Urinary Biomarkers α-GST and π-GST for Evaluation and Monitoring in Living and Deceased Donor Kidney Grafts

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Samples and Data Collection
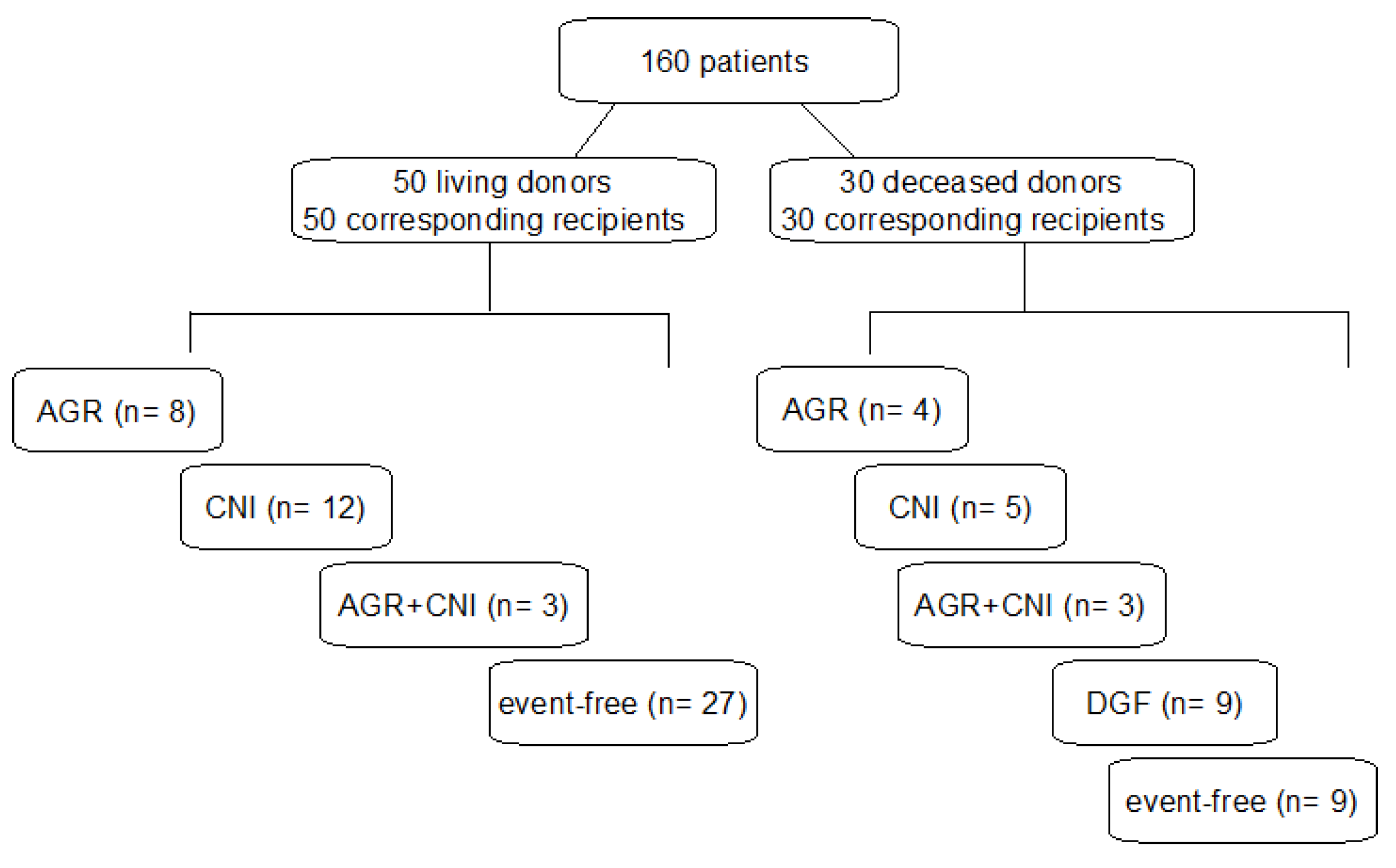
2.2. Immunosuppression Events and Subgroups
2.3. GST Analysis and Statistics
3. Results
3.1. Demographic Data
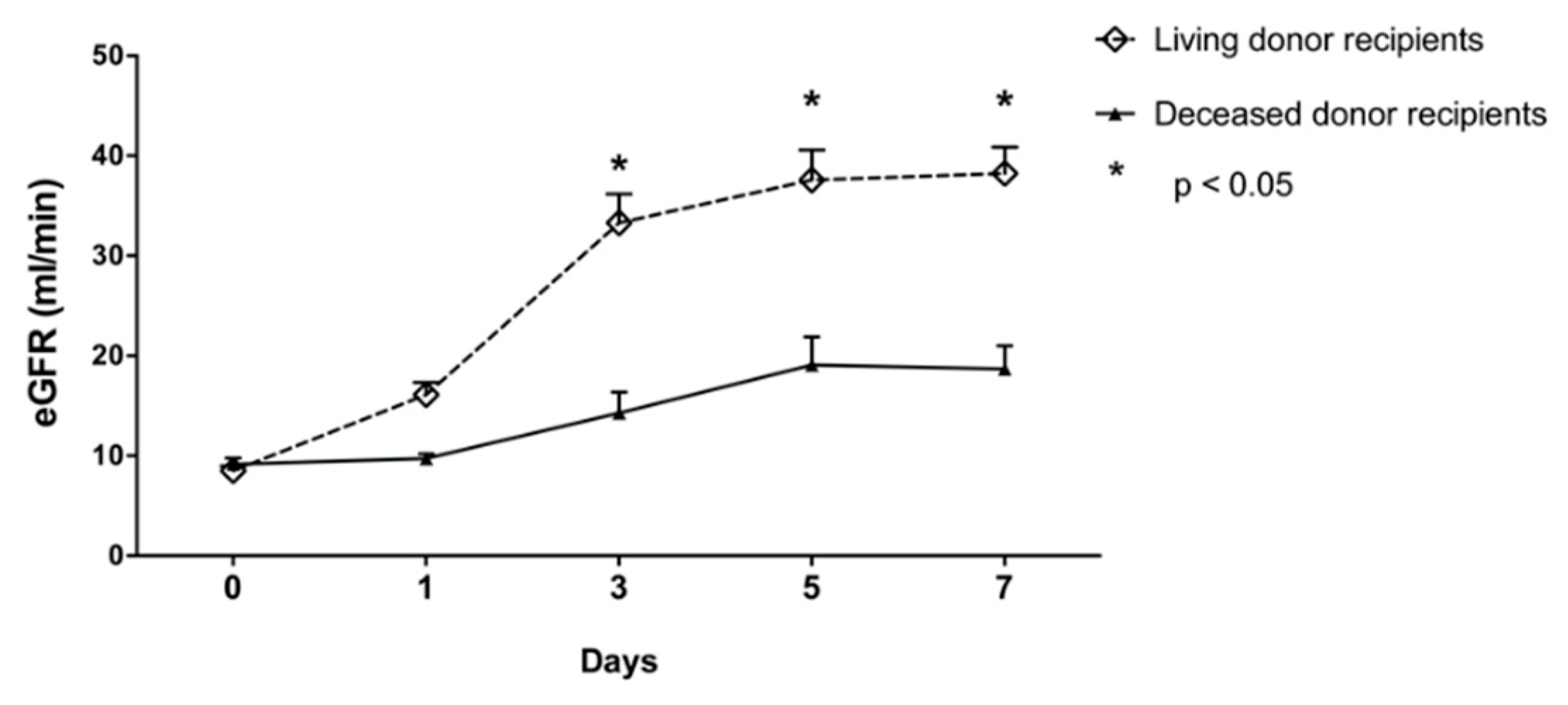
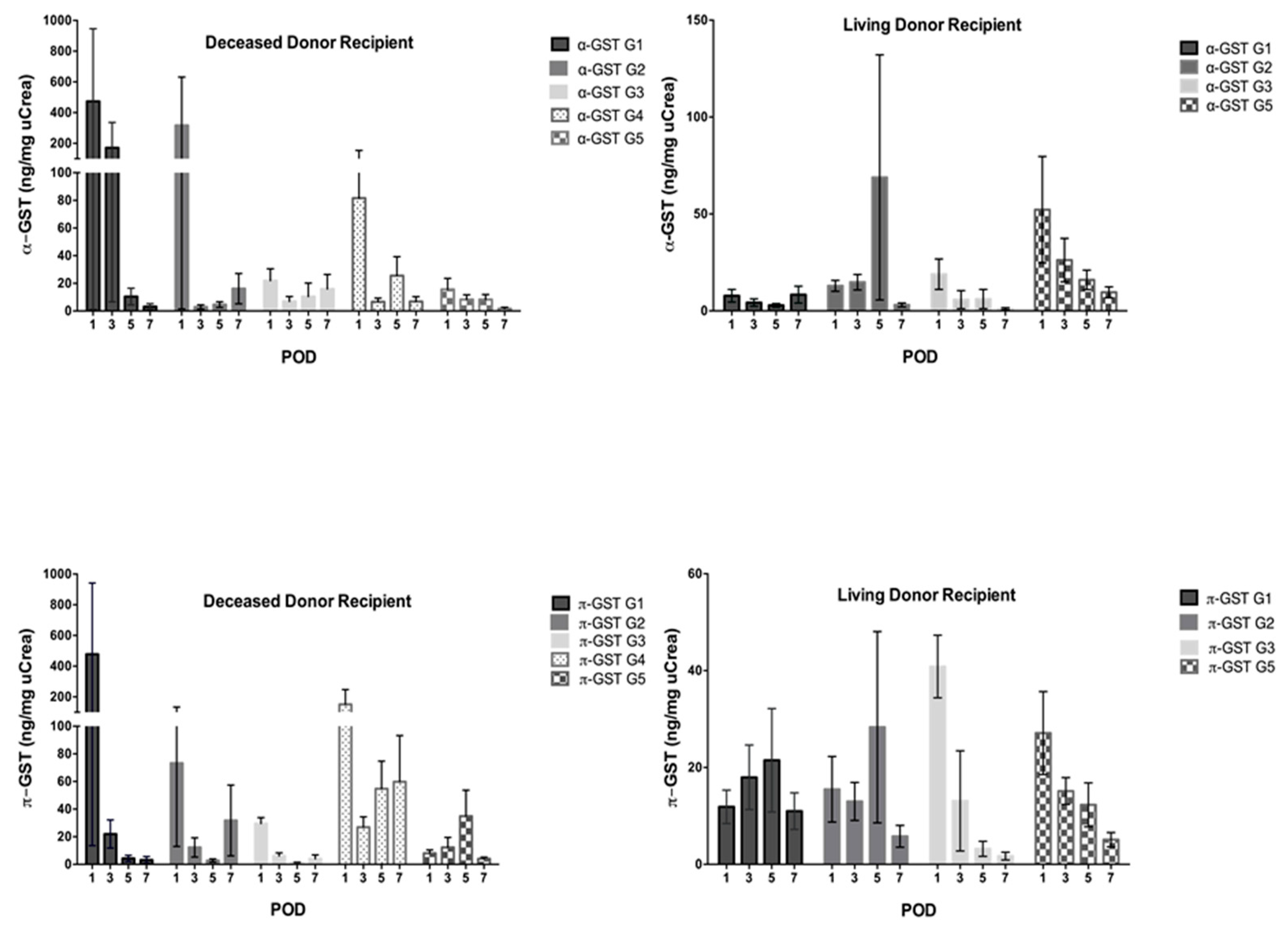
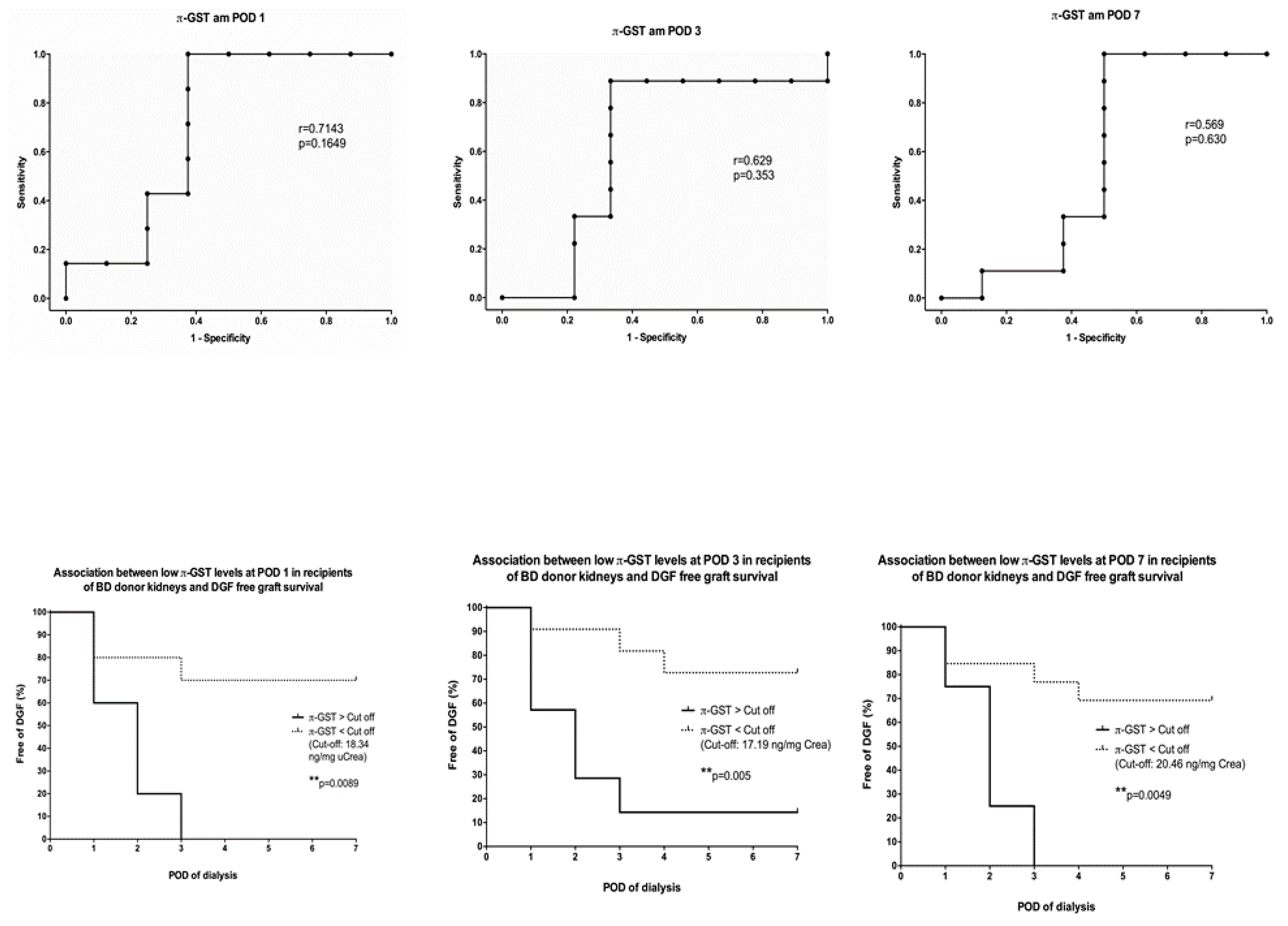
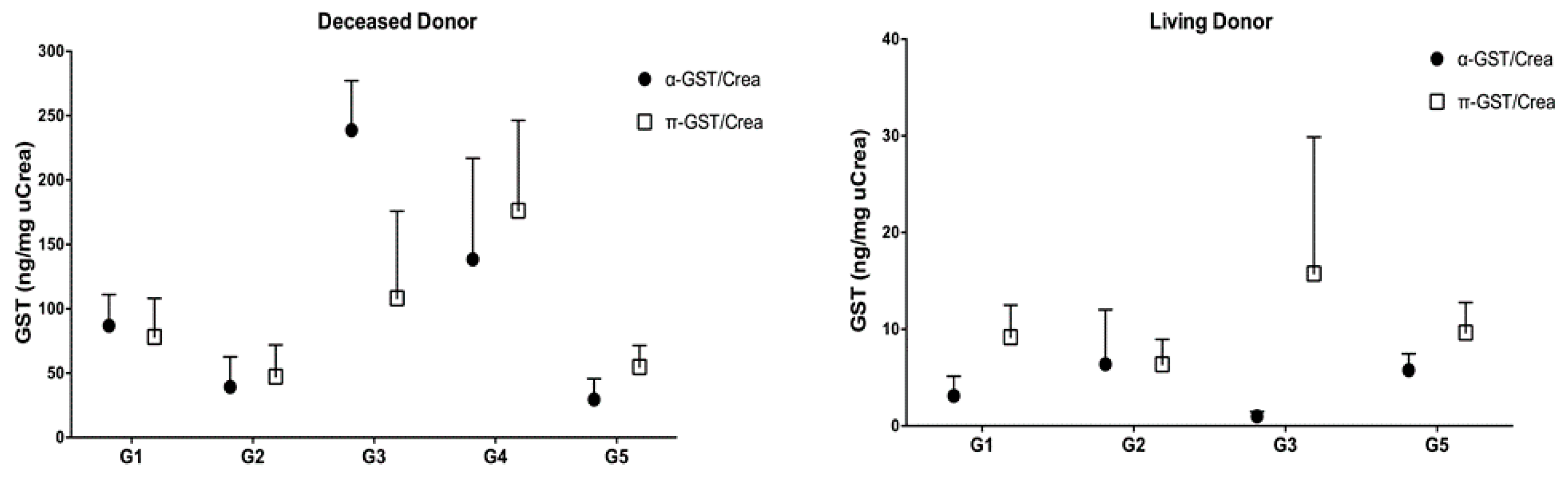
3.2. α- and π-GST in Recipients
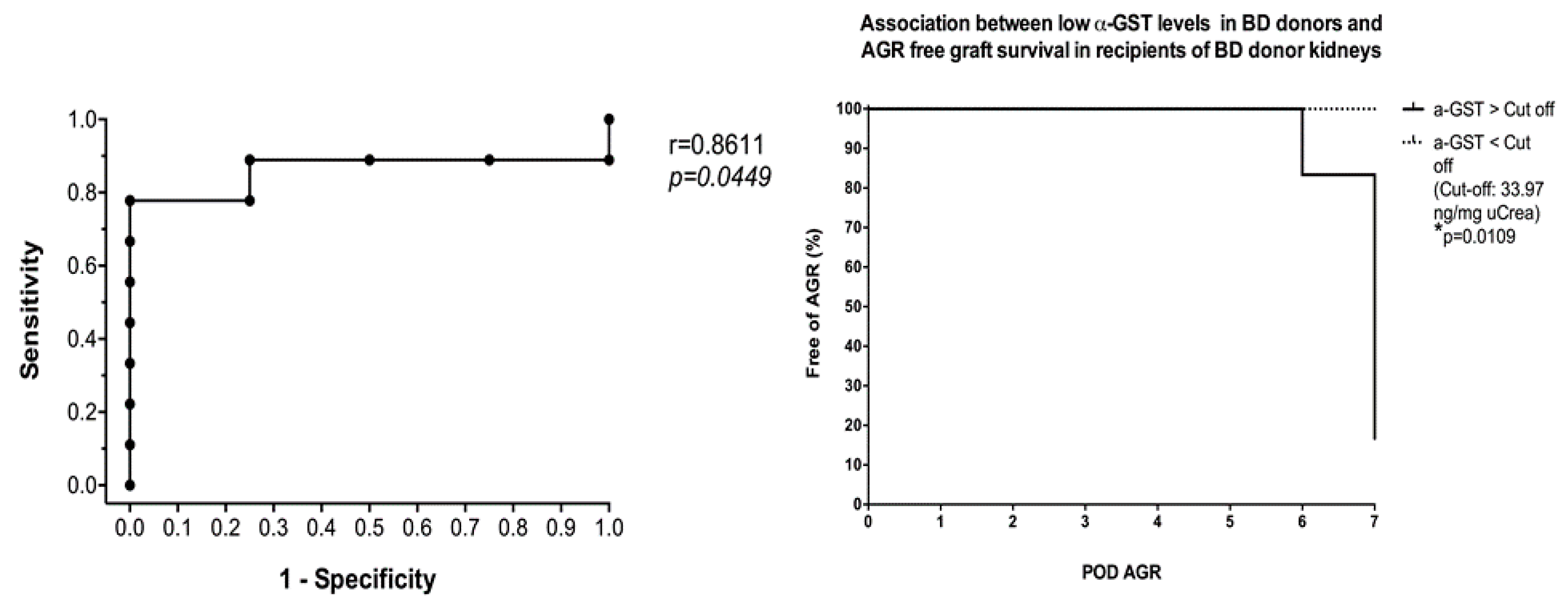
3.3. α- and π-GST in Donors
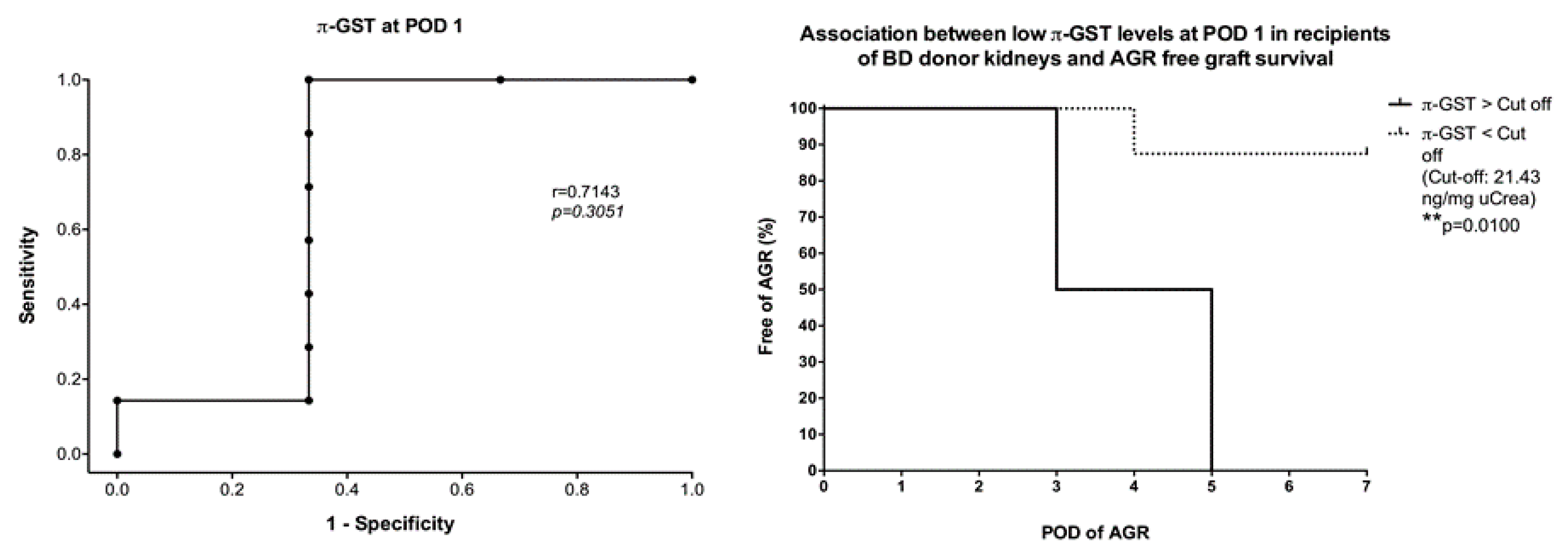
3.4. Six- and 12-Months Graft Survival
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Wu, W.K.; Famure, O.; Li, Y.; Kim, S.J. Delayed graft function and the risk of acute rejection in the modern era of kidney transplantation. Kidney Int. 2015, 88, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Marcen, R.; Fernandez-Rodriguez, A.; Rodriguez-Mendiola, N.; Ponte, B.; Galeano, C.; Villafruela, J.J.; Teruel, J.L.; Burgos, F.J.; Ortuno, J. Evolution of rejection rates and kidney graft survival: A historical analysis. Transplant Proc. 2009, 41, 2357–2359. [Google Scholar] [CrossRef]
