Analysis of Pulse Arrival Time as an Indicator of Blood Pressure in a Large Surgical Biosignal Database: Recommendations for Developing Ubiquitous Blood Pressure Monitoring Methods


Abstract
:1. Introduction
2. Methods
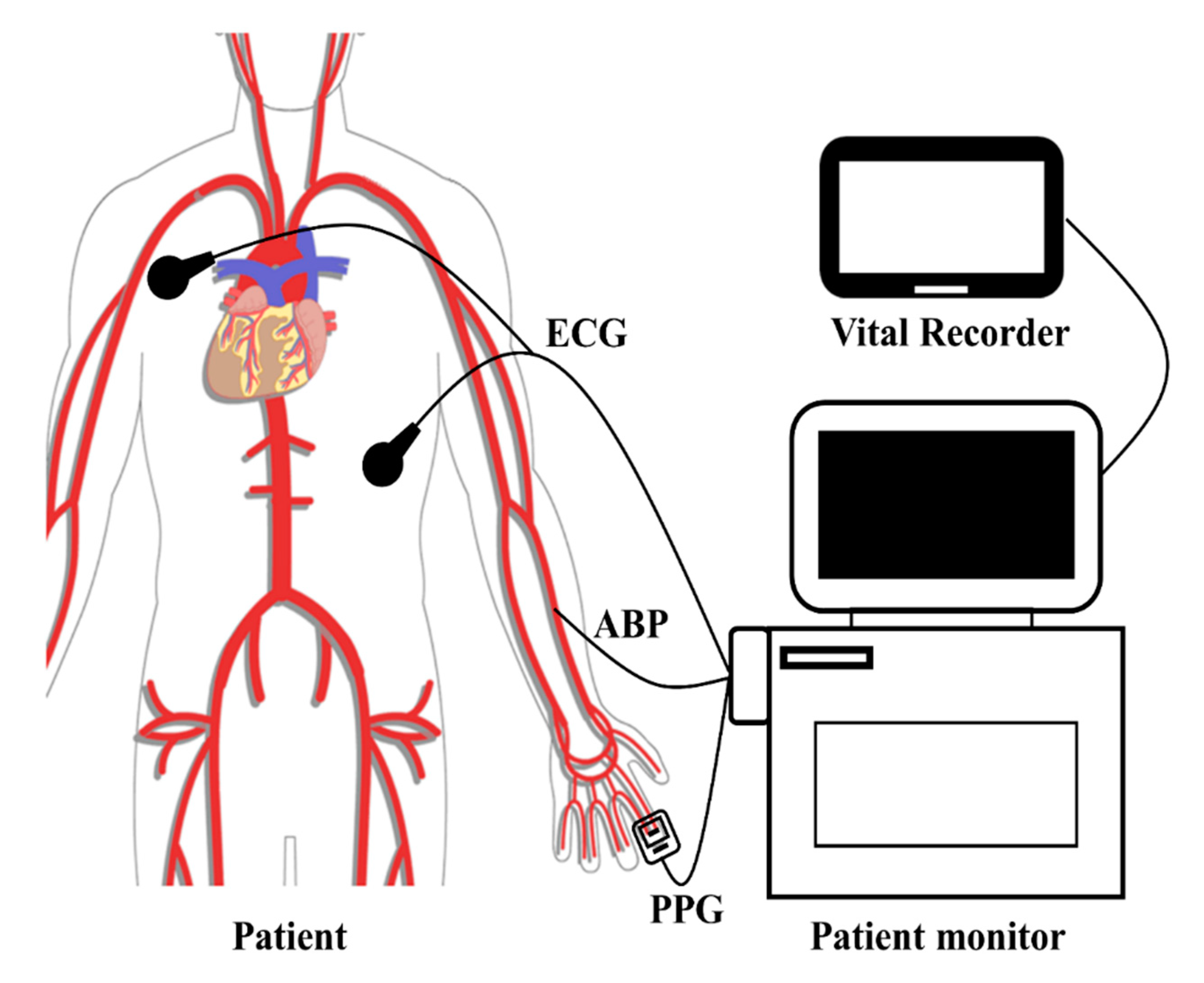
2.1. VitalDB Database
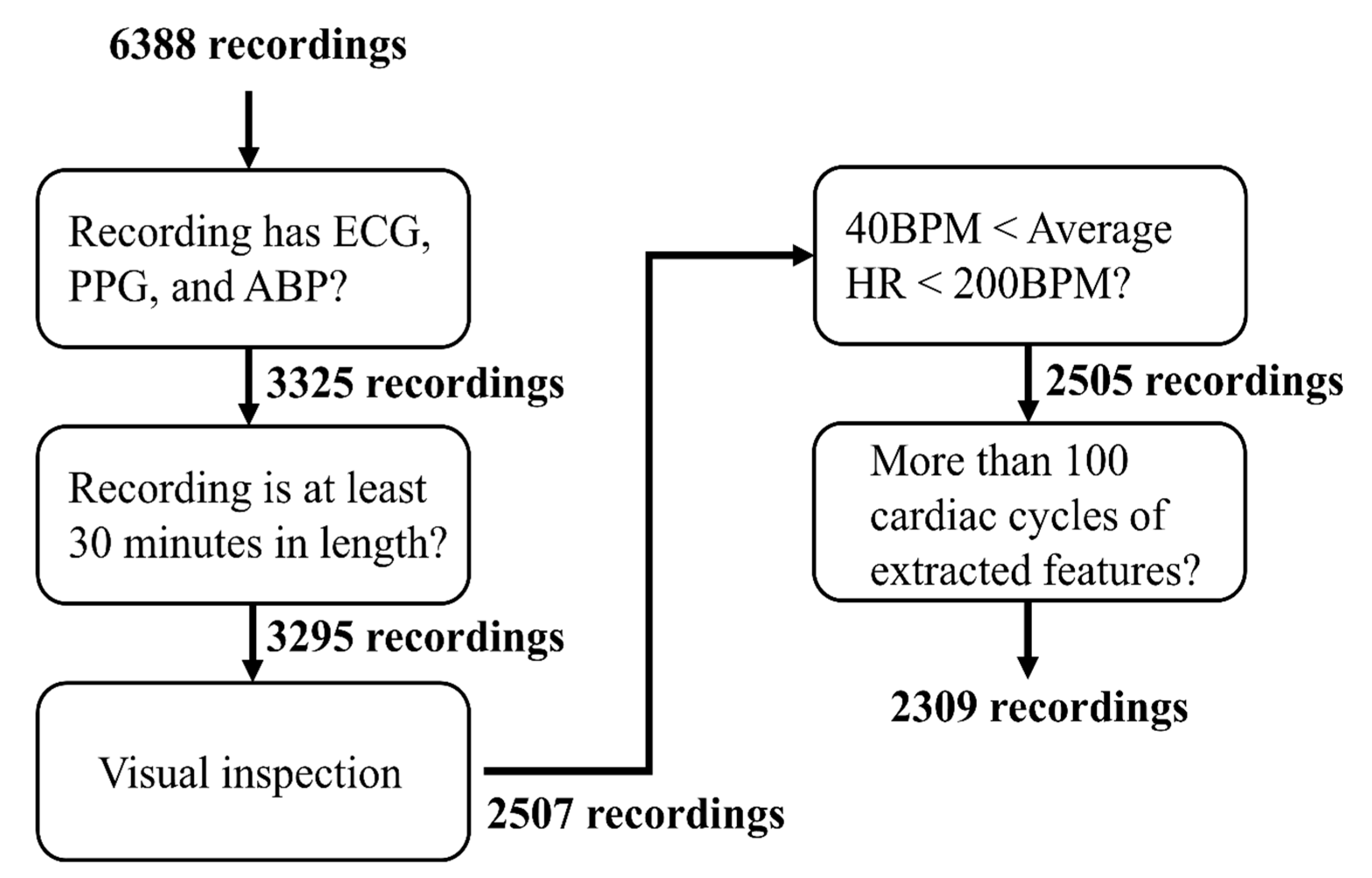
2.2. Data Selection
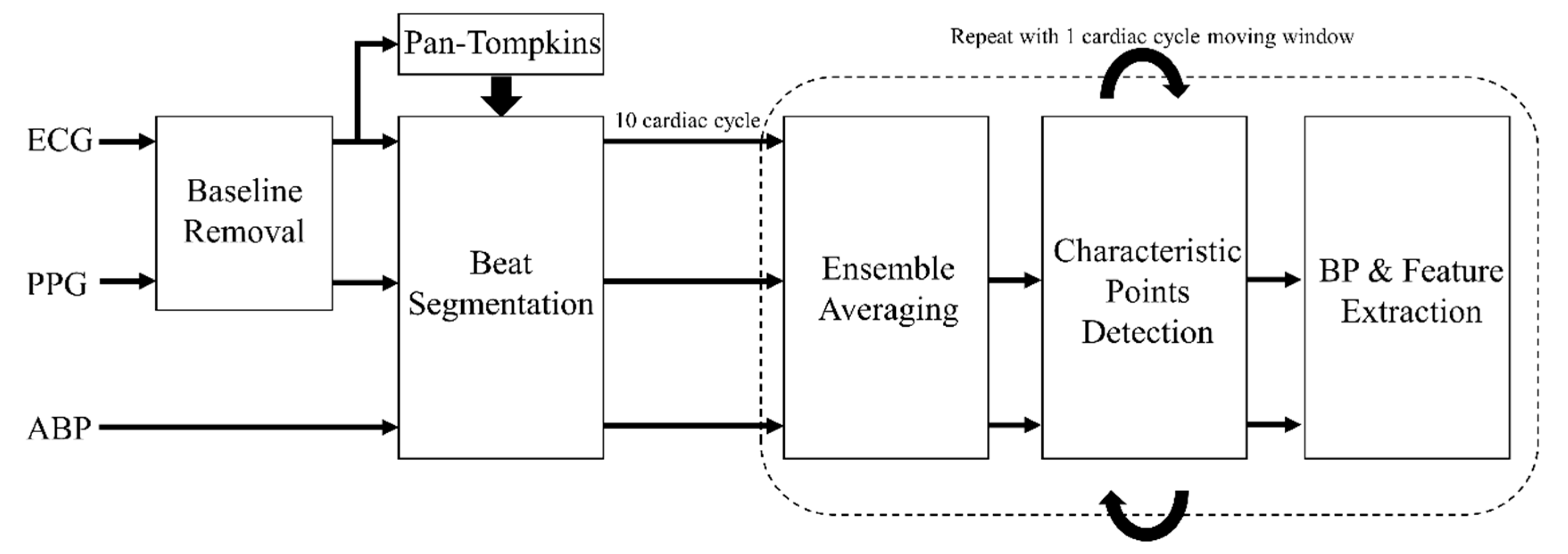
2.3. Pre-Processing and Feature Extraction
- Is the extracted SBP greater than 50 mmHg and less than 250 mmHg?
- Is the extracted DBP greater than 30 mmHg and less than 160 mmHg?
- Is the extracted PP greater than 10 mmHg?
- Is the change in the extracted BP (SBP or DBP) during the previous 5 s interval less than 30 mmHg?
- Is the extracted PATABP greater than 70 ms and less than 250 ms?
- Is the change in the extracted features (PAT or PTT) during the previous 5 s interval less than 300 ms?
