Association of Specific Comorbidities with Monosodium Urate Crystal Deposition in Urate-Lowering Therapy-Naive Gout Patients: A Cross-Sectional Dual-Energy Computed Tomography Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Experimental Section
3. Results
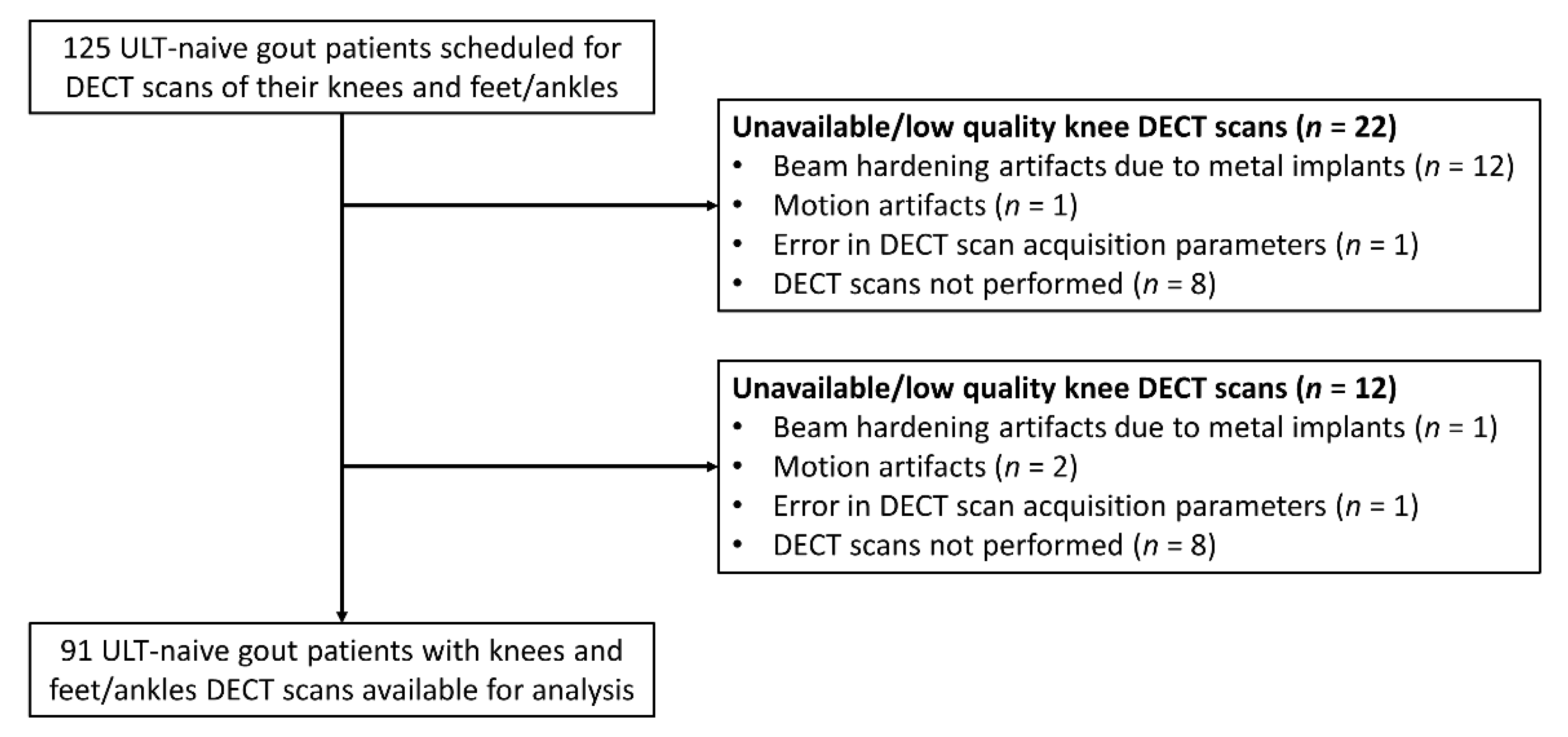
3.1. Patient Characteristics
3.2. Association Between Factors and the Total DECT Volume of MSU Crystal Deposition in the Knees and Feet/Ankles
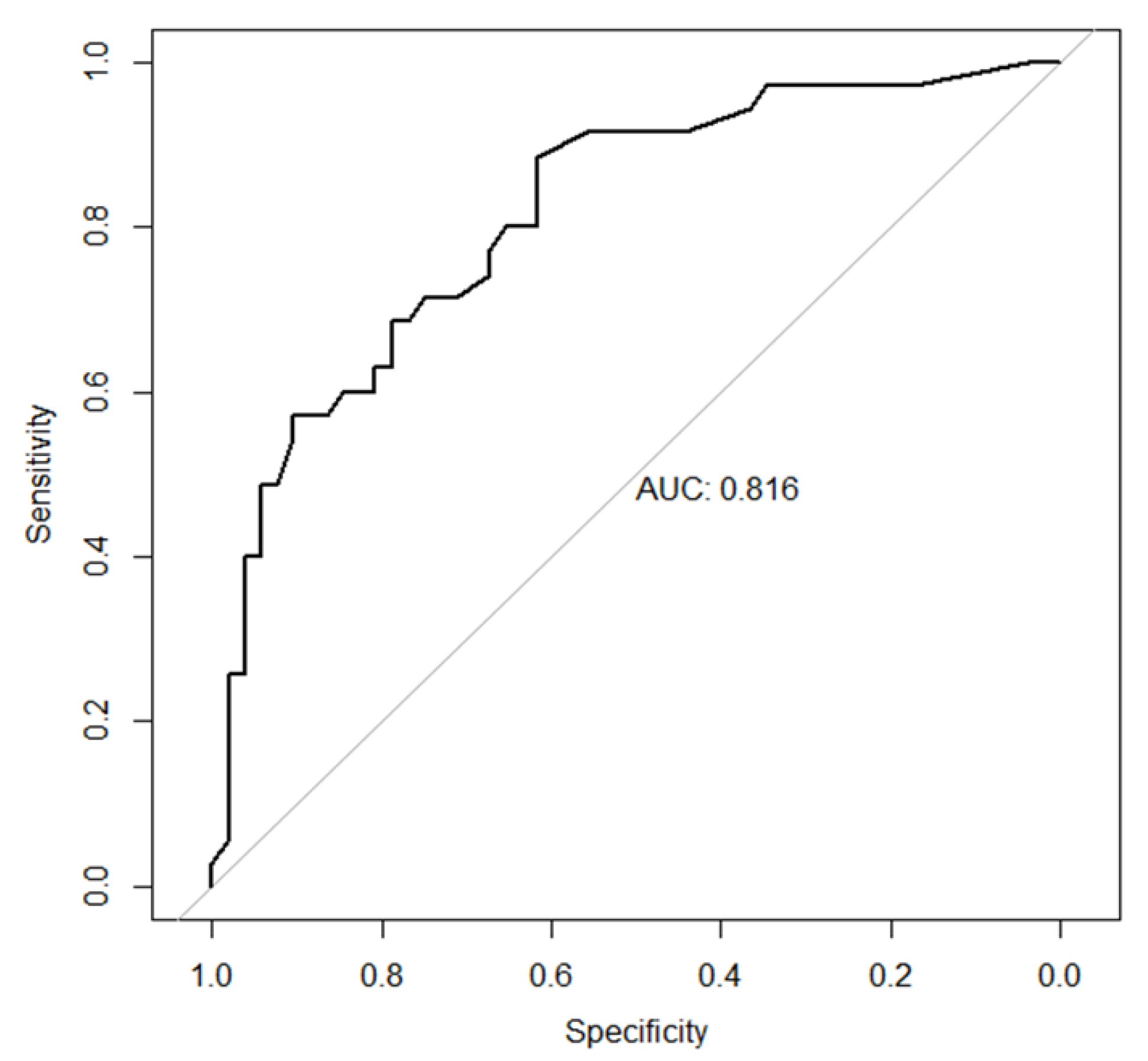
3.3. Factors Associated with the Total DECT Volume of MSU Crystal Deposition ≥1 cm3 in the Knees and Feet/Ankles
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Pascart, T.; Liote, F. Gout: State of the art after a decade of developments. Rheumatology (Oxford) 2019, 58, 27–44. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 388, 2039–2052. [Google Scholar] [CrossRef]
- Pascart, T.; Grandjean, A.; Capon, B.; Legrand, J.; Namane, N.; Ducoulombier, V.; Motte, M.; Vandecandelaere, M.; Luraschi, H.; Godart, C.; et al. Monosodium urate burden assessed with dual-energy computed tomography predicts the risk of flares in gout: A 12-month observational study: MSU burden and risk of gout flare. Arthritis Res. Ther. 2018, 20, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Ruiz, F.; Martinez-Indart, L.; Carmona, L.; Herrero-Beites, A.M.; Pijoan, J.I.; Krishnan, E. Tophaceous gout and high level of hyperuricaemia are both associated with increased risk of mortality in patients with gout. Ann. Rheum. Dis. 2014, 73, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Liote, F.; Lancrenon, S.; Lanz, S.; Guggenbuhl, P.; Lambert, C.; Saraux, A.; Chiarelli, P.; Delva, C.; Aubert, J.P.; Ea, H.K. GOSPEL: Prospective survey of gout in France. Part I: Design and patient characteristics (n = 1003). Joint Bone Spine 2012, 79, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Burns, L.C.; Shojania, K.; Koenig, N.; Reid, G.; Abufayyah, M.; Law, G.; Kydd, A.S.; Ouellette, H.; Nicolaou, S. Dual energy CT in gout: A prospective validation study. Ann. Rheum. Dis. 2012, 71, 1466–1471. [Google Scholar] [CrossRef]
