CMR Tissue Characterization in Patients with HFmrEF

 ,
,
Abstract
:1. Introduction
2. Experimental Section
3. Results
3.1. Patients
3.2. CMR-Parameters
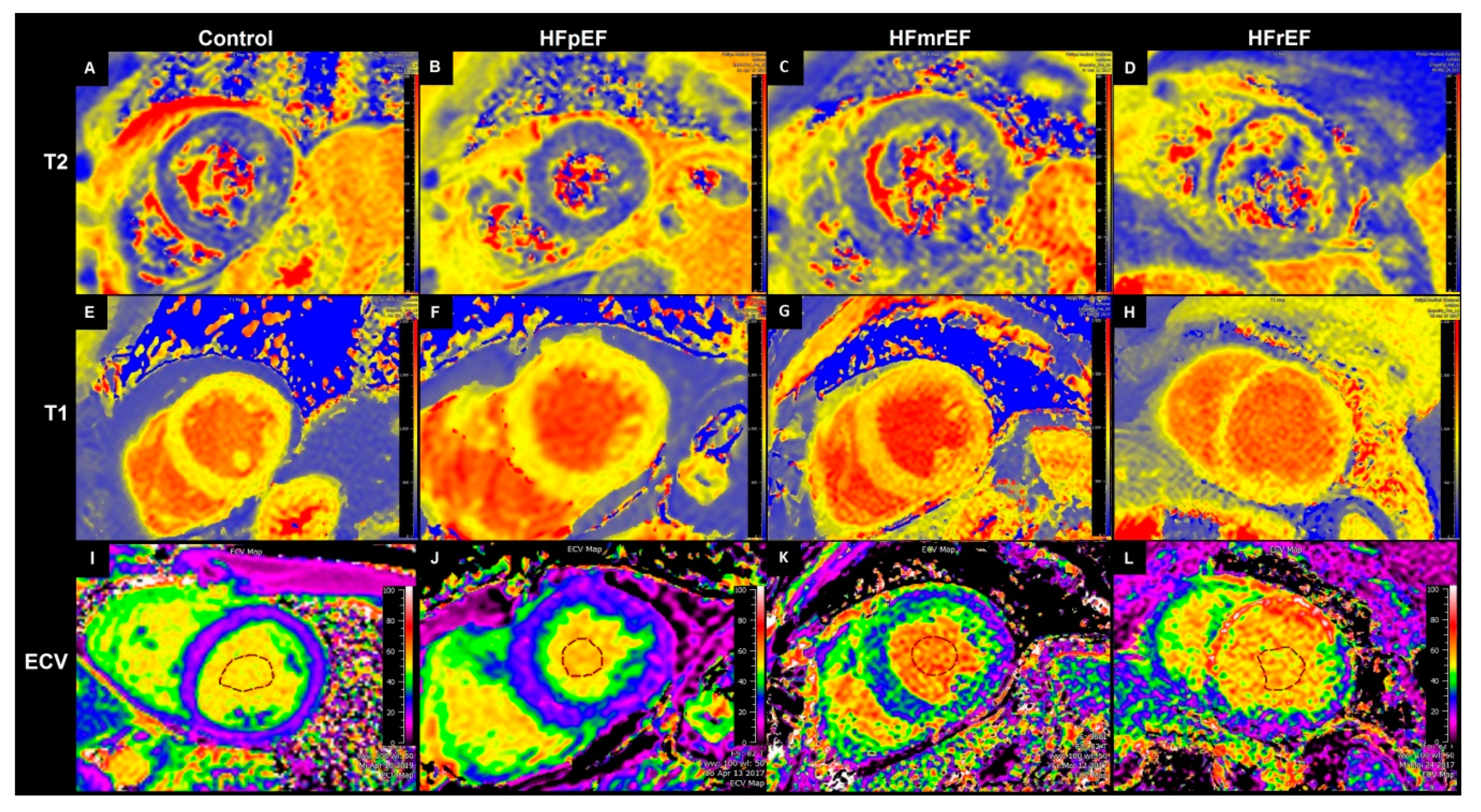
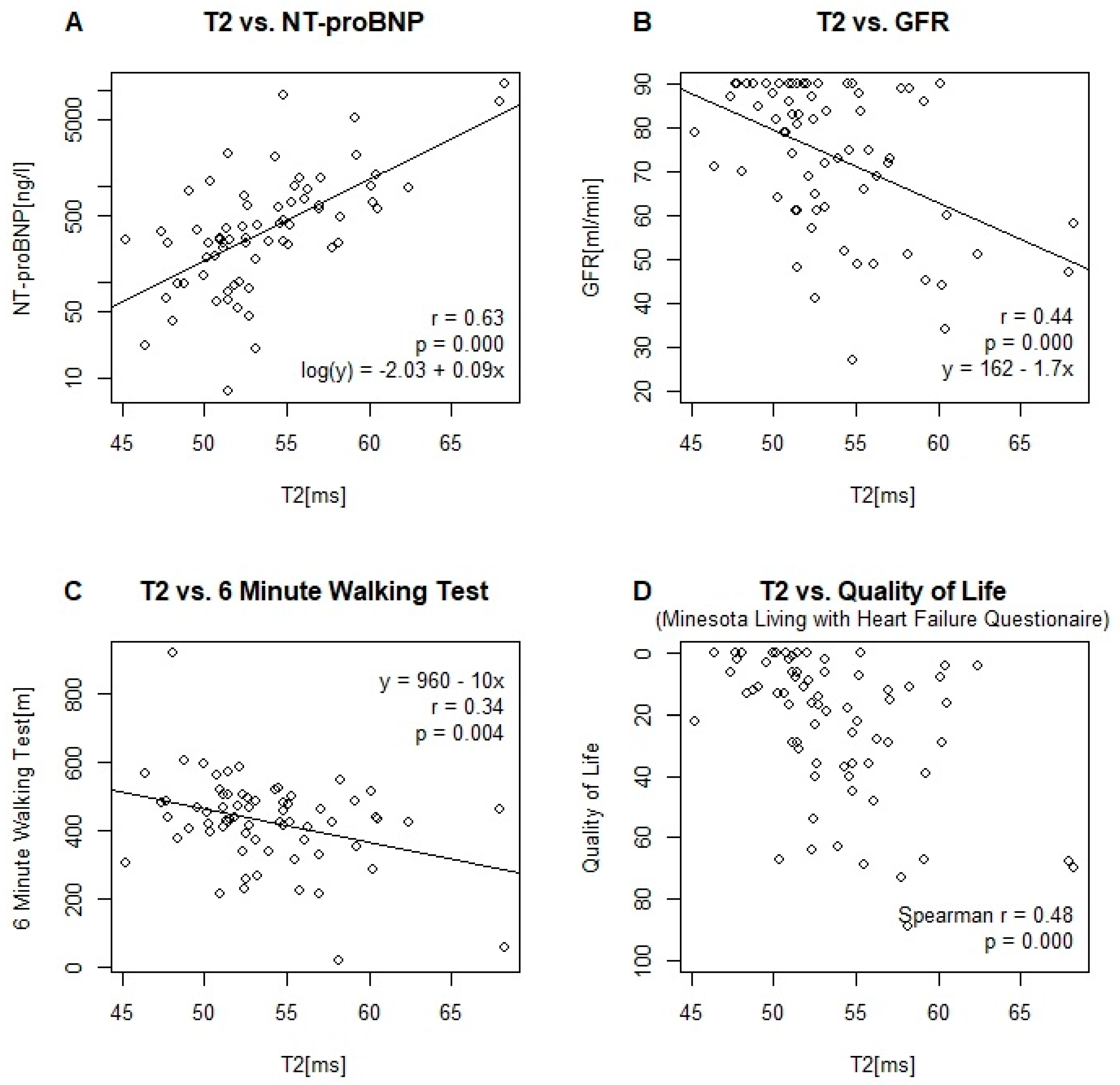
3.2.1. T2 Relaxation Time
3.2.2. T1 Relaxation Time
3.2.3. Extracellular Volume (ECV)
3.2.4. Strain
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Cohn, J.N.; Ferrari, R.; Sharpe, N. Cardiac remodeling—Concepts and clinical implications: A consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J. Am. Coll. Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef]
- Zheng, S.L.; Chan, F.T.; Nabeebaccus, A.A.; Shah, A.M.; McDonagh, T.; Okonko, D.O.; Ayis, S. Drug treatment effects on outcomes in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Heart 2018, 104, 407–415. [Google Scholar] [CrossRef]
