High-Intensity Interval Training is Associated with Improved Long-Term Survival in Heart Failure Patients

 , and
, and
Abstract
:1. Introduction
2. Methods
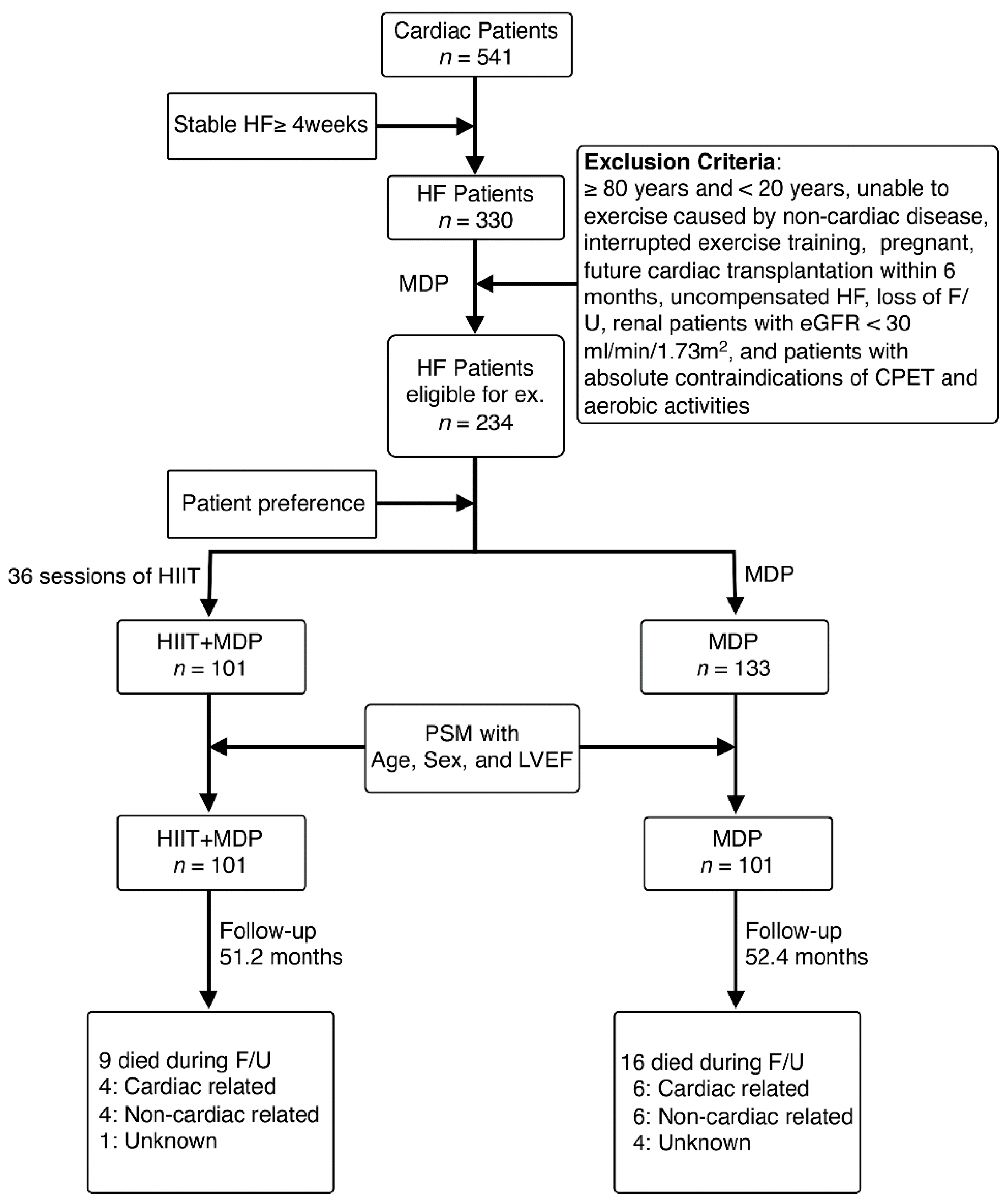
2.1. Participants
2.2. Clinical Assessments
2.2.1. Echocardiography
2.2.2. Cardiopulmonary Exercise Test
2.3. Interventions
2.4. Follow-Up
2.5. Statistical Analysis
2.5.1. Longitudinal Analysis
2.5.2. Functional Principal Component Analysis (FPCA)
- Y (LVEF_Diff) = LVEFF/U − LVEFbaseline.
