Umbilical Cord Milking in Infants Born at <37 Weeks of Gestation: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Data Extraction and Quality Assessment
2.3. Data Synthesis
2.4. Role of the Funding Source
3. Results
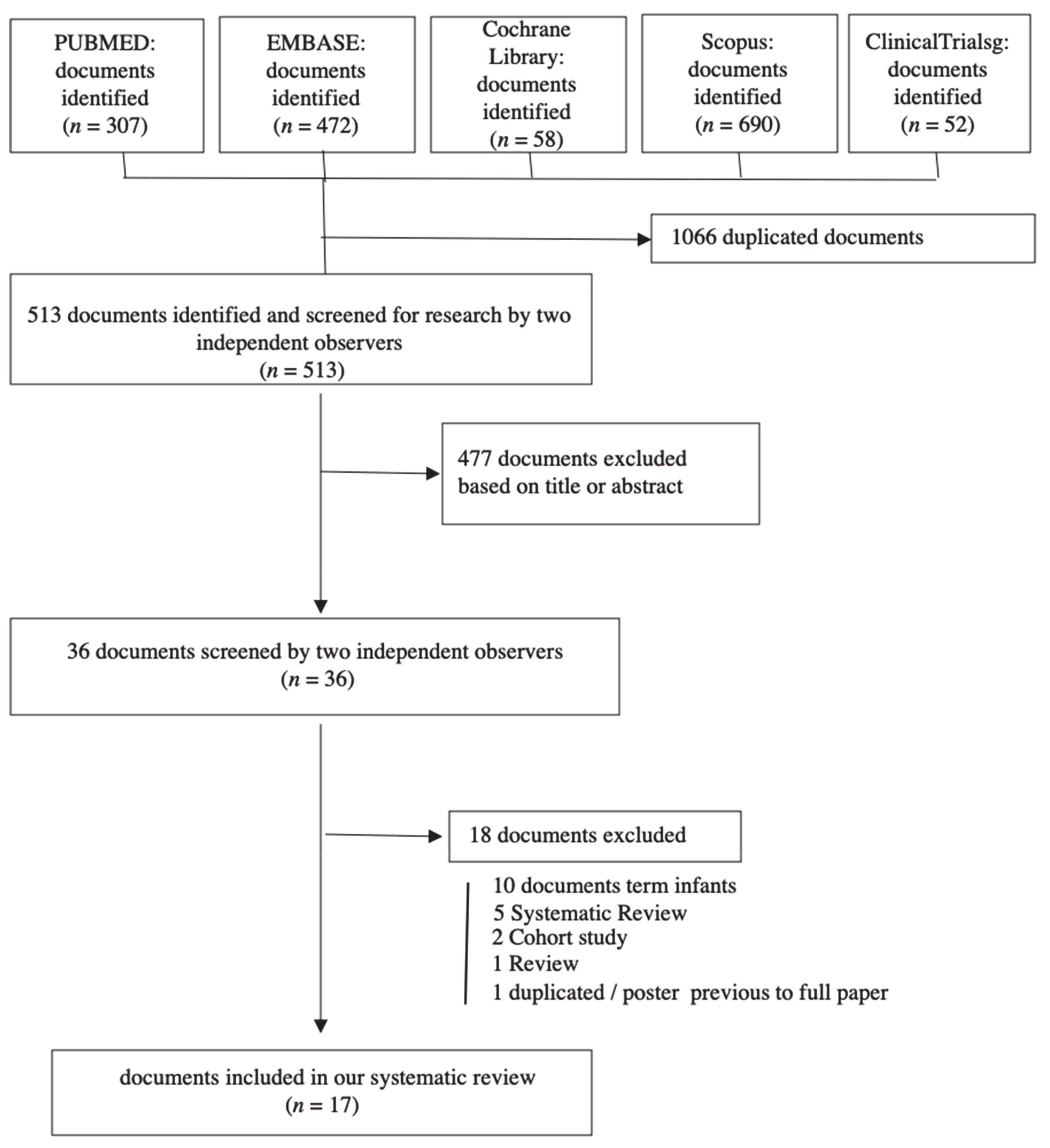
3.1. Study Selection
3.2. Study Characteristics
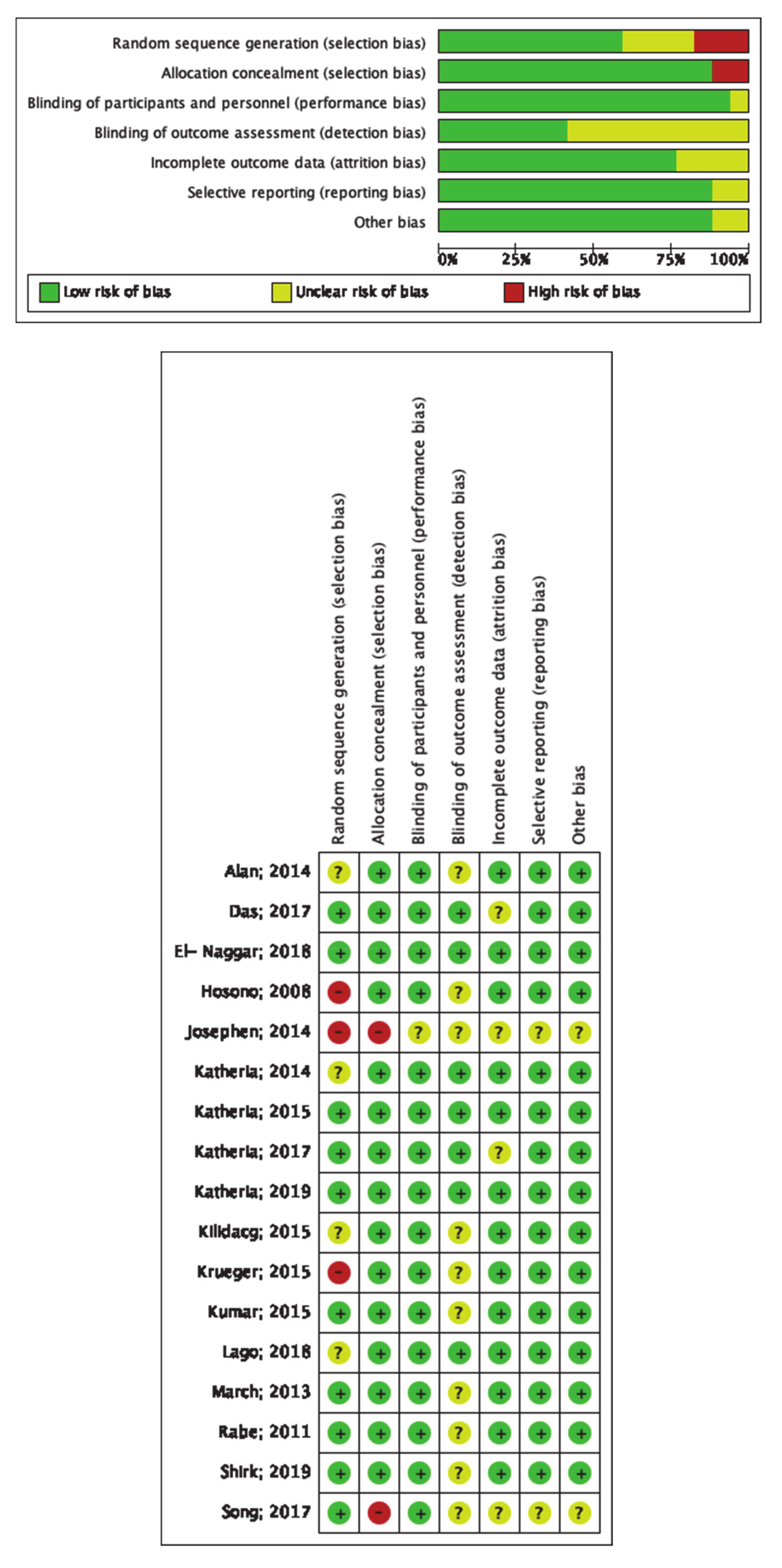
3.3. Study and Data Quality
3.4. Meta-Analysis
3.4.1. Mortality
3.4.2. Phototherapy
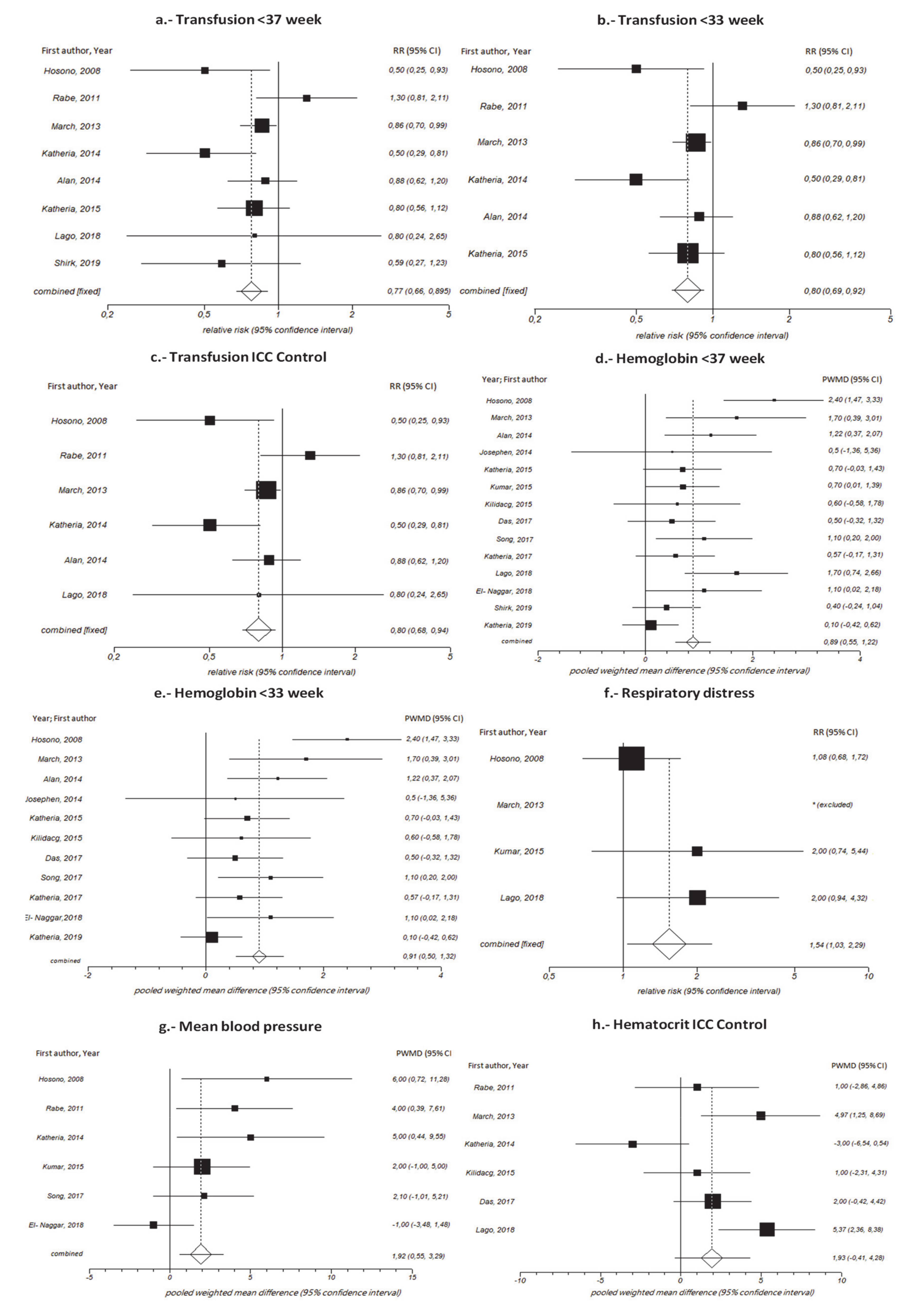
3.4.3. Transfusion
3.4.4. Hemoglobin
3.4.5. Hematocrit
3.4.6. Peak Serum Bilirubin
3.4.7. Mean blood pressure.
3.4.8. Respiratory Distress Syndrome
3.5. Other Variables
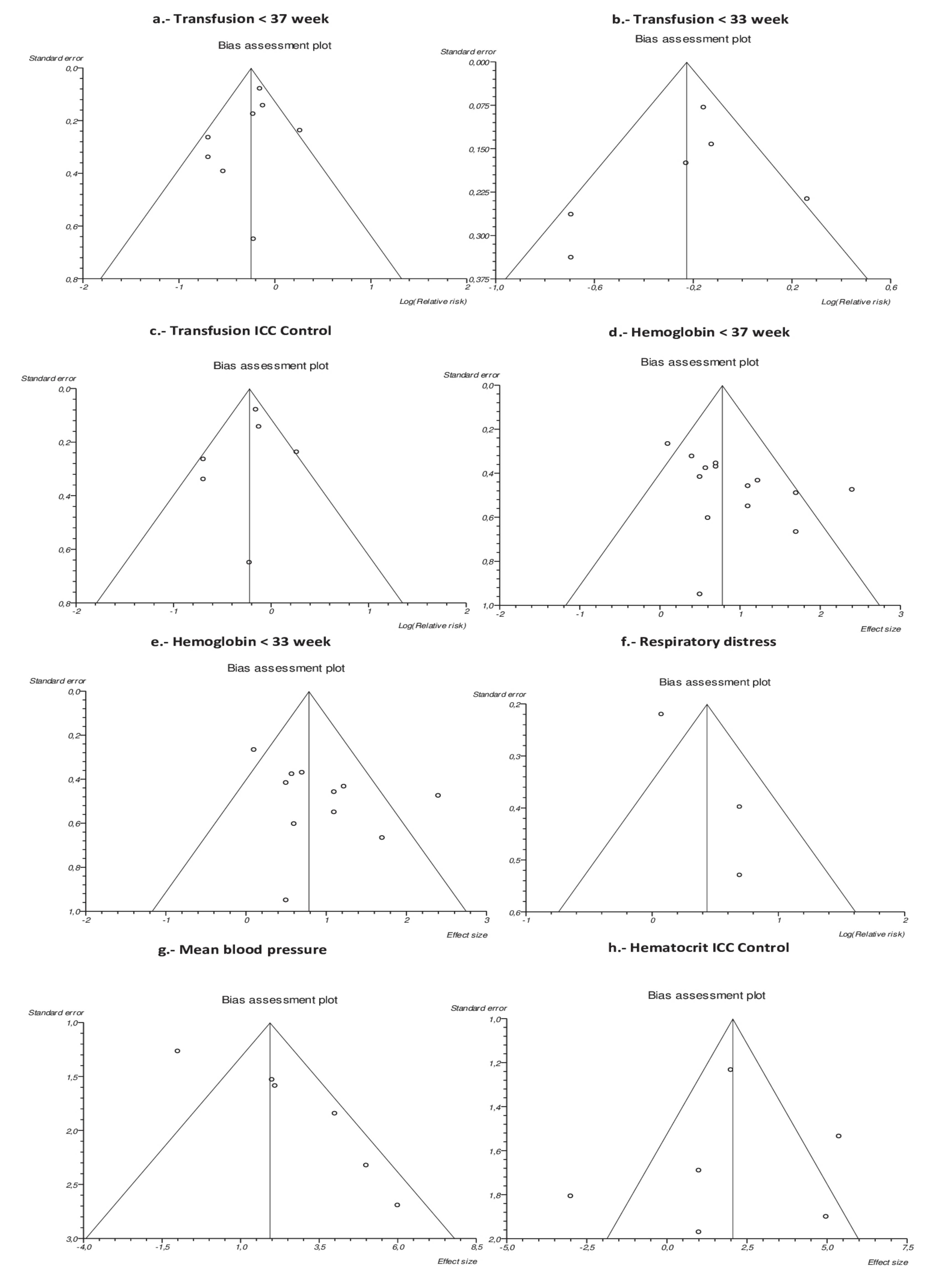
3.6. Publication Bias
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Strategies | Hits |
|---|---|---|
| Pubmed | (stripping[All Fields] OR milking[All Fields] OR squeezing[All Fields]) AND ((“umbilicus”[MeSH Terms] OR “umbilicus”[All Fields]) OR (“umbilical cord”[MeSH Terms] OR (“umbilical”[All Fields] AND “cord”[All Fields]) OR “umbilical cord”[All Fields]) OR (“cone-rod dystrophies”[MeSH Terms] OR (“cone-rod”[All Fields] AND “dystrophies”[All Fields]) OR “cone-rod dystrophies”[All Fields] OR “cord”[All Fields])) | 307 |
| Embase | (‘stripping’/exp OR stripping OR ‘milking’/exp OR milking OR squeezing) AND (‘umbilicus’/exp OR umbilicus OR ‘umbilical cord’/exp OR ‘umbilical cord’ OR ((‘umbilical’/exp OR umbilical) AND cord) OR cord) | 472 |
| Scopus | (strippingORmilkingORsqueezing) AND (umbilicusORumbilical AND cord OR cord) | 690 |
| Clinical trials | (stripping OR milking OR squeezing) AND (umbilical cord OR cord) | 52 |
| Cochrane Library plus | (stripping OR milking OR squeezing) AND (umbilicus OR umbilical AND cord OR cord) | 58 |


| Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment | Incomplete Outcomes Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | |
|---|---|---|---|---|---|---|---|
| Hosono S; 2008 Randomized controlled trial Jan 2001–Dec 2002 N = 40 (20:20) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| No information | Serially numbered opaque envelopes | Not blinded: Clinicians | The variables measured as principal outcomes do not depend on blinding | No missing values Follow up: Not stated (but at least 84 days according to the Kaplan-Meier curves plot) | |||
| Rabe H; 2011 Randomized controlled trial No date N = 58 (31:27) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Randomization was based on computer-created tables performed by a person not involved in the trial (stratified by gestational age) | Sealed opaque envelopes and consecutively numbered. | Not blinded: Clinicians | The variables measured as principal outcomes do not depend on blinding | No missing values Follow up: 42 days | According to sample size calculation, they need 58 (29 in each group and then 27 and 31, possible poor randomization or loss of random sequence masking | ||
| March MI, 2013 Randomized controlled trial Sep 2009–Jun 2011 N = 75 (36:39) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Were randomized before delivery to one of two groups using random permuted blocks of 10; an independent statistician provided the randomization sequence | Serially numbered opaque envelopes contained arm bands | Neonatologists and pediatric support staff were not blinded to treatment assignment | They were not alerted for study participation or treatment assignment and no notation of study participation | Control 18 missing values Milking 20 missing values Follow up: 28 days | |||
| Katheria A; 2014 Randomized controlled trial Feb 2011–Jan 2013 N = 60 (30:60) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Infants were randomized by the placement of their information in opaque, sealed envelopes. The randomization cards assigned a subject identification number that was kept by the research coordinator | In opaque, sealed envelopes | Not blinded: Clinicians | Blinded serial echocardiographic examinations were performed | No missing values | |||