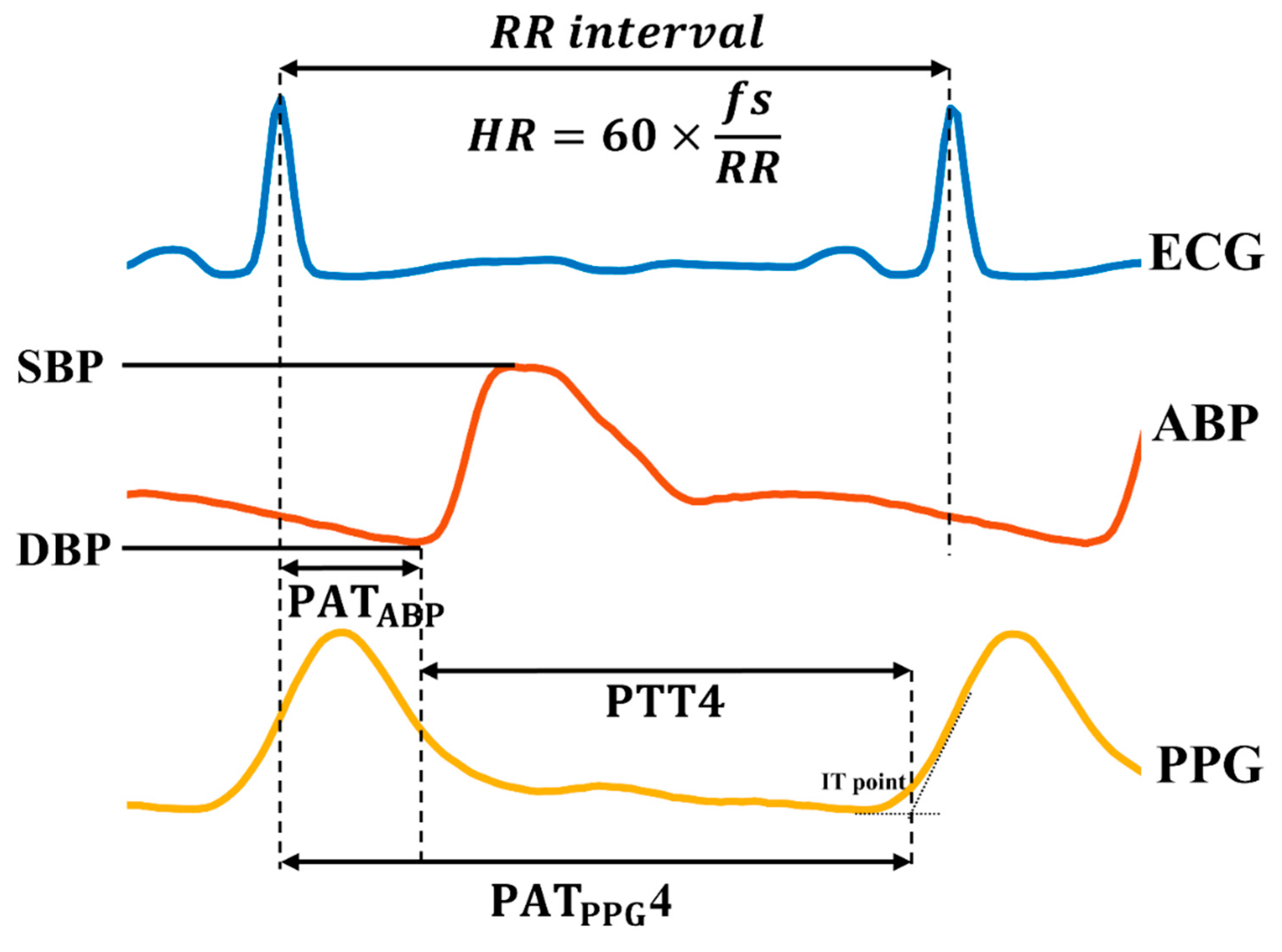
2.4. Feature Analysis
3. Results
4. Discussion
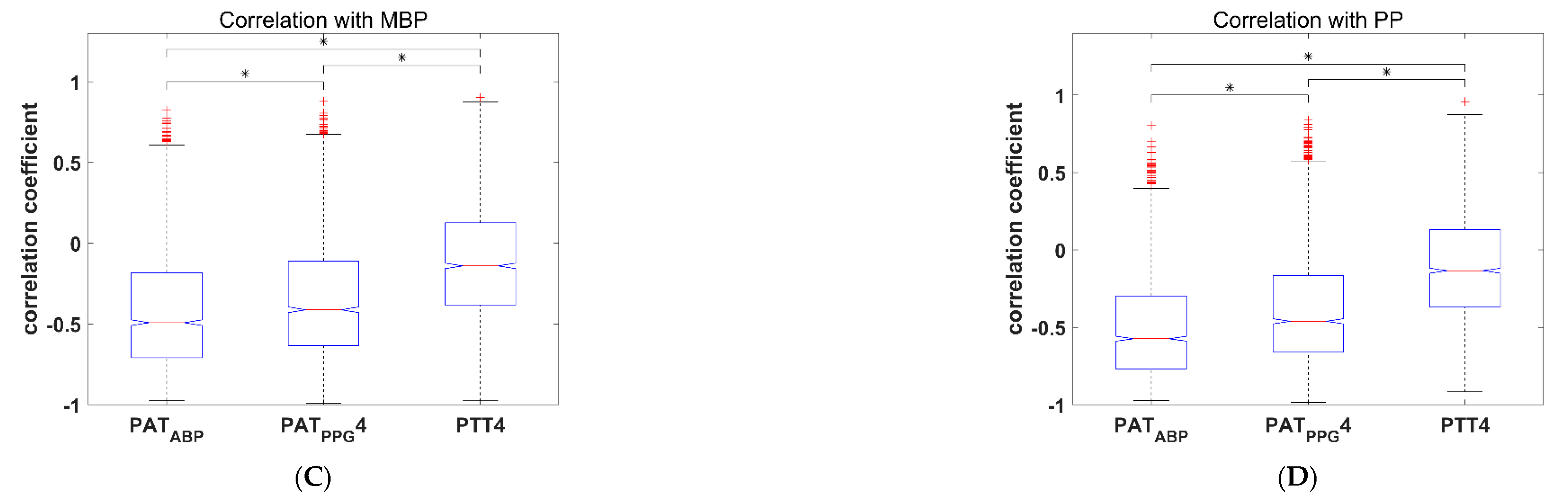
4.1. Pulse Arrival Time Versus Pulse Transit Time: Implications for Practical NCBPM
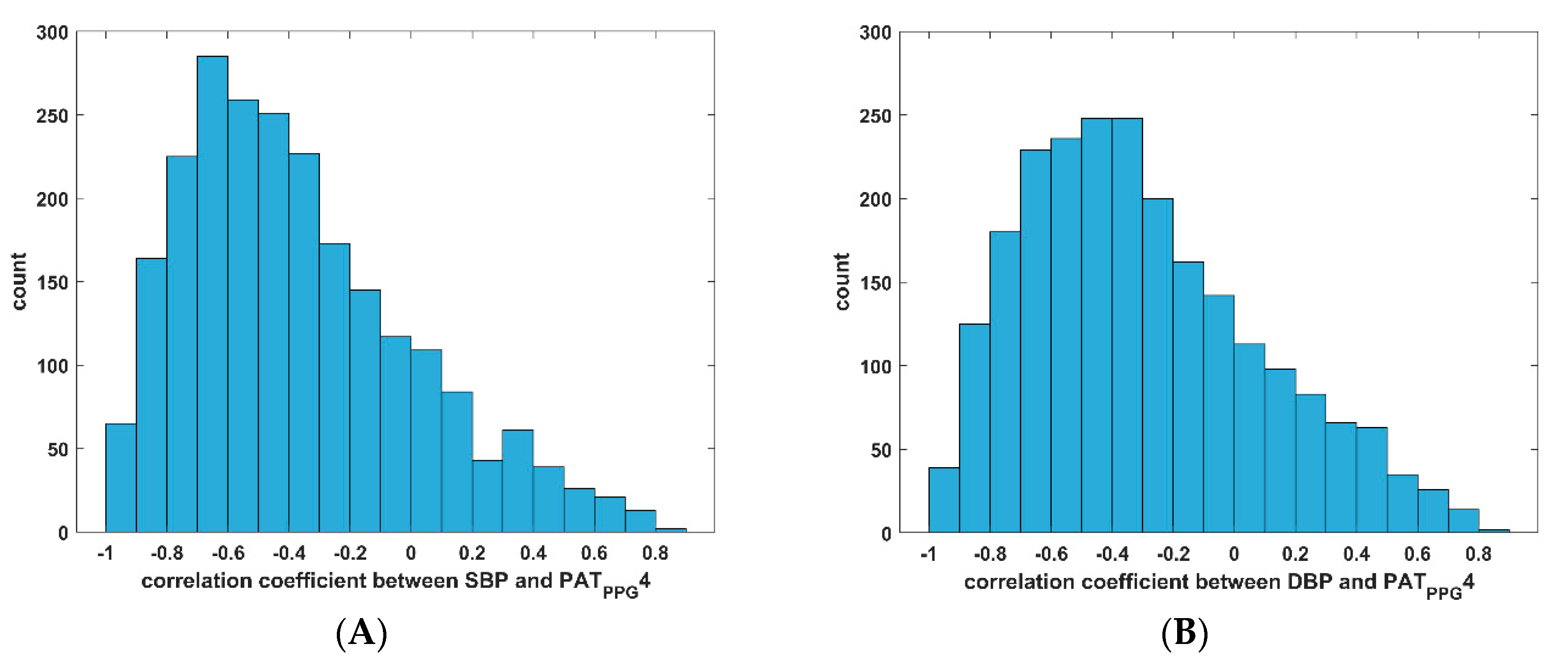
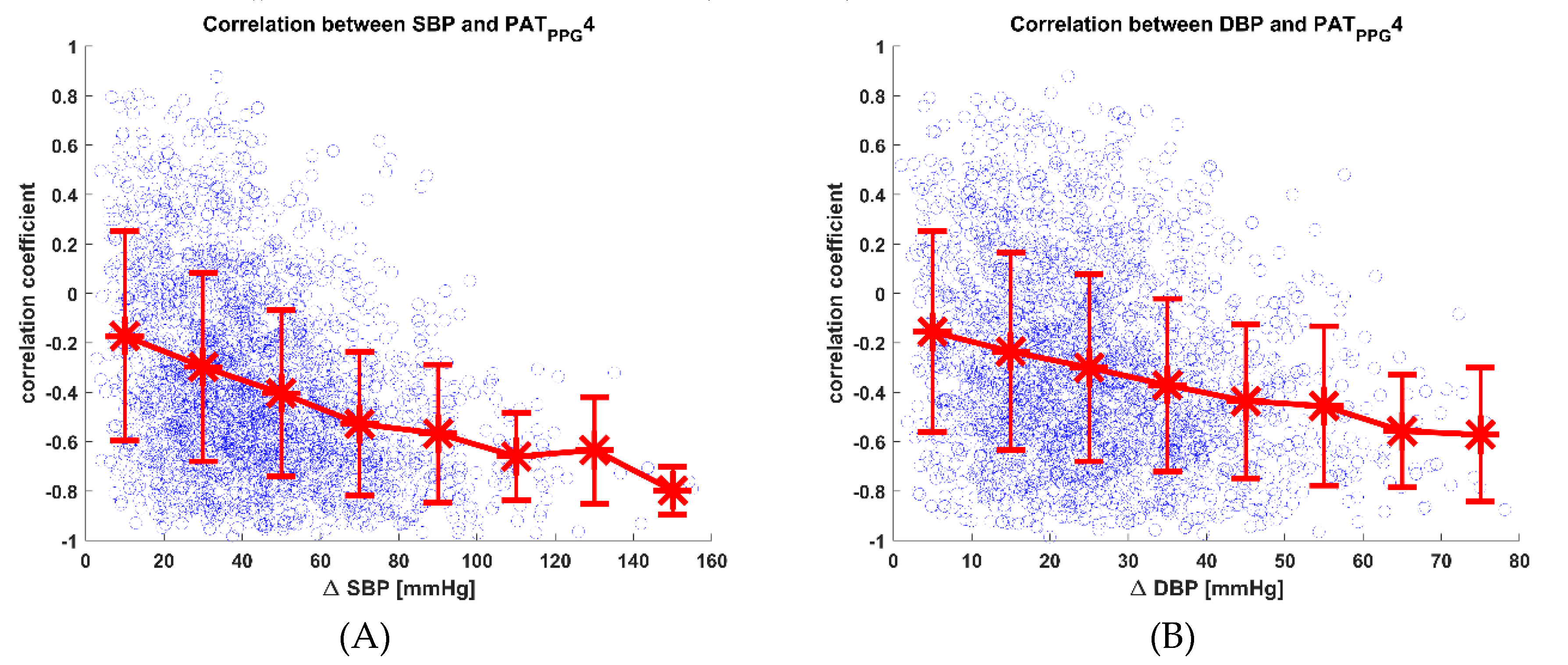
4.2. Variability of PAT-BP Relationship
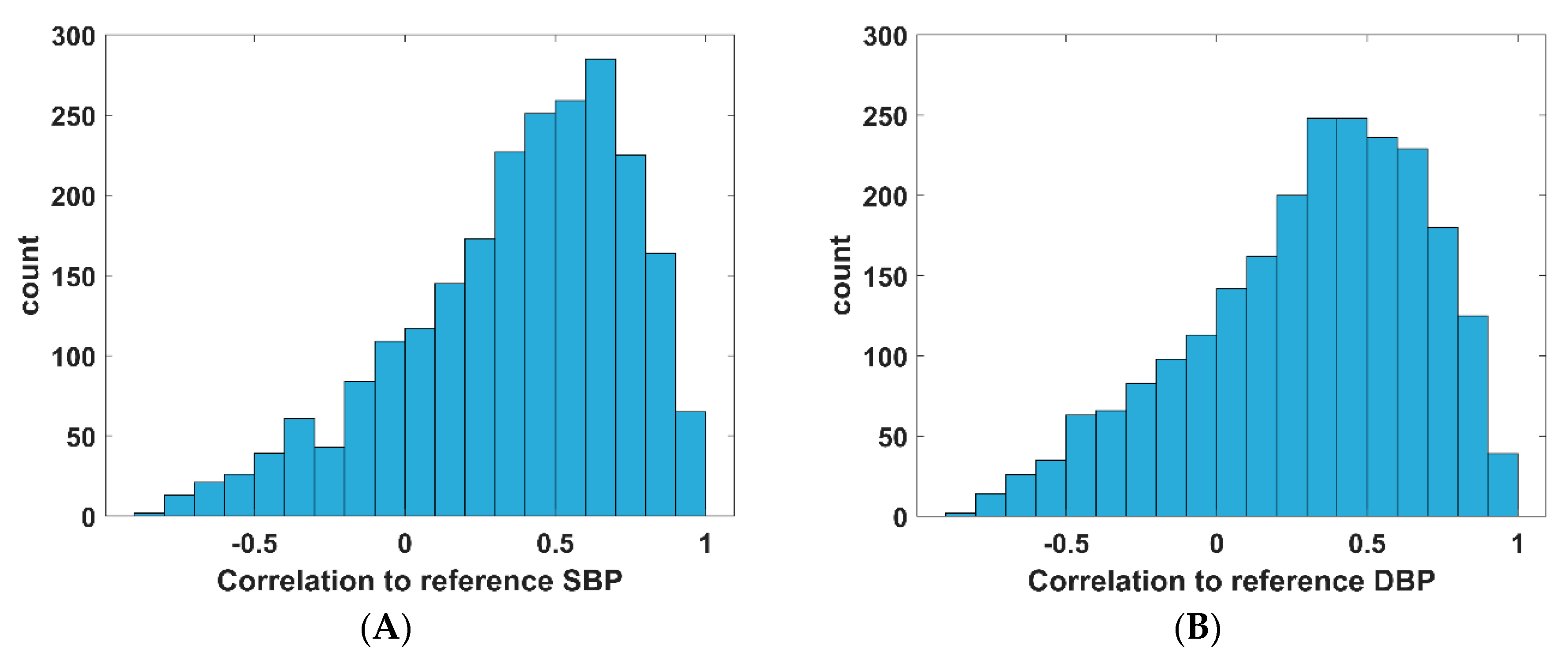
4.3. PAT as a Predictor of BP in Ubiquitous NCBPM
4.4. Shortcomings of Current BP Monitor Standards with Regards to Beat-by-Beat NCBPM
4.5. Large Datasets for BP Estimation Model Development
4.6. Limitations
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Cardiovascular Diseases; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Flebach, N.H.; Hebert, P.R.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C.; Rosner, B.; Spelzer, F.E.; Hennekens, C.H. A prospective study of high blood pressure and cardiovascular disease in women. Am. J. Epidemiol. 1989, 130, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Mac Mahon, S.; Peto, R.; Collins, R.; Godwin, J.; MacMahon, S.; Cutler, J.; Sorlie, P.; Abbott, R.; Collins, R.; Neaton, J.; et al. Blood pressure, stroke, and coronary heart disease: Part 1, prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet 1990, 335, 765–774. [Google Scholar] [CrossRef]
- World Health Organization (WHO). A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis: World Health Day 2013; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Stamler, J.; Stamler, R.; Neaton, J.D. Blood pressure, systolic and diastolic, and cardiovascular risks: Us population data. Arch. Inter. Med. 1993, 153, 598–615. [Google Scholar] [CrossRef]
- Whelton, P.K. Epidemiology of hypertension. Lancet 1994, 344, 101–106. [Google Scholar] [CrossRef]
- Whelton, P.K.; Perneger, T.V.; Brancati, F.L.; Klag, M.J. Epidemiology and prevention of blood pressure-related renal disease. J. Hypertens. 1992, 10, S85. [Google Scholar] [CrossRef]
- Burt, V.L.; Whelton, P.; Roccella, E.J.; Brown, C.; Cutler, J.A.; Higgins, M.; Horan, M.J.; Labarthe, D. Prevalence of hypertension in the US adult population. Results from the third national health and nutrition examination survey, 1988-1991. Hypertension 1995, 25, 305–313. [Google Scholar] [CrossRef]
- Armitage, P.; Rose, G.A. The variability of measurements of casual blood pressure. I. A laboratory study. Clin. Sci. 1966, 30, 325–335. [Google Scholar]
- Pickering, T.G.; Harshfield, G.A.; Devereux, R.B.; Laragh, J.H. What is the role of ambulatory Blood Press. Monitor. in the management of hypertensive patients? Hypertension 1985, 7, 171–177. [Google Scholar] [CrossRef]
- Frattola, A.; Parati, G.; Cuspidi, C.; Albini, F.; Mancia, G. Prognostic value of 24-hour blood pressure variability. J. Hypertens. 1993, 11, 1133–1137. [Google Scholar] [CrossRef]
- Verdecchia, P.; Porcellati, C.; Schillaci, G.; Borgioni, C.; Ciucci, A.; Battistelli, M.; Guerrieri, M.; Gatteschi, C.; Zampi, I.; Santucci, A. Ambulatory blood pressure. An independent predictor of prognosis in essential hypertension. Hypertension 1994, 24, 793–801. [Google Scholar] [CrossRef]