- Filippou, G.; Pascart, T.; Iagnocco, A. Utility of Ultrasound and Dual Energy CT in Crystal Disease Diagnosis and Management. Curr. Rheumatol. Rep. 2020, 22, 15. [Google Scholar]
- Pascart, T.; Grandjean, A.; Norberciak, L.; Ducoulombier, V.; Motte, M.; Luraschi, H.; Vandecandelaere, M.; Godart, C.; Houvenagel, E.; Namane, N.; et al. Ultrasonography and dual-energy computed tomography provide different quantification of urate burden in gout: Results from a cross-sectional study. Arthritis Res. Ther. 2017, 19, 171. [Google Scholar] [CrossRef] [Green Version]
- Mallinson, P.I.; Coupal, T.; Reisinger, C.; Chou, H.; Munk, P.L.; Nicolaou, S.; Ouellette, H. Artifacts in dual-energy CT gout protocol: A review of 50 suspected cases with an artifact identification guide. AJR Am. J. Roentgenol. 2014, 203, W103–W109. [Google Scholar] [CrossRef]
- Chhana, A.; Lee, G.; Dalbeth, N. Factors influencing the crystallization of monosodium urate: A systematic literature review. BMC Musculoskelet. Disord. 2015, 16, 296. [Google Scholar] [CrossRef] [Green Version]
- Neogi, T.; Jansen, T.L.; Dalbeth, N.; Franse, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2015, 74, 1789–1798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bursill, D.; Taylor, W.J.; Terkeltaub, R.; Abhishek, A.; So, A.K.; Vargas-Santos, A.B.; Gaffo, A.L.; Rosenthal, A.; Tausche, A.; Reginato, A.; et al. Gout, Hyperuricaemia and Crystal-Associated Disease Network (G-CAN) consensus statement regarding labels and definitions of disease states of gout. Ann. Rheum. Dis. 2019, 78, 1592–1600. [Google Scholar] [CrossRef]
- Urano, W.; Yamanaka, H.; Tsutani, H.; Nakajima, H.; Matsuda, Y.; Taniguchi, A.; Hara, M.; Kamatani, N. The inflammatory process in the mechanism of decreased serum uric acid concentrations during acute gouty arthritis. J. Rheumatol. 2002, 29, 1950–1953. [Google Scholar] [PubMed]
- Kiefer, T.; Diekhoff, T.; Hermann, S.; Stroux, A.; Mews, J.; Blobel, J.; Hamm, B.; Hermann, K.G. Single source dual-energy computed tomography in the diagnosis of gout: Diagnostic reliability in comparison to digital radiography and conventional computed tomography of the feet. Eur. J. Radiol. 2016, 85, 1829–1834. [Google Scholar] [CrossRef] [PubMed]
