitochondrial Dysfunction?
4.6. Multivariate Associations between Pain Aspects and Spectroscopy and MD Variables
4.7. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability Statement
References
- Albrecht, D.S.; Forsberg, A.; Sandstrom, A.; Bergan, C.; Kadetoff, D.; Protsenko, E.; Lampa, J.; Lee, Y.C.; Hoglund, C.O.; Catana, C.; et al. Brain glial activation in fibromyalgia—A multi-site positron emission tomography investigation. Brain Behav. Immun. 2019, 75, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Gerdle, B.; Larsson, B. Muscle. In Fibromyalgia Syndrome and Widespread Pain—From Construction to Relevant Recognition; Häuser, W., Perrot, S., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2018; pp. 215–231. [Google Scholar]
- Jensen, K.B.; Kosek, E.; Petzke, F.; Carville, S.; Fransson, P.; Marcus, H.; Williams, S.C.R.; Choy, E.; Giesecke, T.; Mainguy, Y.; et al. Evidence of dysfunctional pain inhibition in Fibromyalgia reflected in rACC during provoked pain. PAIN 2009, 144, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Clauw, D.J. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience 2016, 338, 114–129. [Google Scholar] [CrossRef] [PubMed]
- Üçeyler, N.; Sommer, C. Small nerve fiber pathology. In Fibromylagia Syndrome and Widespread Pain—From Construction to Relevant Recognition; Häuser, W., Perrot, S., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2018; pp. 204–214. [Google Scholar]
- Frontera, W.R.; Ochala, J. Skeletal muscle: A brief review of structure and function. Calcif. Tissue Int. 2015, 96, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Bender, T.; Martinou, J.C. The mitochondrial pyruvate carrier in health and disease: To carry or not to carry? Biochim. Biophys. Acta 2016, 1863, 2436–2442. [Google Scholar] [CrossRef] [PubMed]
- Geto, Z.; Molla, M.D.; Challa, F.; Belay, Y.; Getahun, T. Mitochondrial Dynamic Dysfunction as a Main Triggering Factor for Inflammation Associated Chronic Non-Communicable Diseases. J. Inflamm. Res. 2020, 13, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerdle, B.; Soderberg, K.; Salvador Puigvert, L.; Rosendal, L.; Larsson, B. Increased interstitial concentrations of pyruvate and lactate in the trapezius muscle of patients with fibromyalgia: A microdialysis study. J. Rehabil. Med. 2010, 42, 679–687. [Google Scholar] [CrossRef] [Green Version]
- Gerdle, B.; Larsson, B.; Forsberg, F.; Ghafouri, N.; Karlsson, L.; Stensson, N.; Ghafouri, B. Chronic Widespread Pain: Increased Glutamate and Lactate Concentrations in the Trapezius Muscle and Plasma. Clin. J. Pain 2014, 30, 409–420. [Google Scholar] [CrossRef]
- Gerdle, B.; Ernberg, M.; Mannerkorpi, K.; Larsson, B.; Kosek, E.; Christidis, N.; Ghafouri, B. Increased Interstitial Concentrations of Glutamate and Pyruvate in Vastus Lateralis of Women with Fibromyalgia Syndrome Are Normalized after an Exercise Intervention—A Case-Control Study. PLoS ONE 2016, 11, e0162010. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, P.; Harmsen, E.; Ho, C.; Vogel, H.J. Nuclear magnetic resonance studies of cellular metabolism. Anal. Biochem. 1990, 191, 193–222. [Google Scholar] [CrossRef]
- Kemp, G.J.; Meyerspeer, M.; Moser, E. Absolute quantification of phosphorus metabolite concentrations in human muscle in vivo by 31P MRS: A quantitative review. NMR Biomed. 2007, 20, 555–565. [Google Scholar] [CrossRef]
- Gerdle, B.; Forsgren, M.; Bengtsson, A.; Dahlqvist Leinhard, O.; Sören, B.; Karlsson, A.; Brandejsky, V.; Lund, E.; Lundberg, P. Decreased muscle concentrations of ATP and PCR in the quadriceps muscle of fibromyalgia patients—A 31P MRS study. Eur. J. Pain 2013, 17, 1205–1215. [Google Scholar] [CrossRef]
- Park, J.H.; Phothimat, P.; Oates, C.T.; Hernanz-Schulman, M.; Olsen, N.J. Use of P-31 magnetic resonance spectroscopy to detect metabolic abnormalities in muscles of patients with fibromyalgia. Arthritis Rheum. 1998, 41, 406–413. [Google Scholar] [CrossRef]
- Dupont, W.; Plummer, W. Power and Sample Size Calculations: A Review and Computer Program. Control. Clin. Trials 1990, 11, 116–128. [Google Scholar] [CrossRef]
- Rosendal, L.; Larsson, B.; Kristiansen, J.; Peolsson, M.; Søgaard, K.; Kjaer, M.; Sørensen, J.; Gerdle, B. Increase in muscle nociceptive substances and anaerobic metabolism in patients with trapezius myalgia: Microdialysis in rest and during exercise. Pain 2004, 112, 324–334. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Hauser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: A modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J. Rheumatol. 2011, 38, 1113–1122. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Hauser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Wallin, M.; Liedberg, G.; Borsbo, B.; Gerdle, B. Thermal detection and pain thresholds but not pressure pain thresholds are correlated with psychological factors in women with chronic whiplash-associated pain. Clin. J. Pain 2012, 28, 211–221. [Google Scholar] [CrossRef]
- Lemming, D.; Borsbo, B.; Sjors, A.; Lind, E.B.; Arendt-Nielsen, L.; Graven-Nielsen, T.; Gerdle, B. Single-point but not tonic cuff pressure pain sensitivity is associated with level of physical fitness—A study of non-athletic healthy subjects. PLoS ONE 2015, 10, e0125432. [Google Scholar] [CrossRef] [PubMed]