| Alan S; 2014 Randomized controlled trial Apr 2011–Feb 2013 N = 44 (22:22) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Subjects were randomly assigned to one of the two experimental groups | Sequentially numbered sealed non-transparent envelopes | The intervention was unmasked for the attending neonatal and obstetric teams in the delivery room | Nothing stated. Some principal variables do not depend on blinding | Five missing values in each group Follow up: 28 days | |||
| Josephen; 2014 Randomized controlled trial Up to Aug 2013 N = 26 (13:13) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| No information | No information | No information | Nothing stated. Some principal variables do not depend on blinding | No information | No information | No information | |
| Katheria A; 2015 Randomized controlled trial N = 154 (75:79) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Computer-generated randomization | Opaque, sealed envelopes | The blinding was achieved by allowing only the nurse attending the delivery and the obstetrician performing the intervention to be aware of the allocation arm | Blinded echocardiograms and head ultrasounds were performed | No missing values Follow up: 24 h | |||
| Krueger MS; 2015 Prospective randomized trial Aug 2012–Nov 2013 N = 67 (32:35) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| An equal number of envelopes were created for each arm and were scrambled by a third-party registered nurse | Opaque envelopes | The neonatal team was not told which patients were participating in the study, and the randomization arm was not documented on the infants’ charts | Nothing stated. Some principal variables do not depend on blinding. Some secondary outcomes may be subjective. May have blinded the assessor | No missing values | |||
| Kumar B; 2015 Randomized controlled trial 2013–14 N = 200 (100:100) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Used an online generated random number list | Sealed envelope was opened by a delivery room staff nurse | Open-label | Nothing stated. Some variables may be subjective. They may have blinded the analyst | Control: 14 missing values Experimental: nine missing values Follow up: six weeks | |||
| Kilicdag H, 2015 Prospective randomized study Aug 2012–Aug 2013 N = 54 (25:29) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Were randomly assigned to one of the two groups | Using sequentially numbered sealed non-transparent envelopes | No information | Nothing stated. Some variables may be subjective, but it is not clear (segments, bands).If not subjective then low risk. Still, they may have blinded the analyst | Follow up: seven days | |||
| Das S; 2017 Randomized controlled trial Nov 2012–Dec 2013 N = 215 (116:99) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Random sequence was generated using a secure web-based randomization algorithm | Serially numbered, sealed, and opaque envelopes | Blinding of the personnel and participants was not feasible due to the nature of intervention | The laboratory person who analyzed the serum ferritin levels was blinded to group allocation | Follow up: three months | |||
| Song S; 2017 Randomized controlled trial Mar 2012–Jun 2015 N = 66 (34:32) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Randomized by computer-generated random numbers just before delivery | No information | No information | No information | No information | No information | No information | |
| Katheria A; 2017 Randomized controlled trial Aug 2013–Aug 2014 N = 197 (99:98) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Using computer-generated allocation | Sealed envelopes before delivery | The blinding was achieved by allowing only the ALS nurse attending the delivery and the obstetrician performing the intervention to be aware of the allocation arm | Neurodevelopmental assessment was carried out by examiners who were trained in administration of the Bayley-III, had excellent inter-rater reliability (0.90), and masked to the umbilical cord milking or DCC status | Milking: 23 missing values (a lot)DCC: 25 missing values (a lot) Follow up: two years | |||
