Influence of Anesthesia and Clinical Variables on the Firing Rate, Coefficient of Variation and Multi-Unit Activity of the Subthalamic Nucleus in Patients with Parkinson’s Disease

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Anesthetic Management
2.3. Surgical Procedure
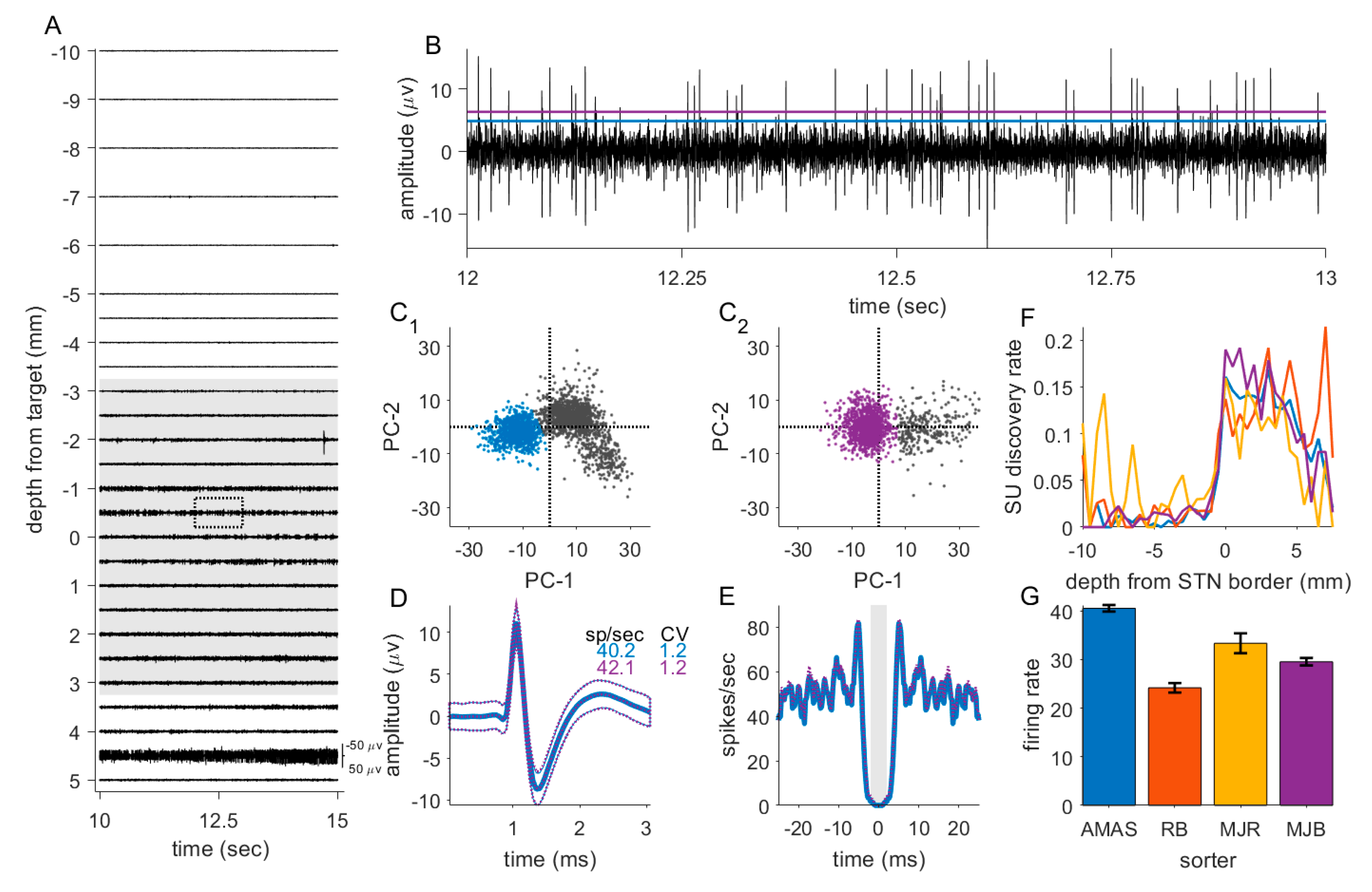
2.4. MER Acquisition
2.5. Data Processing and Analysis
2.6. Statistical Analysis
3. Results
3.1. Demographics
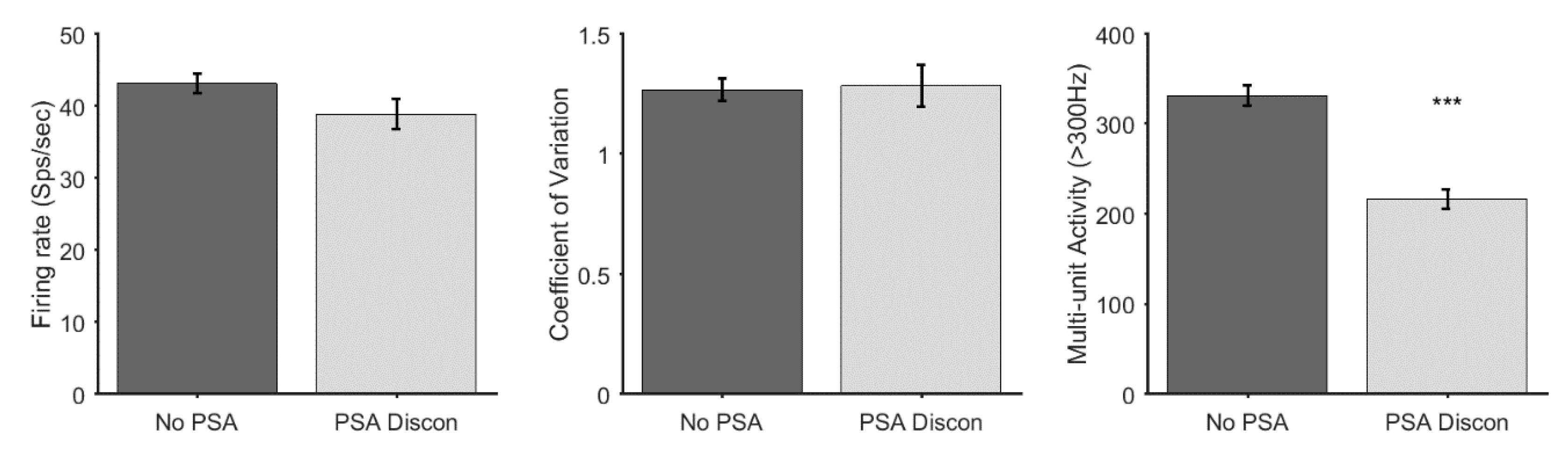
3.2. Discontinuation of Sedative Agents
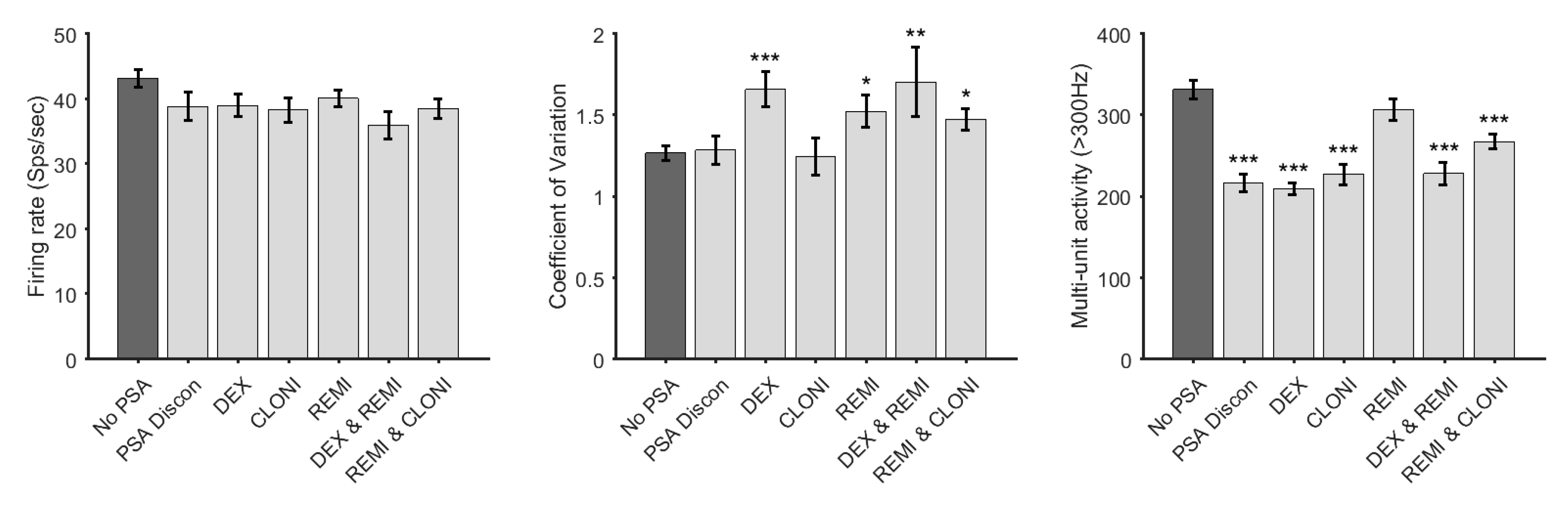
3.3. Effect of PSA Agents on Firing Rate, Coefficient of Variation and Multi-Unit Activity
3.4. Interrater Reliability
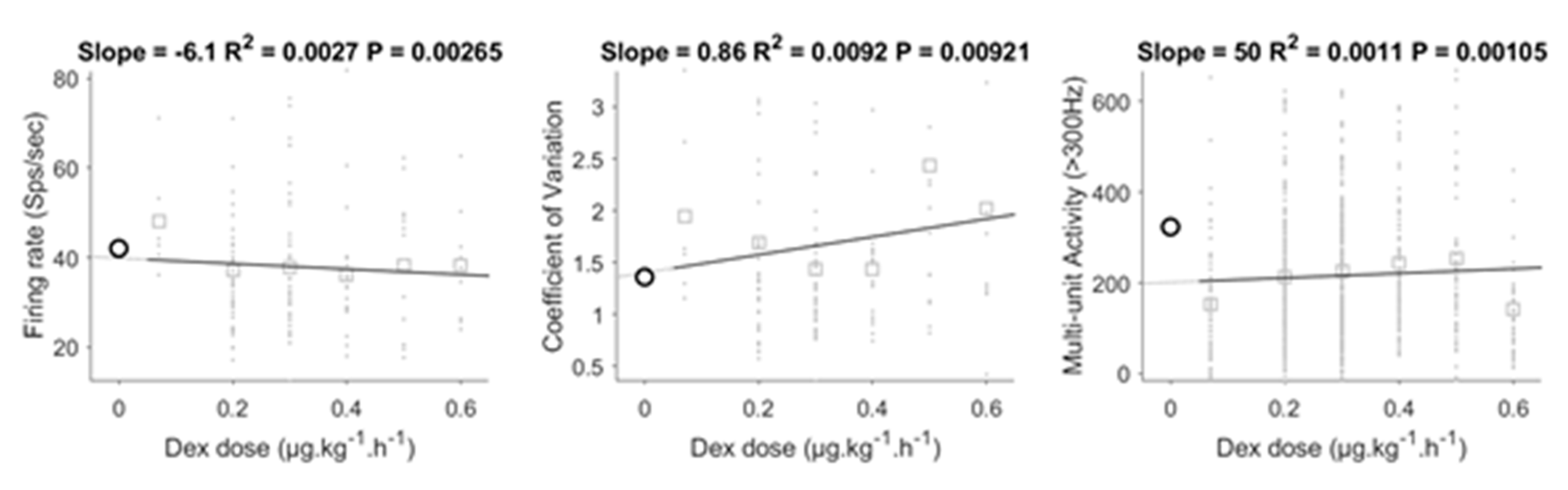
3.5. Dose-Dependent Effect of DEX
4. Discussion
4.1. Effect of Procedural Sedation and Analgesia on Micro-Electrode Recordings
4.1.1. Dexmedetomidine
4.1.2. Clonidine
4.1.3. Remifentanil
4.2. Effect of Clinical and Demographic Variables on Microelectrode Recordings
Multi-Unit Activity
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Fasano, A.; Daniele, A.; Albanese, A. Treatment of motor and non-motor features of Parkinson’s disease with deep brain stimulation. Lancet Neurol. 2012, 11, 429–442. [Google Scholar] [CrossRef]
- Welter, M.-L.; Schüpbach, M.; Czernecki, V.; Karachi, C.; Fernandez-Vidal, S.; Golmard, J.-L.; Serra, G.; Navarro, S.; Welaratne, A.; Hartmann, A.; et al. Optimal target localization for subthalamic stimulation in patients with Parkinson disease. Neurology 2014, 82, 1352–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeely, M.E.; Hershey, T.; Campbell, M.C.; Tabbal, S.D.; Karimi, M.; Hartlein, J.M.; Lugar, H.M.; Revilla, F.J.; Perlmutter, J.S.; Earhart, G.M. Effects of deep brain stimulation of dorsal versus ventral subthalamic nucleus regions on gait and balance in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2011, 82, 1250–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, B.; Machado, A.G.; Baker, K.B. Electrophysiologic mapping for deep brain stimulation for movement disorders. Handb. Clin. Neurol. 