- Martins, L.; Ventura, A.; Branco, A.; Carvalho, M.J.; Henriques, A.C.; Dias, L.; Sarmento, A.M.; Amil, M. Cyclosporine versus tacrolimus in kidney transplantation: Are there differences in nephrotoxicity? Transplant Proc. 2004, 36, 877–879. [Google Scholar] [CrossRef]
- Ojo, A.O.; Wolfe, R.A.; Held, P.J.; Port, F.K.; Schmouder, R.L. Delayed graft function: Risk factors and implications for renal allograft survival. Transplantation 1997, 63, 968–974. [Google Scholar] [CrossRef]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed graft function in the kidney transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef]
- Klintmalm, G.; Sawe, J.; Ringden, O.; von Bahr, C.; Magnusson, A. Cyclosporine plasma levels in renal transplant patients. Association with renal toxicity and allograft rejection. Transplantation 1985, 39, 132–137. [Google Scholar] [CrossRef]
- Wilczek, H.E. Percutaneous needle biopsy of the renal allograft. A clinical safety evaluation of 1129 biopsies. Transplantation 1990, 50, 790–797. [Google Scholar] [CrossRef]
- Branten, A.J.; Mulder, T.P.; Peters, W.H.; Assmann, K.J.; Wetzels, J.F. Urinary excretion of glutathione S transferases alpha and pi in patients with proteinuria: Reflection of the site of tubular injury. Nephron 2000, 85, 120–126. [Google Scholar] [CrossRef]
