Phasic Left Atrial Function in Cancer Patients Before Initiation of Anti-Cancer Therapy

Abstract
:1. Introduction
2. Methodology
2.1. Population
2.2. Echocardiography
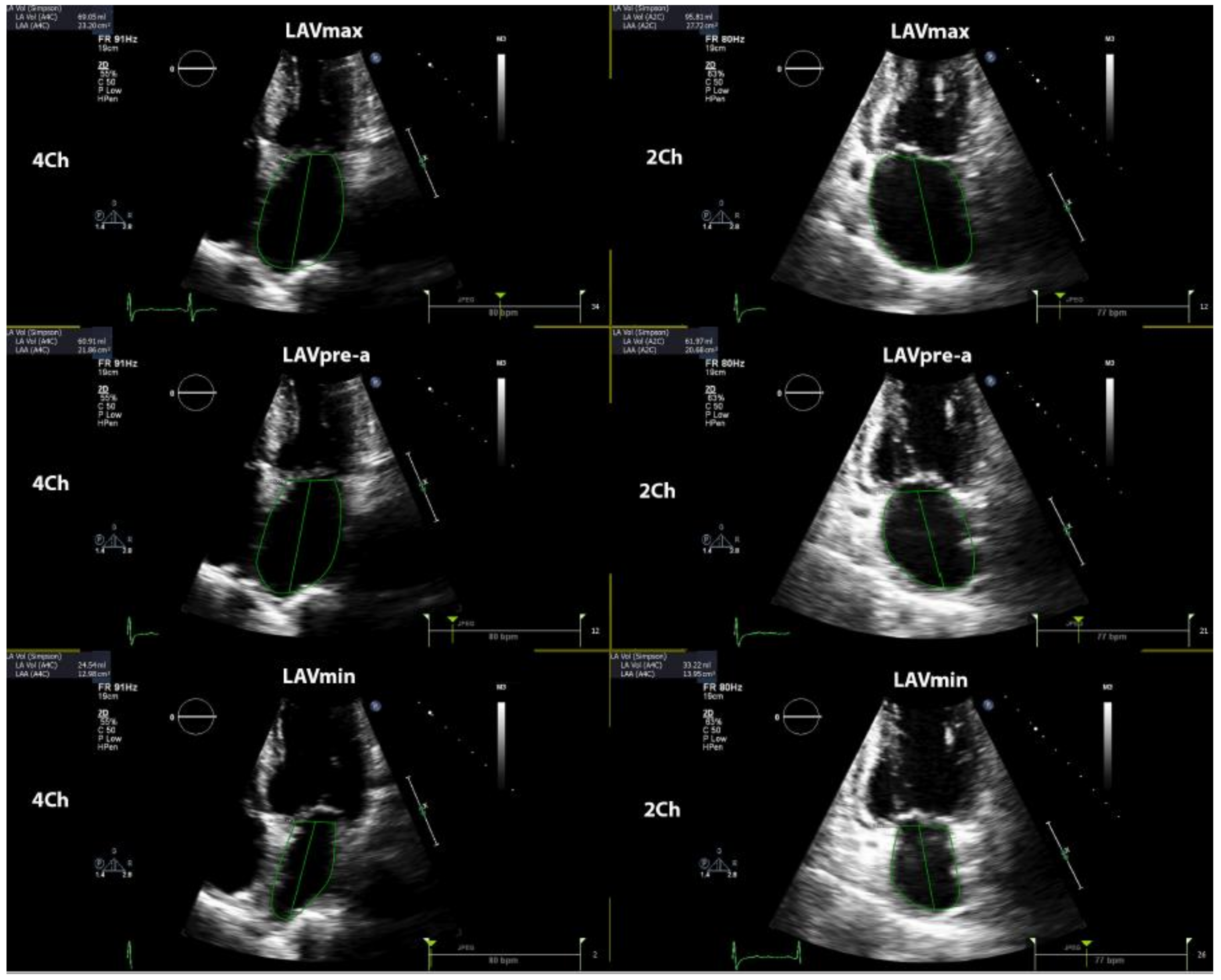
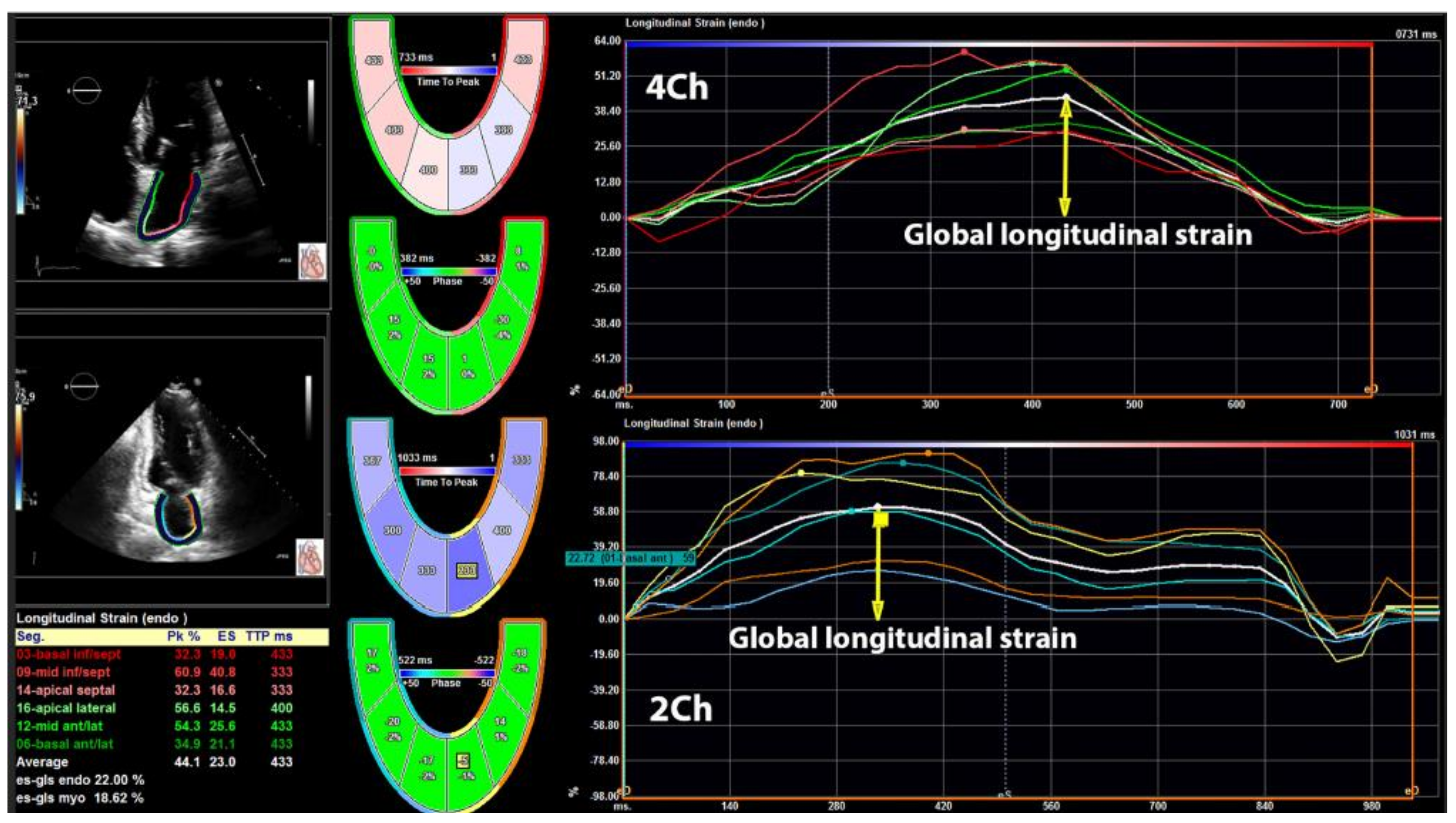
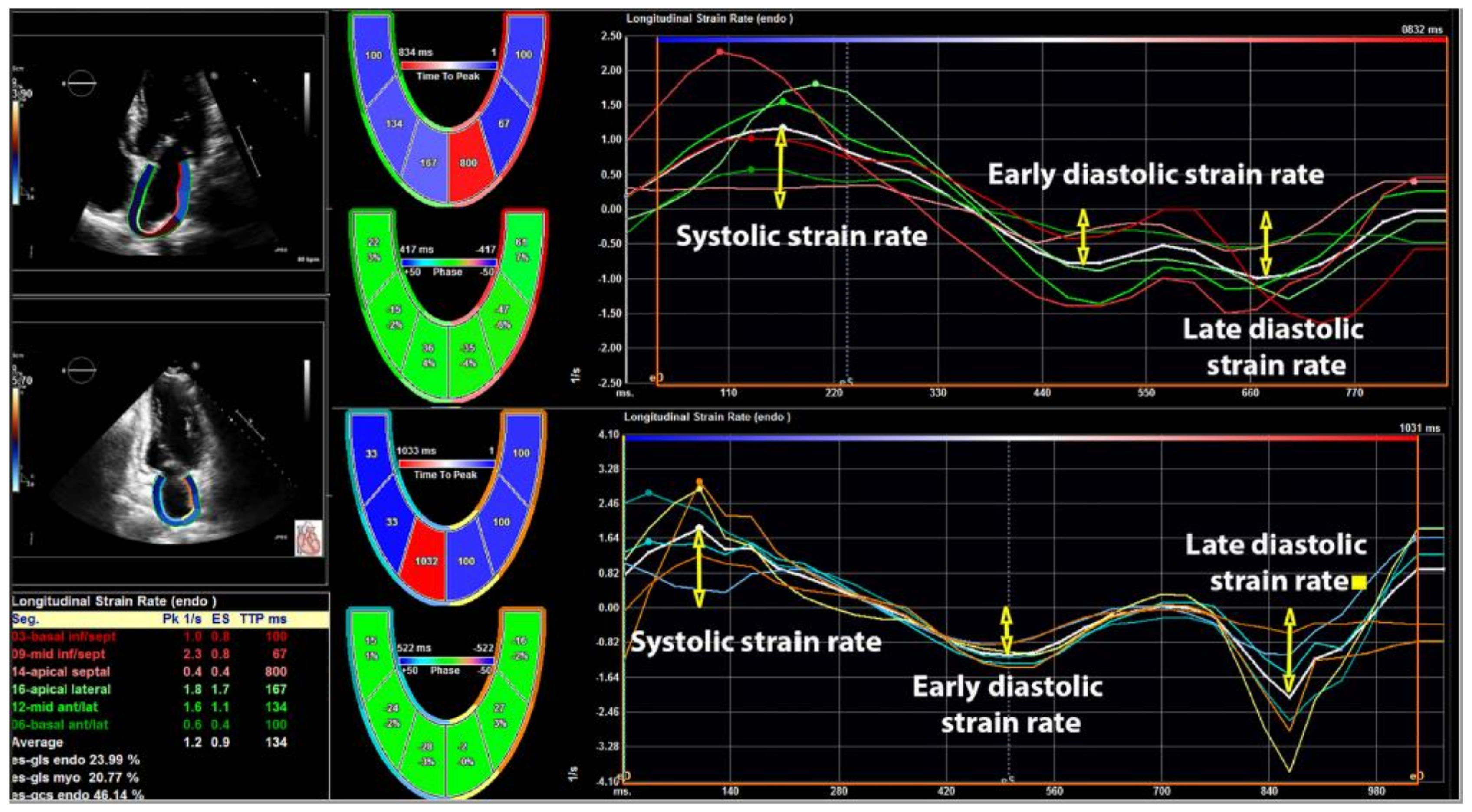
2.3. DE Assessment of Left Atrial Volumes and Function
3. Results
3.1. Left Ventricular Structure and Function
3.2. Left Atrial Phasic Function
3.3. Univariate and Multivariate Logistic Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thavendiranathan, P.; Poulin, F.; Lim, K.D.; Plana, J.C.; Woo, A.; Marwick, T.H. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: A systematic review. J. Am. Coll. Cardiol. 2014, 63, 2751–2768. [Google Scholar] [CrossRef]
- Boyd, A.; Stoodley, P.; Richards, D.; Hui, R.; Harnett, P.; Vo, K.; Marwick, T.; Thomas, L. Anthracyclines induce early changes in left ventricular systolic and diastolic function: A single centre study. PLoS ONE 2017, 12, e0175544. [Google Scholar] [CrossRef]
- Rhea, I.B.; Uppuluri, S.; Sawada, S.; Schneider, B.P.; Feigenbaum, H. Incremental prognostic value of echocardiographic strain and its association with mortality in cancer patients. J. Am. Soc. Echocardiogr. 2015, 28, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Genger, M.; Baudisch, A.; Kelle, S.; Cuspidi, C.; Belyavskiy, E.; Burkhardt, F.; Venneri, L.; Attanasio, P.; Pieske, B. Left ventricular strain in chemotherapy-naive and radiotherapy-naive patients with cancer. Can. J. Cardiol. 2018, 34, 281–287. [Google Scholar] [CrossRef]