- Y (Normalized LVEDD_Diff) = (LVEDDF/U − LVEDDbaseline)/LVEDDbaseline.
- Y (Normalized LVESD_Diff) = (LVESDF/U − LVESDbaseline)/LVESDbaseline.
- Y (Normalized VO2peak_Diff) = (VO2peak_F/U − VO2peak_baseline)/VO2peak_baseline.
3. Results
3.1. Patient Characteristics
3.2. HIIT Improved VO2peak and Quality of Life
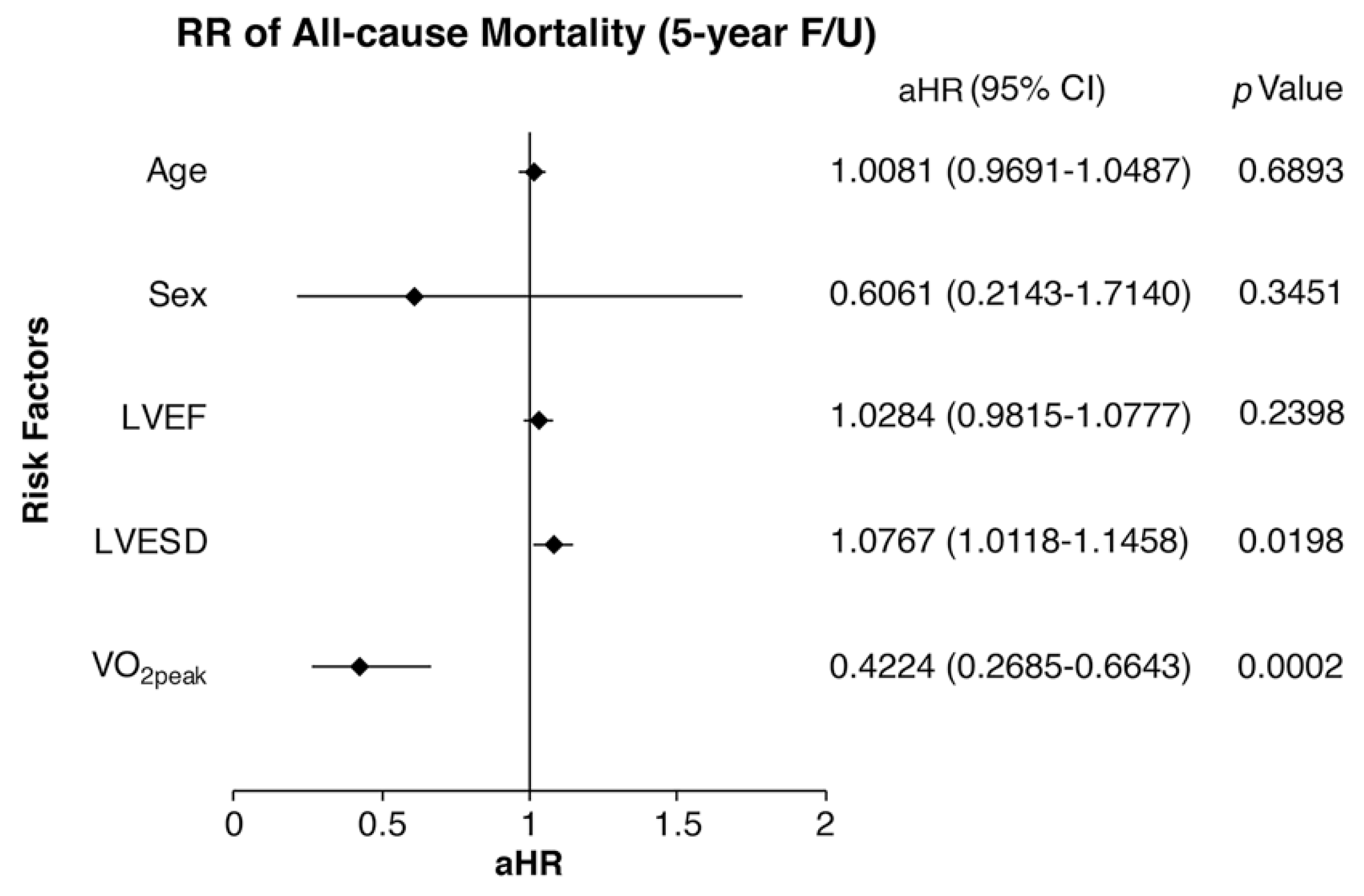
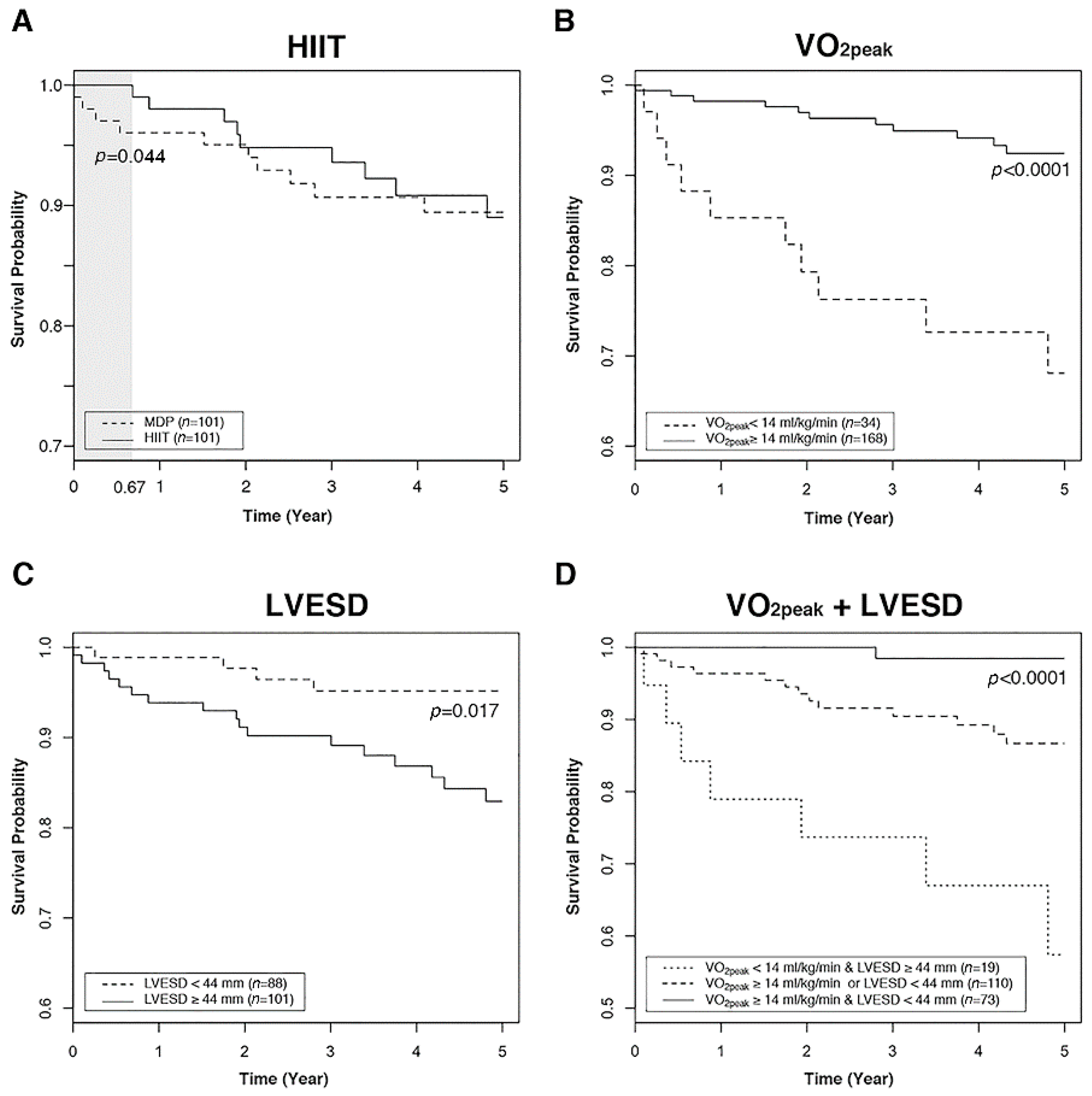
3.3. Increased VO2peak and Decreased LVESD Were Protective Factors Against Mortality
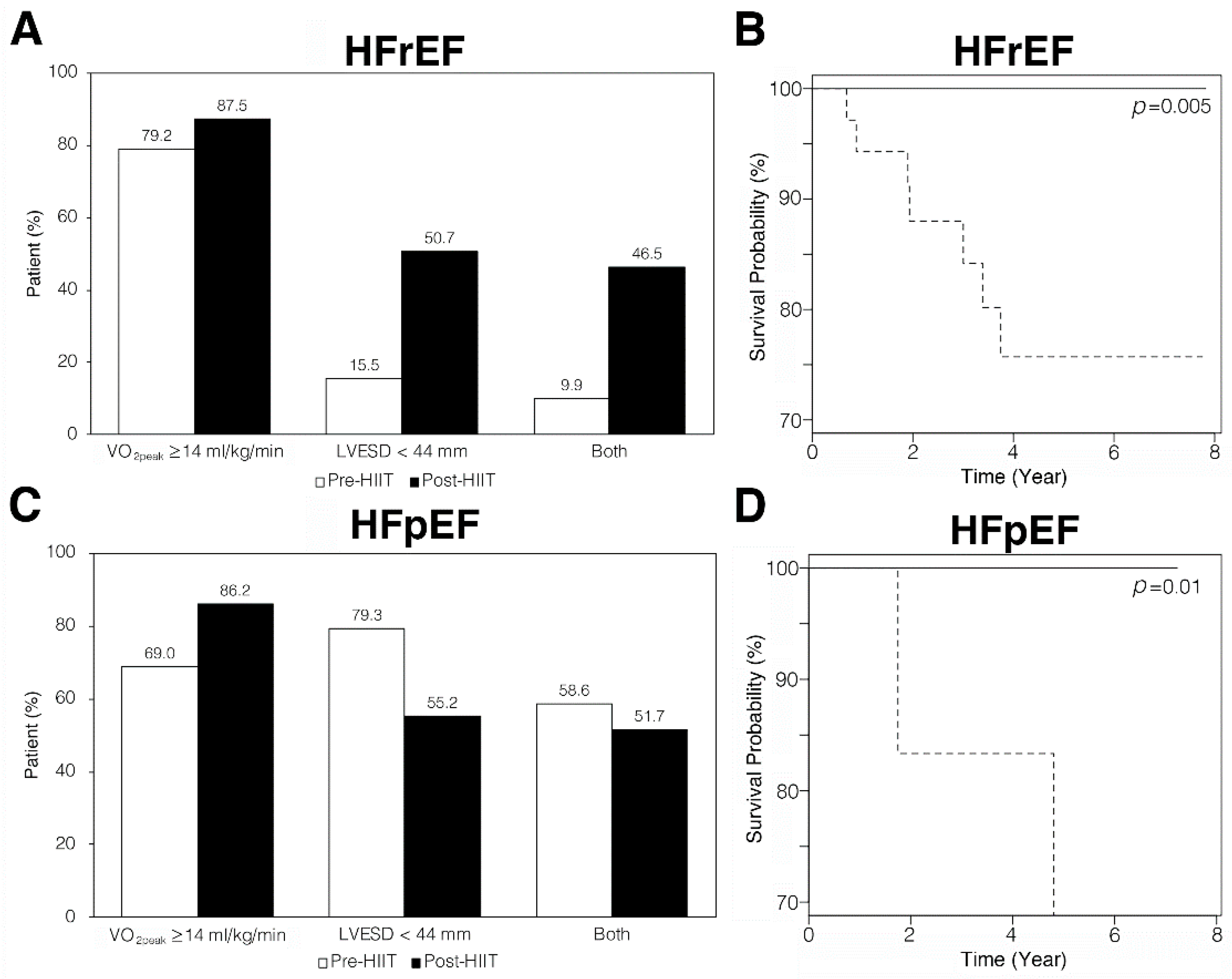
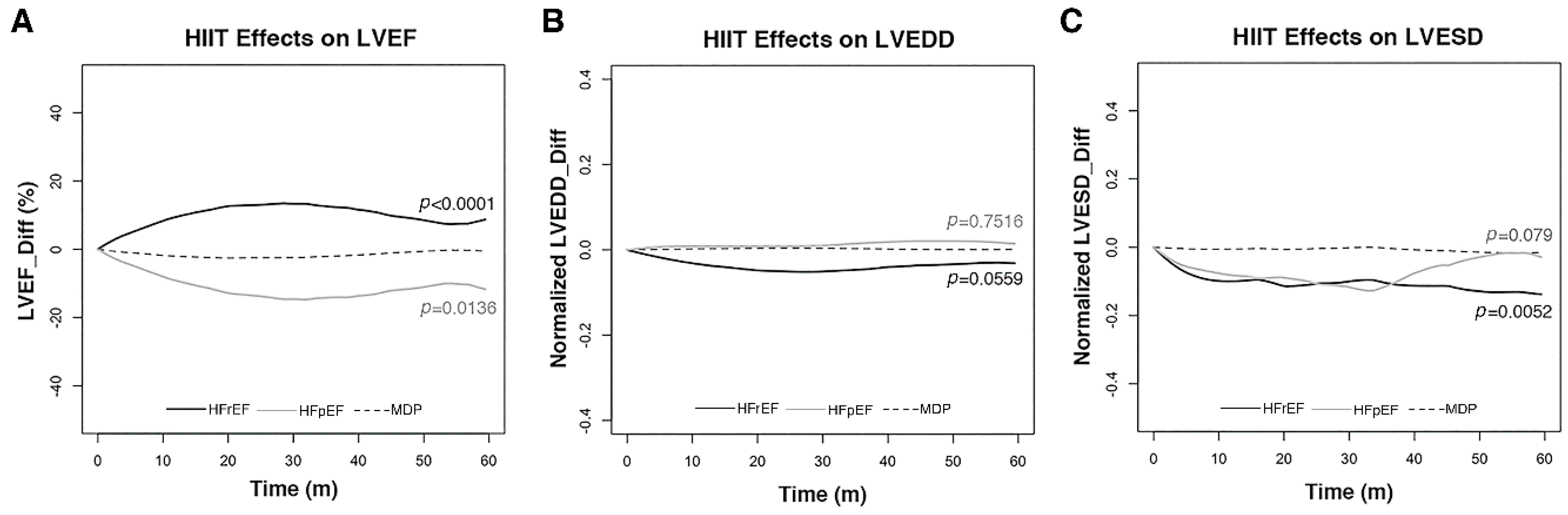
3.4. HIIT Reversed Cardiac Remodeling In HFrEF Patients
3.5. HIIT Induced Mild LV Dilatation and Decreased LVEF in HFpEF Patients
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; et al. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef]
- Bui, A.L.; Horwich, T.B.; Fonarow, G.C. Epidemiology and risk profile of heart failure. Nat. Rev. Cardiol. 2011, 8, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Sakata, Y.; Shimokawa, H. Epidemiology of heart failure in Asia. Circ. J. 2013, 77, 2209–2217. [Google Scholar] [CrossRef]
- Levy, D.; Kenchaiah, S.; Larson, M.G.; Benjamin, E.J.; Kupka, M.J.; Ho, K.K.; Murabito, J.M.; Vasan, R.S. Long-term trends in the incidence of and survival with heart failure. N. Engl. J. Med. 2002, 347, 1397–1402. [Google Scholar] [CrossRef]
- Cook, C.; Cole, G.; Asaria, P.; Jabbour, R.; Francis, D.P. The annual global economic burden of heart failure. Int. J. Cardiol. 2014, 171, 368–376. [Google Scholar] [CrossRef]
- Gossard, D.; Haskell, W.L.; Taylor, C.B.; Mueller, J.K.; Rogers, F.; Chandler, M.; Ahn, D.K.; Miller, N.H.; DeBusk, R.F. Effects of low- and high-intensity home-based exercise training on functional capacity in healthy middle-aged men. Am. J. Cardiol. 1986, 57, 446–449. [Google Scholar] [CrossRef]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, O.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef]