| Lago;2018 Randomized controlled trial Feb 2013–Apr 2016 N = 138 (69:69) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Patients were randomized into one of the two groups: MM or ECC. | Randomization was carried out by a sealed non-transparent envelope and took place just prior to birth | The neonatologist was not aware of the timing of cord clamping. Special attention was paid to mask the intervention to the neonatology staff members (both physician and nurses) who were at the delivery room or theatre giving the first clinical care to the infants | Addition, the cord clamping interval was not registered in the infant’s chart, so this information was not available for the staff in the neonatal intensive care unit (NICU). | 21 missing values or exclusions Follow up: six months | |||
| El-Naggar; 2018 Randomized controlled trial N = 73 (37:36) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Was established using variable block sizes randomization table | Concealed opaque envelopes were prepared ahead of time and were opened just before the time of delivery | Despite our efforts to keep the healthcare providers blinded to the study intervention by not documenting the intervention in the charts, we cannot be absolutely sure that full blinding was achieved | Both the echocardiographer and the offline reader were blinded to patient’s assignment | No missing values Follow up: 48 h | |||
| Shirk; 2019 Randomized controlled trial Apr 2014–Jun 2018 N = 204 (104:100) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| The patients were assigned randomly via block randomization with an allocation ratio of 1:1 | Sealed opaque envelopes | Unblinded | Nothing stated. Some variables do not depend on blinding. They may have blinded the analyst | ||||
| Katheria; 2019 Randomized controlled trial Jun 2017–Dec 2018 N = 474 (236:238) | High Risk | Low Risk | Low Risk | Unclear | Low Risk | Low Risk | Low Risk |
| Opened a sequentially numbered opaque randomization envelope from the appropriate gestational age strata (23 weeks 0 days through 27 weeks six days or 28 weeks zero days through 31 weeks six days). Randomization was computer generated using permuted block sizes of two and four and was stratified by site | Opaque envelopes prior to delivery | All outcome assessments were performed by blinded team members | Were adjudicated by two independent pediatric radiologists or neuroradiologists who were not affiliated with any of the study sites and were blinded to randomization assignment | No missing data were identified for the primary outcome of incidence of death or severe intraventricular hemorrhage at 6 months’ corrected gestational age |
| Mortality | Hypot. Expanders | Hypot. Drugs | Respiratory distress syndrome | Necrotizing enterocolitis | Sepsis | Intraventricular hemorrhage | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control |
| 2008; Hosono | 2/20 | 3/20 | NR | NR | NR | NR | 14/20 | 13/20 | NR | NR | 2/20 | 1/20 | 3/20 | 5/20 |
| 2011; Rabe | 2/27 | 4/31 | NR | NR | NR | NR | NR | NR | 1/27 | 4/31 | 1/27 | 0/31 | 3/27 | 7/31 |
| 2013; March | 2/36 | 4/39 | NR | NR | 0/36 | 1/39 | 36/36 | 39/39 | 6/36 | 10/39 | 10/36 | 18/39 | 9/36 | 20/39 |
| 2014; Katheria | 2/30 | 1/30 | 11/30 | 12/30 | 10/30 | 10/30 | NR | NR | NR | NR | NR | NR | 8/30 | 11/30 |
| 2014; Alan | NR | NR | NR | NR | NR | NR | NR | NR | 2/19 | 1/19 | 16/19 | 16/19 | 3/19 | 0/19 |
| 2014; Josephen | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2015; Katheria | 2/75 | 6/79 | NR | NR | NR | NR | NR | NR | 1/75 | 0/79 | 5/75 | 3/79 | 5/75 | 10/79 |
| 2015; Krueger | 0/35 | 3/32 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 5/35 | 4/32 |
| 2015; Kumar | NR | NR | NR | NR | NR | NR | 10/100 | 5/100 | NR | NR | NR | NR | NR | NR |
| 2015; Kilicdag | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2017; Das | NR | NR | NR | NR | NR | NR | NR | NR | 1/107 | 1/90 | 7/107 | 8/90 | 6/107 | 3/90 |
| 2017; Song | 2/34 | 9/32 | NR | NR | 10/34 | 20/32 | NR | NR | 0/34 | 1/32 | 23/34 | 25/32 | NR | NR |
| 2017; Katheria | NR | NR | NR | NR | 8/70 | 12/65 | NR | NR | NR | NR | 4/70 | 1/65 | 9/70 | 6/65 |
| 2018; Lago | 0/69 | 0/69 | NR | NR | 3/69 | 1/69 | 16/69 | 8/69 | 2/69 | 1/69 | NR | NR | 4/69 | 4/69 |
| 2018; El-Naggar | 1/37 | 1/36 | 1/37 | 0/36 | 1/37 | 0/36 | NR | NR | 4/37 | 4/36 | NR | NR | 13/37 | 10/36 |
