Decline in Carbon Monoxide Transfer Coefficient in Chronic Obstructive Pulmonary Disease

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
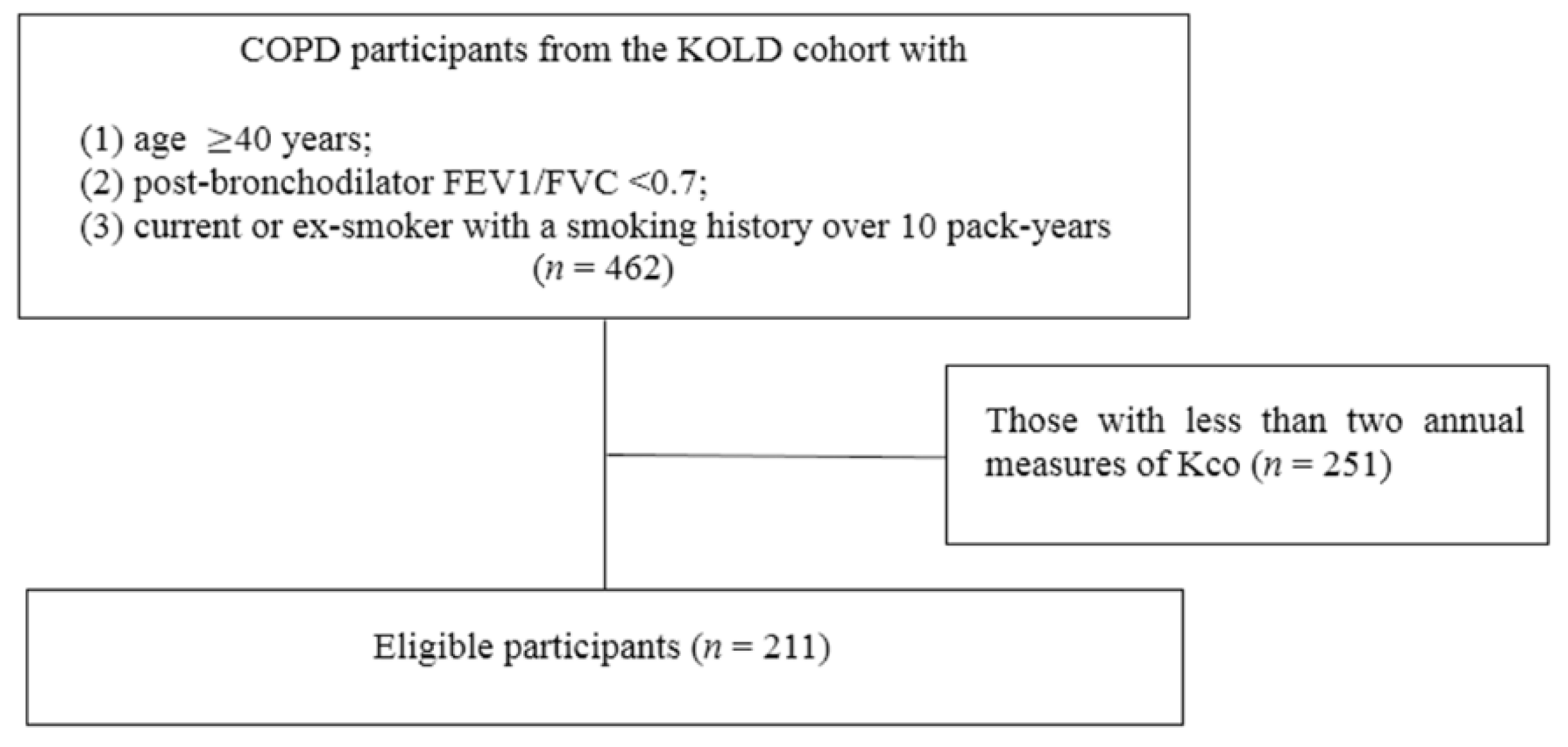