- Shinagawa, M.; Otsuka, K.; Murakami, S.; Kubo, Y.; Cornelissen, G.; Matsubayashi, K.; Yano, S.; Mitsutake, G.; Yasaka, K.-I.; Halberg, F. Seven-day (24-h) ambulatory Blood Press. Monitor., self-reported depression and quality of life scores. Blood Press. Monitor. 2002, 7, 69–76. [Google Scholar] [CrossRef]
- Walker, S.P.; Permezel, M.J.; Brennecke, S.P.; Tuttle, L.K.; Higgins, J.R. Patient satisfaction with the SpaceLabs 90207 ambulatory blood pressure monitor in pregnancy. Hypertens. Pregnancy 2004, 23, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, V.; Dantu, R.; Jonnada, S.; Thiyagaraja, S.; Subbu, K.P. cuffless differential blood pressure estimation using smart phones. IEEE Trans. Biomed. Eng. 2013, 60, 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Kobayashi, T.; Ichikawa, S.; Takeuchi, Y.; Togawa, T. Continuous estimation of systolic blood pressure using the pulse arrival time and intermittent calibration. Med. Biol. Eng. Comput. 2000, 38, 569–574. [Google Scholar] [CrossRef]
- Geddes, L.A.; Voelz, M.H.; Babbs, C.F.; Bourland, J.D.; Tacker, W.A. Pulse transit time as an indicator of arterial blood pressure. Psychophysiology 1981, 18, 71–74. [Google Scholar] [CrossRef]
- Gesche, H.; Grosskurth, D.; Küchler, G.; Patzak, A. Continuous blood pressure measurement by using the pulse transit time: Comparison to a cuff-based method. Eur. J. Appl. Physiol. 2012, 112, 309–315. [Google Scholar] [CrossRef]
- Jae Hyuk, S.; Kang Moo, L.; Kwang Suk, P. Non-constrained monitoring of systolic blood pressure on a weighing scale. Physiol. Meas. 2009, 30, 679. [Google Scholar]
- Parry, F.; Dumont, G.; Ries, C.; Mott, C.; Ansermino, M. Continuous Noninvasive Blood Pressure Measurement by Pulse Transit Time. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; pp. 738–741. [Google Scholar]
- Poon, C.C.Y.; Zhang, Y.T. Cuff-less and Noninvasive Measurements of Arterial Blood Pressure by Pulse Transit Time. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shangai, China, 17–18 January 2006; pp. 5877–5880. [Google Scholar]
- Solà, J.; Proença, M.; Ferrario, D.; Porchet, J.A.; Falhi, A.; Grossenbacher, O.; Allemann, Y.; Rimoldi, S.F.; Sartori, C. Noninvasive and nonocclusive blood pressure estimation via a chest sensor. IEEE Trans. Biomed. Eng. 2013, 60, 3505–3513. [Google Scholar] [CrossRef]
- Winokur, E.S.; He, D.D.; Sodini, C.G. A Wearable Vital Signs Monitor at the Ear for Continuous Heart Rate and Pulse Transit Time Measurements. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 2724–2727. [Google Scholar]
- Wong, M.Y.-M.; Poon, C.C.-Y.; Zhang, Y.-T. An evaluation of the cuffless blood pressure estimation based on pulse transit time technique: A half year study on normotensive subjects. Cardiovasc. Eng. 2009, 9, 32–38. [Google Scholar] [CrossRef]
- Bramwell, J.C. The velocity of pulse wave in man. Proc. R Soc. Lond. B 1922, 93, 298–306. [Google Scholar] [CrossRef] [Green Version]
- Nichols, W.E.A. McDonald’s Blood Flow in Arteries. Theoretical, Experimental and Clinical Principles, 6th ed.; Taylor & Francis: London, UK, 2011. [Google Scholar]
- Mukkamala, R.; Hahn, J.O.; Inan, O.T.; Mestha, L.K.; Kim, C.S.; Töreyin, H.; Kyal, S. Toward ubiquitous blood pressure monitoring via pulse transit time: Theory and practice. IEEE Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef] [PubMed]