| 2019; Shirk | 5/100 | 4/104 | NR | NR | NR | NR | NR | NR | 3/100 | 6/104 | NR | NR | 10/100 | 16/104 |
| 2019;Katheria | 17/236 | 15/238 | NR | NR | NR | NR | NR | NR | 8/236 | 13/238 | 25/236 | 24/238 | 57/236 | 50/238 |
| Egger Bias (p-value) | 0.165 | NC | 0.299 | NC | 0.315 | 0.205 | 0.787 | |||||||
| I2 95% CI | 0% (0–52.7) | NC | 7.3% (0–63.8) | 39.6% (0–82.3) | 0% (0–52.7) | 0% (0–54.4) | 11.1% (0–54.1) | |||||||
| Cochran’s Q (p-value) | 0.482 | 0.475 | 0.370 | 0.191 | 0.920 | 0.615 | 0.334 | |||||||
| RR 95% CI | 0.71 (0.47–1.08) | 1 (0.53–1.88) | 0.70 (0.48–1.03) | 1.54 (1.03–2.29) | 0.71 (0.45–1.12) | 0.96 (0.77–1.19) | 0.93 (0.76–1.15) | |||||||
| Transfusion | Phototherapy | Oxygen at Birth | Oxygen at 28 Days | Patent Ductus Arteriosus | Retinopathy of Prematurity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control |
| 2008; Hosono | 7/20 | 14/20 | NR | NR | NR | NR | NR | NR | 5/20 | 7/20 | 8/20 | 17/20 |
| 2011; Rabe | 17/27 | 15/31 | NR | NR | NR | NR | 4/27 | 6/31 | NR | NR | 1/27 | 0/31 |
| 2013; March | 30/36 | 38/39 | 33/36 | 38/39 | NR | NR | NR | NR | NR | NR | 28/36 | 31/39 |
| 2014; Katheria | 11/30 | 22/30 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2014; Alan | 15/19 | 17/19 | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2014; Josephen | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2015; Katheria | 31/75 | 41/79 | NR | NR | 57/75 | 56/79 | 16/75 | 12/79 | NR | NR | 1/75 | 2/79 |
| 2015; Krueger | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 6/35 | 4/32 |
| 2015; Kumar | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2015; Kilicdag | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2017; Das | NR | NR | 104/107 | 89/90 | NR | NR | NR | NR | NR | NR | 8/107 | 3/90 |
| 2017; Song | NR | NR | NR | NR | 28/34 | 31/32 | NR | NR | NR | NR | 0/34 | 2/32 |
| 2017; Katheria | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2018; Lago | 4/69 | 5/69 | 41/69 | 25/69 | NR | NR | NR | NR | 14/69 | 7/69 | NR | NR |
| 2018; El-Naggar | NR | NR | 36/37 | 33/36 | 31/37 | 26/36 | NR | NR | 12/37 | 10/36 | 2/37 | 3/36 |
| 2019; Shirk | 9/100 | 16/104 | 85/100 | 88/104 | NR | NR | NR | NR | NR | NR | NR | NR |
| 2019; Katheria | NR | NR | NR | NR | NR | NR | NR | NR | 42/236 | 46/238 | 10/236 | 19/238 |
| Egger Bias (p-value) | 0.345 | 0.208 | NC | NC | 0.595 | 0.688 | ||||||
| I2 95% CI | 42.1% (0–72.9) | 81.9% (46.5–90.5) | 67.2% (0–88.4) | NC | 11.7% (0–71.5) | 35.2% (0–69.1) | ||||||
| Cochran’s Q (p-value) | 0.098 | <0.001 | 0.047 | 0.375 | 0.334 | 0.136 | ||||||
| RR 95% CI | 0.78 (0.67–0.90) | 1.03 (0.92–1.15)* | 1.01 (0.82–1.23)* | 1.20 (0.67–2.14) | 1.04 (0.78–1.40) | 0.80 (0.63–1.03) | ||||||
| Hemoglobin | Hematocrit | Mean Blood Pressure | Length of Hospital Stay | Cord Arterial pH | Peak Serum Bilirubin, Median | Apgar Scores 1 min | Apgar Scores 5 min | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control | Milking | Control |
| 2008; Hosono | 16.5 (1.4) | 14.1 (1.6) | NR | NR | 34.0 (9.0) | 28.0 (8.0) | NR | NR | NR | NR | 8.18 (2.57) | 7.83 (2.45) | 5.40 (2.0) | 4.20 (1.80) | 7.3 (1.7) | 6.9 (1.7) |
| 2011; Rabe | NR | NR | 52.0 (8.0) | 51.0 (7.0) | 35.0 (8.0) | 31.0 (6.0) | 105 (75.62) | 72.5 (45.76) | 7.2 (0.15) | 7.2 (0.09) | 10.17 (3.09) | 10.34 (1.81) | NR | NR | 7.0 (2.00) | 8.5 (0.97) |
| 2013; March | 15.43 (3.70) | 13.73 (1.84) | 45.6 (10.57) | 40.63 (5.31) | NR | NR | NR | NR | 7.3 (0.0) | 7.33 (0.07) | 5.16 (0.84) | 5.6 (1.46) | 3.5 (3.47) | 3.66 (2.30) | 6.16 (1.54) | 6.33 (1.53) |
| 2014; Katheria | NR | NR | 43.0 (7.0) | 46.0 (7.0) | 41.0 (9.0) | 36.0 (9.0) | NR | NR | NR | NR | 8.0 (2.0) | 7.0 (2.0) | NR | NR | NR | NR |
| 2014; Alan | 16.62 (1.23) | 15.4 (1.62) | NR | NR | NR | NR | 45.75 (14.4) | 51.5 (17.28) | NR | NR | NR | NR | 6.25 (1.30) | 6.0 (1.57) | 7.75 (0.78) | 7.5 (1.04) |
| 2014; Josephen | 13.9 (2.8) | 13.4 (1.8) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2015; Katheria | 16.3 (2.4) | 15.6 (2.2) | NR | NR | NR | NR | NR | NR | NR | NR | 8.1 (2.9) | 7.3 (2.2) | NR | NR | NR | NR |
| 2015; Krueger | NR | NR | 47.71 (4.7) | 47.75 (8.3) | NR | NR | 67.8 (29.0) | 71.2 (33.0) | NR | NR | 8.27 (2.6) | 8.38 (2.6) | NR | NR | NR | NR |