2.1. Study Design and Participants
2.2. Lung Function Measurements
2.3. Chest CT Measures
2.4. Statistical Analysis
3. Results
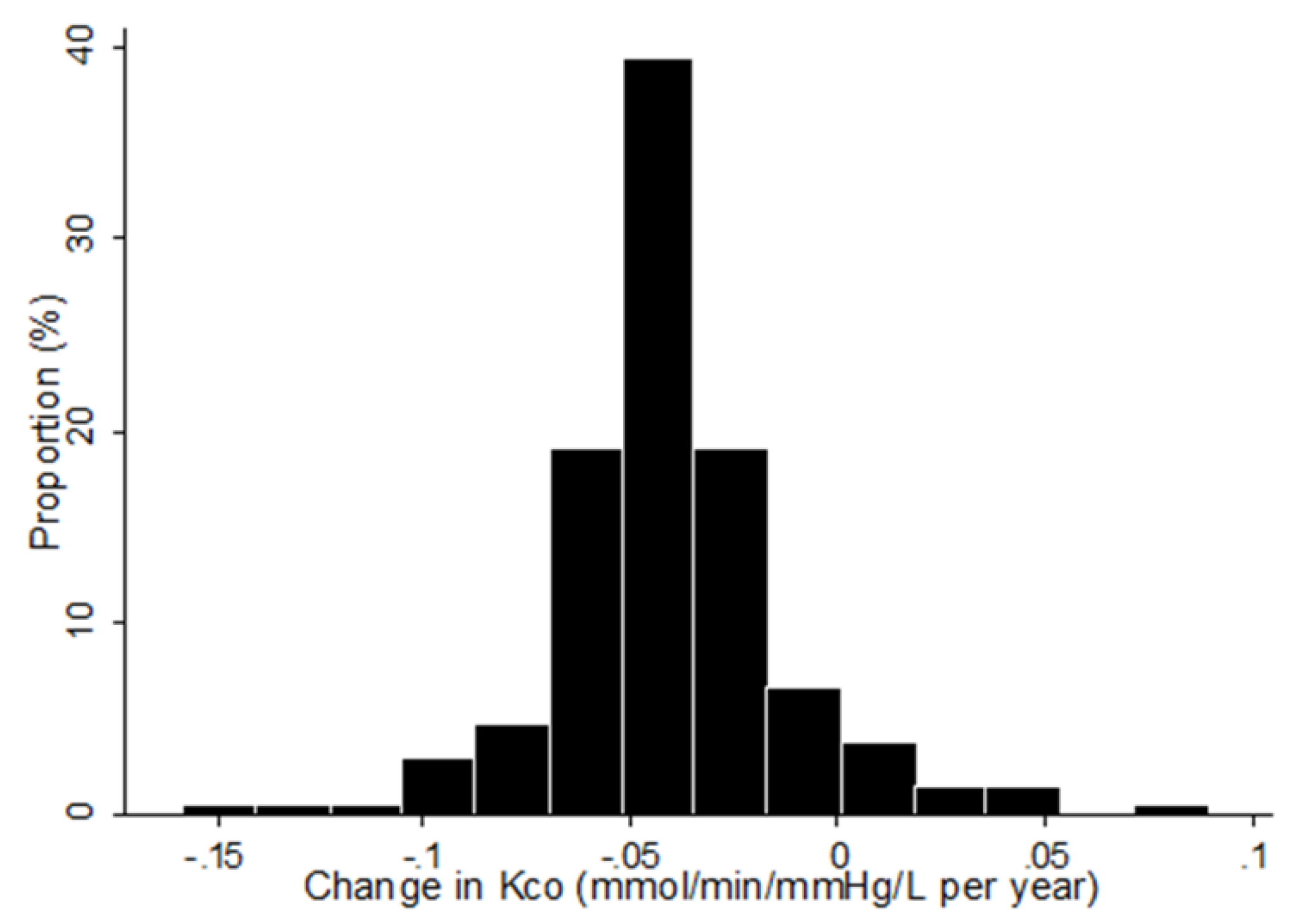