- Tadic, M.; Baudisch, A.; Haßfeld, S.; Heinzel, F.; Cuspidi, C.; Burkhardt, F.; Escher, F.; Attanasio, P.; Pieske, B.; Genger, M. Right ventricular function and mechanics in chemotherapy- and radiotherapy-naïve cancer patients. Int. J. Cardiovasc. Imaging 2018, 34, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Guo, Y.; Cheng, L.; Song, F.; Shu, X. Early change in left atrial function in patients treated with anthracyclines assessed by real-time three-dimensional echocardiography. Sci. Rep. 2016, 6, 25512. [Google Scholar] [CrossRef] [PubMed]
- Yaylali, Y.T.; Saricopur, A.; Yurtdas, M.; Senol, H.; Gokoz-Dogu, G. Atrial function in patients with breast cancer after treatment with anthracyclines. Arq. Bras. Cardiol. 2016, 107, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, C.; Dolci, G.; Rossi, A.; Torelli, F.; Ghiselli, L.; Trevisani, L.; Vinco, G.; Truong, S.; La Russa, F.; Golia, G.; et al. Left atrial volume in patients with HER2-positive breast cancer: One step further to predict trastuzumab-related cardiotoxicity. Clin. Cardiol. 2018, 41, 349–353. [Google Scholar] [CrossRef]
- Bergamini, C.; Benfari, G.; Dolci, G.; Torelli, F.; Ghiselli, L.; Trevisani, L.; Truong, S.; Vinco, G.; La Russa, F.; Golia, G.; et al. Usefulness of left atrial remodeling in predicting cardiac toxicity during trastuzumab therapy for breast cancer. Am. J. Cardiol. 2018, 122, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.A.; Lavie, C.J.; Gilliland, Y.E.; Shah, S.B.; Dinshaw, H.K.; Milani, R.V. Prediction of all-cause mortality by the left atrial volume index in patients with normal left ventricular filling pressure and preserved ejection fraction. Mayo Clin. Proc. 2015, 90, 1499–1505. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American society of echocardiography and the European association of cardiovascular imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd BF 3rd Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Industry representatives. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar]
