Pulsed Electromagnetic Field Therapy Improves Osseous Consolidation after High Tibial Osteotomy in Elderly Patients—A Randomized, Placebo-Controlled, Double-Blind Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Registration
2.2. Ethics Statement
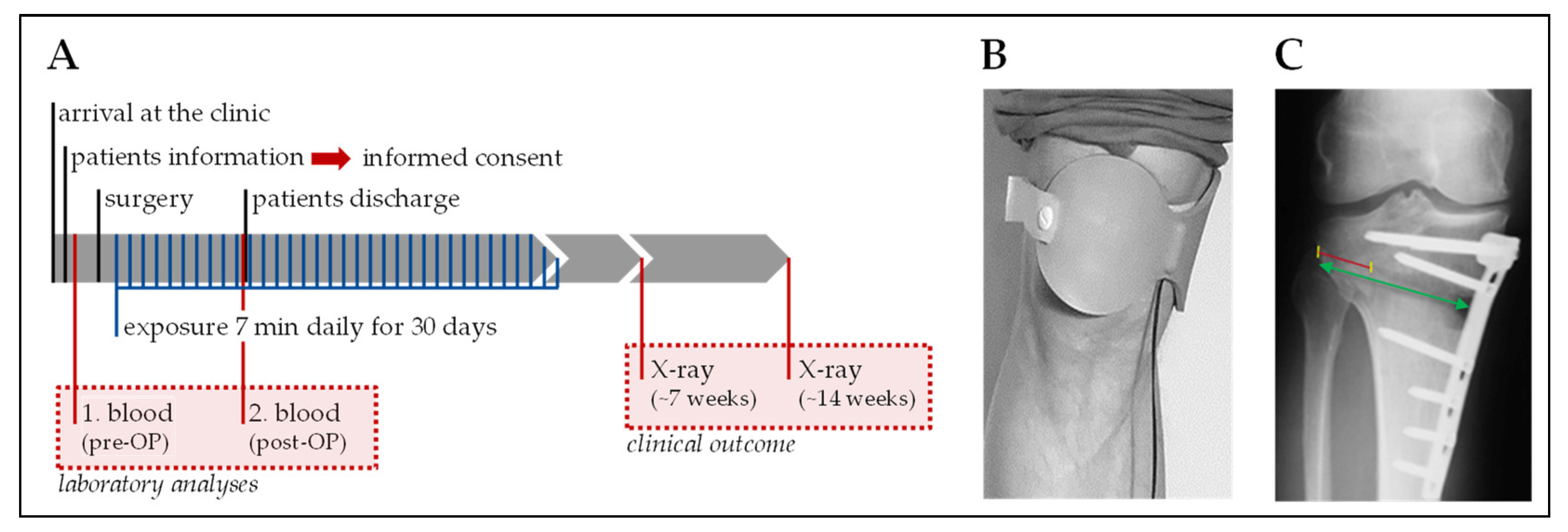
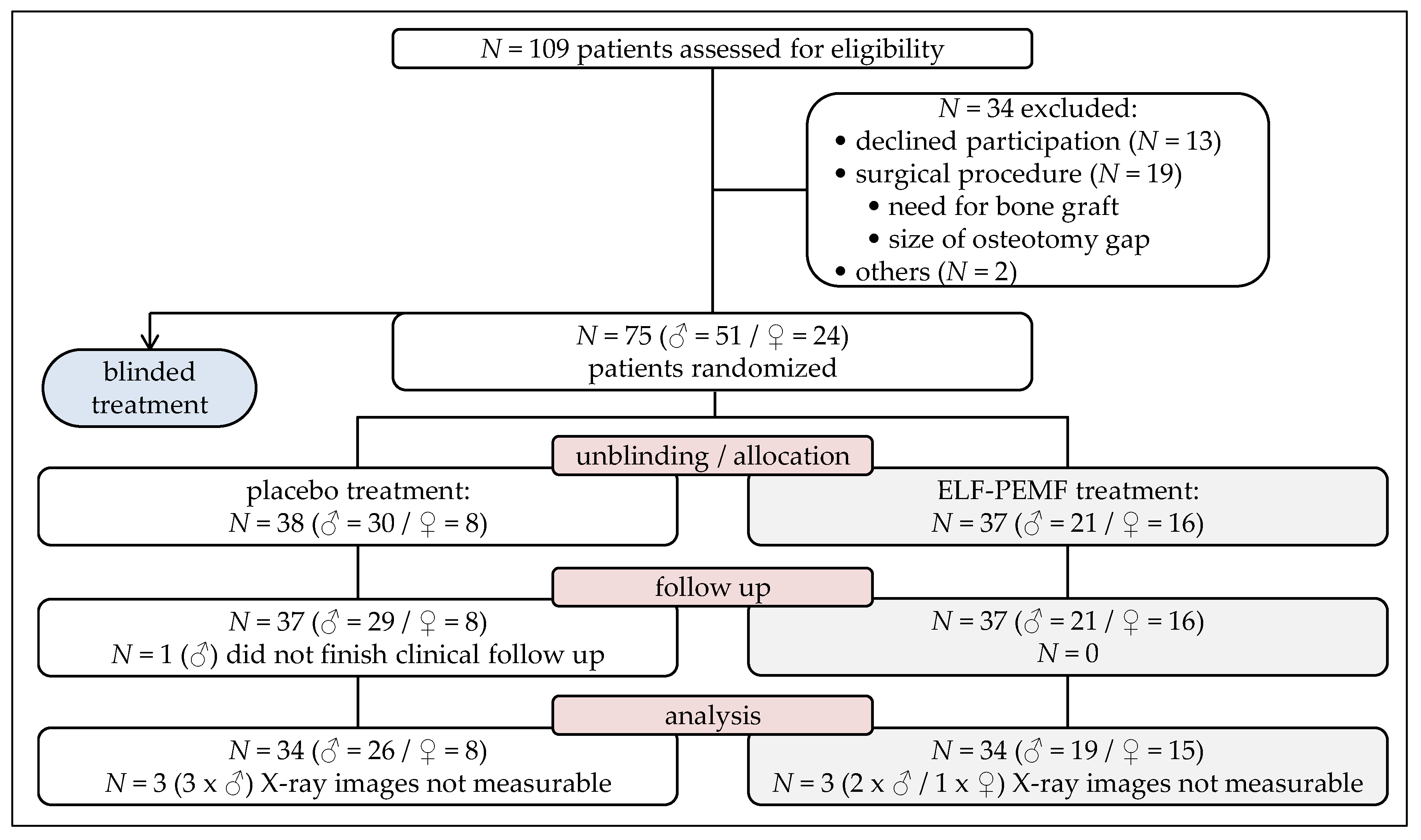
2.3. Study Population and Procedure
2.4. Generation of ELF-PEMF
2.5. Randomization and Unblinding
2.6. Surgery and Post-Surgical Treatment
2.7. Osseous Consolidation
2.8. Blood Parameters
2.9. Statistics
3. Results
3.1. Excellent Acceptance and Compliance of the Treatment
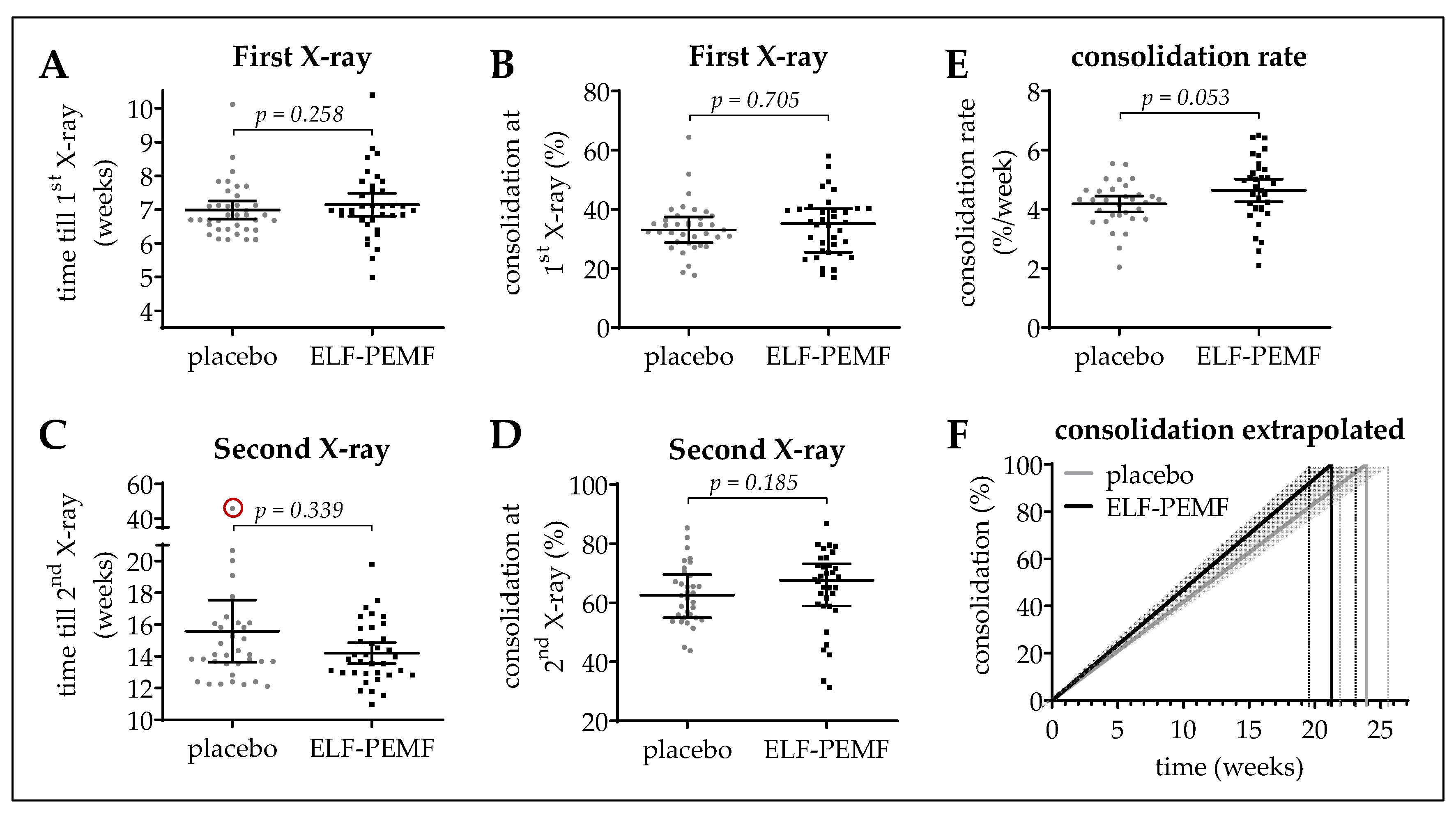
3.2. Osseous Consolidation in the ELF-PEMF and the Placebo Group
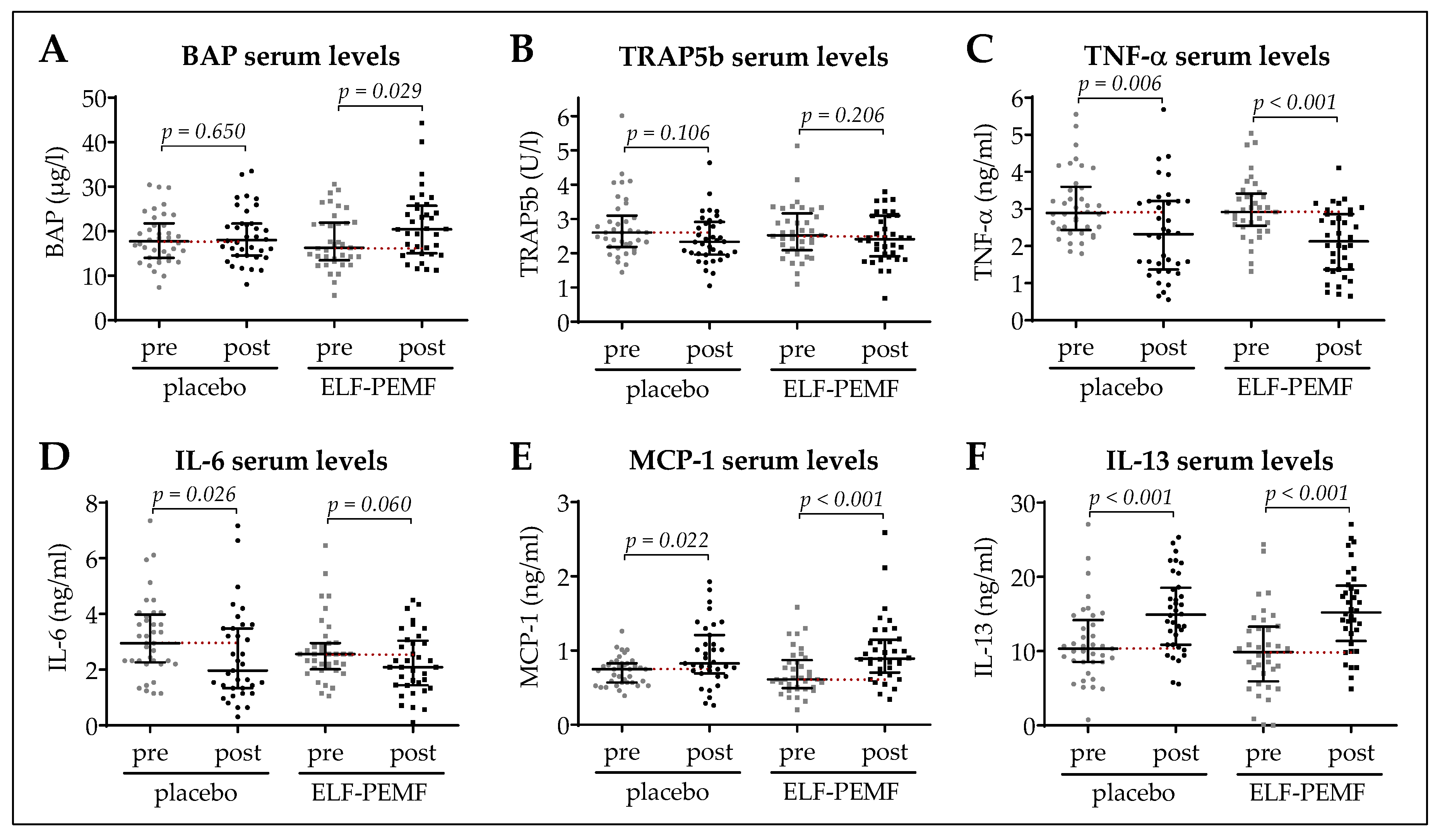
3.3. Early Increase in BAP Serum Levels in the ELF-PEMF Group
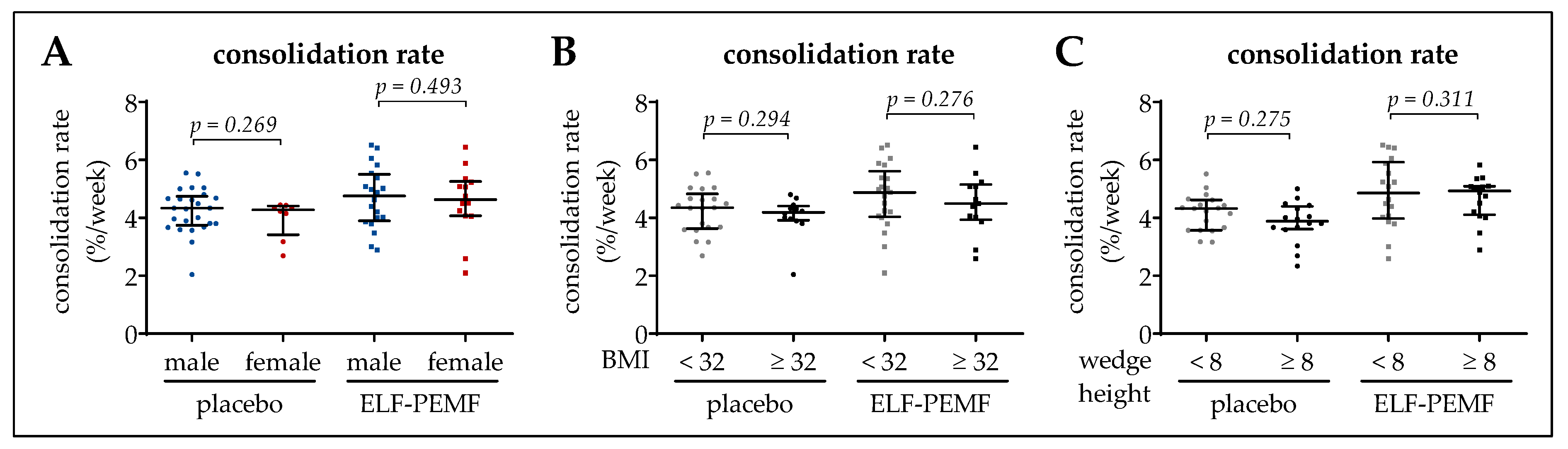
3.4. Osseous Consolidation Was Independent of Sex, BMI, or Wedge Height
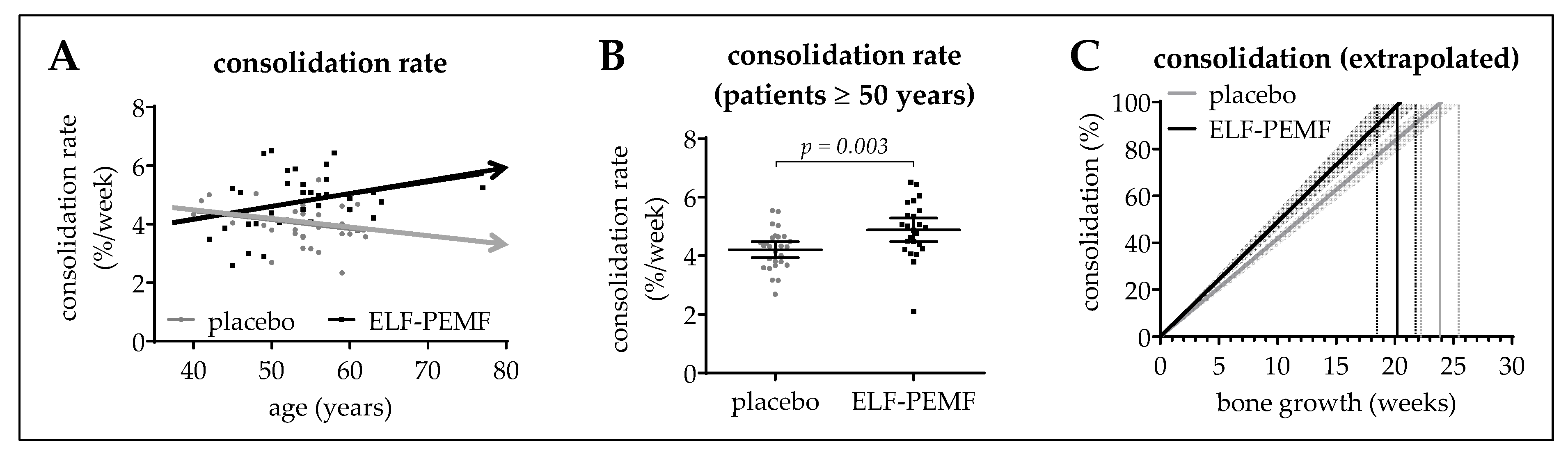
3.5. ELF-PEMF Treatment Improved Osseous Consolidation in Elderly Patients
4. Discussion
5. Summary and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BAP | bone specific alkaline phosphatase |
| BMI | body mass index |
| ELF-PEMF | extremely low frequency pulsed electromagnetic field |
| ELISA | enzyme-linked immunosorbent assay |
| HTO | high tibial osteotomy |
| IL-13 | interleukin 13 |
| IL-6 | interleukin 6 |
| MCP-1 | monocyte chemoattractant protein 1 |
| NRS | nutritional risk screening 2002 |
| TNF-α | tumor necrosis factor alpha |
| TRAP5b | tartrate resistant acidic phosphatase |
References
- Ziegler, P.; Friederichs, J.; Hungerer, S. Fusion of the subtalar joint for post-traumatic arthrosis: A study of functional outcomes and non-unions. Int. Orthop. 2017, 41, 1387–1393. [Google Scholar] [CrossRef]
- Scolaro, J.A.; Schenker, M.L.; Yannascoli, S.; Baldwin, K.; Mehta, S.; Ahn, J. Cigarette smoking increases complications following fracture: A systematic review. J. Bone Jt. Surg. Am. 2014, 96, 674–681. [Google Scholar] [CrossRef]