- Dalbeth, N.; House, M.E.; Aati, O.; Tan, P.; Franklin, C.; Horne, A.; Gamble, G.D.; Stamp, L.K.; Doyle, A.J.; McQueen, F.M. Affiliations Urate crystal deposition in asymptomatic hyperuricaemia and symptomatic gout: A dual energy CT study. Ann. Rheum. Dis. 2015, 74, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Smith, S.E.; Garg, R.; Lu, F.; Wohlfahrt, A.; Campos, A.; Vanni, K.; Yu, Z.; Solomon, D.H.; Kim, S.C. Identification of monosodium urate crystal deposits in patients with asymptomatic hyperuricemia using dual-energy CT. RMD Open 2018, 4, e000593. [Google Scholar] [CrossRef]
- Stamp, L.K.; Zhu, X.; Dalbeth, N.; Jordan, S.; Edwards, N.L.; Taylor, W. Serum urate as a soluble biomarker in chronic gout-evidence that serum urate fulfills the OMERACT validation criteria for soluble biomarkers. Semin. Arthritis Rheum. 2011, 40, 483–500. [Google Scholar] [CrossRef]
- Richette, P.; Clerson, P.; Perissin, L.; Flipo, R.-M.; Bardin, T. Revisiting comorbidities in gout: A cluster analysis. Ann. Rheum. Dis. 2015, 74, 142–147. [Google Scholar] [CrossRef] [Green Version]
- Metra, M.; Teerlink, J.R. Heart failure. Lancet 2017, 390, 1981–1995. [Google Scholar] [CrossRef]
- Drexler, H. Changes in the peripheral circulation in heart failure. Curr. Opin. Cardiol. 1995, 10, 268–273. [Google Scholar] [CrossRef]
- Cicero, A.F.; Salvi, P.; D’Addato, S.; Rosticci, M.; Borghi, C. Association between serum uric acid, hypertension, vascular stiffness and subclinical atherosclerosis: Data from the Brisighella Heart Study. J. Hypertens. 2014, 32, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Klauser, A.S.; Halpern, E.J.; Strobl, S.; Gruber, J.; Feuchtner, G.; Bellmann-Weiler, R.; Weiss, G.; Stofferin, H.; Jaschke, W.R. Dual-Energy Computed Tomography Detection of Cardiovascular Monosodium Urate Deposits in Patients With Gout. JAMA Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bardin, T.; Richette, P. Impact of comorbidities on gout and hyperuricaemia: An update on prevalence and treatment options. BMC Med. 2017, 15, 123. [Google Scholar] [CrossRef] [PubMed]