3.1. Patient Characteristics and the Rate of Change in Kco
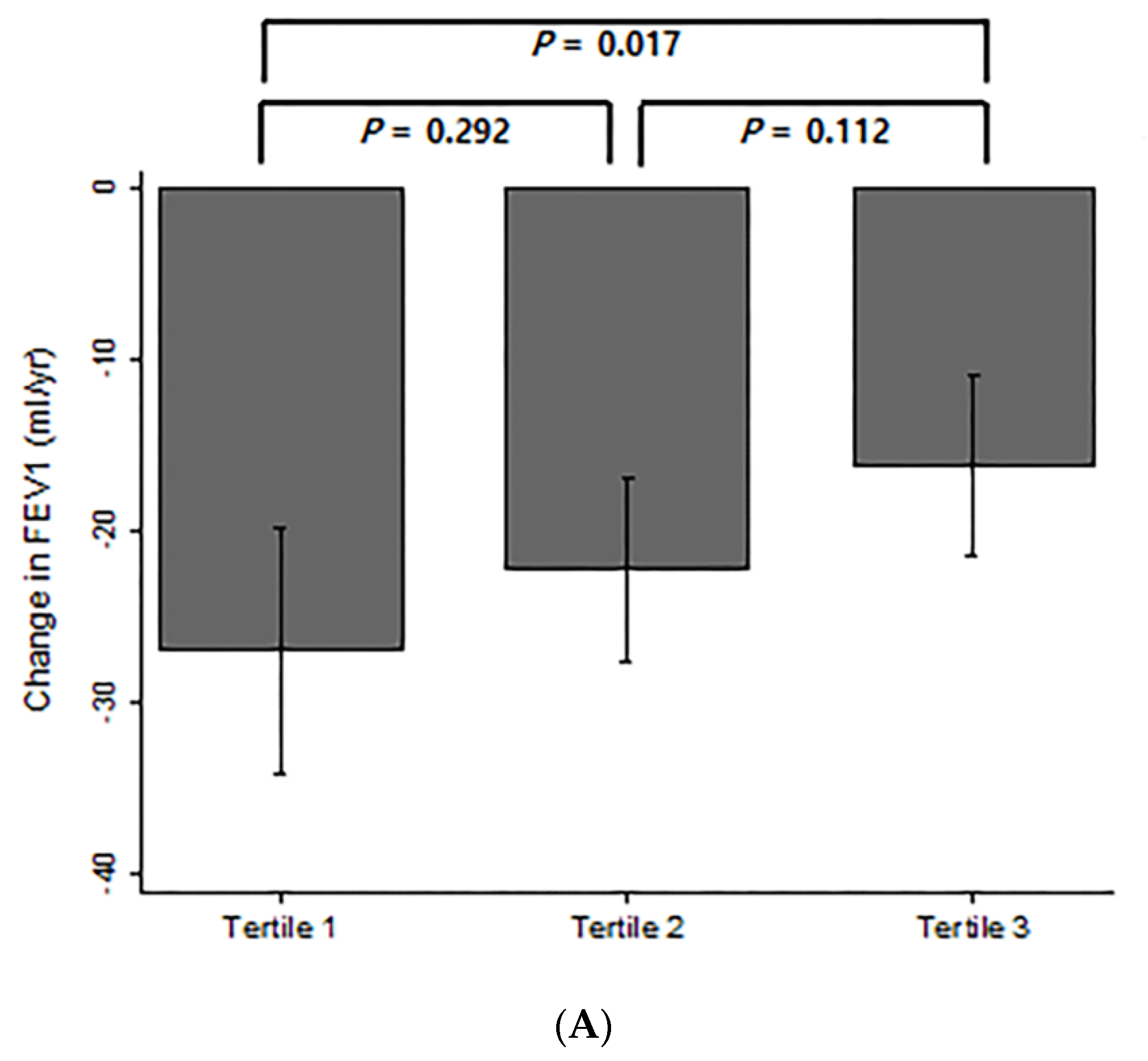
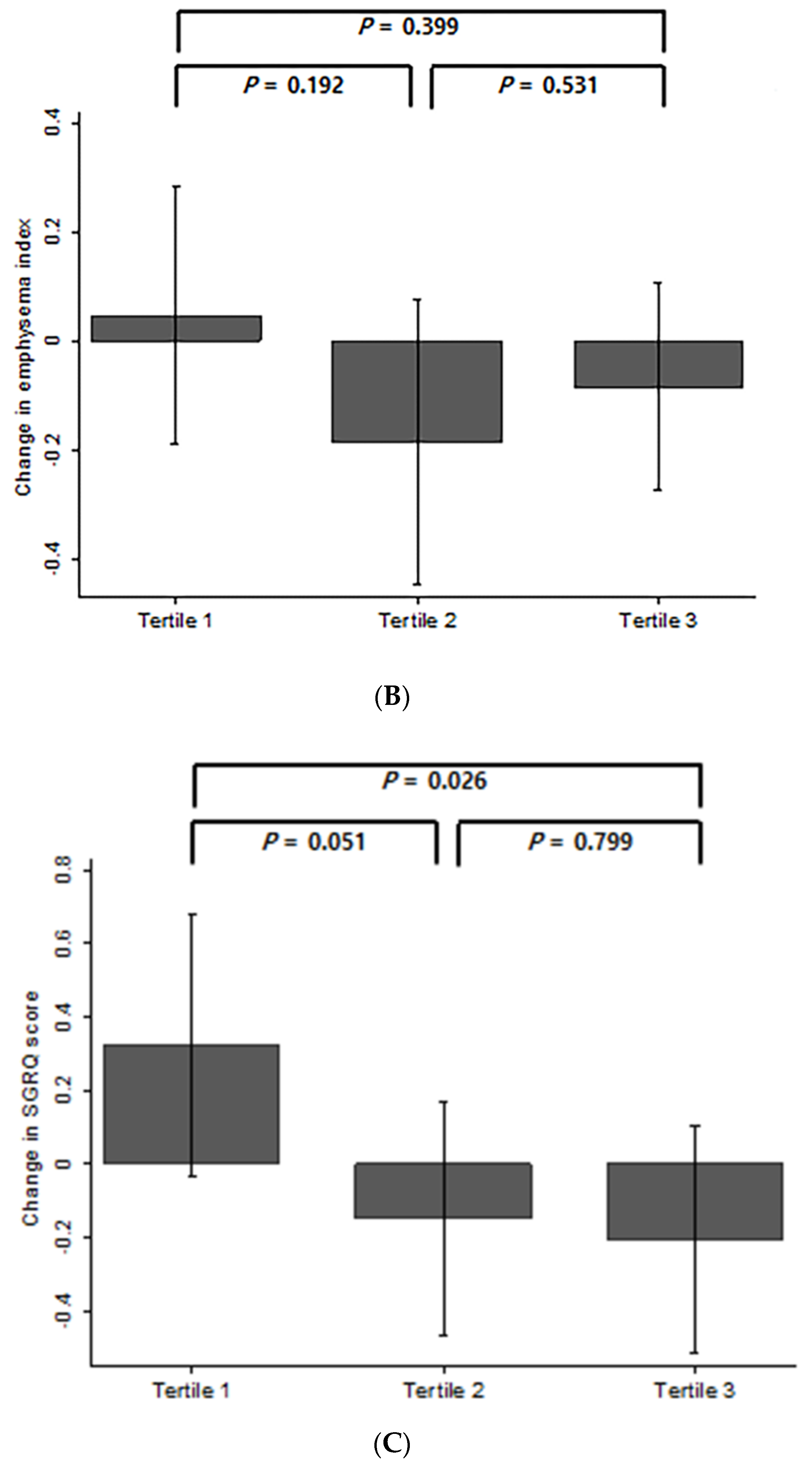
3.2. Comparison of Changes in FEV1, Emphysema Index, and SGRQ Score According to Changes in Kco Over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease (2020 Report). Available online: https://goldcopd.org/gold-reports (accessed on 5 March 2020).