- Nordenskiöld, U.; Grimby, G. Grip force in patients with rheumatoid arthritis and fibromyalgia and in healthy subjects. A study with the Grippit instrument. Scand. J. Rheumatol. 1993, 22, 14–19. [Google Scholar] [CrossRef]
- Åstrand, P.; Rodahl, K. Textbook of Work Physiology; McGraw-Hill: New York, NY, USA, 1986. [Google Scholar]
- Csuka, M.; McCarty, D. Simple method for measurement of lower extremity muscle strength. Am. J. Med. 1985, 78, 77–81. [Google Scholar] [CrossRef]
- Newcomer, K.; Krug, H.; Mahowald, M. Validity and reliability of the timed-stands test for patients with rheumatoid arthritis and other chronic diseases. J. Rheumatol. 1993, 20, 21–27. [Google Scholar] [PubMed]
- Ruscheweyh, R.; Marziniak, M.; Stumpenhorst, F.; Reinholz, J.; Knecht, S. Pain sensitivity can be assessed by self-rating: Development and validation of the Pain Sensitivity Questionnaire. Pain 2009, 146, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Larsson, B.; Gerdle, B.; Bjork, J.; Grimby-Ekman, A. Pain Sensitivity and its Relation to Spreading on the Body, Intensity, Frequency, and Duration of Pain: A Cross-Sectional Population-Based Study (SwePain). Clin. J. Pain 2017, 33, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Ruscheweyh, R.; Yeo, J.H.; Cho, H.G.; Yi, J.M.; Chang, B.S.; Lee, C.K.; Yeom, J.S. Translation, cross-cultural adaptation, and validity of the Korean version of the pain sensitivity questionnaire in chronic pain patients. Pain Pract. 2014, 14, 745–751. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Verneuer, B.; Dany, K.; Marziniak, M.; Wolowski, A.; Colak-Ekici, R.; Schulte, T.L.; Bullmann, V.; Grewe, S.; Gralow, I.; et al. Validation of the pain sensitivity questionnaire in chronic pain patients. Pain 2012, 153, 1210–1218. [Google Scholar] [CrossRef]
- Sellers, A.B.; Ruscheweyh, R.; Kelley, B.J.; Ness, T.J.; Vetter, T.R. Validation of the English language pain sensitivity questionnaire. Reg. Anesth. Pain Med. 2013, 38, 508–514. [Google Scholar] [CrossRef] [Green Version]
- Valeberg, B.T.; Pedersen, L.M.; Girotto, V.; Christensen, V.L.; Stubhaug, A. Validation of the Norwegian Pain Sensitivity Questionnaire. J. Pain Res. 2017, 10, 1137–1142. [Google Scholar] [CrossRef] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LoMartire, R.; Ang, B.O.; Gerdle, B.; Vixner, L. Psychometric properties of Short Form-36 Health Survey, EuroQol 5-dimensions, and Hospital Anxiety and Depression Scale in patients with chronic pain. Pain 2020, 161, 83–95. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.J.; Bishop, S.R.; Pivik, J.R. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Miro, J.; Nieto, R.; Huguet, A. The Catalan version of the Pain Catastrophizing Scale: A useful instrument to assess catastrophic thinking in whiplash patients. J. Pain 2008, 9, 397–406. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Belanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Chibnall, J.T.; Tait, R.C. The Pain Disability Index: Factor structure and normative data. Arch. Phys. Med. Rehabil. 1994, 75, 1082–1086. [Google Scholar] [CrossRef]
- Tait, R.C.; Chibnall, J.T.; Krause, S. The Pain Disability Index: Psychometric properties. Pain 1990, 40, 171–182. [Google Scholar] [CrossRef]
- The EuroQol Group. EuroQol: A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Hermens, H.; Fredriks, B. SENIAM The State of the Art on Sensors and Sensor Placement Procedures for Surface Elecromyography: A Proposal for Sensor Placement Procedures; Roessingh Research and Development: Enschede, The Netherlands, 1997. [Google Scholar]
- Scheller, D.; Kolb, J. The internal reference technique in microdialysis: A practical approach to monitoring dialysis efficiency and to calculating tissue concentration from dialysate samples. J. Neurosci. Methods 1991, 40, 31–38. [Google Scholar] [CrossRef]
- Hickner, R.; Bone, D.; Ungerstedt, U.; Jorfeldt, L.; Henriksson, J. Muscle blood flow during intermittent exercise: Comparison of the microdialysis ethanol technique and 133Xe clearance. Clin. Sci. (Lond.) 1994, 86, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Stallknecht, B.; Donsmark, M.; Enevoldsen, L.H.; Fluckey, J.D.; Galbo, H. Estimation of rat muscle blood flow by microdialysis probes perfused with ethanol, [14C]ethanol, and 3H2O. J. Appl. Physiol. 1999, 86, 1054–1061. [Google Scholar] [CrossRef]
- Naressi, A.; Couturier, C.; Devos, J.M.; Janssen, M.; Mangeat, C.; de Beer, R.; Graveron-Demilly, D. Java-based graphical user interface for the MRUI quantitation package. MAGMA 2001, 12, 141–152. [Google Scholar] [CrossRef]
- Vanhamme, L.; van den Boogaart, A.; Van Huffel, S. Improved method for accurate and efficient quantification of MRS data with use of prior knowledge. J. Magn. Reson. 1997, 129, 35–43. [Google Scholar] [CrossRef] [Green Version]
- De Graaf, R. In Vivo NMR Spectroscopy: Principles and Techniques, 2nd ed.; John Wiley & Sons: Chichester, UK, 2007. [Google Scholar]