2019, 160, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Mulroy, E.; Robertson, N.; Macdonald, L.; Bok, A.; Simpson, M. Patients’ Perioperative Experience of Awake Deep-Brain Stimulation for Parkinson Disease. World Neurosurg. 2017, 105, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Sahinovic, M.M.; Struys, M.; Absalom, A. Clinical Pharmacokinetics and Pharmacodynamics of Propofol. Clin. Pharmacokinet. 2018, 57, 1539–1558. [Google Scholar] [CrossRef] [Green Version]
- Raz, A.; Eimerl, D.; Zaidel, A.; Bergman, H.; Israel, Z. Propofol Decreases Neuronal Population Spiking Activity in the Subthalamic Nucleus of Parkinsonian Patients. Anesthesia Analg. 2010, 111, 1285–1289. [Google Scholar] [CrossRef]
- Martinez-Simon, A.; Alegre, M.; Honorato-Cia, C.; Nuñez-Cordoba, J.M.; Cacho-Asenjo, E.; Trocóniz, I.F.; Carmona-Abellan, M.; Valencia, M.; Guridi, J. Effect of Dexmedetomidine and Propofol on Basal Ganglia Activity in Parkinson Disease. Anesthesiology 2017, 126, 1033–1042. [Google Scholar] [CrossRef]
- Moll, C.K.E.; Payer, S.; Gulberti, A.; Sharrott, A.; Zittel, S.; Boelmans, K.; Köppen, J.; Gerloff, C.; Westphal, M.; Engel, A.K.; et al. STN Stimulation in General Anaesthesia: Evidence Beyond ‘Evidence-Based Medicine’. Stereotact. Funct. Neurosurg. 2013, 117, 19–25. [Google Scholar] [CrossRef]
- Rozet, I.; Muangman, S.; Vavilala, M.S.; Lee, L.A.; Souter, M.J.; Domino, K.J.; Slimp, J.C.; Goodkin, R.; Lam, A.M. Clinical Experience with Dexmedetomidine for Implantation of Deep Brain Stimulators in Parkinson’s Disease. Anesthesia Analg. 2006, 103, 1224–1228. [Google Scholar] [CrossRef]