- Li, V.W.; Lai, C.T.; Liu, A.P.; Cheuk, D.K.; Cheung, Y.F. Left atrial mechanics and integrated calibrated backscatter in anthracycline-treated long-term survivors of childhood cancers. Ultrasound Med. Biol. 2017, 43, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Cuspidi, C.; Pencic, B.; Marjanovic, T.; Celic, V. The association between heart rate variability and biatrial phasic function in arterial hypertension. J. Am. Soc. Hypertens. 2014, 8, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Vukomanovic, V.; Cuspidi, C.; Suzic-Lazic, J.; Stanisavljevic, D.; Celic, V. Left atrial phasic function and heart rate variability in asymptomatic diabetic patients. Acta Diabetol. 2017, 54, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Ilic, S.; Ivanovic, B.; Celic, V. Left atrial phasic function and mechanics in women with subclinical hypothyroidism: The effects of levothyroxine therapy. Echocardiography 2014, 31, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Stoodley, P.W.; Richards, D.A.; Boyd, A.; Hui, R.; Harnett, P.R.; Meikle, S.R.; Clarke, J.L.; Thomas, L. Altered left ventricular longitudinal diastiolic function correlates with reduced systolic function immediately after anthracycline chemotherapy. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.R.; Chyu, C.K.; Satou, G.M.; Halnon, N.J.; Nguyen, K.L. Left atrial function in children and young adult cancer survivors treated with anthracyclines. Echocardiography 2018, 35, 1649–1656. [Google Scholar] [CrossRef] [PubMed]