- Harrison, D.J.; Kharbanda, R.; Cunningham, D.S.; McLellan, L.I.; Hayes, J.D. Distribution of glutathione S-transferase isoenzymes in human kidney: Basis for possible markers of renal injury. J. Clin. Pathol. 1989, 42, 624–628. [Google Scholar] [CrossRef]
- Backman, L.; Appelkvist, E.L.; Ringden, O.; Dallner, G. Glutathione transferase in the urine: A marker for post-transplant tubular lesions. Kidney Int. 1988, 33, 571–577. [Google Scholar] [CrossRef] [Green Version]
- Kuzniar, J.; Marchewka, Z.; Krasnowski, R.; Boratynska, M.; Dlugosz, A.; Klinger, M. Enzymuria and low molecular weight protein excretion as the differentiating marker of complications in the early post kidney transplantation period. Int. Urol. Nephrol. 2006, 38, 753–758. [Google Scholar] [CrossRef]
- Polak, W.P.; Kosieradzki, M.; Kwiatkowski, A.; Danielewicz, R.; Lisik, W.; Michalak, G.; Paczek, L.; Lao, M.; Walaszewski, J.; Rowinski, W.A. Activity of glutathione S-transferases in the urine of kidney transplant recipients during the first week after transplantation. Ann. Transplant. 1999, 4, 42–45. [Google Scholar]