- Murray, C.J.; Atkinson, C.; Bhalla, K.; Birbeck, G.; Burstein, R.; Chou, D.; Dellavalle, R.; Danaei, G.; Ezzati, M.; Fahimi, A.; et al. The state of US health, 1990-2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 310, 591–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Eisner, M.D.; Anthonisen, N.; Coultas, D.; Kuenzli, N.; Perez-Padilla, R.; Postma, D.; Romieu, I.; Silverman, E.K.; Balmes, J.R. Committee on Nonsmoking COPD. An official American Thoracic Society public policy statement: Novel risk factors and the global burden of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2010, 182, 693–718. [Google Scholar] [CrossRef] [PubMed]
- Vestbo, J.; Edwards, L.D.; Scanlon, P.D.; Yates, J.C.; Agusti, A.; Bakke, P.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Crim, C.; et al. Changes in forced expiratory volume in 1 second overtime in COPD. N. Engl. J. Med. 2011, 365, 1184–1192. [Google Scholar] [CrossRef] [Green Version]
- Celli, B.R.; Thomas, N.E.; Anderson, J.A.; Ferguson, G.T.; Jenkins, C.R.; Jones, P.W.; Vestbo, J.; Knobil, K.; Yates, J.C.; Calverley, P.M. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: Results from the TORCH study. Am. J. Respir. Crit. Care Med. 2008, 178, 332–338. [Google Scholar] [CrossRef]
- Nishimura, M.; Makita, H.; Nagai, K.; Konno, S.; Nasuhara, Y.; Hasegawa, M.; Shimizu, K.; Betsuyaku, T.; Ito, Y.M.; Fuke, S.; et al. Hokkaido COPD Cohort Study Investigators. Annual change in pulmonary function and clinical phenotype in chronic obstructive pulmonary disease. Am. J. Respir Crit. Care Med. 2012, 185, 44–52. [Google Scholar] [CrossRef]
- Makita, H.; Nasuhara, Y.; Nagai, K.; Ito, Y.; Hasegawa, M.; Betsuyaku, T.; Onodera, Y.; Hizawa, N.; Nishimura, M. Hokkaido COPD Cohort Study Group. Characterisation of phenotypes based on severity of emphysema in chronic obstructive pulmonary disease. Thorax 2007, 62, 932–937. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.W. Health status and the spiral of decline. COPD 2009, 6, 59–63. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Revill, S.M.; Webb, K.A. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 164, 770–777. [Google Scholar] [CrossRef]
- Hughes, J.M.; Pride, N.B. Examination of the carbon monoxide diffusing capacity (DL(CO)) in relation to its KCO and VA components. Am. J. Respir. Crit. Care Med. 2012, 186, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: The GOLD Science Committee Report 2019. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef] [PubMed]
- Hueper, K.; Vogel-Claussen, J.; Parikh, M.A.; Austin, J.H.; Bluemke, D.A.; Carr, J.; Choi, J.; Goldstein, T.A.; Gomes, A.S.; Hoffman, E.A.; et al. Pulmonary microvascular blood flow in mild chronic obstructive pulmonary disease and emphysema. The MESA COPD Study. Am. J. Respir. Crit. Care Med. 2015, 192, 570–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watz, H.; Waschki, B.; Meyer, T.; Kretschmar, G.; Kirsten, A.; Claussen, M.; Magnussen, H. Decreasing cardiac chamber sizes and associated heart dysfunction in COPD: Role of hyperinflation. Chest 2010, 138, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Arbex, F.F.; Alencar, M.C.; Souza, A.; Mazzuco, A.; Sperandio, P.A.; Rocha, A.; Hirai, D.M.; Mancuso, F.; Berton, D.C.; Borghi-Silva, A.; et al. Exercise ventilation in COPD: Influence of systolic heart failure. COPD 2016, 13, 693–699. [Google Scholar] [CrossRef]
- Park, T.S.; Lee, J.S.; Seo, J.B.; Hong, Y.; Yoo, J.W.; Kang, B.J.; Lee, S.W.; Oh, Y.M.; Lee, S.D. KOLD Study Group. Study design and outcomes of Korean obstructive lung disease (KOLD) cohort study. Tuberc. Respir. Dis. (Seoul) 2014, 76, 169–174. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. ATS/ERS Task Force. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease (2017 Report). Available online: http://goldcopd.org (accessed on 5 March 2020).