- Morace, R.; De Angelis, M.; Aglialoro, E.; Maucione, G.; Cavallo, L.; Solari, D.; Modugno, N.; Santilli, M.; Esposito, V.; Aloj, F. Sedation with α2 Agonist Dexmedetomidine During Unilateral Subthalamic Nucleus Deep Brain Stimulation: A Preliminary Report. World Neurosurg. 2016, 89, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Elias, W.J.; Durieux, M.; Huss, D.; Frysinger, R.C. Dexmedetomidine and arousal affect subthalamic neurons. Mov. Disord. 2008, 23, 1317–1320. [Google Scholar] [CrossRef] [PubMed]
- Krishna, V.; Elias, G.J.; Sammartino, F.; Basha, D.; King, N.K.K.; Fasano, A.; Munhoz, R.; Kalia, S.K.; Hodaie, M.; Venkatraghavan, L.; et al. The effect of dexmedetomidine on the firing properties of STN neurons in Parkinson’s disease. Eur. J. Neurosci. 2015, 42, 2070–2077. [Google Scholar] [CrossRef] [PubMed]
- Mathews, L.; Camalier, C.R.; Kla, K.M.; Mitchell, M.D.; Konrad, P.E.; Neimat, J.S.; Smithson, K.G. The Effects of Dexmedetomidine on Microelectrode Recordings of the Subthalamic Nucleus during Deep Brain Stimulation Surgery: A Retrospective Analysis. Ster. Funct. Neurosurg. 2017, 95, 40–48. [Google Scholar] [CrossRef]
- Kwon, W.-K.; Kim, J.H.; Lee, J.-H.; Lim, B.-G.; Lee, I.-O.; Koh, S.B.; Kwon, T.H. Microelectrode recording (MER) findings during sleep–awake anesthesia using dexmedetomidine in deep brain stimulation surgery for Parkinson’s disease. Clin. Neurol. Neurosurg. 2016, 143, 27–33. [Google Scholar] [CrossRef]
- Bos, M.J.; Buhre, W.; Temel, Y.; Joosten, E.A.; Absalom, A.R.; Janssen, M.L. Effect of Anesthesia on Microelectrode Recordings during Deep Brain Stimulation Surgery. J. Neurosurg. Anesthesiol. 2020. [Google Scholar] [CrossRef]
- Tepper, Á.; Henrich, M.C.; Schiaffino, L.; Rosado-Muñoz, A.; Gutiérrez, A.; Martínez, J.G. Selection of the Optimal Algorithm for Real-Time Estimation of Beta Band Power during DBS Surgeries in Patients with Parkinson’s Disease. Comput. Intell. Neurosci. 2017, 2017, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Oostenveld, R.; Fries, P.; Maris, E.; Schoffelen, J.