- Bogner, W.; Chmelik, M.; Schmid, A.I.; Moser, E.; Trattnig, S.; Gruber, S. Assessment of (31)P relaxation times in the human calf muscle: A comparison between 3 T and 7 T in vivo. Magn. Reson. Med. 2009, 62, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Ringqvist, Å.; Dragioti, E.; Björk, M.; Larsson, B.; Gerdle, B. Moderate and stable pain reductions as a result of Interdisciplinary Pain Rehabilitation—A cohort study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). J. Clin. Med. 2019, 8, 905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheelock, A.M.; Wheelock, C.E. Trials and tribulations of ’omics data analysis: Assessing quality of SIMCA-based multivariate models using examples from pulmonary medicine. Mol. Biosyst. 2013, 9, 2589–2596. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, L.; Byrne, T.; Johansson, E.; Trygg, J.; Vikström, C. Multi- and Megavariate Data Analysis: Basic Principles and Applications, 3rd ed.; MKS Umetrics AB: Malmö, Sweden, 2013. [Google Scholar]
- McCommis, K.S.; Finck, B.N. Mitochondrial pyruvate transport: A historical perspective and future research directions. Biochem. J. 2015, 466, 443–454. [Google Scholar] [CrossRef] [Green Version]
- Brooks, G.A. The Science and Translation of Lactate Shuttle Theory. Cell Metab. 2018, 27, 757–785. [Google Scholar] [CrossRef] [PubMed]
- Schurr, A. Lactate, Not. Pyruvate, Is the End Product of Glucose Metabolism via Glycolysis. Carbohydrate 2017. [Google Scholar] [CrossRef] [Green Version]
- Rogatzki, M.J.; Ferguson, B.S.; Goodwin, M.L.; Gladden, L.B. Lactate is always the end product of glycolysis. Front. Neurosci. 2015, 9, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glancy, B.; Kane, D.A.; Kavazis, A.N.; Goodwin, M.L.; Willis, W.T.; Gladden, L.B. Mitochondrial lactate metabolism: History and implications for exercise and disease. J. Physiol. 2020. [Google Scholar] [CrossRef]
- Layec, G.; Trinity, J.D.; Hart, C.R.; Kim, S.E.; Groot, H.J.; Le Fur, Y.; Sorensen, J.R.; Jeong, E.K.; Richardson, R.S. Impact of age on exercise-induced ATP supply during supramaximal plantar flexion in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, R378–R388. [Google Scholar] [CrossRef] [Green Version]
- Hargreaves, M.; Spriet, L.L. Skeletal muscle energy metabolism during exercise. Nat. Metab. 2020, 2, 817–828. [Google Scholar] [CrossRef]
- Li, M.; Chen, F.; Wang, H.; Wu, W.; Zhang, X.; Tian, C.; Yu, H.; Liu, R.; Zhu, B.; Zhang, B.; et al. Non-invasive assessment of phosphate metabolism and oxidative capacity in working skeletal muscle in healthy young Chinese volunteers using (31)P Magnetic Resonance Spectroscopy. PeerJ 2016, 4, e2259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gouspillou, G.; Bourdel-Marchasson, I.; Rouland, R.; Calmettes, G.; Biran, M.; Deschodt-Arsac, V.; Miraux, S.; Thiaudiere, E.; Pasdois, P.; Detaille, D.; et al. Mitochondrial energetics is impaired in vivo in aged skeletal muscle. Aging Cell 2014, 13, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Dominguez, B.; Bullon, P.; Roman-Malo, L.; Marin-Aguilar, F.; Alcocer-Gomez, E.; Carrion, A.M.; Sanchez-Alcazar, J.A.; Cordero, M.D. Oxidative stress, mitochondrial dysfunction and, inflammation common events in skin of patients with Fibromyalgia. Mitochondrion 2015, 21, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Bazzichi, L.; Giannaccini, G.; Betti, L.; Fabbrini, L.; Schmid, L.; Palego, L.; Giacomelli, C.; Rossi, A.; Giusti, L.; De Feo, F.; et al. ATP, calcium and magnesium levels in platelets of patients with primary fibromyalgia. Clin. Biochem. 2008, 41, 1084–1090. [Google Scholar] [CrossRef]
- García, J.; Carvajal-Gil, J.; Herrero-Olea, A.; Gómez-Galán, R. Altered Inflammatory Mediators in Fibromyalgia. Rheumatology 2017, 7. [Google Scholar] [CrossRef] [Green Version]
- Weibel, E.R.; Hoppeler, H. Exercise-induced maximal metabolic rate scales with muscle aerobic capacity. J. Exp. Biol. 2005, 208, 1635–1644. [Google Scholar] [CrossRef] [Green Version]
- Picard, M.; Gentil, B.J.; McManus, M.J.; White, K.; St Louis, K.; Gartside, S.E.; Wallace, D.C.; Turnbull, D.M. Acute exercise remodels mitochondrial membrane interactions in mouse skeletal muscle. J. Appl. Physiol. (1985) 2013, 115, 1562–1571. [Google Scholar] [CrossRef]
- Hood, D.A.; Memme, J.M.; Oliveira, A.N.; Triolo, M. Maintenance of Skeletal Muscle Mitochondria in Health, Exercise, and Aging. Annu. Rev. Physiol. 2019, 81, 19–41. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, A. Editorial, The muscle in fibromyalgia. Rheumatology 2002, 41, 721–724. [Google Scholar] [CrossRef] [Green Version]
- Bengtsson, A.; Henriksson, K.G.; Larsson, J. Muscle biopsy in primary fibromyalgia. Light-microscopical and histochemical findings. Scand. J. Rheumatol. 1986, 15, 1–6. [Google Scholar] [PubMed]
- Lindh, M.; Johansson, G.; Hedberg, M.; Henning, G.B.; Grimby, G. Muscle fiber characteristics, capillaries and enzymes in patients with fibromyalgia and controls. Scand. J. Rheumatol. 1995, 24, 34–37. [Google Scholar] [CrossRef]
- Drewes, A.M.; Andreasen, A.; Schroder, H.D.; Hogsaa, B.; Jennum, P. Pathology of skeletal muscle in fibromyalgia: A histo-immuno-chemical and ultrastructural study. Br. J. Rheumatol. 1993, 32, 479–483. [Google Scholar] [CrossRef]
- Jacobsen, S.; Bartels, E.M.; Danneskiold-Samsoe, B. Single cell morphology of muscle in patients with chronic muscle pain. Scand. J. Rheumatol. 1991, 20, 336–343. [Google Scholar] [CrossRef]