- Fu, T.C.; Wang, C.H.; Lin, P.S.; Hsu, C.C.; Cherng, W.J.; Huang, S.C.; Liu, M.H.; Chiang, C.L.; Wang, J.S. Aerobic interval training improves oxygen uptake efficiency by enhancing cerebral and muscular hemodynamics in patients with heart failure. Int. J. Cardiol. 2013, 167, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Angadi, S.S.; Mookadam, F.; Lee, C.D.; Tucker, W.J.; Haykowsky, M.J.; Gaesser, G.A. High-intensity interval training vs. moderate-intensity continuous exercise training in heart failure with preserved ejection fraction: A pilot study. J. Appl. Physiol. 2015, 119, 753–758. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.S.; Fu, T.C.; Lien, H.Y.; Wang, C.H.; Hsu, C.C.; Wu, W.C.; Chien, Y.W.; Cherng, W.J. Effect of aerobic interval training on erythrocyte rheological and hemodynamic functions in heart failure patients with anemia. Int. J. Cardiol. 2013, 168, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Hambrecht, R.; Gielen, S.; Linke, A.; Fiehn, E.; Yu, J.; Walther, C.; Schoene, N.; Schuler, G. Effects of exercise training on left ventricular function and peripheral resistance in patients with chronic heart failure: A randomized trial. JAMA 2000, 283, 3095–3101. [Google Scholar] [CrossRef]
- Giannuzzi, P.; Temporelli, P.L.; Corra, U.; Tavazzi, L. Antiremodeling effect of long-term exercise training in patients with stable chronic heart failure: Results of the Exercise in Left Ventricular Dysfunction and Chronic Heart Failure (ELVD-CHF) Trial. Circulation 2003, 108, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Parashar, A.; Kumbhani, D.; Agarwal, S.; Garg, J.; Kitzman, D.; Levine, B.; Drazner, M.; Berry, J. Exercise training in patiensts with heart failure and preserved ejection fraction: Meta-analysis of randomized control trials. Circ. Heart Fail. 2015, 8, 33–40. [Google Scholar] [CrossRef]
