
Fetal Lung Volume Appears to Predict Respiratory Morbidity in Congenital Diaphragmatic Hernia
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Collection
2.2. Patient Care
2.3. Diagnosis of Respiratory Morbidity
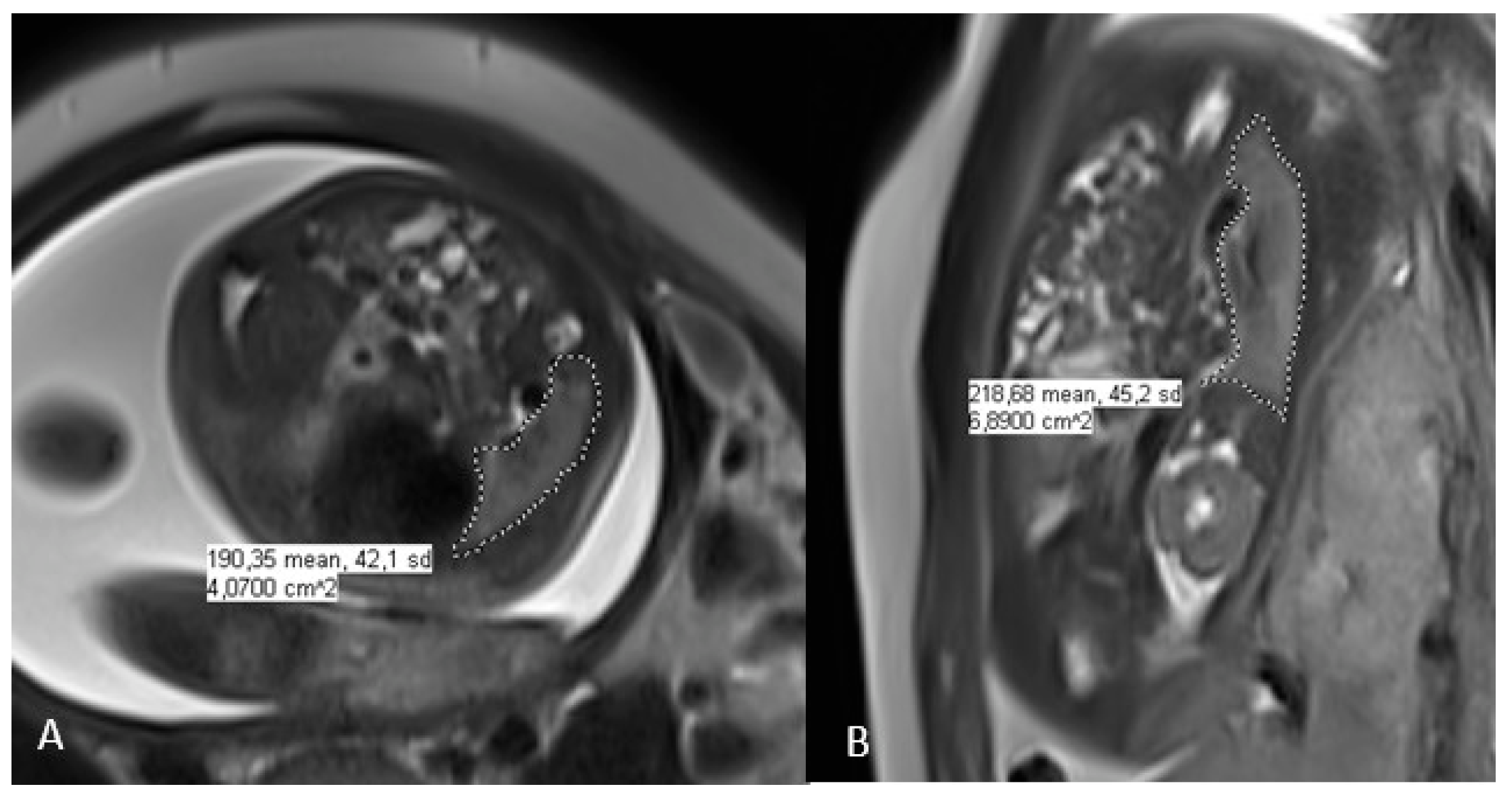
2.4. Fetal Lung Volume Measurement on MRI
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Respiratory Morbidity
3.3. Optimal Threshold Value of o/e FLV and Respiratory Morbidity
4. Discussion
Strengths and Weaknesses of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Platform on Rare Disease Registration. Available online: https://eu-rd-platform.jrc.ec.europa.eu (accessed on 16 June 2020).