- Altaie, S.; Khalife, W. The prognosis of mid-range ejection fraction heart failure: A systematic review and meta-analysis. ESC Heart Fail. 2018, 5, 1008–1016. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef]
- Ugander, M.; Oki, A.J.; Hsu, L.Y.; Kellman, P.; Greiser, A.; Aletras, A.H.; Sibley, C.T.; Chen, M.Y.; Bandettini, W.P.; Arai, A.E. Extracellular volume imaging by magnetic resonance imaging provides insights into overt and sub-clinical myocardial pathology. Eur. Heart J. 2012, 33, 1268–1278. [Google Scholar] [CrossRef] [Green Version]
- Puntmann, V.O.; Carr-White, G.; Jabbour, A.; Yu, C.Y.; Gebker, R.; Kelle, S.; Hinojar, R.; Doltra, A.; Varma, N.; Child, N.; et al. T1-Mapping and Outcome in Nonischemic Cardiomyopathy: All-Cause Mortality and Heart Failure. JACC 2016, 9, 40–50. [Google Scholar] [CrossRef]
- Schelbert, E.B.; Piehler, K.M.; Zareba, K.M.; Moon, J.C.; Ugander, M.; Messroghli, D.R.; Valeti, U.S.; Chang, C.C.; Shroff, S.G.; Diez, J.; et al. Myocardial Fibrosis Quantified by Extracellular Volume Is Associated With Subsequent Hospitalization for Heart Failure, Death, or Both Across the Spectrum of Ejection Fraction and Heart Failure Stage. J. Am. Heart Assoc. 2015, 4, e002613. [Google Scholar] [CrossRef]
- Bohnen, S.; Radunski, U.K.; Lund, G.K.; Kandolf, R.; Stehning, C.; Schnackenburg, B.; Adam, G.; Blankenberg, S.; Muellerleile, K. Performance of t1 and t2 mapping cardiovascular magnetic resonance to detect active myocarditis in patients with recent-onset heart failure. Circ. Cardiovasc. Imaging 2015, 8, e003073. [Google Scholar] [CrossRef]
- Scatteia, A.; Baritussio, A.; Bucciarelli-Ducci, C. Strain imaging using cardiac magnetic resonance. Heart Fail. Rev. 2017, 22, 465–476. [Google Scholar] [CrossRef]
- DRKS-German Clinical Trials Register. DRKS00015615. Available online: https://www.drks.de (accessed on 10 September 2019).