- De Meulemeester, K.; Cagnie, B.; Van Dorpe, J.; Lammens, M.; Petrovic, M.; Calders, P. Differences in the Mitochondrial and Lipid Droplet Morphology in Female Office Workers With Trapezius Myalgia, Compared with Healthy Controls: A Muscle Biopsy Study. Am. J. Phys. Med. Rehabil. 2019, 98, 989–997. [Google Scholar] [CrossRef]
- Tan, E.C.; Janssen, A.J.; Roestenberg, P.; van den Heuvel, L.P.; Goris, R.J.; Rodenburg, R.J. Mitochondrial dysfunction in muscle tissue of complex regional pain syndrome type I patients. Eur. J. Pain 2011, 15, 708–715. [Google Scholar] [PubMed]
- Niyazov, D.M.; Kahler, S.G.; Frye, R.E. Primary Mitochondrial Disease and Secondary Mitochondrial Dysfunction: Importance of Distinction for Diagnosis and Treatment. Mol. Syndromol. 2016, 7, 122–137. [Google Scholar] [CrossRef] [Green Version]
- Olausson, P.; Gerdle, B.; Ghafouri, N.; Sjostrom, D.; Blixt, E.; Ghafouri, B. Protein alterations in women with chronic widespread pain—An explorative proteomic study of the trapezius muscle. Sci. Rep. 2015, 5, 11894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menzies, V.; Starkweather, A.; Yao, Y.; Thacker, L.R., 2nd; Garrett, T.J.; Swift-Scanlan, T.; Kelly, D.L.; Patel, P.; Lyon, D.E. Metabolomic Differentials in Women With and Without Fibromyalgia. Clin. Transl. Sci. 2020, 13, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Malatji, B.G.; Meyer, H.; Mason, S.; Engelke, U.F.H.; Wevers, R.A.; van Reenen, M.; Reinecke, C.J. A diagnostic biomarker profile for fibromyalgia syndrome based on an NMR metabolomics study of selected patients and controls. BMC Neurol. 2017, 17, 88. [Google Scholar] [CrossRef]
- Malatji, B.G.; Mason, S.; Mienie, L.J.; Wevers, R.A.; Meyer, H.; van Reenen, M.; Reinecke, C.J. The GC-MS metabolomics signature in patients with fibromyalgia syndrome directs to dysbiosis as an aspect contributing factor of FMS pathophysiology. Metabolomics 2019, 15, 54. [Google Scholar] [CrossRef] [PubMed]
- Ghafouri, N.; Ghafouri, B.; Larsson, B.; Stensson, N.; Fowler, C.J.; Gerdle, B. Palmitoylethanolamide and stearoylethanolamide levels in the interstitium of the trapezius muscle of women with chronic widespread pain and chronic neck-shoulder pain correlate with pain intensity and sensitivity. Pain 2013, 154, 1649–1658. [Google Scholar] [CrossRef]
- Stensson, N.; Gerdle, B.; Ernberg, M.; Mannerkorpi, K.; Kosek, E.; Ghafouri, B. Increased Anandamide and Decreased Pain and Depression after Exercise in Fibromyalgia. Med. Sci. Sports Exerc. 2020, 52, 1617–1628. [Google Scholar] [CrossRef]
- Jablochkova, A.; Backryd, E.; Kosek, E.; Mannerkorpi, K.; Ernberg, M.; Gerdle, B.; Ghafouri, B. Unaltered low nerve growth factor and high brain-derived neurotrophic factor levels in plasma from patients with fibromyalgia after a 15-week progressive resistance exercise. J. Rehabil. Med. 2019, 51, 779–787. [Google Scholar] [CrossRef] [Green Version]
- Ernberg, M.; Christidis, N.; Ghafouri, B.; Bileviciute-Ljungar, I.; Lofgren, M.; Larsson, A.; Palstam, A.; Bjersing, J.; Mannerkorpi, K.; Kosek, E.; et al. Effects of 15 weeks of resistance exercise on pro-inflammatory cytokine levels in the vastus lateralis muscle of patients with fibromyalgia. Arthritis Res. Ther. 2016, 18, 137. [Google Scholar] [CrossRef] [Green Version]
- Wahlen, K.; Ernberg, M.; Kosek, E.; Mannerkorpi, K.; Gerdle, B.; Ghafouri, B. Significant correlation between plasma proteome profile and pain intensity, sensitivity, and psychological distress in women with fibromyalgia. Sci. Rep. 2020, 10, 12508. [Google Scholar] [CrossRef] [PubMed]
- Wåhlén, K.; Olausson, P.; Carlsson, A.; Ghafouri, N.; Gerdle, B. Systemic alteration of plasma proteins from women with chronic widespread pain compared to healthy controls; a proteomic study. J. Pain Res. 2017, 10, 797–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, C.L.; Sheng, Y.C.; Wang, S.Y.; Chen, Y.H.; Kang, J.H. Serum proteome profiles revealed dysregulated proteins and mechanisms associated with fibromyalgia syndrome in women. Sci. Rep. 2020, 10, 12347. [Google Scholar] [CrossRef]
- Vaamonde-Garcia, C.; Lopez-Armada, M.J. Role of mitochondrial dysfunction on rheumatic diseases. Biochem. Pharmacol. 2019, 165, 181–195. [Google Scholar] [CrossRef] [PubMed]
- Groen, M.B.; Knudsen, T.A.; Finsen, S.H.; Pedersen, B.K.; Hellsten, Y.; Mortensen, S.P. Reduced skeletal-muscle perfusion and impaired ATP release during hypoxia and exercise in individuals with type 2 diabetes. Diabetologia 2019, 62, 485–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulshreshtha, P.; Deepak, K.K. Autonomic nervous system profile in fibromyalgia patients and its modulation by exercise: A mini review. Clin. Physiol. Funct. Imaging 2013, 33, 83–91. [Google Scholar] [CrossRef]
- Shang, Y.; Gurley, K.; Symons, B.; Long, D.; Srikuea, R.; Crofford, L.J.; Peterson, C.A.; Yu, G. Noninvasive optical characterization of muscle blood flow, oxygenation, and metabolism in women with fibromyalgia. Arthritis Res. Ther. 2012, 14, R236. [Google Scholar] [CrossRef] [Green Version]
- Nelson, N.L. Muscle strengthening activities and fibromyalgia: A review of pain and strength outcomes. J. Bodyw. Mov. Ther. 2015, 19, 370–376. [Google Scholar] [CrossRef]
- Umay, E.; Gundogdu, I.; Ozturk, E.A. What happens to muscles in fibromyalgia syndrome. Ir. J. Med. Sci. 2020, 189, 749–756. [Google Scholar] [CrossRef]