- Kotecha, S. Lung Growth for Beginners. Paediatr. Respir. Rev. 2000, 1, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Bebbington, M.; Victoria, T.; Danzer, E.; Moldenhauer, J.; Khalek, N.; Johnson, M.; Hedrick, H.; Adzick, N.S. Comparison of Ultrasound and Magnetic Resonance Imaging Parameters in Predicting Survival in Isolated Left-Sided Congenital Diaphragmatic Hernia. Ultrasound Obstet. Gynecol. 2014, 43, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Metkus, A.P.; Filly, R.A.; Stringer, M.D.; Harrison, M.R.; Adzick, N.S. Sonographic Predictors of Survival in Fetal Diaphragmatic Hernia. J. Pediatr. Surg. 1996, 31, 148–152. [Google Scholar] [CrossRef] [PubMed]
- HAS Avis et Décisions de La HAS Décision N°2012.0169/DC/SBPP Du 24 Octobre 2012 Du Collège de La Haute Autorité de Santé Adoptant Le Protocole National et de Soins: Hernie Diaphragmatique Congénitale. Available online: https://www.has-sante.fr/jcms/c_1333885/en/decision-n2012-0169/dc/sbpp-du-24-octobre-2012-du-college-de-la-haute-autorite-de-sante-portant-adoption-du-protocole-national-de-diagnostic-et-de-soins-pour-la-prise-en-charge-de-la-hernie-diaphragmatique-congenitale (accessed on 13 February 2023).
- Rypens, F.; Metens, T.; Rocourt, N.; Sonigo, P.; Brunelle, F.; Quere, M.P.; Guibaud, L.; Maugey-Laulom, B.; Durand, C.; Avni, F.E.; et al. Fetal Lung Volume: Estimation at MR Imaging—Initial Results. Radiology 2001, 219, 236–241. [Google Scholar] [CrossRef]
- Oluyomi-Obi, T.; Kuret, V.; Puligandla, P.; Lodha, A.; Lee-Robertson, H.; Lee, K.; Somerset, D.; Johnson, J.; Ryan, G. Antenatal Predictors of Outcome in Prenatally Diagnosed Congenital Diaphragmatic Hernia (CDH). J. Pediatr. Surg. 2017, 52, 881–888. [Google Scholar] [CrossRef]
- Neff, K.W.; Kilian, A.K.; Schaible, T.; Schütz, E.-M.; Büsing, K.A. Prediction of Mortality and Need for Neonatal Extracorporeal Membrane Oxygenation in Fetuses with Congenital Diaphragmatic Hernia: Logistic Regression Analysis Based on MRI Fetal Lung Volume Measurements. Am. J. Roentgenol. 2007, 189, 1307–1311. [Google Scholar] [CrossRef]
- Debus, A.; Hagelstein, C.; Kilian, A.K.; Weiss, C.; Schönberg, S.O.; Schaible, T.; Neff, K.W.; Büsing, K.A. Fetal Lung Volume in Congenital Diaphragmatic Hernia: Association of Prenatal MR Imaging Findings with Postnatal Chronic Lung Disease. Radiology 2013, 266, 887–895. [Google Scholar] [CrossRef]
- Büsing, K.A.; Kilian, A.K.; Schaible, T.; Endler, C.; Schaffelder, R.; Neff, K.W. MR Relative Fetal Lung Volume in Congenital Diaphragmatic Hernia: Survival and Need for Extracorporeal Membrane Oxygenation. Radiology 2008, 248, 240–246. [Google Scholar] [CrossRef]
- Snoek, K.G.; Reiss, I.K.M.; Greenough, A.; Capolupo, I.; Urlesberger, B.; Wessel, L.; Storme, L.; Deprest, J.; Schaible, T.; van Heijst, A.; et al. Standardized Postnatal Management of Infants with Congenital Diaphragmatic Hernia in Europe: The CDH EURO Consortium Consensus—2015 Update. Neonatology 2016, 110, 66–74. [Google Scholar] [CrossRef]