- Sundberg, A.G.; Appelkvist, E.L.; Backman, L.; Dallner, G. Urinary Pi-Class Glutathione Transferase as an Indicator of Tubular Damage in the Human Kidney. Nephron 1994, 67, 308–316. [Google Scholar] [CrossRef]
- Backman, L.; Appelkvist, E.L.; Ringden, O.; Dallner, G. Appearance of basic glutathione transferase in the urine during tubular complications in renal transplant recipients. Transplant. Proc. 1988, 20, 427–430. [Google Scholar]
- Westhuyzen, J.; Endre, Z.H.; Reece, G.; Reith, D.M.; Saltissi, D.; Morgan, T.J. Measurement of tubular enzymuria facilitates early detection of acute renal impairment in the intensive care unit. Nephrol. Dial. Transplant. 2003, 18, 543–551. [Google Scholar] [CrossRef]
- Jochum, C.; Beste, M.; Sowa, J.P.; Farahani, M.S.; Penndorf, V.; Nadalin, S.; Saner, F.; Canbay, A.; Gerken, G. Glutathione-S-transferase subtypes alpha and pi as a tool to predict and monitor graft failure or regeneration in a pilot study of living donor liver transplantation. Eur. J. Med. Res. 2011, 16, 34–40. [Google Scholar] [CrossRef]
- Daemen, J.W.; Oomen, A.P.; Janssen, M.A.; van de Schoot, L.; van Kreel, B.K.; Heineman, E.; Kootstra, G. Glutathione S-transferase as predictor of functional outcome in transplantation of machine-preserved non-heart-beating donor kidneys. Transplantation 1997, 63, 89–93. [Google Scholar] [CrossRef]