- Hood, D.A.; Tryon, L.D.; Carter, H.N.; Kim, Y.; Chen, C.C. Unravelling the mechanisms regulating muscle mitochondrial biogenesis. Biochem. J. 2016, 473, 2295–2314. [Google Scholar] [CrossRef] [Green Version]
- Hauser, W.; Klose, P.; Langhorst, J.; Moradi, B.; Steinbach, M.; Schiltenwolf, M.; Busch, A. Efficacy of different types of aerobic exercise in fibromyalgia syndrome: A systematic review and meta-analysis of randomised controlled trials. Arthritis Res. Ther. 2010, 12, R79. [Google Scholar] [CrossRef] [Green Version]
- Sosa-Reina, M.D.; Nunez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martin, D.; Monserrat, J.; Alvarez-Mon, M. Effectiveness of Therapeutic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Biomed. Res. Int. 2017, 2017, 2356346. [Google Scholar] [CrossRef] [PubMed]
- Padrao, A.I.; Ferreira, R.; Amado, F.; Vitorino, R.; Duarte, J.A. Uncovering the exercise-related proteome signature in skeletal muscle. Proteomics 2016, 16, 816–830. [Google Scholar] [CrossRef] [PubMed]
- Kras, K.A.; Hoffman, N.; Roust, L.R.; Benjamin, T.R.; De Filippis, E.A.; Katsanos, C.S. Adenosine Triphosphate Production of Muscle Mitochondria after Acute Exercise in Lean and Obese Humans. Med. Sci. Sports Exerc. 2019, 51, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Elert, J.; Aspegren Kendall, S.; Larsson, B.; Månsson, B.; Gerdle, B. Chronic pain and difficulty in relaxing postural muscles in patients with fibromylgia and chronic whiplash associated disorders. J. Rheumatol. 2001, 28, 1361–1368. [Google Scholar] [PubMed]
- Gerdle, B.; Grönlund, C.; Karlsson, S.; Holtermann, A.; Roeleveld, K. Altered neuromuscular control mechanisms of the trapezius muscle in fibromyalgia. BMC Musculoskelet. Disord. 2010, 11, 42. [Google Scholar] [CrossRef] [Green Version]
- Bazzichi, L.; Dini, M.; Rossi, A.; Corbianco, S.; De Feo, F.; Giacomelli, C.; Zirafa, C.; Ferrari, C.; Rossi, B.; Bombardieri, S. Muscle modifications in fibromyalgic patients revealed by surface electromyography (SEMG) analysis. BMC Musculoskelet. Disord. 2009, 10, 36. [Google Scholar] [CrossRef] [Green Version]
- Falla, D.; Andersen, H.; Danneskiold-Samsøe, B.; Arendt-Nielsen, L.; Farina, D. Adaptations of upper trapezius muscle activity during sustained contractions in women with fibromyalgia. J. Electromyogr. Kinesiol. 2010, 20, 457–464. [Google Scholar] [CrossRef]
- de Paoli, F.V.; Ortenblad, N.; Pedersen, T.H.; Jorgensen, R.; Nielsen, O.B. Lactate per se improves the excitability of depolarized rat skeletal muscle by reducing the Cl- conductance. J. Physiol. 2010, 588, 4785–4794. [Google Scholar] [CrossRef]
- van Hall, G. Lactate kinetics in human tissues at rest and during exercise. Acta Physiol. 2010, 199, 499–508. [Google Scholar] [CrossRef]
- Olausson, P.; Ghafouri, B.; Ghafouri, N.; Gerdle, B. Specific proteins of the trapezius muscle correlate with pain intensity and sensitivity—An explorative multivariate proteomic study of the trapezius muscle in women with chronic widespread pain. J. Pain Res. 2016, 9, 345–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahlen, K.; Ghafouri, B.; Ghafouri, N.; Gerdle, B. Plasma Protein Pattern Correlates with Pain Intensity and Psychological Distress in Women with Chronic Widespread Pain. Front. Psychol. 2018, 9, 2400. [Google Scholar] [CrossRef]
- Gerdle, B.; Ghafouri, B.; Ghafouri, N.; Bäckryd, E.; Gordh, T. Signs of ongoing inflammation in female patients with chronic widespread pain—A multivariate, explorative, cross-sectional study of blood samples. Medicine 2017, 96, e6130. [Google Scholar] [CrossRef]
- Palmer, S.; Bailey, J.; Brown, C.; Jones, A.; McCabe, C.S. Sensory Function and Pain Experience in Arthritis, Complex Regional Pain Syndrome, Fibromyalgia Syndrome, and Pain-Free Volunteers: A Cross-Sectional Study. Clin. J. Pain 2019, 35, 894–900. [Google Scholar] [CrossRef]
- Goubert, D.; Danneels, L.; Graven-Nielsen, T.; Descheemaeker, F.; Meeus, M. Differences in Pain Processing Between Patients with Chronic Low Back Pain, Recurrent Low Back Pain, and Fibromyalgia. Pain Physician 2017, 20, 307–318. [Google Scholar]
- Potvin, S.; Marchand, S. Pain facilitation and pain inhibition during conditioned pain modulation in fibromyalgia and in healthy controls. Pain 2016, 157, 1704–1710. [Google Scholar] [CrossRef]
- O’Brien, A.T.; Deitos, A.; Trinanes Pego, Y.; Fregni, F.; Carrillo-de-la-Pena, M.T. Defective Endogenous Pain Modulation in Fibromyalgia: A Meta-Analysis of Temporal Summation and Conditioned Pain Modulation Paradigms. J. Pain 2018, 19, 819–836. [Google Scholar] [CrossRef]
- Gerdle, B.; Wahlen, K.; Ghafouri, B. Plasma protein patterns are strongly correlated with pressure pain thresholds in women with chronic widespread pain and in healthy controls-an exploratory case-control study. Medicine 2020, 99, e20497. [Google Scholar] [CrossRef]
- van den Ameele, J.; Fuge, J.; Pitceathly, R.D.S.; Berry, S.; McIntyre, Z.; Hanna, M.G.; Lee, M.; Chinnery, P.F. Chronic pain is common in mitochondrial disease. Neuromuscul. Disord. 2020, 30, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Cruz, R.S.; de Aguiar, R.A.; Turnes, T.; Penteado Dos Santos, R.; de Oliveira, M.F.; Caputo, F. Intracellular shuttle: The lactate aerobic metabolism. Sci. World J. 2012, 2012, 420984. [Google Scholar] [CrossRef] [Green Version]