- Massari, L.; Benazzo, F.; Falez, F.; Cadossi, R.; Perugia, D.; Pietrogrande, L.; Aloj, D.C.; Capone, A.; D’Arienzo, M.; Cadossi, M.; et al. Can clinical and surgical parameters be combined to predict how long it will take a tibia fracture to heal? A prospective multicentre observational study: The fracting study. Biomed. Res. Int. 2018, 2018, 1809091. [Google Scholar] [CrossRef]
- Massari, L.; Falez, F.; Lorusso, V.; Zanon, G.; Ciolli, L.; La Cava, F.; Cadossi, M.; Chiarello, E.; De Terlizzi, F.; Setti, S.; et al. Can a combination of different risk factors be correlated with leg fracture healing time? J. Orthop. Traumatol. 2013, 14, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Taormina, D.P.; Shulman, B.S.; Karia, R.; Spitzer, A.B.; Konda, S.R.; Egol, K.A. Older age does not affect healing time and functional outcomes after fracture nonunion surgery. Geriatr. Orthop. Surg. Rehabil. 2014, 5, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Bassett, C.A.; Becker, R.O. Generation of electric potentials by bone in response to mechanical stress. Science 1962, 137, 1063–1064. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.F.; Xiong, J.; Chen, Y.X.; Wang, J.F.; Qiu, X.S.; Wang, Y.H.; Qiu, Y. Early application of pulsed electromagnetic field in the treatment of postoperative delayed union of long-bone fractures: A prospective randomized controlled study. BMC Musculoskelet. Disord. 2013, 14, 35. [Google Scholar] [CrossRef]
- Borsalino, G.; Bagnacani, M.; Bettati, E.; Fornaciari, F.; Rocchi, R.; Uluhogian, S.; Ceccherelli, G.; Cadossi, R.; Traina, G.C. Electrical stimulation of human femoral intertrochanteric osteotomies. Double-blind study. Clin. Orthop. Relat. Res. 1988, 237, 256–263. [Google Scholar]
- Hannemann, P.F.; van Wezenbeek, M.R.; Kolkman, K.A.; Twiss, E.L.; Berghmans, C.H.; Dirven, P.A.; Brink, P.R.; Poeze, M. Ct scan-evaluated outcome of pulsed electromagnetic fields in the treatment of acute scaphoid fractures: A randomised, multicentre, double-blind, placebo-controlled trial. Bone Jt. J. 2014, 96, 1070–1076. [Google Scholar] [CrossRef]
- Zorzi, C.; Dall’Oca, C.; Cadossi, R.; Setti, S. Effects of pulsed electromagnetic fields on patients’ recovery after arthroscopic surgery: Prospective, randomized and double-blind study. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 830–834. [Google Scholar] [CrossRef]