- Sundberg, A.; Appelkvist, E.L.; Dallner, G.; Nilsson, R. Glutathione transferases in the urine—Sensitive methods for detection of kidney damage-induced by nephrotoxic agents in humans. Environ. Health Perspect. 1994, 102, 293–296. [Google Scholar]
- Min, D.I.; Perry, P.J.; Chen, H.Y.; Hunsicker, L.G. Cyclosporine trough concentrations in predicting allograft rejection and renal toxicity up to 12 months after renal transplantation. Pharmacotherapy 1998, 18, 282–287. [Google Scholar]
- Bottiger, Y.; Brattstrom, C.; Tyden, G.; Sawe, J.; Groth, C.G. Tacrolimus whole blood concentrations correlate closely to side-effects in renal transplant recipients. Br. J. Clin. Pharmacol. 1999, 48, 445–448. [Google Scholar] [CrossRef]
- Schiff, J.; Cole, E.; Cantarovich, M. Therapeutic monitoring of calcineurin inhibitors for the nephrologist. Clin. J. Am. Soc. Nephrol. 2007, 2, 374–384. [Google Scholar] [CrossRef]
- Undre, N.A.; van Hooff, J.; Christiaans, M.; Vanrenterghem, Y.; Donck, J.; Heeman, U.; Kohnle, M.; Zanker, B.; Land, W.; Morales, J.M.; et al. Stevenson, P. Low systemic exposure to tacrolimus correlates with acute rejection. Transplant. Proc. 1999, 31, 296–298. [Google Scholar] [CrossRef]