- Puke, S.; Suzuki, T.; Nakayama, K.; Tanaka, H.; Minami, S. Blood pressure estimation from pulse wave velocity measured on the chest. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 6107–6110. [Google Scholar]
- Kim, C.-S.; Ober, S.L.; McMurtry, M.S.; Finegan, B.A.; Inan, O.T.; Mukkamala, R.; Hahn, J.-O. Ballistocardiogram: Mechanism and potential for unobtrusive cardiovascular health monitoring. Sci. Rep. 2016, 6, 31297. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Carek, A.M.; Inan, O.T.; Mukkamala, R.; Hahn, J. Ballistocardiogram-Based approach to cuffless blood pressure monitoring: Proof of concept and potential challenges. IEEE Trans. Biomed. Eng. 2018, 65, 2384–2391. [Google Scholar] [CrossRef]
- Proença, J.; Muehlsteff, J.; Aubert, X.; Carvalho, P. Is Pulse Transit Time a Good Indicator of Blood Pressure Changes during Short Physical Exercise in a Young Population? In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 21 August–4 September 2010; pp. 598–601. [Google Scholar]
- Peter, L.; Noury, N.; Cerny, M. A review of methods for non-invasive and continuous blood pressure monitoring: Pulse transit time method is promising? IRBM 2014, 35, 271–282. [Google Scholar] [CrossRef]
- Tang, Z.; Tamura, T.; Sekine, M.; Huang, M.; Chen, W.; Yoshida, M.; Sakatani, K.; Kobayashi, H.; Kanaya, S. A chair-based unobtrusive cuffless blood pressure monitoring system based on pulse arrival time. IEEE J. Biomed. Health Inf. 2017, 21, 1194–1205. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Spiesshoefer, J.; Brix, T.; Tuleta, I.; Mohr, M.; Emdin, M.; Boentert, M.; Giannoni, A. Validity of transit time–based blood pressure measurements in patients with and without heart failure or pulmonary arterial hypertension across different breathing maneuvers. Sleep Breath. 2019. [Google Scholar] [CrossRef]
- Choi, Y.; Zhang, Q.; Ko, S. Noninvasive cuffless blood pressure estimation using pulse transit time and Hilbert–Huang transform. Comput. Electr. Eng. 2013, 39, 103–111. [Google Scholar] [CrossRef]
- Ruiz-Rodríguez, J.C.; Ruiz-Sanmartín, A.; Ribas, V.; Caballero, J.; García-Roche, A.; Riera, J.; Nuvials, X.; de Nadal, M.; de Sola-Morales, O.; Serra, J.; et al. Innovative continuous non-invasive cuffless blood pressure monitoring based on photoplethysmography technology. Intensive Care Med. 2013, 39, 1618–1625. [Google Scholar] [CrossRef]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuffless blood pressure estimation algorithms for continuous health-care monitoring. IEEE Trans. Biomed. Eng. 2017, 64, 859–869. [Google Scholar] [CrossRef]
- Lo, F.P.-W.; Li, C.X.-T.; Wang, J.; Cheng, J.; Meng, M.Q.-H. Continuous systolic and diastolic blood pressure estimation utilizing long short-term memory network. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Korea, 11–15 July 2017; pp. 1853–1856. [Google Scholar]