- Cadossi, M.; Buda, R.E.; Ramponi, L.; Sambri, A.; Natali, S.; Giannini, S. Bone marrow-derived cells and biophysical stimulation for talar osteochondral lesions: A randomized controlled study. Foot Ankle Int. 2014, 35, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Collarile, M.; Sambri, A.; Lullini, G.; Cadossi, M.; Zorzi, C. Biophysical stimulation improves clinical results of matrix-assisted autologous chondrocyte implantation in the treatment of chondral lesions of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Catalano, A.; Loddo, S.; Bellone, F.; Pecora, C.; Lasco, A.; Morabito, N. Pulsed electromagnetic fields modulate bone metabolism via rankl/opg and wnt/beta-catenin pathways in women with postmenopausal osteoporosis: A pilot study. Bone 2018, 116, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Tabrah, F.; Hoffmeier, M.; Gilbert, F., Jr.; Batkin, S.; Bassett, C.A. Bone density changes in osteoporosis-prone women exposed to pulsed electromagnetic fields (PEMFs). J. Bone Miner. Res. 1990, 5, 437–442. [Google Scholar] [CrossRef]
- Aaron, R.K.; Ciombor, D.M.; Simon, B.J. Treatment of nonunions with electric and electromagnetic fields. Clin. Orthop. Relat. Res. 2004, 21–29. [Google Scholar] [CrossRef]
- Ciombor, D.M.; Aaron, R.K. The role of electrical stimulation in bone repair. Foot Ankle Clin. 2005, 10, 579–593. [Google Scholar] [CrossRef]
- Reilingh, M.L.; van Bergen, C.J.; Gerards, R.M.; van Eekeren, I.C.; de Haan, R.J.; Sierevelt, I.N.; Kerkhoffs, G.M.; Krips, R.; Meuffels, D.E.; van Dijk, C.N.; et al. Effects of pulsed electromagnetic fields on return to sports after arthroscopic debridement and microfracture of osteochondral talar defects: A randomized, double-blind, placebo-controlled, multicenter trial. Am. J. Sports Med. 2016, 44, 1292–1300. [Google Scholar] [CrossRef]
- Mammi, G.I.; Rocchi, R.; Cadossi, R.; Massari, L.; Traina, G.C. The electrical stimulation of tibial osteotomies. Double-blind study. Clin. Orthop. Relat. Res. 1993, 288, 246–253. [Google Scholar] [CrossRef]
- Martinez-Rondanelli, A.; Martinez, J.P.; Moncada, M.E.; Manzi, E.; Pinedo, C.R.; Cadavid, H. Electromagnetic stimulation as coadjuvant in the healing of diaphyseal femoral fractures: A randomized controlled trial. Colom. Med. 2014, 45, 67–71. [Google Scholar]