- Willicombe, M.; Rizzello, A.; Goodall, D.; Papalois, V.; McLean, A.G.; Taube, D. Risk factors and outcomes of delayed graft function in renal transplant recipients receiving a steroid sparing immunosuppression protocol. World J. Transplant. 2017, 7, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Irish, W.D.; Ilsley, J.N.; Schnitzler, M.A.; Feng, S.; Brennan, D.C. A risk prediction model for delayed graft function in the current era of deceased donor renal transplantation. Am. J. Transplant. 2010, 10, 2279–2286. [Google Scholar] [CrossRef]
- Sundberg, A.G.; Nilsson, R.; Appelkvist, E.L.; Dallner, G. Immunohistochemical Localization of Alpha-Class and Pi-Class Glutathione Transferases in Normal Human Tissues. Pharmacol. Toxicol. 1993, 72, 321–331. [Google Scholar] [CrossRef]
- Seabra, V.F.; Perianayagam, M.C.; Tighiouart, H.; Liangos, O.; dos Santos, O.F.; Jaber, B.L. Urinary alpha-GST and pi-GST for prediction of dialysis requirement or in-hospital death in established acute kidney injury. Biomarkers 2011, 16, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Hall, I.E.; Bhangoo, R.S.; Reese, P.P.; Doshi, M.D.; Weng, F.L.; Hong, K.; Lin, H.; Han, G.; Hasz, R.D.; Goldstein, M.J.; et