- Lanza, I.R.; Nair, K.S. Mitochondrial function as a determinant of life span. Pflugers Arch. 2010, 459, 277–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbieri, E.; Sestili, P. Reactive oxygen species in skeletal muscle signaling. J. Signal Transduct. 2012, 2012, 982794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallenborn-Gerhardt, W.; Schroder, K.; Geisslinger, G.; Schmidtko, A. NOXious signaling in pain processing. Pharmacol. Ther. 2013, 137, 309–317. [Google Scholar] [CrossRef]
- Ponnalagu, D.; Singh, H. Insights Into the Role of Mitochondrial Ion Channels in Inflammatory Response. Front. Physiol. 2020, 11, 258. [Google Scholar] [CrossRef] [PubMed]
- Angajala, A.; Lim, S.; Phillips, J.B.; Kim, J.H.; Yates, C.; You, Z.; Tan, M. Diverse Roles of Mitochondria in Immune Responses: Novel Insights Into Immuno-Metabolism. Front. Immunol. 2018, 9, 1605. [Google Scholar] [CrossRef]
- De Lavera, I.; Pavon, A.D.; Paz, M.V.; Oropesa-Avila, M.; de la Mata, M.; Alcocer-Gomez, E.; Garrido-Maraver, J.; Cotan, D.; Alvarez-Cordoba, M.; Sanchez-Alcazar, J.A. The Connections Among Autophagy, Inflammasome and Mitochondria. Curr. Drug Targets 2017, 18, 1030–1038. [Google Scholar] [CrossRef]
- Cordero, M.D.; Diaz-Parrado, E.; Carrion, A.M.; Alfonsi, S.; Sanchez-Alcazar, J.A.; Bullon, P.; Battino, M.; de Miguel, M. Is inflammation a mitochondrial dysfunction-dependent event in fibromyalgia? Antioxid. Redox Signal. 2013, 18, 800–807. [Google Scholar] [CrossRef] [Green Version]
- Meeus, M.; Nijs, J.; Hermans, L.; Goubert, D.; Calders, P. The role of mitochondrial dysfunctions due to oxidative and nitrosative stress in the chronic pain or chronic fatigue syndromes and fibromyalgia patients: Peripheral and central mechanisms as therapeutic targets? Expert Opin. Ther. Targets 2013, 17, 1081–1089. [Google Scholar] [CrossRef]
- Cordero, M.D.; Alcocer-Gomez, E.; Culic, O.; Carrion, A.M.; de Miguel, M.; Diaz-Parrado, E.; Perez-Villegas, E.M.; Bullon, P.; Battino, M.; Sanchez-Alcazar, J.A. NLRP3 inflammasome is activated in fibromyalgia: The effect of coenzyme Q10. Antioxid. Redox Signal. 2014, 20, 1169–1180. [Google Scholar] [CrossRef] [Green Version]
- Cowie, A.M.; Dittel, B.N.; Stucky, C.L. A Novel Sex-Dependent Target for the Treatment of Postoperative Pain: The NLRP3 Inflammasome. Front. Neurol. 2019, 10, 622. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Li, F.; Li, W.W.; Stary, C.; Clark, J.D.; Xu, S.; Xiong, X. The inflammasome as a target for pain therapy. Br. J. Anaesth. 2016, 117, 693–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andres-Rodriguez, L.; Borras, X.; Feliu-Soler, A.; Perez-Aranda, A.; Angarita-Osorio, N.; Moreno-Peral, P.; Montero-Marin, J.; Garcia-Campayo, J.; Carvalho, A.F.; Maes, M.; et al. Peripheral immune aberrations in fibromyalgia: A systematic review, meta-analysis and meta-regression. Brain Behav. Immun. 2020, 87, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Goncalves Dos Santos, G.; Delay, L.; Yaksh, T.L.; Corr, M. Neuraxial Cytokines in Pain States. Front. Immunol. 2019, 10, 3061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez-Tejero, J.A.; Martinez-Lara, E.; Rus, A.; Camacho, M.V.; Del Moral, M.L.; Siles, E. Insight into the biological pathways underlying fibromyalgia by a proteomic approach. J. Proteom. 2018, 186, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Suppers, A.; van Gool, A.J.; Wessels, H. Integrated Chemometrics and Statistics to Drive Successful Proteomics Biomarker Discovery. Proteomes 2018, 6, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Group | CON | FM | Statistics | ||||
|---|---|---|---|---|---|---|---|
| Variables | n | Mean | SD | n | Mean | SD | p-value |
| Age (years) | 31 | 42.26 | 10.17 | 33 | 40.06 | 11.36 | 0.417 |
| FM duration (years) | − | − | − | 33 | 6.12 | 6.04 | NA |
| Pain intensity global 7days | − | − | − | 31 | 6.55 | 1.71 | NA |
| HADS | 31 | 4.23 | 3.59 | 31 | 13.32 | 6.17 | < 0.001 * |
| PCS | 31 | 11.45 | 8.97 | 31 | 19.94 | 10.34 | 0.001 * |
| ISI | 31 | 4.23 | 4.47 | 31 | 13.58 | 5.96 | < 0.001 * |
| PSQ | 31 | 3.50 | 0.91 | 31 | 5.64 | 1.80 | < 0.001 * |
| PDI | 30 | 8.43 | 4.93 | 31 | 36.45 | 11.25 | < 0.001 * |
| EQ5D-VAS | 30 | 86.67 | 7.54 | 31 | 52.16 | 18.85 | < 0.001 * |
| Group | CON | FM | Statistics | ||||
|---|---|---|---|---|---|---|---|
| Variables | n | Mean | SD | n | Mean | SD | p-value |
| Blood pressure systolic (mm Hg) | 31 | 113.35 | 8.64 | 33 | 120.88 | 12.58 | 0.007 * |
| Blood pressure diastolic (mm Hg) | 31 | 75.58 | 8.23 | 33 | 80.55 | 10.07 | 0.035 * |
| Weight (kg) | 31 | 68.57 | 10.72 | 33 | 81.04 | 18.68 | 0.002 * |
| Height (m) | 31 | 1.70 | 0.06 | 33 | 1.66 | 0.06 | 0.038 * |
| BMI (kg/m2) | 31 | 23.81 | 3.16 | 33 | 29.18 | 6.13 | <0.001 * |
| Number of tender points | 31 | 0.32 | 0.87 | 33 | 16.48 | 2.66 | <0.001 * |
| Mean PPT all sites (kPa) | 31 | 383.66 | 109.91 | 33 | 132.55 | 84.66 | <0.001 * |
| PPT Trapezius catheter side (kPa) | 31 | 303.74 | 103.01 | 33 | 109.54 | 69.01 | <0.001 * |
| PPT Erector Spine catheter side (kPa) | 31 | 432.61 | 147.15 | 33 | 121.79 | 87.91 | <0.001 * |
| MaxVO2 per kg (mL/kg/min) | 30 | 2.64 | 0.49 | 30 | 2.17 | 0.53 | 0.001 * |
| Grip force-max (N) | 30 | 311.59 | 51.58 | 33 | 240.38 | 63.94 | <0.001 * |