- American Thoracic Society. Single-breath carbon monoxide diffusing capacity (transfer factor). Recommendations for a standard technique—1995 update. Am. J. Respir. Crit. Care Med. 1995, 152, 2185–2198. [Google Scholar] [CrossRef]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [Green Version]
- Laird, N.M.; Ware, J.H. Random-effects models for longitudinal data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef]
- Han, M.K.; Agusti, A.; Calverley, P.M.; Celli, B.R.; Criner, G.; Curtis, J.L.; Fabbri, L.M.; Goldin, J.G.; Jones, P.W.; Macnee, W.; et al. Chronic obstructive pulmonary disease phenotypes: The future of COPD. Am. J. Respir. Crit. Care Med. 2010, 182, 598–604. [Google Scholar] [CrossRef] [Green Version]
- Casanova, C.; de Torres, J.P.; Aguirre-Jaime, A.; Pinto-Plata, V.; Marin, J.M.; Cordoba, E.; Baz, R.; Cote, C.; Celli, B.R. The progression of chronic obstructive pulmonary disease is heterogeneous: The experience of the BODE cohort. Am. J. Respir. Crit. Care Med. 2011, 184, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; MacNee, W.; Martinez, F.J.; Rabe, K.F.; Franciosi, L.G.; Barnes, P.J.; Brusasco, V.; Burge, P.S.; Calverley, P.M.; Celli, B.R.; et al. American Thoracic Society; European Respiratory Society Task Force on outcomes of COPD. Outcomes for COPD pharmacological trials: From lung function to biomarkers. Eur. Respir. J. 2008, 31, 416–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Mullerova, H.; Tal-Singer, R.; Miller, B.; Lomas, D.A.; Agusti, A.; Macnee, W.; et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N. Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, M.; Makita, H.; Ito, Y.M.; Nagai, K.; Konno, S.; Nishimura, M. Hokkaido COPD Cohort Study Investigators. Clinical features and determinants of COPD exacerbation in the Hokkaido COPD cohort study. Eur. Respir. J. 2014, 43, 1289–1297. [Google Scholar] [CrossRef] [Green Version]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [Green Version]
- Puhan, M.A.; Garcia-Aymerich, J.; Frey, M.; ter Riet, G.; Anto, J.M.; Agusti, A.G.; Gomez, F.P.; Rodriguez-Roisin, R.; Moons, K.G.; Kessels, A.G.; et al. Expansion of the prognostic assessment of patients with chronic obstructive pulmonary disease: The updated BODE index and the ADO index. Lancet 2009, 374, 704–711. [Google Scholar] [CrossRef]
- Tantucci, C.; Modina, D. Lung function decline in COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2012, 7, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Coxson, H.O.; Dirksen, A.; Edwards, L.D.; Yates, J.C.; Agusti, A.; Bakke, P.; Calverley, P.M.; Celli, B.; Crim, C.; Duvoix, A.; et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. The presence and progression of emphysema in COPD as determined by CT scanning and biomarker expression: A prospective analysis from the ECLIPSE study. Lancet Respir. Med. 2013, 1, 129–136. [Google Scholar] [CrossRef]
- Park, J.; Lee, C.H.; Lee, Y.J.; Park, J.S.; Cho, Y.J.; Lee, J.H.; Lee, C.T.; Yoon, H.I. Longitudinal changes in lung hyperinflation in COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.W.; Lee, C.H.; Hwang, H.G.; Kim, Y.I.; Kim, D.K.; Oh, Y.M.; Lee, S.H.; Kim, K.U.; Lee, S.D. Resting hyperinflation and emphysema on the clinical course of COPD. Sci. Rep. 2019, 9, 3764. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, J.D.; McKenzie, A.S.; Zach, J.A.; Wilson, C.G.; Curran-Everett, D.; Stinson, D.S.; Newell, J.D., Jr.; Lynch, D.A. Relationships between airflow obstruction and quantitative CT measurements of emphysema, air trapping, and airways in subjects with and without chronic obstructive pulmonary disease. AJR Am. J. Roentgenol. 