| 2015; Kumar | 16.7 (2.3) | 16 (2.7) | NR | NR | 50 (11.4) | 48 (10.2) | NR | NR | NR | NR | NR | NR | 6.90 (0.30) | 6.90 (0.30) | NR | NR |
| 2015; Kilicdag | 18.2 (2.3) | 17.6 (2.1) | 52.3 (6.1) | 51.3 (6.3) | NR | NR | NR | NR | NR | NR | NR | NR | 5.75 (1.23) | 5.25 (1.27) | 8.0 (0.49) | 7.5 (1.01) |
| 2017; Das | 15.0 (2.0) | 14.5 (3.0) | 47.0 (7.0) | 45.0 (8.0) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 9.0 (0.00) | 8.66 (0.75) |
| 2017; Song | 15.8 (1.6) | 14.7 (2.1) | NR | NR | 31.7 (6.2) | 29.6 (6.7) | 54.7 (19.3) | 51.5 (44.8) | 7.3 (0.9) | 7.3 (0.2) | NR | NR | 5.5 (2.7) | 5.1 (2.4) | 7.8 (1.8) | 7.5 (1.7) |
| 2017; Katheria | 16.35 (2.39) | 15.78 (1.94) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| 2018; Lago | 17.93 (2.96) | 16.23 (2.80) | 54.20 (9.27) | 48.83 (8.76) | NR | NR | NR | NR | NR | NR | 11.09 (3.21) | 11.24 (3.56) | NR | NR | NR | NR |
| 2018; El-Naggar | 16.1 (2.3) | 15.0 (2.4) | NR | NR | 33.0 (5.6) | 34.0 (5.2) | 75.66 (37.79) | 77.66 (38.6) | NR | NR | 9.76 (2.47) | 9.01 (1.89) | 4.66 (0.77) | 4.66 (3.86) | 7.00 (1.54) | 7.00 (1.54) |
| 2019; Shirk | 17.2 (2.1) | 16.8 (2.5) | 51.8 (6.2) | 49.9 (7.7) | NR | NR | NR | NR | 7.14 (0.77) | 7.23 (0.09) | 8.8 (2.2) | 8.8 (2.5) | 6.66 (2.25) | 6.66 (2.25) | 8.00 (1.50) | 8.33 (1.50) |
| 2019; Katheria | 16.5 (3.1) | 16.4 (2.7) | 48.6 (8.2) | 48.6 (7.9) | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Egger Bias (p value) | 0.037 | 0.526 | 0.007 | 0.039 | 0.969 | 0.313 | 0.1 | 0.177 | ||||||||
| I2 95% CI | 53% (0–73) | 61.2% (0–79.5) | 52.9% (0–79.3) | 24.1% (0–72.1) | 0% (0–67.9) | 35% (0–69) | 0 (0–56.3) | 72.1 (33.9–84.2) | ||||||||
| Cochran’s Q (p-value) | 0.01 | 0.008 | 0.059 | 0.260 | 0.705 | 0.138 | 0.455 | 0.001 | ||||||||
| PWMD CI 95% | 0.89 (0.55 to 1.22) b | 1.43 (–0.03 to 2.89) a | 1.92 (0.55 to 3.25) | –1.92 (–8.44 to 4.60) a | –0.03 (–0.05 to–0.01) a | 0.11 (–0.18 to 0.40) a | 0.02 (–0.06 to 0.1) a | 0.02 (–0.31 to 0.35) b | ||||||||
References
- Katheria, A.C.; Lakshminrusimha, S.; Rabe, H.; McAdams, R.; Mercer, J.S. Placental transfusion: A review. J. Perinatol. 2017, 37, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Brune, T.; Garritsen, H.; Witteler, R.; Schlake, A.; Wüllenweber, J.; Louwen, F.; Jorch, G.; Harms, E. Autologous placental blood transfusion for the therapy of anaemic neonates. Neonatology 2002, 81, 236–243. [Google Scholar] [CrossRef]
- Farrar, D.; Airey, R.; Law, G.R.; Tuffnell, D.; Cattle, B.; Duley, L. Measuring placental transfusion for term births: Weighing babies with cord intact. BJOG 2011, 118, 70–75. [Google Scholar] [CrossRef]
- Aladangady, N.; McHugh, S.; Aitchison, T.C.; Wardrop, C.A.J.; Holland, B.M. Infants’ blood volume in a controlled trial of placental transfusion at preterm delivery. Pediatrics 2006, 117, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Hutton, E.K.; Hassan, E.S. Late vs. early clamping of the umbilical cord in full-term neonates: Systematic review and meta-analysis of controlled trials. JAMA 2007, 297, 1241–1252. [Google Scholar] [CrossRef] [PubMed]
- Rabe, H.; Reynolds, G.J.; Diaz-Rosello, J.L. Early versus delayed umbilical cord clamping in preterm infants. In Cochrane Database of Systematic Reviews; Rabe, H., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2004; No. CD003248. [Google Scholar]
- Fogarty, M.; Osborn, D.A.; Askie, L.; Seidler, A.L.; Hunter, K.; Lui, K.; Simes, J.; Tarnow-Mordi, W. Delayed vs. early umbilical cord clamping for preterm infants: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2018, 218, 1–18. [Google Scholar] [CrossRef]
- Grupo de trabajo de la Guía de Práctica Clínica sobre Atención al Parto Normal. Guía de Práctica Clínica sobre la Atención al Parto Normal. In Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad y Política Social; Agencia de Evaluació: Madrid, Spain, 2010. [Google Scholar]
- National Institute for Health and Care Excellence. Intrapartum Care for Healthy Women and Babies; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- WHO Recommendations on Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018.