| Grip force-average (N) | 30 | 232.77 | 45.26 | 33 | 162.31 | 54.07 | <0.001 * |
| Grip force-endurance (N) | 30 | 233.05 | 127.05 | 33 | 137.80 | 47.75 | <0.001 * |
| TST | 30 | 17.80 | 3.03 | 32 | 13.63 | 3.47 | <0.001 * |
| Groups | Controls | FM | Statistics | ||||
|---|---|---|---|---|---|---|---|
| Variables | n | Mean | SD | n | Mean | SD | p−value |
| NRS pre insertion | 31 | 0.13 | 0.43 | 33 | 4.82 | 2.89 | <0.001 * |
| NRS 140 min | 31 | 0.42 | 0.85 | 33 | 5.55 | 2.21 | <0.001 * |
| NRS 160 min | 31 | 1.74 | 1.84 | 33 | 7.67 | 1.67 | <0.001 * |
| Difference NRS 160 min−140 min | 31 | 1.32 | 1.38 | 33 | 2.12 | 1.75 | 0.047 * |
| Mean NRS 140−220 min | 31 | 0.61 | 0.84 | 33 | 6.07 | 1.85 | <0.001 * |
| Blood flow Trapezius 140 min | 30 | 0.68 | 0.07 | 32 | 0.65 | 0.07 | 0.054 |
| Blood flow Trapezius 160 min | 30 | 0.70 | 0.10 | 32 | 0.67 | 0.11 | 0.249 |
| Difference Blood flow Trapezius 160 min−140 min | 30 | 0.02 | 0.05 | 32 | 0.03 | 0.09 | 0.825 |
| Mean Blood flow Trapezius 140−220 min | 30 | 0.69 | 0.07 | 32 | 0.66 | 0.07 | 0.107 |
| Blood flow Erector spinae 140 min | 26 | 0.54 | 0.19 | 31 | 0.36 | 0.19 | 0.001 * |
| Blood flow Erector spinae 160 min | 26 | 0.59 | 0.17 | 31 | 0.39 | 0.19 | <0.001* |
| Difference Blood flow Erector spinae 160 min−140 min | 25 | 0.03 | 0.08 | 31 | 0.03 | 0.08 | 0.886 |
| Mean Blood flow Erector spinae 140−220 min | 27 | 0.55 | 0.18 | 31 | 0.37 | 0.18 | <0.001 * |
| Glucose Trapezius 140 min (mmol L−1) | 29 | 10.00 | 6.92 | 32 | 8.41 | 5.24 | 0.312 |
| Glucose Trapezius 160 min (mmol L−1) | 30 | 13.25 | 19.05 | 32 | 7.89 | 5.44 | 0.132 |
| Difference Glucose Trapezius 160 min–140 min (mmolLl−1) | 29 | 3.11 | 19.08 | 32 | −0.52 | 4.94 | 0.303 |
| Mean Glucose Trapezius 140−220 min (mmol L−1) | 30 | 9.65 | 5.94 | 32 | 8.27 | 4.39 | 0.300 |
| Glucose Erector spinae 140 min (mmol L−1) | 24 | 8.35 | 6.32 | 31 | 9.12 | 6.33 | 0.657 |
| Glucose Erector spinae 160 min (mmol L−1) | 24 | 12.89 | 21.88 | 31 | 12.57 | 26.87 | 0.962 |
| Difference Glucose Erector spinae 160 min−140 min (mmol L−1) | 23 | 4.91 | 22.89 | 31 | 3.45 | 28.59 | 0.841 |
| Mean Glucose Erector spinae 140−220 min (mmol Lv1) | 25 | 9.48 | 6.34 | 31 | 10.55 | 8.81 | 0.613 |
| Lactate Trapezius 140 min (mmol L−1) | 28 | 2.55 | 1.62 | 32 | 2.71 | 1.67 | 0.709 |
| Lactate Trapezius 160 min (mmol L−1) | 28 | 4.61 | 7.29 | 32 | 2.88 | 2.05 | 0.234 |
| Difference Lactate Trapezius 160 min − 140 min (mmol L−1) | 27 | 2.19 | 6.80 | 32 | 0.17 | 1.90 | 0.145 |
| Mean Lactate Trapezius 140−220 min (mmol L−1) | 30 | 3.51 | 2.33 | 32 | 3.22 | 1.48 | 0.552 |
| Lactate Erector spinae 140 min (mmol L−1) | 23 | 1.86 | 1.04 | 29 | 2.68 | 3.80 | 0.275 |
| Lactate Erector spinae 160 min (mmol L−1) | 23 | 2.91 | 4.32 | 29 | 2.74 | 2.66 | 0.862 |
| Difference Lactate Erector spinae 160 min−140 min (mmol L−1) | 23 | 1.04 | 4.21 | 28 | 0.08 | 3.36 | 0.369 |
| Mean Lactate Erector spinae 140–220 min (mmol L−1) | 23 | 2.23 | 1.36 | 30 | 3.65 | 5.58 | 0.237 |
| Pyruvate Trapezius 140 min (μmol L−1) | 30 | 12.97 | 10.98 | 32 | 27.96 | 18.19 | < 0.001 * |
| Pyruvate Trapezius 160 min (μmol L−1) | 30 | 25.54 | 34.47 | 32 | 33.84 | 31.16 | 0.323 |
| Difference Pyruvate Trapezius 160 min−140 min (μmol L−1) | 30 | 12.57 | 31.74 | 32 | 5.88 | 24.81 | 0.357 |
| Mean Pyruvate Trapezius 140−220 min (μmol L−1) | 30 | 20.10 | 17.87 | 32 | 38.64 | 29.75 | 0.005 * |
| Pyruvate Erector spinae 140 min (μmol L−1) | 25 | 12.37 | 10.97 | 31 | 26.59 | 30.74 | 0.032 * |
| Pyruvate Erector spinae 160 min (μmol L−1) | 25 | 27.22 | 45.69 | 31 | 80.37 | 270.52 | 0.337 |
| Difference Pyruvate Erector spinae 160 min−140 min (μmol L−1) | 24 | 14.66 | 46.09 | 31 | 53.79 | 275.61 | 0.495 |
| Mean Pyruvate Erector spinae 140−220 min (μmol L−1) | 26 | 18.57 | 15.97 | 31 | 44.15 | 71.35 | 0.079 |
| Glycerol Trapezius 140 min (mmol L−1) | 30 | 90.37 | 60.04 | 32 | 95.26 | 52.10 | 0.733 |
| Glycerol Trapezius 160 min (mmol L−1) | 29 | 108.94 | 82.71 | 32 | 105.91 | 85.78 | 0.889 |
| Difference Glycerol Trapezius 160 min−140 min (mmol L−1) | 29 | 19.35 | 92.43 | 32 | 10.65 | 72.58 | 0.683 |
| Mean Glycerol Trapezius 140−220 min (mmol L−1) | 30 | 90.06 | 41.68 | 32 | 103.28 | 57.53 | 0.307 |
| Glycerol Erector spinae 140 min (mmol L−1) | 25 | 138.79 | 96.15 | 31 | 149.73 | 119.08 | 0.712 |
| Glycerol Erector spinae 160 min (mmol L−1) | 25 | 141.55 | 177.53 | 29 | 136.95 | 101.51 | 0.906 |
| Difference Glycerol Erector spinae 160 min − 140 min (mmol L−1) | 24 | 7.17 | 198.28 | 29 | −10.62 | 97.96 | 0.673 |
| Mean Glycerol Erector spinae 140−220 min (mmol L−1) | 26 | 126.60 | 65.65 | 31 | 150.91 | 90.05 | 0.258 |
| Glutamate Trapezius 140 min (mmol L−1) | 30 | 49.77 | 31.65 | 32 | 56.06 | 32.50 | 0.444 |
| Glutamate Trapezius 160 min (mmol L−1) | 29 | 81.88 | 56.69 | 32 | 79.47 | 55.15 | 0.867 |
| Difference Glutamate Trapezius 160 min−140 min (mmol L−1) | 29 | 32.56 | 57.77 | 32 | 23.42 | 40.17 | 0.473 |
| Mean Glutamate Trapezius 140−220 min (mmol L−1) | 30 | 63.24 | 30.87 | 32 | 67.55 | 34.33 | 0.606 |
| Glutamate Erector spinae 140 min (mmol L−1) | 25 | 41.40 | 26.52 | 31 | 30.20 | 43.02 | 0.260 |
| Glutamate Erector spinae 160 min (mmol L−1) | 25 | 48.96 | 78.95 | 31 | 41.44 | 88.96 | 0.742 |