- Griffin, X.L.; Costa, M.L.; Parsons, N.; Smith, N. Electromagnetic field stimulation for treating delayed union or non-union of long bone fractures in adults. Cochrane Database Syst. Rev. 2011, CD008471. [Google Scholar] [CrossRef]
- Ebrahim, S.; Mollon, B.; Bance, S.; Busse, J.W.; Bhandari, M. Low-intensity pulsed ultrasonography versus electrical stimulation for fracture healing: A systematic review and network meta-analysis. Can. J. Surg. 2014, 57, E105–E118. [Google Scholar] [CrossRef] [PubMed]
- Ehnert, S.; Falldorf, K.; Fentz, A.K.; Ziegler, P.; Schroter, S.; Freude, T.; Ochs, B.G.; Stacke, C.; Ronniger, M.; Sachtleben, J.; et al. Primary human osteoblasts with reduced alkaline phosphatase and matrix mineralization baseline capacity are responsive to extremely low frequency pulsed electromagnetic field exposure—Clinical implication possible. Bone Rep. 2015, 3, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Ehnert, S.; Fentz, A.K.; Schreiner, A.; Birk, J.; Wilbrand, B.; Ziegler, P.; Reumann, M.K.; Wang, H.; Falldorf, K.; Nussler, A.K. Extremely low frequency pulsed electromagnetic fields cause antioxidative defense mechanisms in human osteoblasts via induction of *o2(-) and h2o2. Sci. Rep. 2017, 7, 14544. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Sklar, G.E.; Min Sen Oh, V.; Chuen Li, S. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther. Clin. Risk Manag. 2008, 4, 269–286. [Google Scholar]
- Maciel, L.; Franzosi, O.S.; Nunes, D.S.L.; Loss, S.H.; Dos Reis, A.M.; Rubin, B.A.; Vieira, S.R.R. Nutritional risk screening 2002 cut-off to identify high-risk is a good predictor of icu mortality in critically ill patients. Nutr. Clin. Pract. 2018, 34, 137–141. [Google Scholar] [CrossRef]
- Schroter, S.; Freude, T.; Kopp, M.M.; Konstantinidis, L.; Dobele, S.; Stockle, U.; van Heerwaarden, R. Smoking and unstable hinge fractures cause delayed gap filling irrespective of early weight bearing after open wedge osteotomy. Arthroscopy 2015, 31, 254–265. [Google Scholar] [CrossRef]