-M. FieldTrip: Open Source Software for Advanced Analysis of MEG, EEG, and Invasive Electrophysiological Data. Comput. Intell. Neurosci. 2010, 2011, 1–9. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Hertel, F.; Züchner, M.; Weimar, I.; Gemmar, P.; Noll, B.; Bettag, M.; Decker, C. Implantation of electrodes for deep brain stimulation of the subthalamic nucleus in advanced Parkinson’s disease with the aid of intraoperative microrecording under general anesthesia. Neurosurgery 2006, 59, 1138. [Google Scholar] [CrossRef]
- Brohan, J.; Goudra, B.G. The Role of GABA Receptor Agonists in Anesthesia and Sedation. CNS Drugs 2017, 31, 845–856. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.W.; Ehm, G.; Yang, H.J.; Song, I.H.; Lim, Y.H.; Kim, M.R.; Kim, Y.E.; Hwang, J.H.; Park, H.R.; Lee, J.M.; et al. Bilateral Deep Brain Stimulation of the Subthalamic Nucleus under Sedation with Propofol and Fentanyl. PLoS ONE 2016, 11, e0152619. [Google Scholar] [CrossRef] [PubMed]
- Duque, P.; Mateo, O.; Ruiz, F.; De Viloria, J.G.; Contreras, A.; Grandas, F. Intraoperative microrecording under general anaesthesia with bispectral analysis monitoring in a case of deep brain stimulation surgery for Parkinsons disease. Eur. J. Neurol. 2008, 15, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Maciver, M.B.; Bronte-Stewart, H.M.; Henderson, J.M.; Jaffe, R.A.; Brock-Utne, J.G.; Henderson, J.M. Human Subthalamic Neuron Spiking Exhibits Subtle Responses to Sedatives. Anesthesiology 2011, 115, 254–264. [Google Scholar] [CrossRef] [Green Version]
- Bhana, N.; Goa, K.L.; McClellan, K.J. Dexmedetomidine. Drugs 2000, 59, 263–268. [Google Scholar] [CrossRef]
- Weerink, M.; Struys, M.; Hannivoort, L.N.; Barends, C.R.M.; Absalom, A.R.; Colin, P. Clinical Pharmacokinetics and Pharmacodynamics of Dexmedetomidine. Clin. Pharmacokinet. 2017, 56, 893–913. [Google Scholar] [CrossRef] [Green Version]
- Jamadarkhana, S.; Gopal, S. Clonidine in Adults as a Sedative Agent in the Intensive Care Unit. J. Anaesthesiol. Clin. Pharmacol. 2010, 26, 439–445. [Google Scholar]