- American College of Nurse Midwives. Delayed Umbilical Cord Clamping. Position Stawtement; ACNM: Silver Spring, MD, USA, 2014. [Google Scholar]
- Committee on Obstetric Practice. Committee opinion No. 684: Delayed umbilical cord clamping after birth. Obstet. Gynecol. 2017, 129, e5–e10. [Google Scholar] [CrossRef]
- Al-Wassia, H.; Shah, P.S. Efficacy and safety of umbilical cord milking at birth: A systematic review and meta-analysis. JAMA Pediatr. 2015, 169, 18–25. [Google Scholar] [CrossRef]
- Katheria, A.C. Umbilical Cord Milking: A Review. Front. Pediatr. 2018, 6, 335. [Google Scholar] [CrossRef] [Green Version]
- Nagano, N.; Saito, M.; Sugiura, T.; Miyahara, F.; Namba, F.; Ota, E. Benefits of umbilical cord milking versus delayed cord clamping on neonatal outcomes in preterm infants: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0201528. [Google Scholar] [CrossRef] [Green Version]
- Josephsen, J.; Vlastos, E.; Potter, S.; Al-Hosni, M. Milking the umbilical cord in extreme preterm infants. Am. J. Obstet. Gynecol. 2014. [Google Scholar] [CrossRef]
- Krueger, M.S.; Eyal, F.G.; Peevy, K.J.; Hamm, C.R.; Whitehurst, R.M.; Lewis, D.F. Delayed cord clamping with and without cord stripping: A prospective randomized trial of preterm neonates. Am. J. Obstet. Gynecol. 2015, 212, 394.e1–394.e5. [Google Scholar] [CrossRef]
- Kumar, B.; Upadhyay, A.; Gothwal, S.; Jaiswal, V.; Joshi, P.; Dubey, K. Umbilical cord milking and hematological parameters in moderate to late preterm neonates: A randomized controlled trial. Indian Pediatr. 2015, 52, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Kilicdag, H.; Gulcan, H.; Hanta, D.; Torer, B.; Gokmen, Z.; Ozdemir, S.I.; Antmen, B.A. Is umbilical cord milking always an advantage? J. Matern. Neonatal Med. 2016, 29, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Das, B.; Sundaram, V.; Kumar, P.; Mordi, W.T.; Dhaliwal, L.K.; Das, R. Effect of placental transfusion on iron stores in moderately preterm neonates of 30–33 weeks gestation. Indian J. Pediatr. 2018, 85, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Song, S.-Y.; Kim, Y.; Kang, B.-H.; Yoo, H.-J.; Lee, M. Safety of umbilical cord milking in very preterm neonates: A randomized controlled study. Obstet. Gynecol. Sci. 2017, 60, 527. [Google Scholar] [CrossRef]
- Katheria, A.; Garey, D.; Truong, G.; Akshoomoff, N.; Steen, J.; Maldonado, M.; Poeltler, D.; Harbert, M.J.; Vaucher, Y.E.; Finer, N. A randomized clinical trial of umbilical cord milking vs. delayed cord clamping in preterm infants: Neurodevelopmental outcomes at 22–26 months of corrected age. J. Pediatr. 2018, 194, 76–80. [Google Scholar] [CrossRef]
- Lago Leal, V.; Pamplona Bueno, L.; Cabanillas Vilaplana, L.; Nicolás Montero, E.; Martín Blanco, M.; Fernández Romero, C.; El Bakkali, S.; Pradillo Aramendi, T.; Sobrino Lorenzano, L.; Castellano Esparza, P.; et al. Effect of milking maneuver in preterm infants: A randomized controlled trial. Fetal Diagn. Ther. 2019, 45, 57–61. [Google Scholar] [CrossRef]
- El-Naggar, W.; Simpson, D.; Hussain, A.; Armson, A.; Dodds, L.; Warren, A.; Whyte, R.; McMillan, D. Cord milking versus immediate clamping in preterm infants: Arandomised controlled trial. Arch. Dis. Child.Fetal Neonatal Ed. 2019, 104, F145–F150. [Google Scholar] [CrossRef]
- Shirk, S.K.; Manolis, S.A.; Lambers, D.S.; Smith, K.L. Delayed clamping vs. milking of umbilical cord in preterm infants: A randomized controlled trial. Am. J. Obstet. Gynecol. 2019, 220, e1–e482. [Google Scholar] [CrossRef]
- Katheria, A.; Reister, F.; Essers, J.; Mendler, M.; Hummler, H.; Subramaniam, A.; Carlo, W.; Tita, A.; Truong, G.; Davis-Nelson, S.; et al. Association of umbilical cord milking vs. delayed umbilical cord clamping with death or severe intraventricular hemorrhage among preterm infants. JAMA 2019, 322, 1877. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Green, S. (Eds.) Chapter 7: Selecting studies and collecting data. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; (Updated March 2011); The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Hosono, S.; Mugishima, H.; Fujita, H.; Hosono, A.; Minato, M.; Okada, T.; Takahashi, S.; Harada, K. Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks’ gestation: Arandomised controlled trial. Arch. Dis. Child. Fetal Neonatal Ed. 2008, 93, F14–F19. [Google Scholar] [CrossRef]
- Rabe, H.; Jewison, A.; Fernandez Alvarez, R.; Crook, D.; Stilton, D.; Bradley, R.; Holden, D. Brighton perinatal study group milking compared with delayed cord clamping to increase placental transfusion in preterm neonates. Obstet. Gynecol. 2011, 117, 205–211. [Google Scholar] [CrossRef]
- March, M.I.; Hacker, M.R.; Parson, A.W.; Modest, A.M.; de Veciana, M. The effects of umbilical cord milking in extremely preterm infants: A randomized controlled trial. J. Perinatol. 2013, 33, 763–767. [Google Scholar] [CrossRef]
- Katheria, A.C.; Leone, T.A.; Woelkers, D.; Garey, D.M.; Rich, W.; Finer, N.N. The effects of umbilical cord milking on hemodynamics and neonatal outcomes in premature neonates. J. Pediatr. 2014, 164, 1045–1050. [Google Scholar] [CrossRef]
- Katheria, A.C.; Truong, G.; Cousins, L.; Oshiro, B.; Finer, N.N. Umbilical cord milking versus delayed cord clamping in preterm infants. Pediatrics 2015, 136, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Alan, S.; Arsan, S.; Okulu, E.; Akin, I.M.; Kilic, A.; Taskin, S.; Cetinkaya, E.; Erdeve, O.; Atasay, B. Effects of umbilical cord milking on the need for packed red blood cell transfusions and early neonatal hemodynamic adaptation in preterm infants born ≤1500 g: A prospective, randomized, controlled trial. J. Pediatr. Hematol. Oncol. 2014, 36, e493–e498. [Google Scholar] [CrossRef]