- Ellingsen, Ø.; Halle, M.; Conraads, V.; Støylen, A.; Dalen, H.; Delagardelle, C.; Larsen, A.I.; Hole, T.; Mezzani, A.; Van Craenenbroeck, E.M.; et al. High-intensity interval training in patients with heart failure with reduced ejection fraction. Circulation 2017, 135, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sorensen, H.T.; von Elm, E.; Langan, S.M. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef] [PubMed]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The natural history of congestive heart failure: The framingham study. N. Engl. J. Med. 1971, 285, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Working Group on Cardiac Rehabilitation & Exercise Physiology; Working Group on Heart Failure of the European Society of Cardiology. Recommendations for exercise testing in chronic heart failure patients. Eur. Heart J. 2001, 22, 37–45. [Google Scholar] [CrossRef]
- Lee, M.F.; Chen, W.S.; Fu, T.C.; Liu, M.H.; Wang, J.S.; Hsu, C.C.; Huang, Y.Y.; Cherng, W.J.; Wang, C.H. Non-invasive cardiac index monitoring during cardiopulmonary functional testing provides additional prognostic value in patients after acute heart failure. Int. Heart J. 2012, 53, 364–369. [Google Scholar] [CrossRef]
- Mao, C.T.; Liu, M.H.; Hsu, K.H.; Fu, T.C.; Wang, J.S.; Huang, Y.Y.; Yang, N.I.; Wang, C.H. Effect of multidisciplinary disease management for hospitalized heart failure under a national health insurance programme. J. Cardiovasc. Med. 2015, 16, 616–624. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Arena, R.; Riebe, D.; Thompson, P.D. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Bruggink, A.H.; de Jonge, N.; van Oosterhout, M.F.; Van Wichen, D.F.; de Koning, E.; Lahpor, J.R.; Kemperman, H.; Gmelig-Meyling, F.H.; de Weger, R.A. Brain natriuretic peptide is produced both by cardiomyocytes and cells infiltrating the heart in patients with severe heart failure supported by a left ventricular assist device. J. Heart Lung Transplant. 2006, 25, 174–180. [Google Scholar] [CrossRef]