2013, 201, 460–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, X.; de Jong, P.A.; Oudkerk, M.; Wang, Y.; Ten Hacken, N.H.; Miao, J.; Zhang, G.; de Bock, G.H.; Vliegenthart, R. Morphological measurements in computed tomography correlate with airflow obstruction in chronic obstructive pulmonary disease: Systematic review and meta-analysis. Eur. Radiol. 2012, 22, 2085–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, K.; Konno, S.; Makita, H.; Kimura, H.; Kimura, H.; Suzuki, M.; Nishimura, M. Transfer coefficients better reflect emphysematous changes than carbon monoxide diffusing capacity in obstructive lung diseases. J. Appl. Physiol. 2018, 125, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Gould, G.A.; Redpath, A.T.; Ryan, M.; Warren, P.M.; Best, J.J.; Flenley, D.C.; MacNee, W. Lung CT density correlates with measurements of airflow limitation and the diffusing capacity. Eur. Respir. J 1991, 4, 141–146. [Google Scholar] [PubMed]
- Nambu, A.; Zach, J.; Schroeder, J.; Jin, G.Y.; Kim, S.S.; Kim, Y.I.; Schnell, C.; Bowler, R.; Lynch, D.A. Relationships between diffusing capacity for carbon monoxide (DLCO), and quantitative computed tomography measurements and visual assessment for chronic obstructive pulmonary disease. Eur. J. Radiol. 2015, 84, 980–985. [Google Scholar] [CrossRef] [PubMed]
- Dowson, L.J.; Guest, P.J.; Stockley, R.A. Longitudinal changes in physiological, radiological, and health status measurements in alpha (1)-antitrypsin deficiency and factors associated with decline. Am. J. Respir. Crit. Care Med. 2001, 164, 1805–1809. [Google Scholar] [CrossRef]
- Barjaktarevic, I.; Springmeyer, S.; Gonzalez, X.; Sirokman, W.; Coxson, H.O.; Cooper, C.B. Diffusing capacity for carbon monoxide correlates best with tissue volume from quantitative CT scanning analysis. Chest 2015, 147, 1485–1493. [Google Scholar] [CrossRef]
- Roman, M.A.; Rossiter, H.B.; Casaburi, R. Exercise, ageing and the lung. Eur. Respir. J. 2016, 48, 1471–1486. [Google Scholar] [CrossRef] [Green Version]
- Yamato, H.; Sun, J.P.; Churg, A.; Wright, J.L. Cigarette smoke-induced emphysema in guinea pigs is associated with diffusely decreased capillary density and capillary narrowing. Lab. Investig. 1996, 75, 211–219. [Google Scholar]
- Mishima, M.; Hirai, T.; Itoh, H.; Nakano, Y.; Sakai, H.; Muro, S.; Nishimura, K.; Oku, Y.; Chin, K.; Ohi, M.; et al. Complexity of terminal airspace geometry assessed by lung computed tomography in normal subjects and patients with chronic obstructive pulmonary disease. Proc. Natl. Acad. Sci. USA 1999, 96, 8829–8834. [Google Scholar] [CrossRef] [Green Version]
- Prescott, E.; Bjerg, A.M.; Andersen, P.K.; Lange, P.; Vestbo, J. Gender difference in smoking effects on lung function and risk of hospitalization for COPD: Results from a Danish longitudinal population study. Eur. Respir. J. 1997, 10, 822–827. [Google Scholar] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Washko, G.R.; Hunninghake, G.M.; Fernandez, I.E.; Nishino, M.; Okajima, Y.; Yamashiro, T.; Ross, J.C.; Estépar, R.S.; Lynch, D.A.; Brehm, J.M.; et al. Lung volumes and emphysema in smokers with interstitial lung abnormalities. N. Engl. J. Med. 2011, 364, 897–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calverley, P.M.; Albert, P.; Walker, P.P. Bronchodilator Reversibility in Chronic Obstructive Pulmonary Disease: Use and Limitations. Lancet Respir. Med. 2013, 1, 564–573. [Google Scholar] [CrossRef]