- Linderkamp, O. Placental transfusion: Determinants and effects. Clin. Perinatol. 1982, 9, 559–592. [Google Scholar] [CrossRef]
- Bell, E.F.; Strauss, R.G.; Widness, J.A.; Mahoney, L.T.; Mock, D.M.; Seward, V.J.; Cress, G.A.; Johnson, K.J.; Kromer, I.J.; Zimmerman, M.B. Randomized trial of liberal versus restrictive guidelines for red blood cell transfusion in preterm infants. Pediatrics 2005, 115, 1685–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dang, D.; Zhang, C.; Shi, S.; Mu, X.; Lv, X.; Wu, H. Umbilical cord milking reduces need for red cell transfusions and improves neonatal adaptation in preterm infants: Meta-analysis. J. Obstet. Gynaecol. Res. 2015, 41, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Blank, D.A.; Polglase, G.R.; Kluckow, M.; Gill, A.W.; Crossley, K.J.; Moxham, A.; Rodgers, K.; Zahra, V.; Inocencio, I.; Stenning, F.; et al. Haemodynamic effects of umbilical cord milking in premature sheep during the neonatal transition. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F539–F546. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Author | Year | N | Country | Gestational Age | UCM No. of Times | UCM Speed | Control Condition | Exclusion Criteria |
|---|---|---|---|---|---|---|---|---|
| Hosono et al. | 2008 | 40 | Tokyo (Japan) | 24–28 wk | 2–3 | 20 cm within 2s | ICC | Multiple births, major congenital anomalies, or chromosomal anomalies and hydrops fetalis. |
| Rabe et al. | 2011 | 58 | Brighton (United Kingdom) | 24 0/7–326/7wk | 4 | 20 cm within 2s | ICC | Multiple births, inadequate time to obtain consent before delivery, known congenital abnormalities of the fetus, rhesus sensitization, or fetal hydrops. |
| March et al. | 2013 | 75 | Virginia (USA) | 24–28 wk | 3 | – | ICC | Antenatally diagnosed major fetal congenital anomaly, known Factor Rh sensitization, hydrops fetalis, known recent maternal exposure to parvovirus, elevated peak systolic velocity of the fetal middle cerebral artery, or clinical suspicion of placental abruption at delivery due to excessive maternal bleeding or uterine hypertonicity. |
| Katheria et al. | 2014 | 60 | San Diego (USA) | 230/7–316/7wk | 2 | 20 cm within 2s | ICC | Monochorionic multiples, incarcerated mothers, placenta previa, concern for abruptions, or refusal to perform the intervention by the obstetrician. |
| Alan et al. | 2014 | 44 | Ankara (Turkey) | <32 wk | 3 | 5 cm within 1s | ICC | Suspected twin to twin transfusion syndrome or discordant twins, major congenital anomalies or chromosomal anomalies, vaginal bleeding due to placenta previa or abruption or placental tear, hemolytic disease of the fetus and newborn such as rhesus sensitization, intrauterine growth restriction, maternal gestational diabetes treated with insulin, hydrops fetalis; and refused parental consent. |
| Josephen et al. | 2014 | 26 | – | 24–266/7wk | 3 | – | ICC | Multiple gestation, congenital abnormalities, hydrops fetalis, and known fetal anemia. |
| Krueger et al. | 2015 | 67 | South Alabama (USA) | 22–316/7wk | 4 | – | DCC | The fetus had known anomalies or there was a suspected placental abruption. |
| Kumar et al. | 2015 | 200 | Northern India | 320/7–366/7wk | 3 | 10 cm within 1s | ICC | Umbilical cord length less than 25 cm, or were non-vigorous at birth, multiple births (twins, triplets), those born to Rh negative or retrovirus positive mothers, hydrops fetalis and those with major congenital anomalies, cord prolapse or cord anomalies like true knots were also excluded. Babies born to mothers with complications such as placental abruption, placental implantation disorders (placenta previa or accreta), or chorioamnionitis were excluded only if they were born limp. |
| Kilicdag et al. | 2015 | 54 | Istanbul (Turkey) | ≤32 wk | 4 | 20 cm within 2s | ICC | Congenital anomalies, placenta abruption, intrauterine growth restriction, twin–twin transfusion syndrome, discordant twin growth, vaginal delivery, and Rh hemolytic disease. |
| Katheria et al. | 2015 | 154 |
San Diego (USA) | 230/7–316/7wk | 4 | 20 cm within 2s | DCC | Monochorionic multiples, incarcerated mothers, placenta previa, concern for abruptions, Rh sensitization, hydrops, congenital anomalies, or the obstetrician declining to perform the intervention. |
| Daset al | 2017 | 215 | Northern India | 30–33 wk | 2 | – | ICC | Pregnant women with multiple pregnancies, suspected or proven major congenital malformation in the fetus, and antenatally diagnosed hydrops fetalis. |
| Song et al. | 2017 | 66 | Chungnam (South Korea) | 240/7–326/7wk | 4 | 20 cm within 2s | ICC | Multiple gestations, rhesus sensitization, fetal hydrops, or major fetal anomalies, and women without antenatal written consent. |
| Katheria et al. | 2017 | 135 | San Diego (USA) | 230/7–316/7wk | 3 | – | DCC | Monochorionic multiples, incarcerated mothers, placenta previa, concern for placental abruption, Rh sensitization, hydrops, and congenital anomalies. |
| Lago et al. | 2018 | 138 | – | 240–366wk | 4 | – | ICC | Umbilical cord abnormalities (true and false knots, short cord, nuchal cords), major congenital anomalies or chromosomal anomalies, hydrops fetalis twin–twin transfusion syndrome, clinical suspicion or diagnosis of placental abruption, and infants whose parents refused to consent. |
| El-Naggar et al. | 2018 | 73 | Halifax (Canada) | 24–31 wk | 3 | 10 cm within 1s | ICC | Monochorionic twins, major congenital anomalies, placental abruption, fetal anemia, and intention to withhold resuscitation. |