- Carr, K.W.; Engler, R.L.; Forsythe, J.R.; Johnson, A.D.; Gosink, B. Measurement of left ventricular ejection fraction by mechanical cross-sectional echocardiography. Circulation 1979, 59, 1196–1206. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the american society of echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the european association of echocardiography, a branch of the european society of cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar]
- Fu, T.C.; Wang, C.H.; Hsu, C.C.; Cherng, W.J.; Huang, S.C.; Wang, J.S. Suppression of cerebral hemodynamics is associated with reduced functional capacity in patients with heart failure. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H1545–H1555. [Google Scholar] [CrossRef] [Green Version]
- Fu, T.C.; Yang, N.I.; Wang, C.H.; Cherng, W.J.; Chou, S.L.; Pan, T.L.; Wang, J.S. Aerobic Interval Training Elicits Different Hemodynamic Adaptations Between Heart Failure Patients with Preserved and Reduced Ejection Fraction. Am. J. Phys. Med. Rehabil. 2016, 95, 15–27. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef] [Green Version]
- Kou, S.; Caballero, L.; Dulgheru, R.; Voilliot, D.; De Sousa, C.; Kacharava, G.; Athanassopoulos, G.D.; Barone, D.; Baroni, M.; Cardim, N.; et al. Echocardiographic reference ranges for normal cardiac chamber size: Results from the NORRE study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 680–690. [Google Scholar] [CrossRef]
- Yao, F.; Müller, H.G.; Wang, J.L. Functional Data Analysis for Sparse Longitudinal Data. J. Am. Stat. Assoc. 2005, 100, 577–590. [Google Scholar] [CrossRef]
- Konstam, M.A.; Kramer, D.G.; Patel, A.R.; Maron, M.S.; Udelson, J.E. Left ventricular remodeling in heart failure: Current concepts in clinical significance and assessment. J. Am. Coll. Cardiol. 2011, 4, 98–108. [Google Scholar] [CrossRef]
- Cahalin, L.P.; Chase, P.; Arena, R.; Myers, J.; Bensimhon, D.; Peberdy, M.A.; Ashley, E.; West, E.; Forman, D.E.; Pinkstaff, S.; et al. A meta-analysis of the prognostic significance of cardiopulmonary exercise testing in patients with heart failure. Heart Fail. Rev. 2013, 18, 79–94. [Google Scholar] [CrossRef]