al. Glutathione S-transferase iso-enzymes in perfusate from pumped kidneys are associated with delayed graft function. Am. J. Transplant. 2014, 14, 886–896. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Deceased Donor Grafts | Living Donor Grafts | p Value | |
|---|---|---|---|
| Donor | 30 | 50 | |
| Age (years) | 58 ± 15 | 53 ± 10 | n.s. |
| Sex (male/female) | 11/19 | 22/28 | n.s. |
| BMI | 27.3 ± 6.5 | 25.3 ± 3.2 | n.s. |
| eGFR, d0 (mL/min) | 96 ± 39 | 97 ± 18 | n.s. |
| Diuresis in last hour (mL) | 152 ± 81 | - | |
| Recipient | 30 | 50 | |
| Age (years) | 58 ± 12 | 47 ± 15 | <0.05 |
| Sex (male/female) | 22/8 | 35/15 | n.s. |
| BMI | 26.4 ± 4 | 25.8 ± 4.9 | n.s. |
| eGFR, d0 (mL/min) | 9 ± 3 | 8 ± 4 | n.s. |
| Primary disease | |||
| Glomerulonephritis | 9 | 24 | n.s. |
| Hypertensive nephrosclerosis | 7 | 9 | n.s. |
| Polycystic kidney disease | 6 | 2 | n.s. |
| Autoimmune disease | 2 | 5 | n.s. |
| Diabetes | 2 | 3 | n.s. |
| Urologic disease | 2 | 2 | n.s. |
| Calcineurin-induced nephrotoxicity | 0 | 2 | n.s. |
| Others | 2 | 3 | n.s. |
| Dialysis | |||
| Hemodialysis | 29 | 28 | n.s. |
| Peritoneal dialysis | 1 | 3 | n.s. |
| No dialysis | 0 | 19 | <0.05 |