- Lobenhoffer, P.; Agneskirchner, J.; Zoch, W. Open valgus alignment osteotomy of the proximal tibia with fixation by medial plate fixator. Orthopade 2004, 33, 153–160. [Google Scholar] [CrossRef]
- Staubli, A.E.; De Simoni, C.; Babst, R.; Lobenhoffer, P. Tomofix: A new lcp-concept for open wedge osteotomy of the medial proximal tibia—Early results in 92 cases. Injury 2003, 34 (Suppl. 2), B55–B62. [Google Scholar] [CrossRef]
- Sabzevari, S.; Ebrahimpour, A.; Roudi, M.K.; Kachooei, A.R. High tibial osteotomy: A systematic review and current concept. Arch. Bone Jt. Surg. 2016, 4, 204–212. [Google Scholar]
- Kumar, A.; Shalmanova, L.; Hammad, A.; Christmas, S.E. Induction of il-8(cxcl8) and mcp-1(ccl2) with oxidative stress and its inhibition with n-acetyl cysteine (nac) in cell culture model using hk-2 cell. Transpl. Immunol. 2016, 35, 40–46. [Google Scholar] [CrossRef]
- Jacobsen, S.E.; Okkenhaug, C.; Veiby, O.P.; Caput, D.; Ferrara, P.; Minty, A. Interleukin 13: Novel role in direct regulation of proliferation and differentiation of primitive hematopoietic progenitor cells. J. Exp. Med. 1994, 180, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Ehnert, S.; van Griensven, M.; Unger, M.; Scheffler, H.; Falldorf, K.; Fentz, A.K.; Seeliger, C.; Schroter, S.; Nussler, A.K.; Balmayor, E.R. Co-culture with human osteoblasts and exposure to extremely low frequency pulsed electromagnetic fields improve osteogenic differentiation of human adipose-derived mesenchymal stem cells. Int. J. Mol. Sci. 2018, 19, 994. [Google Scholar] [CrossRef] [PubMed]
- Adie, S.; Harris, I.A.; Naylor, J.M.; Rae, H.; Dao, A.; Yong, S.; Ying, V. Pulsed electromagnetic field stimulation for acute tibial shaft fractures: A multicenter, double-blind, randomized trial. J. Bone Jt. Surg. Am. 2011, 93, 1569–1576. [Google Scholar] [CrossRef]
- Zura, R.; Mehta, S.; Della Rocca, G.J.; Steen, R.G. Biological risk factors for nonunion of bone fracture. JBJS Rev. 2016, 4. [Google Scholar] [CrossRef]
- Bishop, J.A.; Palanca, A.A.; Bellino, M.J.; Lowenberg, D.W. Assessment of compromised fracture healing. J. Am. Acad. Orthop. Surg. 2012, 20, 273–282. [Google Scholar] [CrossRef]