| Shirk et al. | 2019 | 204 | Cincinnati (USA) | 230–346wk | 4 | – | DCC | Congenital anomalies that had been identified on prenatal sonography (not including trisomy markers), those with precipitous delivery that prevented completion of the protocol, placental abruption at the time of/or as the indication for delivery, uterine rupture, infants known to be at risk of anemia (i.e., parvovirus B19 infection and allo/isoimmunization), or patient delivered at outside institution after random assignment. |
| Katheriaet al. | 2019 | 474 | 9 participating sites (6 in the United States and 1 site in Ireland, Germany, and Canada) | <32wk | 3 | 20 cm within 2s | DCC | Major congenital anomalies, severe placental abruption, transplacental incision, umbilical cord prolapse, hydrops, bleeding accreta, monochorionic multiple births, fetal or maternal risk for severe compromise at delivery, and family unlikely to return for 24month neurodevelopmental testing. |
| Outcome | Gestational Age | No of Studies | No of Participants | RR (95% CI)b | PWMD (95% CI)b | I 2 Value, % | Cochran’s Q | Egger Bias |
|---|---|---|---|---|---|---|---|---|
| Mortality | <37 weeks | 11 | 1.409 | 0.71 (0.47–1.08) | 0% (0–52.7) | 0.482 | 0.165 | |
| <33 weeks | 9 | 1.067 | 0.66 (0.43–1.03) | 0% (0–54.4) | 0.455 | 0.166 | ||
| ≥33 weeks | NC | NC | NC | NC | NC | NC | ||
| ICC control | 7 | 510 | 0.51 (0.26–1.06) | 0% (0–61) | 0.687 | 0.073 | ||
| DCCcontrol | 4 | 899 | 0.87 (0.52–1.47) | 23.3% (0–74.8) | 0.271 | 0.177 | ||
| Transfusion | <37 weeks | 8 | 767 | 0.78 (0.67–0.90) | 42.1% (0–72.9) | 0.098 | 0.345 | |
| <33 weeks | 6 | 425 | 0.80 (0.69–0.92) * | 53% (0–79.3) | 0.059 | 0.483 | ||
| ≥33 weeks | 2 | 342 | 0.64 (0.33–1.23) | NC | 0.680 | NC | ||
| ICC control | 6 | 409 | 0.80(0.68–0.94) | 53% (0–79.3) | 0.059 | 0.567 | ||
| DCC control | 2 | 358 | –0.08 (–0.16–0.00) | NC | 0.621 | NC | ||
| Hemoglobin | <37 weeks | 14 | 1.830 | 0.89 (0.55 to 1.22) * | 53% (0–73) | 0.01 | 0.037 | |
| <33 weeks | 11 | 1.288 | 0.91 (0.50 to 1.32) * | 56% (0–76) | 0.012 | 0.104 | ||
| ≥33 weeks | 3 | 542 | 0.85 (0.17 to 1.53) * | 59.6% (0–86.6) | 0.084 | NC | ||
| ICC control | 10 | 863 | 1.14 (0.83 to 1.44) | 36.4% (0–68.5) | 0.117 | 0.716 | ||
| DCC control | 4 | 967 | 0.38 (0.06 to 0.70) | 0% (0–67.9) | 0.549 | 0.011 | ||
| Phototherapy | <37 weeks | 5 | 687 | 1.03 (0.92–1.15)* | 81.9% (46.5–90.5) | 0.001 | 0.208 | |
| <33 weeks | 3 | 345 | 0.99 (0.95–1.02) | 17.1% (0–77.2) | 0.299 | NC | ||
| ≥33 weeks | 2 | 342 | 1.15 (1.00–1.31) | NC | 0.033 | NC | ||
| ICC control | 4 | 483 | 1.06 (0.89–1.26)* | 90.2% (76–94.5) | <0.001 | 0.294 | ||
| DCC control | 1 | 204 | 1.00 (0.89–1.12) | NC | NC | NC | ||
| Hematocrit | <37 weeks <33 weeks >33 weeks ICC control DCC control | 9 7 2 6 3 | 804 700 342 533 745 | 1.43 (–0.03 to 2.89)* 0.57 (–0.41 to 1.55) 2.90 (1.28 to 4.52) 1.93 (–0.41 to 4.28) * 0.61 (–0.48 to 1.70) | 61.2% (0–79.5) 46.1% (0–75.6) NC 67.5% (0–84.3) 22.3% (0–78.4) | 0.008 0.084 0.057 0.009 0.276 | 0.526 0.616 NC 0.732 NC | |
| Respiratory distress syndrome | <37 weeks <33 weeks >33 weeks ICC control DCC control | 4 NC 2 NC NC | 453NC338NCNC | 1.54 (1.03–2.29) NC 2 (1.07–3.73) NC NC | 39.6% (0–82.3) NC NC NC NC | 0.191 NC >0.999 NC NC | NC NC NC NC NC | |
| Intraventricular hemorrhage | <37 weeks<33 weeks >33 weeks ICC control DCC control | 13 11 2 8 5 | 1.713 1.233 342 345 518 | 0.93 (0.76–1.15) 0.97 (0.77–1.20) 0.72 (0.38–1.38) 0.83 (0.6–1.16) 1 (0.77–1.31) | 11.1% (0–54.1) 20.3% (0–60.5) NC 15.8% (0–62.8) 0% (0–64.1) | 0.334 0.25 0.58 0.305 0.413 | 0.787 0.814 NC 0.271 0.447 | |
| Peak serum bilirubin | <37 weeks | 9 | 869 | 0.11 (–0.18 to0.40) | 35% (0–69) | 0.138 | 0.313 | |
| Mean blood pressure | <37 weeks | 6 | 497 | 1.92 (0.55 to 3.25) | 52.9% (0–79.3) | 0.059 | 0.007 | |
| Length of hospital stay | <37 weeks | 5 | 308 | –1.92 (–8.44 to 4.60) | 24.1% (0–72.1) | 0.260 | 0.039 | |
| Cord arterial pH | <37 weeks | 4 | 380 | –0.03 (–0.05 to 0.01) | 0% (0–67.9) | 0.705 | 0.969 | |
| Apgar scores 1 min | <37 weeks | 8 | 756 | 0.02 (–0.06 to 0.10) | 0.0% (0–56.3) | 0.455 | 0.1 | |
| Apgar scores 5 min | <37 weeks | 9 | 766 | 0.02 (–0.31 to 0.35)* | 72.1% (33.9–84.2) | 0.001 | 0.177 | |
| Oxygen at birth | <37 weeks | 3 | 293 | 1.01 (0.82–1.23)* | 67.2% (0–88.4) | 0.047 | NC | |
| Oxygen at 28 days | <37 weeks | 2 | 212 | 1.20 (0.67–2.14) | NC | 0.375 | NC | |
| Retinopathy of prematurity | <37 weeks | 9 | 1.204 | 0.80 (0.63–1.03) | 35.2% (0–69.1) | 0.136 | 0.688 | |
| Hypotensive expanders | <37 weeks | 2 | 133 | 1.00 (0.53–1.88) | NC | 0.475 | NC | |
| Hypotensive drugs | <37 weeks | 6 | 547 | 0.70 (0.48–1.03) | 7.3% (0–63.8) | 0.370 | 0.299 | |
| Necrotizing enterocolitis | <37 weeks | 10 | 1.477 | 0.71 (0.45–1.12) | 0% (0–52.7) | 0.920 | 0.315 | |
| Patent ductus arteriosus | <37 weeks | 4 | 725 | 1.04 (0.78–1.40) | 11.7% (0–71.5) | 0.334 | 0.595 | |
| Sepsis | <37 weeks | 9 | 1.237 | 0.96 (0.77–1.19) | 0% (0–54.4) | 0.615 | 0.205 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Esquinas, I.; Gómez-Salgado, J.; Rodriguez-Almagro, J.; Arias-Arias, Á.; Ballesta-Castillejos, A.; Hernández-Martínez, A. Umbilical Cord Milking in Infants Born at <37 Weeks of Gestation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1071. https://doi.org/10.3390/jcm9041071
Ortiz-Esquinas I, Gómez-Salgado J, Rodriguez-Almagro J, Arias-Arias Á, Ballesta-Castillejos A, Hernández-Martínez A. Umbilical Cord Milking in Infants Born at <37 Weeks of Gestation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(4):1071. https://doi.org/10.3390/jcm9041071
Chicago/Turabian StyleOrtiz-Esquinas, Inmaculada, Juan Gómez-Salgado, Julián Rodriguez-Almagro, Ángel Arias-Arias, Ana Ballesta-Castillejos, and Antonio Hernández-Martínez. 2020. "Umbilical Cord Milking in Infants Born at <37 Weeks of Gestation: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 4: 1071. https://doi.org/10.3390/jcm9041071