- Wang, L.; Zhou, W.; Xing, Y.; Zhou, X. A novel neural network model for blood pressure estimation using photoplethesmography without electrocardiogram. J. Healthcare Eng. 2018. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.-K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet. Compon. N. Res. Resour. Complex Physiol. Signals 2000, 101, e215–e220. [Google Scholar] [CrossRef]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Li-Wei, H.L.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.; Abbott, D.; Howard, N.; Lim, K.; Ward, R.; Elgendi, M. How effective is pulse arrival time for evaluating blood pressure? Challenges and recommendations from a study using the MIMIC database. J. Clin. Med. 2019, 8, 337. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-C.; Jung, C.-W. Vital Recorder-a free research tool for automatic recording of high-resolution time-synchronised physiological data from multiple anaesthesia devices. Sci. Rep. 2018, 8, 1527. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Łęski, J.M.; Henzel, N. ECG baseline wander and powerline interference reduction using nonlinear filter bank. Signal Proc. 2005, 85, 781–793. [Google Scholar] [CrossRef]
- Gaddum, N.; Alastruey, J.; Beerbaum, P.; Chowienczyk, P.; Schaeffter, T. A technical assessment of pulse wave velocity algorithms applied to non-invasive arterial waveforms. Ann. Biomed. Eng. 2013, 41, 2617–2629. [Google Scholar] [CrossRef]
- Tavakolian, K. Characterization and Analysis of Seismocardiogram for Estimation of Hemodynamic Parameters. Ph.D. Thesis, Simon Fraser University, Burnaby, BC, Canada, 2010. [Google Scholar]
- The Association for the Advancement of Medical Instrumentation. American national standard. In Electronic or Automated Sphygmomanometers; ANSI/AAMI SP10-1992/A1; ANSI: New York, NY, USA, 1996. [Google Scholar]
- O’Brien, E.; Petrie, J.; Littler, W.; de Swiet, M.; Padfield, P.L.; Altman, D.; Bland, M.; Coats, A.; Atkins, N. The british hypertension society protocol for the evaluation of blood pressure measuring devices. J. Hypertens. 1993, 11, S43–S62. [Google Scholar]
- International Standardization Association. IEEE standard for wearable cuffless blood pressure measuring devices. IEEE Std. 2014, 1708–2014. [Google Scholar] [CrossRef]
- Muehlsteff, J.; Aubert, X.L.; Schuett, M. Cuffless Estimation of Systolic Blood Pressure for Short Effort Bicycle Tests: The Prominent Role of the Pre-Ejection Period. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 5088–5092. [Google Scholar]
- Payne, R.A.; Symeonides, C.N.; Webb, D.J.; Maxwell, S.R.J. Pulse transit time measured from the ECG: An unreliable marker of beat-to-beat blood pressure. J. Appl. Physiol. 2006, 100, 136–141. [Google Scholar] [CrossRef]
- Zhang, G.; Gao, M.; Xu, D.; Olivier, N.B.; Mukkamala, R. Pulse arrival time is not an adequate surrogate for pulse transit time as a marker of blood pressure. J. Appl. Physiol. 2011, 111, 1681–1686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngim, C.; Abdul, A.R.; Ibrahim, A. Pulse wave velocity as an index of arterial stiffness: A comparison between newly diagnosed (untreated) hypertensive and normotensive middle-aged Malay men and its relationship with fasting insulin. Acta Cardiologica 1999, 54, 277–282. [Google Scholar] [PubMed]