- Messroghli, D.R.; Radjenovic, A.; Kozerke, S.; Higgins, D.M.; Sivananthan, M.U.; Ridgway, J.P. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn. Reson. Med. 2004, 52, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Baessler, B.; Schaarschmidt, F.; Stehning, C.; Schnackenburg, B.; Maintz, D.; Bunck, A.C. Cardiac T2-mapping using a fast gradient echo spin echo sequence-first in vitro and in vivo experience. J. Cardiovasc. Magn. Reson. 2015, 17, 67. [Google Scholar] [CrossRef] [PubMed]
- Dabir, D.; Child, N.; Kalra, A.; Rogers, T.; Gebker, R.; Jabbour, A.; Plein, S.; Yu, C.Y.; Otton, J.; Kidambi, A.; et al. Reference values for healthy human myocardium using a T1 mapping methodology: Results from the International T1 Multicenter cardiovascular magnetic resonance study. J. Cardiovasc. Magn. Reson. 2014, 16, 69. [Google Scholar] [CrossRef] [PubMed]
- Suinesiaputra, A.; Bluemke, D.A.; Cowan, B.R.; Friedrich, M.G.; Kramer, C.M.; Kwong, R.; Plein, S.; Schulz-Menger, J.; Westenberg, J.J.; Young, A.A.; et al. Quantification of LV function and mass by cardiovascular magnetic resonance: Multi-center variability and consensus contours. J. Cardiovasc. Magn. Reson. 2015, 17, 63. [Google Scholar] [CrossRef]
- aus dem Siepen, F.; Buss, S.J.; Messroghli, D.; Andre, F.; Lossnitzer, D.; Seitz, S.; Keller, M.; Schnabel, P.A.; Giannitsis, E.; Korosoglou, G.; et al. T1 mapping in dilated cardiomyopathy with cardiac magnetic resonance: Quantification of diffuse myocardial fibrosis and comparison with endomyocardial biopsy. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Lurz, P.; Luecke, C.; Eitel, I.; Fohrenbach, F.; Frank, C.; Grothoff, M.; de Waha, S.; Rommel, K.P.; Lurz, J.A.; Klingel, K.; et al. Comprehensive Cardiac Magnetic Resonance Imaging in Patients With Suspected Myocarditis: The MyoRacer-Trial. J. Am. Coll. Cardiol. 2016, 67, 1800–1811. [Google Scholar] [CrossRef] [PubMed]
- Mordi, I.; Carrick, D.; Bezerra, H.; Tzemos, N. T1 and T2 mapping for early diagnosis of dilated non-ischaemic cardiomyopathy in middle-aged patients and differentiation from normal physiological adaptation. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 797–803. [Google Scholar] [CrossRef]
- Rommel, K.P.; von Roeder, M.; Latuscynski, K.; Oberueck, C.; Blazek, S.; Fengler, K.; Besler, C.; Sandri, M.; Lucke, C.; Gutberlet, M.; et al. Extracellular Volume Fraction for Characterization of Patients With Heart Failure and Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2016, 67, 1815–1825. [Google Scholar] [CrossRef]
- Roy, C.; Slimani, A.; de Meester, C.; Amzulescu, M.; Pasquet, A.; Vancraeynest, D.; Beauloye, C.; Vanoverschelde, J.L.; Gerber, B.L.; Pouleur, A.C. Associations and prognostic significance of diffuse myocardial fibrosis by cardiovascular magnetic resonance in heart failure with preserved ejection fraction. J. Cardiovasc. Magn. Reson. 2018, 20, 55. [Google Scholar] [CrossRef]