- Farmakis, D.; Parissis, J.; Filippatos, G. Insights into onco-cardiology: Atrial fibrillation in cancer. J. Am. Coll. Cardiol. 2014, 63, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Pavo, N.; Raderer, M.; Hülsmann, M.; Neuhold, S.; Adlbrecht, C.; Strunk, G.; Goliasch, G.; Gisslinger, H.; Steger, G.G.; Hejna, M.; et al. Cardiovascular biomarkers in patients with cancer and their association with all-cause mortality. Heart 2015, 101, 1874–1880. [Google Scholar] [CrossRef] [PubMed]
- Cole, S.W.; Nagaraja, A.S.; Lutgendorf, S.K.; Green, P.A.; Sood, A.K. Sympathetic nervous system regulation of the tumour microenvironment. Nat. Rev. Cancer 2015, 15, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Jain, R.K. Targeting the renin-angiotensin system to improve cancer treatment: Implications for immunotherapy. Sci. Transl. Med. 2017, 9, eaan5616. [Google Scholar] [CrossRef] [PubMed]
- Dimitroula, H.; Damvopoulou, E.; Giannakoulas, G.; Dalamanga, E.; Dimitroulas, T.; Sarafidis, P.A.; Styliadis, H.; Hatzitolios, A.; Karvounis, H.; Parcharidis, G. Effects of renin-angiotensin system inhibition on left atrial function of hypertensive patients: An echocardiographic tissue deformation imaging study. Am. J. Hypertens. 2010, 23, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Belloum, Y.; Rannou-Bekono, F.; Favier, F.B. Cancer-induced cardiac cachexia: Pathogenesis and impact of physical activity (Review). Oncol. Rep. 2017, 37, 2543–2552. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Ryu, S.; Cheong, E.; Sung, K.C. Association of physical activity and inflammation with all-cause, cardiovascular-related, and cancer-related mortality. Mayo Clin. Proc. 2016, 91, 1706–1716. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Controls (n = 40) | Cancer (n = 92) | p | |