- Rho, Y.H.; Lu, N.; Peloquin, C.E.; Man, A.; Zhu, Y.; Zhang, Y.; Choi, H.K. Independent impact of gout on the risk of diabetes mellitus among women and men: A population-based, BMI-matched cohort study. Ann. Rheum. Dis. 2016, 75, 91–95. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients (n = 91) Mean ± SD (Median (Interquartile Range)) | Complete Data | |
|---|---|---|
| Demographics | ||
| Age (years) | 65.3 ± 15.7 | 91 |
| Gout duration (years) | 7.4 ± 9.7 (3 (0.5; 8)) | 91 |
| Male gender | 76 (83.5%) | 91 |
| BMI (kg/m2) | 29.2 ± 5.1 | 90 |
| Disease history | ||
| Number of flares (in last six months) | 2.2 ± 2.2 (2 (1; 2)) | 90 |
| Tophi | 18 (20%) | 90 |
| Urolithiasis | 13 (14.3%) | 91 |
| Comorbidities | ||
| Hypertension | 63 (70%) | 90 |
| Stroke | 4 (4.5%) | 89 |
| Myocardial infarction | 16 (18%) | 89 |
| Diabetes mellitus | 26 (29.2%) | 89 |
| Chronic heart failure | 18 (20.2%) | 89 |
| Ongoing drugs | ||
| Diuretics | 27 (30.3%) | 89 |
| Anti-inflammatory drugs | 4 (4.4%) | 90 |
| Lipid-lowering drugs | 35 (41.7%) | 84 |
| Laboratory results | ||
| Serum urate level (mg/dL) | 9.1 ± 2.2 (88 (77; 99)) | 88 |
| eGFR (mL/min/1.73 m2) | 70.7 ± 27.0 | 89 |
| Triglycerides level (mg/dL) | 197 ± 349 (160 (111; 206)) | 54 |
| Cholesterol level (mg/dL) | 179 ± 55 | 56 |
| LDL level (mg/dL) | 100 ± 39 | 54 |
| HDL level (mg/dL) | 43 ± 12 | 54 |
| Variable | N | Spearman Correlation Coefficient | 95% CI | p-Value |
|---|---|---|---|---|
| Age | 91 | 0.22 | (0.01; 0.42) | 0.03 |
| Gout duration | 91 | 0.31 | (0.10; 0.51) | 0.003 |
| Number of flares (in last six months) | 90 | 0.19 | (−0.03; 0.38) | 0.08 |
| eGFR | 89 | −0.14 | (−0.34; 0.08) | 0.19 |
| Serum urate level | 88 | 0.07 | (−0.14; 0.26) | 0.52 |
| BMI | 90 | −0.10 | (−0.32; 0.12) | 0.37 |
| Triglycerides level | 53 | 0.04 | (−0.26; 0.32) | 0.77 |
| Cholesterol level | 56 | −0.06 | (−0.31; 0.20) | 0.68 |
| LDL level | 54 | −0.09 | (−0.37; 0.20) | 0.51 |
| HDL level | 54 | 0.06 | (−0.21; 0.32) | 0.66 |
| 9 | N | Median MSU Crystal DECT Volume (cm3) (Q1; Q3) | p-Value | |
|---|---|---|---|---|
| Gender | Female | 15 | 0.87 (0.18; 2.41) | 0.70 |
| Male | 76 | 0.45 (0.15; 2.08) | ||
| Ongoing anti-inflammatory drugs | No | 86 | 0.56 (0.16; 2.24) | 0.48 |