- Delaville, C.; Zapata, J.; Cardoit, L.; Benazzouz, A. Activation of subthalamic alpha 2 noradrenergic receptors induces motor deficits as a consequence of neuronal burst firing. Neurobiol. Dis. 2012, 47, 322–330. [Google Scholar] [CrossRef]
- Belujon, P.; Bezard, E.; Taupignon, A.; Bioulac, B.; Benazzouz, A. Noradrenergic Modulation of Subthalamic Nucleus Activity: Behavioral and Electrophysiological Evidence in Intact and 6-Hydroxydopamine-Lesioned Rats. J. Neurosci. 2007, 27, 9595–9606. [Google Scholar] [CrossRef] [Green Version]
- Michelsen, L.G.; Hug, C.C., Jr. The pharmacokinetics of remifentanil. J. Clin. Anesthesia 1996, 8, 679–682. [Google Scholar] [CrossRef]
- Stanford, I.M.; Cooper, A.J. Presynaptic mu and delta opioid receptor modulation of GABAA IPSCs in the rat globus pallidus in vitro. J. Neurosci. 1999, 19, 4796–4803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, K.Z.; Johnson, S.W. Presynaptic modulation of synaptic transmission by opioid receptor in rat subthalamic nucleusin vitro. J. Physiol. 2002, 541, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Song, I.H.; Lim, Y.H.; Kim, M.R.; Kim, Y.E.; Hwang, J.H.; Kim, I.K.; Song, S.W.; Kim, J.W.; Lee, W.W.; et al. Influence of Propofol and Fentanyl on Deep Brain Stimulation of the Subthalamic Nucleus. J. Korean Med. Sci. 2014, 29, 1278–1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, M.L.; Zwartjes, D.G.; Tan, S.K.; Vlamings, R.; Jahanshahi, A.; Heida, T.; Hoogland, G.; Steinbusch, H.W.; Visser-Vandewalle, V.; Temel, Y. Mild dopaminergic lesions are accompanied by robust changes in subthalamic nucleus activity. Neurosci. Lett. 2012, 508, 101–105. [Google Scholar] [CrossRef]
- Bergman, H.; Wichmann, T.; Karmon, B.; DeLong, M.R. The primate subthalamic nucleus. II. Neuronal activity in the MPTP model of parkinsonism. J. Neurophysiol. 1994, 72, 507–520. [Google Scholar] [CrossRef]