- Emura, S.; Takashima, T.; Ohmori, K. Risk factors of atherosclerosis and aortic pulse wave velocity. Angiology 2000, 51, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Amar, J.; Ruidavets, J.B.; Chamontin, B.; Drouet, L.; Ferrières, J. Arterial stiffness and cardiovascular risk factors in a population-based study. J. Hypertens. 2001, 19, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Park, C.G.; Park, J.; Suh, S.; Choi, C.U.; Kim, J.W.; Kim, S.; Lim, H.E.; Rha, S.-W.; Seo, H.S. Relationship between blood pressure parameters and pulse wave velocity in normotensive and hypertensive subjects: Invasive study. J. Hum. Hypertens. 2007, 21, 141. [Google Scholar] [CrossRef] [PubMed]
- White, W.B.; Schulman, P.; McCabe, E.J.; Dey, H.M. Average daily blood pressure, not office blood pressure, determines cardiac function in patients with hypertension. Jama 1989, 261, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Wiinberg, N.; Høegholm, A.; Christensen, H.R.; Bang, L.E.; Mikkelsen, K.L.; Nielsen, P.E.; Svendsen, T.L.; Kampmann, J.P.; Madsen, N.H.; Bentzon, M.W. 24-h ambulatory blood pressure in 352 normal Danish subjects, related to age and gender. Am. J. Hypertens. 1995, 8, 978–986. [Google Scholar] [CrossRef]
- Omboni, S.; Parati, G.; Castiglioni, P.; Di Rienzo, M.; Imholz, B.P.; Langewouters, G.J.; Wesseling, K.H.; Mancia, G. Estimation of blood pressure variability from 24-hour ambulatory finger blood pressure. Hypertension 1998, 32, 52–58. [Google Scholar] [CrossRef]
- Feng, J.; Huang, Z.; Zhou, C.; Ye, X. Study of continuous blood pressure estimation based on pulse transit time, heart rate and photoplethysmography-derived hemodynamic covariates. Australas. Phys. Eng. Sci. Med. 2018, 41, 403–413. [Google Scholar] [CrossRef]
- Huang, J.-J.; Syu, H.-Y.; Cai, Z.-L.; See, A.R. Development of a long term dynamic Blood Press. Monitor. system using cuff-less method and pulse transit time. Measurement 2018, 124, 309–317. [Google Scholar] [CrossRef]
- Huynh, T.H.; Jafari, R.; Chung, W.-Y. Noninvasive cuffless blood pressure estimation using pulse transit time and impedance plethysmography. IEEE Trans. Biomed. Eng. 2018, 66, 967–976. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Sohn, J.; Park, J.; Yang, S.; Lee, S.; Kim, H.C. Novel blood pressure and pulse pressure estimation based on pulse transit time and stroke volume approximation. Biomed. Eng. Online 2018, 17, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasool, A.; Rafiq, M.; Nasir, A.; Kashif, F.M. Continuous and Noninvasive Blood Pressure Estimation by Two-Sensor Measurement of Pulse Transit Time. In Proceedings of the 2018 14th International Conference on Emerging Technologies (ICET), Islamabad, Pakistan, 21–22 November 2018; pp. 1–5. [Google Scholar]
- Wang, Y.; Liu, Z.; Ma, S. Cuff-less blood pressure measurement from dual-channel photoplethysmographic signals via peripheral pulse transit time with singular spectrum analysis. Physiol. Meas. 2018, 39, 025010. [Google Scholar] [CrossRef]
- Hietanen, E. Cardiovascular responses to static exercise. Scand. J. Work Environ. Health 1984, 10, 397–402. [Google Scholar] [CrossRef]
- Haennel, R.G.; Snydmiller, G.D.; Teo, K.K.; Greenwood, P.V.; Quinney, H.A.; Kappagoda, C.T. Changes in blood pressure and cardiac output during maximal isokinetic exercise. Arch. Phys. Med. Rehab 1992, 73, 150–155. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Subjects (N = 2309) |