|---|---|---|---|
| Age (years) | 52 ± 7 | 54 ± 8 | 0.173 |
| Female (%) | 18 (45) | 48 (52) | 0.570 |
| BMI (kg/m2) | 26.5 ± 3.1 | 26.7 ± 3.3 | 0.745 |
| Heart rate (beats/min) | 67 ± 8 | 70 ± 9 | 0.071 |
| Systolic blood pressure (mmHg) | 132 ± 10 | 134 ± 11 | 0.326 |
| Diastolic blood pressure (mmHg) | 76 ± 7 | 78 ± 8 | 0.173 |
| Diabetes (%) | 4 (10) | 9 (10) | 1.00 |
| Hypertension (%) | 7 (18) | 19 (21) | 0.813 |
| Smoking (%) | 8 (20) | 34 (37) | 0.068 |
| Cancer localization | |||
| Gynecological (%) a | - | 14 (15) | - |
| Breast (%) | - | 15 (16) | - |
| Gastrointestinal (%) b | - | 38 (41) | - |
| Sarcoma (%) | - | 10 (11) | - |
| Lungs (%) | - | 15 (16) | - |
| Controls (n = 40) | Cancer (n = 92) | p | |
|---|---|---|---|
| LVEDD (mm) | 47.7 ± 3.9 | 47.4 ± 3.7 | 0.674 |
| LVESD (mm) | 30.1 ± 3.3 | 30.4 ± 3.5 | 0.646 |
| IVS (mm) | 9.6 ± 1.0 | 9.8 ± 1.1 | 0.326 |
| LVMI (g/m2) | 78 ± 14 | 81 ± 16 | 0.306 |
| EF (%) | 63 ± 4 | 62 ± 4 | 0.189 |
| E/A ratio | 1.18 ± 0.25 | 1.11 ± 0.22 | 0.110 |
| E/e´ | 8.4 ± 2.5 | 8.9 ± 2.7 | 0.320 |
| Controls (n = 40) | Cancer (n = 92) | p | |
|---|---|---|---|
| LA volume analysis | |||
| LAVmax/BSA (mL/m2) | 26.8 ± 4.8 | 28.7 ± 5.2 | 0.051 |
| LAVmin/BSA (mL/m2) | 12.1 ± 3.9 | 14.1 ± 4.5 | 0.016 |
| LAVpre-a/BSA (mL/m2) | 18.3 ± 5.5 | 22.7 ± 6.2 | < 0.001 |
| LA TotEF (%) | 55 ± 7 | 51 ± 7 | 0.003 |
| LA PassEF (%) | 32 ± 6 | 21 ± 6 | < 0.001 |
| LA ActEF (%) | 34 ± 7 | 38 ± 8 | 0.009 |
| LA mechanics | |||
| Total longitudinal strain (%) | 38 ± 8 | 32 ± 7 | < 0.001 |
| Systolic strain rate (s−1) | 1.81 ± 0.55 | 1.53 ± 0.45 | 0.003 |
| Early diastolic strain rate (s−1) | −2.03 ± 0.67 | −1.64 ± 0.55 | < 0.001 |