- Duca, F.; Kammerlander, A.A.; Zotter-Tufaro, C.; Aschauer, S.; Schwaiger, M.L.; Marzluf, B.A.; Bonderman, D.; Mascherbauer, J. Interstitial Fibrosis, Functional Status, and Outcomes in Heart Failure With Preserved Ejection Fraction: Insights From a Prospective Cardiac Magnetic Resonance Imaging Study. Circ. Cardiovasc. Imaging 2016, 9, e005277. [Google Scholar] [CrossRef]
- Su, M.Y.; Lin, L.Y.; Tseng, Y.H.; Chang, C.C.; Wu, C.K.; Lin, J.L.; Tseng, W.Y. CMR-verified diffuse myocardial fibrosis is associated with diastolic dysfunction in HFpEF. JACC Cardiovasc. Imaging 2014, 7, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Schelbert, E.B.; Fridman, Y.; Wong, T.C.; Abu Daya, H.; Piehler, K.M.; Kadakkal, A.; Miller, C.A.; Ugander, M.; Maanja, M.; Kellman, P.; et al. Temporal Relation Between Myocardial Fibrosis and Heart Failure With Preserved Ejection Fraction: Association With Baseline Disease Severity and Subsequent Outcome. JAMA Cardiol. 2017, 2, 995–1006. [Google Scholar] [CrossRef] [PubMed]
- Kawel-Boehm, N.; Maceira, A.; Valsangiacomo-Buechel, E.R.; Vogel-Claussen, J.; Turkbey, E.B.; Williams, R.; Plein, S.; Tee, M.; Eng, J.; Bluemke, D.A. Normal values for cardiovascular magnetic resonance in adults and children. J. Cardiovasc. Magn. Reson. 2015, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.; Fonarow, G.C.; Zile, M.R.; Lam, C.S.; Roessig, L.; Schelbert, E.B.; Shah, S.J.; Ahmed, A.; Bonow, R.O.; Cleland, J.G.; et al. Developing therapies for heart failure with preserved ejection fraction: Current state and future directions. JACC Heart Fail. 2014, 2, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Ge, J.; Lam, C.S.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; et al. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2019, 381, 65–72. [Google Scholar] [CrossRef]
- Baessler, B.; Schaarschmidt, F.; Stehning, C.; Schnackenburg, B.; Maintz, D.; Bunck, A.C. A systematic evaluation of three different cardiac T2-mapping sequences at 1.5 and 3T in healthy volunteers. Eur. J. Radiol. 2015, 84, 2161–2170. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Walls, M.; Giri, S.; Verhaert, D.; Rajagopalan, S.; Moore, S.; Simonetti, O.P.; Raman, S.V. Improved detection of myocardial involvement in acute inflammatory cardiomyopathies using T2 mapping. Circ. Cardiovasc. Imaging 2012, 5, 102–110. [Google Scholar] [CrossRef]
- Nishii, T.; Kono, A.K.; Shigeru, M.; Takamine, S.; Fujiwara, S.; Kyotani, K.; Aoyama, N.; Sugimura, K. Cardiovascular magnetic resonance T2 mapping can detect myocardial edema in idiopathic dilated cardiomyopathy. Int. J. Cardiovasc. Imaging 2014, 30, 65–72. [Google Scholar] [CrossRef]
- Verhaert, D.; Thavendiranathan, P.; Giri, S.; Mihai, G.; Rajagopalan, S.; Simonetti, O.P.; Raman, S.V. Direct T2 quantification of myocardial edema in acute ischemic injury. JACC Cardiovasc. Imaging 2011, 4, 269–278. [Google Scholar] [CrossRef]
- Dick, S.A.; Epelman, S. Chronic Heart Failure and Inflammation: What Do We Really Know? Circ. Res. 2016, 119, 159–176. [Google Scholar] [CrossRef]