|---|---|
| Age (yrs) | 58 ± 15 (range 5–92) |
| Gender (male) | 1218 (53%) |
| Height (cm) | 162 ± 9 |
| Weight (kg) | 61 ± 12 |
| BMI (kg/m2) | 23 ± 4 |
| Hypertension | 777 (34%) |
| Diabetes | 262 (11%) |
| Arrhythmia | 13 (1%) |
| # of features | 2935 ± 2226 |
| SBP | |
| Mean value (mmHg) | 116 ± 15 |
| value * (mmHg) | 44 ± 23 |
| DBP | |
| Mean value (mmHg) | 63 ± 10 |
| value * (mmHg) | 26 ± 13 |
| MBP | |
| Mean value (mmHg) | 82 ± 11 |
| value * (mmHg) | 33 ± 17 |
| PP | |
| Mean value (mmHg) | 54 ± 12 |
| value * (mmHg) | 25 ± 14 |
| PATABP | PATPPG1 | PATPPG2 | PATPPG3 | PATPPG4 | PTT1 | PTT2 | PTT3 | PTT4 | |
|---|---|---|---|---|---|---|---|---|---|
| SBP | −0.46 ± 0.35 | −0.22 ± 0.40 | −0.24 ± 0.43 | −0.35 ± 0.36 | −0.37 ± 0.37 | −0.04 ± 0.39 | −0.01 ± 0.41 | −0.11 ± 0.36 | −0.12±0.37 |
| DBP | −0.35 ± 0.38 | −0.18 ± 0.40 | −0.19 ± 0.42 | −0.28 ± 0.37 | −0.30 ± 0.38 | −0.05 ± 0.38 | −0.01 ± 0.40 | −0.10 ± 0.36 | −0.11±0.37 |
| MBP | −0.42 ± 0.36 | −0.21 ± 0.40 | −0.21 ± 0.43 | −0.32 ± 0.37 | −0.34 ± 0.38 | −0.05 ± 0.39 | −0.01 ± 0.40 | −0.11 ± 0.36 | −0.12±0.37 |
| PP | −0.50 ± 0.34 | −0.23 ± 0.39 | −0.25 ± 0.42 | −0.36 ± 0.35 | −0.39 ± 0.37 | −0.04 ± 0.38 | −0.01 ± 0.40 | −0.11 ± 0.35 | −0.11±0.36 |
| Performance Measure | SBP | DBP |
|---|---|---|
| Correlation to reference | 0.37 ± 0.37 | 0.30 ± 0.38 |
| ME (mmHg) | <0.001 | <0.001 |
| SDE (mmHg) | 11.04 | 6.25 |
| Cumulative Error < 5 mmHg (%) | 41.6 | 65.7 |
| Cumulative Error < 10 mmHg (%) | 69.7 | 89.8 |
| Cumulative Error < 15 mmHg (%) | 85.0 | 97.0 |
| MAD (mmHg) | 8.21 | 4.58 |
| Slope between PATPPG4 and SBP | Correlation between PATPPG4 and SBP | |||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | P-Value | VIF | β | SE | P-Value | VIF | |
| Age | −0.004 | 0.001 | 0.000 * | 1.145 | −0.001 | 0.001 | 0.165 | 1.145 |
| Gender | −0.016 | 0.020 | 0.411 | 1.015 | −0.014 | 0.016 | 0.370 | 1.015 |
| BMI | 0.001 | 0.003 | 0.812 | 1.032 | 0.001 | 0.002 | 0.722 | 1.032 |
| Hypertension | −0.017 | 0.022 | 0.442 | 1.157 | −0.003 | −0.004 | 0.860 | 1.157 |
| Diabetes | −0.034 | 0.031 | 0.281 | 1.041 | −0.03 | −0.025 | 0.233 | 1.041 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Yang, S.; Lee, S.; Kim, H.C. Analysis of Pulse Arrival Time as an Indicator of Blood Pressure in a Large Surgical Biosignal Database: Recommendations for Developing Ubiquitous Blood Pressure Monitoring Methods. J. Clin. Med. 2019, 8, 1773. https://doi.org/10.3390/jcm8111773
Lee J, Yang S, Lee S, Kim HC. Analysis of Pulse Arrival Time as an Indicator of Blood Pressure in a Large Surgical Biosignal Database: Recommendations for Developing Ubiquitous Blood Pressure Monitoring Methods. Journal of Clinical Medicine. 2019; 8(11):1773. https://doi.org/10.3390/jcm8111773
Chicago/Turabian StyleLee, Joonnyong, Seungman Yang, Saram Lee, and Hee Chan Kim. 2019. "Analysis of Pulse Arrival Time as an Indicator of Blood Pressure in a Large Surgical Biosignal Database: Recommendations for Developing Ubiquitous Blood Pressure Monitoring Methods" Journal of Clinical Medicine 8, no. 11: 1773. https://doi.org/10.3390/jcm8111773