- Ismail, H.; McFarlane, J.R.; Nojoumian, A.H.; Dieberg, G.; Smart, N.A. Clinical outcomes and cardiovascular responses to different exercise training intensities in patients with heart failure: A systematic review and meta-analysis. JACC. Heart Fail. 2013, 1, 514–522. [Google Scholar] [CrossRef]
- Wang, J.S. Effect of exercise training on exercise capacity and quality of life in patients with heart failure. Int. J. Cardiol. 2018, 261, 144–145. [Google Scholar] [CrossRef]
- Liu, S.; Guan, Z.; Jin, X.; Meng, P.; Wang, Y.; Zheng, X.; Jia, D.; Ma, C.; Yang, J. Left ventricular diastolic and systolic dyssynchrony and dysfunction in heart failure with preserved ejection fraction and a narrow QRS complex. Int. J. Med. Sci. 2018, 15, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Thaman, R.; Gimeno, J.R.; Reith, S.; Esteban, M.T.; Limongelli, G.; Murphy, R.T.; Mist, B.; McKenna, W.J.; Elliott, P.M. Progressive left ventricular remodeling in patients with hypertrophic cardiomyopathy and severe left ventricular hypertrophy. J. Am. Coll. Cardiol. 2004, 44, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Weiner, R.B.; Baggish, A.L. Exercise-induced cardiac remodeling. Prog. Cardiovasc. Dis. 2012, 54, 380–386. [Google Scholar] [CrossRef]
- Dawes, T.J.; Corden, B.; Cotter, S.; de Marvao, A.; Walsh, R.; Ware, J.S.; Cook, S.A.; O’Regan, D.P. Moderate physical activity in healthy adults Is associated with cardiac remodeling. Circ. Cardiovasc. Imaging 2016, 9, e004712. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Whellan, D.J.; Lee, K.L.; Keteyian, S.J.; Cooper, L.S.; Ellis, S.J.; Leifer, E.S.; Kitzman, D.W.; Blumenthal, J.A.; Rendall, D.S.; et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-Action randomized controlled trial. JAMA 2009, 301, 1439–1450. [Google Scholar] [CrossRef]
- Lam, C.S.; Donal, E.; Kraigher-Krainer, E.; Vasan, R.S. Epidemiology and clinical course of heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2011, 13, 18–28. [Google Scholar] [CrossRef]