- Mordi, I.R.; Singh, S.; Rudd, A.; Srinivasan, J.; Frenneaux, M.; Tzemos, N.; Dawson, D.K. Comprehensive Echocardiographic and Cardiac Magnetic Resonance Evaluation Differentiates Among Heart Failure With Preserved Ejection Fraction Patients, Hypertensive Patients, and Healthy Control Subjects. JACC Cardiovasc. Imaging 2018, 11, 577–585. [Google Scholar] [CrossRef] [PubMed]
- DeVore, A.D.; McNulty, S.; Alenezi, F.; Ersboll, M.; Vader, J.M.; Oh, J.K.; Lin, G.; Redfield, M.M.; Lewis, G.; Semigran, M.J.; et al. Impaired left ventricular global longitudinal strain in patients with heart failure with preserved ejection fraction: Insights from the RELAX trial. Eur. J. Heart Fail. 2017, 19, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Obokata, M.; Nagata, Y.; Wu, V.C.; Kado, Y.; Kurabayashi, M.; Otsuji, Y.; Takeuchi, M. Direct comparison of cardiac magnetic resonance feature tracking and 2D/3D echocardiography speckle tracking for evaluation of global left ventricular strain. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Hamatani, Y.; Nagai, T.; Shiraishi, Y.; Kohsaka, S.; Nakai, M.; Nishimura, K.; Kohno, T.; Nagatomo, Y.; Asaumi, Y.; Goda, A.; et al. Long-Term Prognostic Significance of Plasma B-Type Natriuretic Peptide Level in Patients With Acute Heart Failure With Reduced, Mid-Range, and Preserved Ejection Fractions. Am. J. Cardiol. 2018, 121, 731–738. [Google Scholar] [CrossRef]
- Guisado-Espartero, M.E.; Salamanca-Bautista, P.; Aramburu-Bodas, O.; Conde-Martel, A.; Arias-Jimenez, J.L.; Llacer-Iborra, P.; Davila-Ramos, M.F.; Cabanes-Hernandez, Y.; Manzano, L.; Montero-Perez-Barquero, M.; et al. Heart failure with mid-range ejection fraction in patients admitted to internal medicine departments: Findings from the RICA Registry. Int. J. Cardiol. 2018, 255, 124–128. [Google Scholar] [CrossRef]
- Lauritsen, J.; Gustafsson, F.; Abdulla, J. Characteristics and long-term prognosis of patients with heart failure and mid-range ejection fraction compared with reduced and preserved ejection fraction: A systematic review and meta-analysis. ESC Heart Fail. 2018, 4, 685–694. [Google Scholar] [CrossRef]
- Choi, K.H.; Lee, G.Y.; Choi, J.O.; Jeon, E.S.; Lee, H.Y.; Cho, H.J.; Lee, S.E.; Kim, M.S.; Kim, J.J.; Hwang, K.K.; et al. Outcomes of de novo and acute decompensated heart failure patients according to ejection fraction. Heart 2018, 104, 525–532. [Google Scholar] [CrossRef]
- Farmakis, D.; Simitsis, P.; Bistola, V.; Triposkiadis, F.; Ikonomidis, I.; Katsanos, S.; Bakosis, G.; Hatziagelaki, E.; Lekakis, J.; Mebazaa, A.; et al. Acute heart failure with mid-range left ventricular ejection fraction: Clinical profile, in-hospital management, and short-term outcome. Clin. Res. Cardiol. 2017, 106, 359–368. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Clinical Data | Control | HFpEF | HFmrEF | HFrEF | |
|---|---|---|---|---|---|
| Female | 8/17 (47%) | 9/17 (53%) | 6/18 (33%) | 3/17 (18%) | |
| Age | Mean ± SD | 61.7 ± 8.5 | 78.1 ± 8.2 | 67.8 ± 9.0 | 64.4 ± 10.3 |