- Bočková, M.; Chladek, J.; Jurak, P.; Halamek, J.; Balaz, M.; Rektor, I. Involvement of the subthalamic nucleus and globus pallidus internus in attention. J. Neural Transm. 2010, 118, 1235–1245. [Google Scholar] [CrossRef]
- Baunez, C.; Robbins, T.W. Bilateral lesions of the subthalamic nucleus induce multiple deficits in an attentional task in rats. Eur. J. Neurosci. 1997, 9, 2086–2099. [Google Scholar] [CrossRef]
- Asanowicz, D.; Marzecová, A.; Jaśkowski, P.; Wolski, P. Hemispheric asymmetry in the efficiency of attentional networks. Brain Cogn. 2012, 79, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Eitan, R.; Shamir, R.R.; Linetsky, E.; Rosenbluh, O.; Moshel, S.; Ben-Hur, T.; Bergman, H.; Israel, Z. Asymmetric right/left encoding of emotions in the human subthalamic nucleus. Front. Syst. Neurosci. 2013, 7, 69. [Google Scholar] [CrossRef] [Green Version]
- Voytek, B.; Kramer, M.A.; Case, J.; Lepage, K.Q.; Tempesta, Z.R.; Knight, R.T.; Gazzaley, A. Age-related changes in 1/f neural electrophysiological noise. J. Neurosci. 2015, 35, 13257–13265. [Google Scholar] [CrossRef]
- Dave, S.; Brothers, T.A.; Swaab, T.Y. 1/f neural noise and electrophysiological indices of contextual prediction in aging. Brain Res. 2018, 1691, 34–43. [Google Scholar] [CrossRef]
- Leenders, M.P.; Lozano-Soldevilla, D.; Roberts, M.; Jensen, O.; De Weerd, P. Diminished Alpha Lateralization During Working Memory but Not During Attentional Cueing in Older Adults. Cereb. Cortex 2016, 28, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.L.; Rebec, G.V. A new perspective on behavioral inconsistency and neural noise in aging: Compensatory speeding of neural communication. Front. Aging Neurosci. 2012, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Dunnen, W.F.D.; Staal, M.J. Anatomical alterations of the subthalamic nucleus in relation to age: A postmortem study. Mov. Disord. 