- Hannemann, P.F.; Gottgens, K.W.; van Wely, B.J.; Kolkman, K.A.; Werre, A.J.; Poeze, M.; Brink, P.R. The clinical and radiological outcome of pulsed electromagnetic field treatment for acute scaphoid fractures: A randomised double-blind placebo-controlled multicentre trial. J. Bone Jt. Surg. Br. 2012, 94, 1403–1408. [Google Scholar] [CrossRef] [Green Version]
- Cebrian, J.L.; Gallego, P.; Frances, A.; Sanchez, P.; Manrique, E.; Marco, F.; Lopez-Duran, L. Comparative study of the use of electromagnetic fields in patients with pseudoarthrosis of tibia treated by intramedullary nailing. Int. Orthop. 2010, 34, 437–440. [Google Scholar] [CrossRef] [Green Version]
- Punt, B.J.; den Hoed, P.T.; Fontijne, W.P.J. Pulsed electromagnetic fields in the treatment of nonunion. Eur. J. Orthop. Surg. Traumatol. 2008, 18, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Luna Gonzalez, F.; Lopez Arevalo, R.; Meschian Coretti, S.; Urbano Labajos, V.; Delgado Rufino, B. Pulsed electromagnetic stimulation of regenerate bone in lengthening procedures. Acta Orthop. Belg. 2005, 71, 571–576. [Google Scholar]
- Hernandez, R.K.; Do, T.P.; Critchlow, C.W.; Dent, R.E.; Jick, S.S. Patient-related risk factors for fracture-healing complications in the united kingdom general practice research database. Acta Orthop. 2012, 83, 653–660. [Google Scholar] [CrossRef]
- Ohnuma, K.; Kasagi, S.; Uto, K.; Noguchi, Y.; Nakamachi, Y.; Saegusa, J.; Kawano, S. Microrna-124 inhibits tnf-alpha- and il-6-induced osteoclastogenesis. Rheumatol. Int. 2019, 39, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Yokota, K.; Sato, K.; Miyazaki, T.; Kitaura, H.; Kayama, H.; Miyoshi, F.; Araki, Y.; Akiyama, Y.; Takeda, K.; Mimura, T. Combination of tumor necrosis factor alpha and interleukin-6 induces mouse osteoclast-like cells with bone resorption activity both in vitro and in vivo. Arthritis Rheumatol. 2014, 66, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Jiang, H.; Wang, B.; Gu, M.; Bi, X.; Yin, Y.; Wang, Y. Magnetic resonance spectroscopy for evaluating the effect of pulsed electromagnetic fields on marrow adiposity in postmenopausal women with osteopenia. J. Comput. Assist. Tomogr. 2018, 42, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Elsisi, H.F.; Mousa, G.S.; MT, E.L. Electromagnetic field versus circuit weight training on bone mineral density in elderly women. Clin. Interv. Aging 2015, 10, 539–547. [Google Scholar] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Placebo | ELF-PEMF | p-Value * | |