- Bhatia, R.S.; Tu, J.V.; Lee, D.S.; Austin, P.C.; Fang, J.; Haouzi, A.; Gong, Y.; Liu, P.P. Outcome of heart failure with preserved ejection fraction in a population-based study. N. Engl. J. Med. 2006, 355, 260–269. [Google Scholar] [CrossRef]
- Akiyama, E.; Van Aelst, L.N.L.; Arrigo, M.; Lassus, J.; Miro, O.; Celutkiene, J.; Choi, D.J.; Cohen-Solal, A.; Ishihara, S.; Kajimoto, K.; et al. East Asia may have a better 1-year survival following an acute heart failure episode compared with Europe: Results from an international observational cohort. Eur. J. Heart Fail. 2018, 20, 1071–1075. [Google Scholar] [CrossRef]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HIIT + MDP (n = 101) | MDP (n = 101) | p-Value | ||
|---|---|---|---|---|
| HFrEF/HFpEF | 72/29 | 71/30 | 1.000 | |
| Age, years | 61.5 (58.7–64.2) | 62.8 (60.1–65.5) | 0.492 | |
| Sex (F/M) | 31/70 | 27/74 | 0.641 | |
| BMI, kg/m2 | 25.7 (24.7–26.6) | 25.2 (24.3–26.2) | 0.504 | |
| HF duration, month | 7.76 (4.50–11.0) | 11.3 (7.39–15.3) | 0.168 | |
| NYHA Functional Class, n (%) | ||||
| I | 2 (2) | 7 (7) | 0.109 | |
| II | 75 (74) | 78 (77) | ||
| III | 24 (24) | 16 (16) | ||
| Etiology, n (%) | ||||
| CAD | 47 (47) | 46 (46) | 1.000 | |
| DCM | 19 (19) | 21 (21) | 0.860 | |
| Hypertension | 56 (55) | 62 (61) | 0.475 | |
| Comorbidity, n (%) | ||||
| Hyperlipidemia | 50 (50) | 50 (50) | 1.000 | |
| DM | 42 (42) | 40 (40) | 0.886 | |
| Arrhythmia | 34 (34) | 33 (33) | 1.000 | |
| Resting BP, mmHg | SBP | 123 (119–128) | 127 (122–131) | 0.318 |
| DBP | 76 (73–79) | 77 (74–80) | 0.776 | |
| Resting HR, bpm | 77 (75–79) | 81 (78–84) | 0.040 b | |
| LVEF, % | 34.3 (31.3–37.2) | 37.0 (34.1–39.9) | 0.190 | |
| BNP, pg/mL a | 667 (508–801) | 635 (482–787) | 0.765 | |
| Medication, n (%) | ||||
| ACEI/ARB | 82 (81) | 83 (82) | 1.000 | |
| β-blocker | 80 (79) | 81 (80) | 1.000 | |
| Diuretics | 56 (55) | 63 (62) | 0.391 | |
| MRA | 20 (20) | 11 (11) | 0.117 | |
| Type | Assessment | Initial | End-HIIT | p-Value | |
|---|---|---|---|---|---|