2005, 20, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Valsky, D.; Marmor-Levin, O.; Deffains, M.; Eitan, R.; Blackwell, K.T.; Bergman, H.; Israel, Z. Stop! border ahead: Automatic detection of subthalamic exit during deep brain stimulation surgery. Mov. Disord. 2017, 32, 70–79. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Patients M/F | Hemispheres (n) | Electrodes (n) | SU/MUA (n) | Age (y) | UPDRS III | Dose Range | ||
|---|---|---|---|---|---|---|---|---|---|
| Awake | No PSA | 15/6 | 42 | 149 | 165/1257 | 59.4 ± 8.3 | 38.2 ± 16.5 | ||
| PSA discon | 4/3 | 14 | 42 | 51/339 | 59.3 ± 7.6 | 42.0 ± 8.5 | |||
| Sedation | DEX | 7/4 | 22 | 70 | 86/565 | 60.9 ± 5.9 | 33.4 ± 12.4 | 0.07–0.6 µg kg−1 h−1 | |
| REMI | 8/6 | 28 | 99 | 93/636 | 58.1 ± 8.0 | 37.9 ± 14.3 | 0.02–0.25 µg kg−1 min−1 | ||
| CLONI | 6/2 | 16 | 56 | 41/339 | 64.8 ± 8.3 | 35.8 ± 11.9 | 20–50 µg h−1 or 30–150 µg IV in bolus | ||
| DEX + REMI | 4/1 | 10 | 35 | 46/267 | 65.8 ± 6.5 | 34.3 ± 7.8 | DEX 0.3–0.5 µg kg−1 h−1 | REMI 0.02–0.05 µg kg−1 min−1 | |
| CLONI + REMI | 6/6 | 24 | 84 | 106/679 | 59.5 ± 7.3 | 36.4 ± 9.1 | CLONI 20 µg h−1 or 45–150 µg IV in bolus | REMI 0.01–0.09 µg kg−1 min−1 | |
| Total | 50/28 | 156 | 535 | 588/4082 | 60.5 ± 7.7 | 37.0 ± 12.8 | |||
| Variable | Firing Rate | Coefficient of Variation | Multi-Unit Activity | ||||
|---|---|---|---|---|---|---|---|
| Estimate | p-Value | Estimate | p-Value | Estimate | p-Value | ||
| DEX | Yes | −3.121 | 0.068 | 0.313 | 0.001 | −88.814 | <0.001 |
| REMI | Yes | −2.105 | 0.141 | 0.163 | 0.040 | 2.607 | 0.806 |
| CLONI | Yes | −2.156 | 0.203 | −0.004 | 0.963 | −50.923 | 0.675 |
| PSA (DISCONTINUED) | Yes | −3.836 | 0.120 | −0.011 | 0.933 | −115.240 | <0.001 |
| SEX | Male | 0.379 | 0.808 | −0.031 | 0.720 | −2.112 | 0.855 |
| ONSET SIDE | Ipsilateral (*) | −1.840 | 0.152 | 0.100 | 0.161 | −16.353 | 0.090 |
| HEMISPHERE | Right | 1.854 | 0.150 | −0.087 | 0.222 | 24.785 | 0.010 |