|---|---|---|---|---|
| Number of patients | (1) | 37 | 37 | - |
| Sex distribution | (♂/♀) | 29/8 | 21/16 | 0.081 |
| Age | (a) | 52.9 ± 1.0 | 54.1 ± 1.3 | 0.865 |
| BMI | (kg/m2) | 29.9 ± 0.6 | 29.9 ± 1.0 | 0.887 |
| Mean wedge height | (mm) | 7.8 ± 1.8 | 7.6 ± 1.5 | 0.872 |
| Number of co-morbidities | (1) | 2.8 ± 0.2 | 2.6 ± 0.3 | 0.139 |
| NRS | (1) | 0.34 ± 0.09 | 0.43 ± 0.09 | 0.463 |
| Pre-Surgical Blood Values | Placebo | ELF-PEMF | p-Value * | |
|---|---|---|---|---|
| monocytes | (103/µL) | 0.43 ± 0.03 (0.38–0.48) | 0.44 ± 0.02 (0.39–0.48) | 0.791 |
| leucocytes | (103/µL) | 7.3 ± 0.3 (6.7–8.0) | 6.8 ± 0.3 (6.3–7.4) | 0.328 |
| lymphocytes | (103/µL) | 1.9 ± 0.1 (1.6–2.1) | 2.0 ± 0.1 (1.7–2.3) | 0.956 |
| neutrophils | (103/µL) | 4.4 ± 0.3 (3.8–5.0) | 4.1 ± 0.2 (3.7–4.5) | 0.405 |
| eosinophils | (103/µL) | 0.17 ± 0.02 (0.13–0.21) | 0.2 ± 0.0 (0.1–0.2) | 0.817 |
| basophils | (103/µL) | 0.05 ± 0.01 (0.04–0.06) | 0.05 ± 0.00 (0.04–0.06) | 0.900 |
| erythrocytes | (106/µL) | 4.9 ± 0.1 (4.8–5.0) | 4.8 ± 0.1 (4.7–5.0) | 0.646 |
| HB | (g/dL) | 15.1 ± 0.2 (14.8–15.4) | 14.6 ± 0.2 (14.2–15.0) | 0.061 |
| HKT | (%) | 44.2 ± 0.5 (43.3–45.2) | 43.3 ± 0.6 (42.1–44.4) | 0.141 |
| MCV | (fL) | 90.8 ± 0.6 (89.5–92.1) | 90.0 ± 0.7 (88.5–91.5) | 0.459 |
| MCH | (pg) | 31.0 ± 0.2 (30.5–31.4) | 30.4 ± 0.3 (29.8–30.9) | 0.203 |
| MCHC | (g/dL) | 34.2 ± 0.1 (33.9–34.4) | 33.8 ± 0.1 (33.6–34.0) | 0.104 |
| thrombocytes | (103/µL) | 241.2 ± 7.8 (227.8–264.4) | 275.2 ± 10.9 (253.1–297.4) | 0.031 |
| Quick | (%) | 106.6 ± 2.6 (101.5–111.6) | 112.5 ± 2.3 (107.9–117.1) | 0.299 |
| INR | (1) | 0.99 ± 0.01 (0.96–1.01) | 0.96 ± 0.01 (0.95–0.98) | 0.309 |
| PTT | (s) | 29.1 ± 0.5 (28.0–30.1) | 29.0 ± 0.5 (27.9–30.1) | 0.746 |
| CRP | (mg/L) | 6.0 ± 2.3 (1.5–10.5) | 7.2 ± 2.4 (2.4–12.1) | 0.668 |
| creatinine | (mg/dL) | 0.96 ± 0.03 (0.90–1.02) | 0.91 ± 0.03 (0.85–0.97) | 0.310 |