| Yes | 4 | 1.9 (0.29; 8.63) | ||
| Subcutaneous tophi | No | 72 | 0.43 (0.12; 1.90) | 0.004 |
| Yes | 18 | 2.68 (0.71; 6.33) | ||
| Urolithiasis | No | 78 | 0.56 (0.16; 2.24) | 0.56 |
| Yes | 13 | 0.3 (0.07; 2.28) | ||
| Hypertension | No | 27 | 0.38 (0.10; 0.62) | 0.02 |
| Yes | 63 | 1.01 (0.18; 2.66) | ||
| Stroke | No | 85 | 0.59 (0.16; 2.28) | 0.06 |
| Yes | 4 | 0.16 (0.12; 0.18) | ||
| Myocardial infarction | No | 73 | 0.46 (0.16; 1.96) | 0.15 |
| Yes | 16 | 2.05 (0.30; 4.46) | ||
| Diabetes mellitus | No | 63 | 0.41 (0.09; 2.11) | 0.05 |
| Yes | 26 | 1.09 (0.29; 2.63) | ||
| Ongoing lipid-lowering drugs | No | 49 | 0.54 (0.13; 2.28) | 0.57 |
| Yes | 35 | 0.36 (0.14; 2.11) | ||
| Chronic heart failure | No | 71 | 0.42 (0.12; 1.96) | 0.03 |
| Yes | 18 | 2.04 (0.70; 2.95) | ||
| Ongoing diuretics | No | 62 | 0.45 (0.16; 2.26) | 0.89 |
| Yes | 27 | 1.79 (0.13; 2.26) | ||
| Gout duration | ≤2 years | 37 | 0.25 (0.10; 0.70) | 0.007 |
| >2 years | 54 | 1.01 (0.22; 3.00) | ||
| eGFR (mL/min/1.73 m2) | <60 | 30 | 1.21 (0.19; 2.48) | 0.51 |
| ≥60 | 59 | 0.44 (0.12; 1.99) |
| Factor | Original Coefficient | Standard Error | 95% CI |
|---|---|---|---|
| Age | −0.15 | 0.08 | (−0.36; 0.05) |
| Gout duration | 0.36 | 0.13 | (0.02; 0.97) |
| Number of flares (in last six months) | 0.86 | 0.51 | (−0.43; 3.45) |
| Subcutaneous tophi | 7.30 | 3.02 | (−0.21; 16.93) |
| Chronic heart failure | 7.13 | 2.99 | (−2.32; 16.36) |
| MSU Volume < 1 cm3 (n = 55) | MSU Volume ≥1 cm3 (n = 36) | p-Value | |
|---|---|---|---|
| Age (years) | 61.4 ± 16.8 | 71.2 ± 11.7 | 0.006 |
| Gout duration (years) | 4.9 ± 6.6 | 11.2 ± 12.1 | 0.002 |
| Gout duration >2 years | 26 (47.3%) | 28 (77.8%) | 0.007 |
| Male gender | 47 (85.5%) | 29 (80.6%) | 0.74 |
| BMI (kg/m2) | 29.3 ± 4.6 | 29 ± 5.8 | 0.38 |
| Number of flares (in last six months) | 2.1 ± 2.3 | 2.3 ± 2.1 | 0.35 |
| Tophi | 6 (11.1%) | 12 (33.3%) | 0.021 |
| MSU DECT volume (cm3) | 0.27 ± 0.25 | 8.4 ± 17.2 | <0.0001 |
| Anti-inflammatory drugs | 2 (3.7%) | 2 (5.6%) | 1 |
| Serum urate level (mg/dL) | 8.9 ± 1.9 | 9.5 ± 2.5 | 0.50 |
| eGFR ≥ 60 (mL/min/1.73 m2) | 39 (72.2%) | 20 (57.1%) | 0.21 |
| Urolithiasis | 8 (14.5%) | 5 (13.9%) | 1 |