| Cold ischemia time (minutes) | 613 ± 269 | 193 ± 62 | <0.05 |
| Warm ischemia time (minutes) | 34 ± 11 | 23 ± 7 | <0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katou, S.; Globke, B.; Morgul, M.H.; Vogel, T.; Struecker, B.; Otto, N.M.; Reutzel-Selke, A.; Marksteiner, M.; Brockmann, J.G.; Pascher, A.; et al. Urinary Biomarkers α-GST and π-GST for Evaluation and Monitoring in Living and Deceased Donor Kidney Grafts. J. Clin. Med. 2019, 8, 1899. https://doi.org/10.3390/jcm8111899
Katou S, Globke B, Morgul MH, Vogel T, Struecker B, Otto NM, Reutzel-Selke A, Marksteiner M, Brockmann JG, Pascher A, et al. Urinary Biomarkers α-GST and π-GST for Evaluation and Monitoring in Living and Deceased Donor Kidney Grafts. Journal of Clinical Medicine. 2019; 8(11):1899. https://doi.org/10.3390/jcm8111899
Chicago/Turabian StyleKatou, Shadi, Brigitta Globke, M. Haluk Morgul, Thomas Vogel, Benjamin Struecker, Natalie Maureen Otto, Anja Reutzel-Selke, Marion Marksteiner, Jens G. Brockmann, Andreas Pascher, and et al. 2019. "Urinary Biomarkers α-GST and π-GST for Evaluation and Monitoring in Living and Deceased Donor Kidney Grafts" Journal of Clinical Medicine 8, no. 11: 1899. https://doi.org/10.3390/jcm8111899