| Late diastolic strain rate (s−1) | −1.56 ± 0.51 | −1.88 ± 0.66 | 0.007 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Reduced LA longitudinal strain (<|–27%|) | ||||||
| Age (years) | 1.11 | 0.88–1.33 | 0.208 | 1.03 | 0.85–2.34 | 0.241 |
| Gender (M) | 1.13 | 0.92–1.54 | 0.136 | 0.98 | 0.66–2.12 | 0.177 |
| BMI (kg/m2) | 1.48 | 0.73–4.68 | 0.349 | 1.25 | 0.72–6.53 | 0.239 |
| E/e’ ratio | 1.87 | 0.94–3.65 | 0.206 | 1.43 | 0.87–4.79 | 0.329 |
| LV hypertrophy (Y/N) | 2.93 | 1.45–7.16 | 0.003 | 2.27 | 1.87–10.20 | 0.018 |
| Diabetes (Y/N) | 1.23 | 1.05–1.46 | 0.038 | 1.14 | 0.83–8.67 | 0.314 |
| Hypertension (Y/N) | 2.45 | 1.25–5.37 | < 0.001 | 2.06 | 1.10–10.13 | 0.012 |
| Cancer (Y/N) | 4.04 | 1.74–16.46 | < 0.001 | 3.55 | 2.11–18.70 | < 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tadic, M.; Genger, M.; Cuspidi, C.; Belyavskiy, E.; Frydas, A.; Dordevic, A.; Morris, D.A.; Völkl, J.; Parwani, A.S.; Pieske, B.; et al. Phasic Left Atrial Function in Cancer Patients Before Initiation of Anti-Cancer Therapy. J. Clin. Med. 2019, 8, 421. https://doi.org/10.3390/jcm8040421
Tadic M, Genger M, Cuspidi C, Belyavskiy E, Frydas A, Dordevic A, Morris DA, Völkl J, Parwani AS, Pieske B, et al. Phasic Left Atrial Function in Cancer Patients Before Initiation of Anti-Cancer Therapy. Journal of Clinical Medicine. 2019; 8(4):421. https://doi.org/10.3390/jcm8040421
Chicago/Turabian StyleTadic, Marijana, Martin Genger, Cesare Cuspidi, Evgeny Belyavskiy, Athanasios Frydas, Aleksandar Dordevic, Daniel A. Morris, Jakob Völkl, Abdul Shokor Parwani, Burkert Pieske, and et al. 2019. "Phasic Left Atrial Function in Cancer Patients Before Initiation of Anti-Cancer Therapy" Journal of Clinical Medicine 8, no. 4: 421. https://doi.org/10.3390/jcm8040421