| sodium | (nmol/L) | 141.6 ± 0.3 (141.0–142.3) | 141.0 ± 0.4 (140.2–141.8) | 0.227 |
| potassium | (nmol/L) | 4.2 ± 0.1 (4.1–4.4) | 4.3 ± 0.1 (4.1–4.4) | 0.623 |
| GOT | (U/L) | 24.3 ± 1.7 (20.5–27.5) | 23.4 ± 1.4 (20.6–26.3) | 0.946 |
| g-GT | (U/L) | 44.6 ± 11.0 (22.0–65.5) | 31.6 ± 5.7 (20.0–43.1) | 0.572 |
| glucose | (mg/dL) | 110.8 ± 4.6 (101.3–119.7) | 105.2 ± 4.0 (97.0–113.5) | 0.605 |
| Placebo | ELF-PEMF | p-Value * | |||
|---|---|---|---|---|---|
| Number of patients | (1) | 27 | 24 | - | |
| Sex distribution | (♂/♀) | 20/7 | 13/11 | 0.156 | |
| Age | all | (a) | 55.6 ± 0.7 | 57.5 ± 1.3 | 0.398 |
| ♂ | (a) | 56.3 ± 0.8 | 55.5 ± 1.1 | 0.612 | |
| ♀ | (a) | 53.3 ± 0.7 | 58.6 ± 2.2 | 0.056 | |
| BMI | (kg/m2) | 29.6 ± 0.7 | 29.5 ± 1.1 | 0.578 | |
| Mean wedge height | (mm) | 7.9 ± 0.3 | 7.8 ± 0.3 | 0.834 | |
| Number of co-morbidities | (1) | 2.9 ± 0.2 | 2.8 ± 0.4 | 0.655 | |
| NRS | (1) | 0.38 ± 0.10 | 0.29 ± 0.10 | 0.513 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziegler, P.; Nussler, A.K.; Wilbrand, B.; Falldorf, K.; Springer, F.; Fentz, A.-K.; Eschenburg, G.; Ziegler, A.; Stöckle, U.; Maurer, E.; et al. Pulsed Electromagnetic Field Therapy Improves Osseous Consolidation after High Tibial Osteotomy in Elderly Patients—A Randomized, Placebo-Controlled, Double-Blind Trial. J. Clin. Med. 2019, 8, 2008. https://doi.org/10.3390/jcm8112008
Ziegler P, Nussler AK, Wilbrand B, Falldorf K, Springer F, Fentz A-K, Eschenburg G, Ziegler A, Stöckle U, Maurer E, et al. Pulsed Electromagnetic Field Therapy Improves Osseous Consolidation after High Tibial Osteotomy in Elderly Patients—A Randomized, Placebo-Controlled, Double-Blind Trial. Journal of Clinical Medicine. 2019; 8(11):2008. https://doi.org/10.3390/jcm8112008
Chicago/Turabian StyleZiegler, Patrick, Andreas K. Nussler, Benjamin Wilbrand, Karsten Falldorf, Fabian Springer, Anne-Kristin Fentz, Georg Eschenburg, Andreas Ziegler, Ulrich Stöckle, Elke Maurer, and et al. 2019. "Pulsed Electromagnetic Field Therapy Improves Osseous Consolidation after High Tibial Osteotomy in Elderly Patients—A Randomized, Placebo-Controlled, Double-Blind Trial" Journal of Clinical Medicine 8, no. 11: 2008. https://doi.org/10.3390/jcm8112008