| LVEF | Mean ± SD | 63.8 ± 5.4 | 61.7 ± 6.1 | 44.7 ± 2.9 | 33.1 ± 4.8 |
| LA (cm2) | Mean ± SD | 19.5 ± 6.5 | 23.4 ± 4.9 | 22.8 ± 8.3 | 25.2 ± 6.6 |
| RVEDD (mm) | Mean ± SD | 31.5 ± 4.7 | 30.6 ± 3.8 | 29.6 ± 3.7 | 31.4 ± 5.4 |
| Any LGE | 7/17 (41%) | 16/18 (89%) | 15/17 (88%) | ||
| Transmural LGE | 4/17 (24%) | 7/18 (39%) | 8/17 (47%) | ||
| Coronary Artery Disease | 0/17 (0%) | 11/17 (65%) | 16/18 (89%) | 11/17 (65%) | |
| 6 min Walking Test (m) | Mean ± SD | 524 ± 126 | 345 ± 122 | 414 ± 88 | 414 ± 125 |
| NYHA Class | 2 | 9/17 (53%) | 15/18 (83%) | 12/17 (71%) | |
| 3 | 8/17 (47%) | 3/18 (17%) | 5/16 (29%) | ||
| Quality of Life 1 | Mean ± SD | 5.0 ± 5.9 | 27.3 ± 22.8 | 28.3 ± 22.8 | 28.5 ± 24.9 |
| Borg Score | Mean ± SD | 7.5 ± 1.7 | 12.4 ± 2.4 | 10.67 ± 2.3 | 10.9 ± 2.5 |
| Laboratory Values | |||||
| Hemoglobin (g/dL) | Mean ± SD | 13.9 ± 1.1 | 12.8 ± 1.2 | 13.6 ± 1.1 | 15.0 ± 1.1 |
| Hematocrit | Mean ± SD | 0.40 ± 0.03 | 0.38 ± 0.03 | 0.40 ± 0.03 | 0.43 ± 0.04 |
| Creatinin (mg/dL) | Mean ± SD | 0.87 ± 0.20 | 0.92 ± 0.18 | 1.07 ± 0.33 | 1.09 ± 0.38 |
| GFR (mL/min) | Mean ± SD | 81 ± 10 | 71 ± 16 | 70 ± 18 | 72 ± 21 |
| NT-proBNP (ng/L) | Mean ± SD | 91 ± 62 | 614 ± 607 | 829 ± 1158 | 2257 ± 3447 |
| Troponin T (ng/L) | Mean ± SD | 7 ± 3 | 16 ± 12 | 19 ± 20 | 18 ± 12 |
| CRP (mg/dL) | Mean ± SD | 1.3 ± 1.4 | 2.9 ± 2.7 | 3.0 ± 4.2 | 1.0 ± 0.7 |
| WBC (/nL) | Mean ± SD | 6.1 ± 1.6 | 7.2 ± 2.4 | 8.5 ± 2.4 | 8.4 ± 2.3 |
| Medication | |||||
| ACE-Inhibitors | 2/17 (12%) | 4/17 (24%) | 7/18 (39%) | 9/17 (53%) | |
| Angiotensin-Receptor-Blocker | 4/17 (24%) | 11/17 (65%) | 7/18 (39%) | 8/17 (47%) | |
| Calcium-Antagonist | 4/17 (24%) | 3/17 (18%) | 3/18 (17%) | 1/17 (6%) | |
| Mineralocorticoid-Receptor-Antagonist | 0/17 (0%) | 2/17 (12%) | 4/18 (22%) | 11/17 (65%) | |
| Angiotensin-Receptor-Neprilysin-Inhibitor | 0/17 (0%) | 0/17 (0%) | 0/18 (0%) | 4/17 (24%) | |
| Beta-Blocker | 6/17 (35%) | 10/17 (59%) | 14/18 (78%) | 17/17 (100%) | |
| Statin | 2/17 (12%) | 8/17 (47%) | 15/18 (83%) | 11/17 (65%) | |
| Thiazide Diuretic | 4/17 (24%) | 4/17 (24%) | 2/18 (11%) | 1/17 (6%) | |
| Loop Diuretic | 0/17 (0%) | 3/17 (18%) | 7/18 (39%) | 6/17 (35%) | |
| Heart Failure Group | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | HFpEF | HFmrEF | HFrEF | Controls vs. HFpEF | Controls vs. HFmrEF | HFpEF vs. HFmrEF | HFpEF vs. HFrEF | HFmrEF vs. HFrEF | |
| T2 (ms) | 50.6 ± 2.1 | 52.6 ± 3.6 | 55.4 ± 3.4 | 56.0 ± 6.0 | 0.499 | 0.005 ** | 0.190 | 0.078 | 0.967 |
| T1 native (ms) | 972 ± 31 | 985 ± 32 | 1027 ± 40 | 1033 ± 54 | 0.776 | 0.001 ** | 0.023 * | 0.005 ** | 0.954 |
| ECV (%) | 27 ± 4 † | 27.3 ± 2.6 | 29.2 ± 2.6 | 29.3 ± 3.4 | 0.993 | 0.186 | 0.303 | 0.271 | >0.999 |
| GLS (%) | −23.0 ± 3.5 | −20.8 ± 3.9 | −15.7 ± 2.1 | −11.0 ± 3.6 | 0.252 | <0.001 ** | <0.001 ** | <0.001 ** | <0.001 ** |
| GCS (%) | −34.5 ± 6.2 | −35.8 ± 6.7 | −19.9 ± 4.1 | −12.4 ± 4.6 | 0.902 | <0.001 ** | <0.001 ** | <0.001 ** | 0.001 ** |