| Hypertension | 30 (55.6%) | 33 (91.7%) | 0.0006 |
| Stroke | 4 (7.5%) | 0 (0%) | 0.14 |
| Myocardial infarction | 7 (13.2%) | 9 (25%) | 0.25 |
| Diabetes mellitus | 12 (22.6%) | 14 (38.9%) | 0.16 |
| Chronic heart failure | 5 (9.4%) | 13 (36.1%) | 0.005 |
| Diuretics | 12 (22.6%) | 15 (41.7%) | 0.09 |
| Lipid-lowering drugs | 20 (40%) | 15 (44.1%) | 0.88 |
| Triglycerides level (mg/dL) | 224 ± 448 | 154 ± 59 | 0.86 |
| Cholesterol level (mg/dL) | 184 ± 65 | 172 ± 36 | 0.71 |
| LDL level (mg/dL) | 103 ± 41 | 96 ± 35 | 0.50 |
| HDL level (mg/dL) | 43 ± 11 | 44 ± 15 | 0.84 |
| Model Coefficient | OR | 95% CI | p-Value | |
|---|---|---|---|---|
| Gout symptom duration (per 10-year increase) | 1.15 | 3.15 | (1.60; 7.63) | 0.004 |
| Diabetes mellitus | 1.56 | 4.75 | (1.58; 15.63) | 0.007 |
| Chronic heart failure | 2.06 | 7.82 | (2.29; 31.38) | 0.002 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascart, T.; Ramon, A.; Ottaviani, S.; Legrand, J.; Ducoulombier, V.; Houvenagel, E.; Norberciak, L.; Richette, P.; Becce, F.; Ornetti, P.; et al. Association of Specific Comorbidities with Monosodium Urate Crystal Deposition in Urate-Lowering Therapy-Naive Gout Patients: A Cross-Sectional Dual-Energy Computed Tomography Study. J. Clin. Med. 2020, 9, 1295. https://doi.org/10.3390/jcm9051295
Pascart T, Ramon A, Ottaviani S, Legrand J, Ducoulombier V, Houvenagel E, Norberciak L, Richette P, Becce F, Ornetti P, et al. Association of Specific Comorbidities with Monosodium Urate Crystal Deposition in Urate-Lowering Therapy-Naive Gout Patients: A Cross-Sectional Dual-Energy Computed Tomography Study. Journal of Clinical Medicine. 2020; 9(5):1295. https://doi.org/10.3390/jcm9051295
Chicago/Turabian StylePascart, Tristan, André Ramon, Sébastien Ottaviani, Julie Legrand, Vincent Ducoulombier, Eric Houvenagel, Laurène Norberciak, Pascal Richette, Fabio Becce, Paul Ornetti, and et al. 2020. "Association of Specific Comorbidities with Monosodium Urate Crystal Deposition in Urate-Lowering Therapy-Naive Gout Patients: A Cross-Sectional Dual-Energy Computed Tomography Study" Journal of Clinical Medicine 9, no. 5: 1295. https://doi.org/10.3390/jcm9051295