| Difference Glutamate Erector spinae 160 min − 140 min (mmol L−1) | 24 | 6.21 | 79.89 | 31 | 11.24 | 88.62 | 0.828 |
| Mean Glutamate Erector spinae 140 − 220 min (mmol L−1) | 26 | 41.79 | 26.23 | 31 | 33.82 | 39.23 | 0.381 |
| Group | CON | FM | Statistics | ||||
|---|---|---|---|---|---|---|---|
| Variables | n | Mean | SD | n | Mean | SD | p-value |
| PCr (mM) | 30 | 40.06 | 8.54 | 32 | 34.07 | 11.49 | 0.024 * |
| Pi (mM) | 30 | 5.68 | 1.84 | 32 | 5.29 | 1.76 | 0.409 |
| ATP (mM) | 30 | 8.64 | 1.49 | 32 | 7.57 | 1.91 | 0.017 * |
| pH | 30 | 7.03 | 0.03 | 32 | 7.03 | 0.03 | 0.514 |
| Ratio ATP/Ptot | 30 | 0.30 | 0.02 | 32 | 0.30 | 0.02 | 0.897 |
| Ratio PCr/Ptot | 30 | 1.37 | 0.06 | 32 | 1.30 | 0.13 | 0.018 * |
| Ratio Pi/Ptot | 30 | 0.19 | 0.03 | 32 | 0.20 | 0.03 | 0.098 |
| Ratio ATP/PCr | 30 | 0.22 | 0.02 | 32 | 0.23 | 0.04 | 0.101 |
| Ratio Pi/PCr | 30 | 0.14 | 0.03 | 32 | 0.16 | 0.04 | 0.017 * |
| Variables | VIP | p(corr) |
|---|---|---|
| Blood flow Erector spinae 140 min | 2.37 | −0.83 |
| Mean Blood flow Erector spinae 140−220 min | 2.27 | −0.81 |
| Blood flow Erector spinae 160 min | 2.23 | −0.80 |
| PCR (mM) | 1.97 | −0.70 |
| PCr/Ptot | 1.94 | −0.69 |
| ATP (mainly ATP; mM) | 1.94 | −0.69 |
| Pi/PCr | 1.82 | 0.65 |
| Pyruvate trapezius 140 min | 1.60 | 0.57 |
| Mean Blood flow Trapezius 140–220 min | 1.57 | −0.55 |
| ATP/PCr | 1.49 | 0.53 |
| Blood flow Trapezius 160 min | 1.42 | −0.50 |
| R2 | 0.26 | |
| Q2 | 0.18 | |
| CV-ANOVA p-value | 0.003 | |
| n | 61 |
| Variables | VIP | p(corr) |
|---|---|---|
| Pi/PCr | 1.71 | 0.65 |
| Mean Blood flow Trapezius 140–220 min | 1.70 | −0.64 |
| Glutamate Trapezius 160 min | 1.53 | −0.57 |
| Blood flow Trapezius 140 min | 1.52 | −0.57 |
| Blood flow Erector spinae 140 min | 1.51 | −0.57 |
| Pi/Ptot | 1.51 | 0.57 |
| PCr/Ptot | 1.51 | −0.57 |
| Difference Pyruvate Erector spinae 160 min–140 min | 1.48 | 0.56 |
| Pyruvate Erector spinae 160 min | 1.48 | 0.56 |
| Blood flow Trapezius 160 min | 1.48 | −0.55 |
| Difference Glutamate Erector spinae 160 min–140 min | 1.46 | 0.55 |
| Mean Pyruvate Erector spinae 140–220 min | 1.46 | 0.55 |
| Difference Glucose Erector spinae 160 min–140 min | 1.39 | 0.52 |
| PCr | 1.38 | −0.53 |
| Mean Blood flow Erector spinae 140–220 min | 1.37 | −0.51 |
| Blood flow Erector spinae 160 min | 1.35 | −0.51 |
| R2 | 0.52 | |
| Q2 | 0.32 | |
| CV-ANOVA p-value | 0.006 | |
| n | 30 |
| Variables | VIP | p(corr) |
|---|---|---|
| Difference Glutamate Trapezius 160 min–140 min | 1.84 | 0.78 |
| Difference Lactate Trapezius 160 min–140 min | 1.71 | 0.72 |
| Glutamate Trapezius 160 min | 1.51 | 0.64 |
| Blood flow Trapezius 140 min | 1.41 | 0.60 |
| Difference Glycerol Trapezius 160 min–140 min | 1.39 | 0.59 |
| Mean Blood flow Trapezius 140–220 min | 1.36 | 0.57 |
| Difference Pyruvate Trapezius 160 min–140 min | 1.20 | 0.51 |
| R2 | 0.32 | |
| Q2 | 0.19 | |
| CV-ANOVA P-value | 0.050 | |
| n | 30 |
| Variables | VIP | p(corr) |
|---|---|---|
| Pi/PCr | 1.73 | −0.69 |
| Pi/Ptot | 1.58 | −0.63 |
| Mean Glycerol Erector spinae 140–220 min | 1.52 | −0.60 |
| Glycerol Erector spinae 140 min | 1.51 | −0.60 |
| Pyruvate Erector spinae 140 min | 1.46 | −0.58 |
| Difference Blood flow Erector spinae 160 min–140 min | 1.44 | −0.57 |
| Blood flow Erector spinae 140 min | 1.41 | 0.56 |
| Lactate Erector spinae 140 min | 1.38 | −0.54 |
| PCr/Ptot | 1.36 | 0.54 |
| R2 | 0.32 | |
| Q2 | 0.24 | |
| CV-ANOVA P-value | 0.020 | |
| n | 31 |
| All | CON | FM | ||||||
|---|---|---|---|---|---|---|---|---|
| Variables | VIP | p(corr) | Variables | VIP | p(corr) | Variables | VIP | p(corr) |
| ATP | 1.63 | 0.71 | Pi/PCr | 1.53 | −0.68 | Pi/PCr | 1.87 | −0.86 |
| Pi/PCr | 1.62 | −0.71 | ATP | 1.42 | 0.64 | Pi/Ptot | 1.69 | −0.78 |
| Pi/Ptot | 1.45 | −0.64 | Glycerol Erector spinae 140 min | 1.39 | −0.63 | PCr/Ptot | 1.68 | 0.78 |
| PCR | 1.43 | 0.62 | Pi/Ptot | 1.37 | −0.61 | PCR | 1.17 | 0.54 |
| PCr/Ptot | 1.42 | 0.62 | PCr/Ptot | 1.20 | 0.54 | ATP | 1.14 | 0.52 |
| R2 | 0.50 | R2 | 0.56 | R2 | 0.37 | |||
| Q2 | 0.45 | Q2 | 0.47 | Q2 | 0.25 | |||
| CV-ANOVA p-value | < 0.001 | CV-ANOVA P-value | <0.001 | CV-ANOVA P-value | 0.022 | |||
| n | 55 | n | 25 | n | 30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerdle, B.; Ghafouri, B.; Lund, E.; Bengtsson, A.; Lundberg, P.; Ettinger-Veenstra, H.v.; Leinhard, O.D.; Forsgren, M.F. Evidence of Mitochondrial Dysfunction in Fibromyalgia: Deviating Muscle Energy Metabolism Detected Using Microdialysis and Magnetic Resonance. J. Clin. Med. 2020, 9, 3527. https://doi.org/10.3390/jcm9113527
Gerdle B, Ghafouri B, Lund E, Bengtsson A, Lundberg P, Ettinger-Veenstra Hv, Leinhard OD, Forsgren MF. Evidence of Mitochondrial Dysfunction in Fibromyalgia: Deviating Muscle Energy Metabolism Detected Using Microdialysis and Magnetic Resonance. Journal of Clinical Medicine. 2020; 9(11):3527. https://doi.org/10.3390/jcm9113527
Chicago/Turabian StyleGerdle, Björn, Bijar Ghafouri, Eva Lund, Ann Bengtsson, Peter Lundberg, Helene van Ettinger-Veenstra, Olof Dahlqvist Leinhard, and Mikael Fredrik Forsgren. 2020. "Evidence of Mitochondrial Dysfunction in Fibromyalgia: Deviating Muscle Energy Metabolism Detected Using Microdialysis and Magnetic Resonance" Journal of Clinical Medicine 9, no. 11: 3527. https://doi.org/10.3390/jcm9113527