| AGE | Years | −0.091 | 0.314 | 0.001 | 0.788 | −43.996 | <0.001 |
| WEIGHT | Kg | −0.004 | 0.931 | −0.003 | 0.337 | 0.452 | 0.181 |
| UPDRS III | 0.068 | 0.196 | 0.002 | 0.428 | −0.026 | 0.946 | |
| DISEASE DURATION | Months | −0.002 | 0.914 | −0.002 | 0.020 | −0.018 | 0.882 |
| STN DEPTH | mm | 0.560 | 0.130 | −0.008 | 0.681 | 25.024 | <0.001 |
| Model data | R-squared: 0.035 Adjusted R-Squared 0.0149 p-value = 0.0553 | R-squared: 0.0511 Adjusted R-Squared 0.0313 p-value = 0.00241 | R-squared: 0.0586 Adjusted R-Squared 0.0558 p-value = 9.1e−46 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bos, M.J.; Alzate Sanchez, A.M.; Bancone, R.; Temel, Y.; de Greef, B.T.A.; Absalom, A.R.; Gommer, E.D.; van Kranen-Mastenbroek, V.H.J.M.; Buhre, W.F.; Roberts, M.J.; et al. Influence of Anesthesia and Clinical Variables on the Firing Rate, Coefficient of Variation and Multi-Unit Activity of the Subthalamic Nucleus in Patients with Parkinson’s Disease. J. Clin. Med. 2020, 9, 1229. https://doi.org/10.3390/jcm9041229
Bos MJ, Alzate Sanchez AM, Bancone R, Temel Y, de Greef BTA, Absalom AR, Gommer ED, van Kranen-Mastenbroek VHJM, Buhre WF, Roberts MJ, et al. Influence of Anesthesia and Clinical Variables on the Firing Rate, Coefficient of Variation and Multi-Unit Activity of the Subthalamic Nucleus in Patients with Parkinson’s Disease. Journal of Clinical Medicine. 2020; 9(4):1229. https://doi.org/10.3390/jcm9041229
Chicago/Turabian StyleBos, Michael J., Ana Maria Alzate Sanchez, Raffaella Bancone, Yasin Temel, Bianca T.A. de Greef, Anthony R. Absalom, Erik D. Gommer, Vivianne H.J.M. van Kranen-Mastenbroek, Wolfgang F. Buhre, Mark J. Roberts, and et al. 2020. "Influence of Anesthesia and Clinical Variables on the Firing Rate, Coefficient of Variation and Multi-Unit Activity of the Subthalamic Nucleus in Patients with Parkinson’s Disease" Journal of Clinical Medicine 9, no. 4: 1229. https://doi.org/10.3390/jcm9041229