- Jo, Y.S.; Lee, J.; Yoon, H.I.; Kim, D.K.; Yoo, C.G.; Lee, C.H. Different prevalence and clinical characteristics of asthma-chronic obstructive pulmonary disease overlap syndrome according to accepted criteria. Ann. Allergy Asthma Immunol. 2017, 118, 696–703. [Google Scholar] [CrossRef]
- Sin, D.D.; Miravitlles, M.; Mannino, D.M.; Soriano, J.B.; Price, D.; Celli, B.R.; Leung, J.M.; Nakano, Y.; Park, H.Y.; Wark, P.A.; et al. What is asthma-COPD overlap syndrome? Towards a consensus definition from a round table discussion. Eur. Respir. J. 2016, 48, 664–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, X.; Cho, M.H.; Anderson, W.; Coxson, H.O.; Muller, N.; Washko, G.; Hoffman, E.A.; Bakke, P.; Gulsvik, A.; Lomas, D.A.; et al. Genome-wide association study identifies BICD1 as a susceptibility gene for emphysema. Am. J. Respir. Crit. Care Med. 2011, 183, 43–49. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Tertile 1 (Group with the Most Rapid Decline, n = 71) | Tertile 2 (n = 70) | Tertile 3 (Group with the Slowest Decline, n = 70) | p-Value * |
|---|---|---|---|---|
| Annual change in Kco (mmol/min/mmHg/L per year) | −0.07 ± 0.02 | −0.04 ± 0.00 | −0.01 ± 0.02 | <0.001 |
| Age | 66.8 ± 6.8 | 68.1± 6.6 | 64.7 ± 7.4 | 0.014 |
| Men, n (%) | 70 (98.6) | 68 (97.1) | 65 (92.9) | 0.180 |
| BMI, kg/m2 | 22.8 ± 2.9 | 22.2 ± 3.2 | 23.5 ± 3.3 | 0.079 |
| Smoking status at baseline, n (%) | 0.165 | |||
| Current smokers | 25 (35.2) | 17 (24.3) | 28 (40.0) | 0.129 |
| Former smokers | 46 (64.8) | 53 (75.7) | 42 (60.0) | |
| Pack-years of smoking | 51.4 ± 30.7 | 48.2 ± 28.6 | 48.6± 26.9 | 0.775 |
| Total SGRQ score | 37.7 ± 17.3 | 34.5 ± 17.0 | 34.1 ± 17.6 | 0.411 |
| mMRC grade | 1.9 ± 1.0 | 1.6 ± 1.1 | 1.6 ± 0.8 | 0.154 |
| Exacerbation in previous year baseline, n (%) | 13 (18.3) | 19 (27.1) | 13 (18.6) | 0.348 |
| Eosinophil count, cells/µL | 312.8 ± 380.4 | 275.1 ± 192.4 | 313.6 ± 507.2 | 0.798 |
| Hemoglobin, g/dL | 14.9 ± 1.7 | 14.9 ± 1.1 | 14.9 ± 1.0 | 0.917 |
| Baseline pulmonary function | ||||
| FEV1, L | 1.5 ± 0.5 | 1.6 ± 0.5 | 1.6 ± 0.6 | 0.553 |
| FEV1, % predicted | 57.6 ± 18.2 | 57.9 ± 16.2 | 60.5 ± 19.5 | 0.588 |
| FVC, L | 3.5 ± 0.6 | 3.4 ± 0.8 | 3.3 ± 0.8 | 0.341 |
| FEV1/FVC, % | 43.8 ± 9.7 | 46.4 ± 10.5 | 49.2 ± 10.4 | 0.008 |
| Bronchodilator reversibility, n (%) | 9 (12.7) | 7 (10.0) | 10 (14.3) | 0.738 |
| Kco, mmol/min/mmHg/L | 2.8 ± 0.9 | 2.9 ± 0.9 | 3.0 ± 1.0 | 0.539 |
| RV/TLC, % | 46.2 ± 13.1 | 46.0 ± 13.0 | 49.7 ± 13.8 | 0.188 |
| Baseline CT indices | ||||
| CT emphysema index | 27.7 ± 14.8 | 22.4 ± 16.1 | 18.1 ± 14.5 | 0.001 |
| CT air-trapping index | 94.6 ± 2.8 | 95.1 ± 3.6 | 94.2 ± 3.6 | 0.335 |
| Percentage wall area, % | 66.3 ± 4.8 | 67.7 ± 4.3 | 66.9 ± 5.0 | 0.207 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.W.; Lee, C.-H.; Hwang, H.-G.; Kim, Y.-I.; Kim, D.-K.; Oh, Y.-M.; Lee, S.H.; Kim, K.U.; Lee, S.-D. Decline in Carbon Monoxide Transfer Coefficient in Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2020, 9, 1512. https://doi.org/10.3390/jcm9051512
Kim YW, Lee C-H, Hwang H-G, Kim Y-I, Kim D-K, Oh Y-M, Lee SH, Kim KU, Lee S-D. Decline in Carbon Monoxide Transfer Coefficient in Chronic Obstructive Pulmonary Disease. Journal of Clinical Medicine. 2020; 9(5):1512. https://doi.org/10.3390/jcm9051512
Chicago/Turabian StyleKim, Yeon Wook, Chang-Hoon Lee, Hun-Gyu Hwang, Yu-Il Kim, Deog-Kyeom Kim, Yeon-Mok Oh, Sang Haak Lee, Ki Uk Kim, and Sang-Do Lee. 2020. "Decline in Carbon Monoxide Transfer Coefficient in Chronic Obstructive Pulmonary Disease" Journal of Clinical Medicine 9, no. 5: 1512. https://doi.org/10.3390/jcm9051512