| SR | 0.68 ± 0.09 | 0.59 ± 0.11 | 0.82 ± 0.17 | 0.96 ± 0.33 | 0.600 | 0.159 | 0.007 ** | <0.001 ** | 0.151 |
| T2 | ECV | T1 Native | GLS | GCS | SR | LV-EF | ||
|---|---|---|---|---|---|---|---|---|
| ECV | Pearson r | 0.353 ** | ||||||
| p Value | 0.010 | |||||||
| T1 native | Pearson r | 0.660 ** | 0.472 ** | |||||
| p Value | <0.001 | <0.001 | ||||||
| GLS | Pearson r | 0.351 ** | 0.294 * | 0.518 ** | ||||
| p Value | 0.003 | 0.034 | <0.001 | |||||
| GCS | Pearson r | 0.372 ** | 0.256 | 0.484 ** | 0.868 ** | |||
| p Value | 0.002 | 0.067 | <0.001 | <0.001 | ||||
| SR | Pearson r | 0.309 ** | 0.062 | 0.308 ** | 0.353 ** | 0.698 ** | ||
| p Value | 0.009 | 0.663 | 0.010 | 0.003 | <0.001 | |||
| LV-EF | Pearson r | −0.422 ** | −0.242 | −0.518 ** | −0.882 ** | −0.929 ** | −0.614 ** | |
| p Value | <0.001 | 0.090 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| Age | Pearson r | 0.234 | −0.100 | 0.064 | −0.199 | −0.270 * | −0.202 | 0.246 * |
| p Value | 0.052 | 0.483 | 0.603 | 0.095 | 0.023 | 0.091 | 0.020 | |
| log(NT-proBNP) | Pearson r | 0.642 ** | 0.287 * | 0.601 ** | 0.544 ** | 0.544 ** | 0.234 * | −0.538 ** |
| p Value | <0.001 | 0.039 | <0.001 | <0.001 | <0.001 | 0.050 | <0.001 | |
| Glomerular filtration rate | Pearson r | −0.441 ** | 0.106 | −0.123 | −0.065 | −0.057 | −0.054 | 0.085 |
| p Value | <0.001 | 0.455 | 0.314 | 0.589 | 0.637 | 0.655 | 0.487 | |
| C-reactive protein (mg/dL) | Pearson r | 0.105 | −0.154 | −0.006 | −0.044 | −0.087 | −0.112 | 0.062 |
| p Value | 0.393 | 0.281 | 0.961 | 0.715 | 0.473 | 0.357 | 0.614 | |
| Hematocrit | Pearson r | 0.101 | −0.180 | 0.150 | 0.330 ** | 0.405 ** | 0.343 ** | −0.471 ** |
| p Value | 0.407 | 0.201 | 0.219 | 0.005 | <0.001 | 0.003 | <0.001 | |
| 6 min walking test | Pearson r | −0.345 ** | 0.273 | -0.150 | −0.102 | 0.014 | 0.138 | 0.037 |
| p Value | 0.004 | 0.055 | 0.224 | 0.403 | 0.912 | 0.258 | 0.765 | |
| Quality of life | Spearman r | 0.484 ** | 0.187 | 0.359 ** | 0.184 | 0.168 | 0.097 | −0.230 |
| p Value | <0.001 | 0.185 | 0.002 | 0.124 | 0.162 | 0.420 | 0.058 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doeblin, P.; Hashemi, D.; Tanacli, R.; Lapinskas, T.; Gebker, R.; Stehning, C.; Motzkus, L.A.; Blum, M.; Tahirovic, E.; Dordevic, A.; et al. CMR Tissue Characterization in Patients with HFmrEF. J. Clin. Med. 2019, 8, 1877. https://doi.org/10.3390/jcm8111877
Doeblin P, Hashemi D, Tanacli R, Lapinskas T, Gebker R, Stehning C, Motzkus LA, Blum M, Tahirovic E, Dordevic A, et al. CMR Tissue Characterization in Patients with HFmrEF. Journal of Clinical Medicine. 2019; 8(11):1877. https://doi.org/10.3390/jcm8111877
Chicago/Turabian StyleDoeblin, Patrick, Djawid Hashemi, Radu Tanacli, Tomas Lapinskas, Rolf Gebker, Christian Stehning, Laura Astrid Motzkus, Moritz Blum, Elvis Tahirovic, Aleksandar Dordevic, and et al. 2019. "CMR Tissue Characterization in Patients with HFmrEF" Journal of Clinical Medicine 8, no. 11: 1877. https://doi.org/10.3390/jcm8111877