| HFrEF | LVEF, % | 26.8 (24.6–28.9) | 48.2 (44.3–52.1) | <0.001 a | |
| LVEDD, mm | 63.2 (60.7–65.7) | 60.0 (57.5–62.5) | 0.002 a | ||
| LVESD, mm | 54.8 (52.2–57.4) | 45.0 (41.9–48.2) | <0.001 a | ||
| VO2peak, mL/kg/min | 17.2 (16.3–18.1) | 20.5 (19.2–21.8) | <0.001 a | ||
| Peak HR, bpm | 132 (126–137) | 139 (133–146) | 0.001 a | ||
| Peak O2 pulse, mL/beat | 9.22 (8.61–9.82) | 10.2 (9.48–10.9) | <0.001 a | ||
| SF-36 | PCS | 47.0 (45.0–48.9) | 50.9 (48.8–52.9) | <0.001 a | |
| MCS | 45.1 (42.8–47.3) | 47.6 (45.2–49.9) | 0.012 a | ||
| HFpEF | LVEF, % | 52.9 (48.5–57.2) | 53.1 (48.2–57.9) | 0.803 | |
| LVEDD, mm | 54.3 (51.3–57.4) | 56.3 (53.0–59.6) | 0.285 | ||
| LVESD, mm | 38.7 (35.4–42.0) | 40.6 (37.1–44.1) | 0.387 | ||
| VO2peak, mL/kg/min | 16.2 (15.1–17.4) | 18.5 (16.8–20.2) | <0.001 a | ||
| Peak HR, bpm | 136 (126–146) | 144 (133–154) | 0.010 a | ||
| Peak O2 pulse, mL/beat | 8.49 (7.45–9.52) | 9.38 (8.19–10.6) | 0.008 a | ||
| SF-36 | PCS | 45.9 (43.0–48.8) | 50.8 (47.6–53.9) | 0.005 a | |
| MCS | 42.6 (37.9–47.2) | 46.5 (42.3–50.8) | 0.084 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-C.; Fu, T.-C.; Yuan, S.-S.; Wang, C.-H.; Liu, M.-H.; Shyu, Y.-C.; Cherng, W.-J.; Wang, J.-S. High-Intensity Interval Training is Associated with Improved Long-Term Survival in Heart Failure Patients. J. Clin. Med. 2019, 8, 409. https://doi.org/10.3390/jcm8030409
Hsu C-C, Fu T-C, Yuan S-S, Wang C-H, Liu M-H, Shyu Y-C, Cherng W-J, Wang J-S. High-Intensity Interval Training is Associated with Improved Long-Term Survival in Heart Failure Patients. Journal of Clinical Medicine. 2019; 8(3):409. https://doi.org/10.3390/jcm8030409
Chicago/Turabian StyleHsu, Chih-Chin, Tieh-Cheng Fu, Shin-Sheng Yuan, Chao-Hung Wang, Min-Hui Liu, Yu-Chiau Shyu, Wen-Jin Cherng, and Jong-Shyan Wang. 2019. "High-Intensity Interval Training is Associated with Improved Long-Term Survival in Heart Failure Patients" Journal of Clinical Medicine 8, no. 3: 409. https://doi.org/10.3390/jcm8030409