- Storme, L.; Boubnova, J.; Mur, S.; Pognon, L.; Sharma, D.; Aubry, E.; Sfeir, R.; Vaast, P.; Rakza, T.; Benachi, A.; et al. Review Shows That Implementing a Nationwide Protocol for Congenital Diaphragmatic Hernia Was a Key Factor in Reducing Mortality and Morbidity. Acta Paediatr. 2018, 107, 1131–1139. [Google Scholar] [CrossRef] [Green Version]
- Muratore, C.S.; Kharasch, V.; Lund, D.P.; Sheils, C.; Friedman, S.; Brown, C.; Utter, S.; Jaksic, T.; Wilson, J.M. Pulmonary Morbidity in 100 Survivors of Congenital Diaphragmatic Hernia Monitored in a Multidisciplinary Clinic. J. Pediatr. Surg. 2001, 36, 133–140. [Google Scholar] [CrossRef]
- Benoist, G.; Mokhtari, M.; Deschildre, A.; Khen-Dunlop, N.; Storme, L.; Benachi, A.; Delacourt, C. Risk of Readmission for Wheezing during Infancy in Children with Congenital Diaphragmatic Hernia. PLoS ONE 2016, 11, e0155556. [Google Scholar] [CrossRef]
- Heindel, K.; Holdenrieder, S.; Patel, N.; Bartmann, P.; Schroeder, L.; Berg, C.; Merz, W.M.; Mueller, A.; Kipfmueller, F. Early Postnatal Changes of Circulating N-Terminal-pro-B-Type Natriuretic Peptide in Neonates with Congenital Diaphragmatic Hernia. Early Hum. Dev. 2020, 146, 105049. [Google Scholar] [CrossRef]
- Büsing, K.A.; Kilian, A.K.; Schaible, T.; Debus, A.; Weiss, C.; Neff, K.W. Reliability and Validity of MR Image Lung Volume Measurement in Fetuses with Congenital Diaphragmatic Hernia and in Vitro Lung Models. Radiology 2008, 246, 553–561. [Google Scholar] [CrossRef]
- Gonçalves, A.N.; Correia-Pinto, J.; Nogueira-Silva, C. Imagiological Methods for Prediction of Fetal Pulmonary Hypoplasia: A Systematic Review. J. Matern. Fetal. Neonatal. Med. 2019, 34, 1459–1468. [Google Scholar] [CrossRef]
- Kim, A.G.; Norwitz, G.; Karmakar, M.; Ladino-Torres, M.; Berman, D.R.; Kreutzman, J.; Treadwell, M.C.; Mychaliska, G.B.; Perrone, E.E. Discordant Prenatal Ultrasound and Fetal MRI in CDH: Wherein Lies the Truth? J. Pediatr. Surg. 2019, 55, S0022346819308401. [Google Scholar] [CrossRef]
- Abbasi, N.; Cortes, M.S.; Ruano, R.; Johnson, A.; Morgan, T.; Coleman, B.; Baschat, A.; Zaretsky, M.; Lim, F.Y.; Bulas, D.; et al. Variability in Antenatal Prognostication of Fetal Diaphragmatic Hernia across the North American Fetal Therapy Network (NAFTNet). Prenat. Diagn. 2020, 40, 342–350. [Google Scholar] [CrossRef]
- Cannie, M.M.; Cordier, A.-G.; Laveaucoupet, J.D.; Franchi-Abella, S.; Cagneaux, M.; Prodhomme, O.; Senat, M.-V.; Mokhtari, M.; Vlieghe, V.; Nowakowska, D.; et al. Liver-to-Thoracic Volume Ratio: Use at MR Imaging to Predict Postnatal Survival in Fetuses with Isolated Congenital Diaphragmatic Hernia with or without Prenatal Tracheal Occlusion. Eur. Radiol. 2013, 23, 1299–1305. [Google Scholar] [CrossRef]
- Tanacan, A.; Orgul, G.; Aydin, E.; Kayki, G.; Celik, T.; Yalcin, S.; Soyer, T.; Yigit, S.; Yurdakök, M.; Sinan Beksac, M. Antenatal Management and Outcomes of Pregnancies with Congenital Diaphragmatic Hernia. J. Neonatal-Perinat. Med. 2020, 13, 323–330. [Google Scholar] [CrossRef]
- Zamora, I.J.; Olutoye, O.O.; Cass, D.L.; Fallon, S.C.; Lazar, D.A.; Cassady, C.I.; Mehollin-Ray, A.R.; Welty, S.E.; Ruano, R.; Belfort, M.A.; et al. Prenatal MRI Fetal Lung Volumes and Percent Liver Herniation Predict Pulmonary Morbidity in Congenital Diaphragmatic Hernia (CDH). J. Pediatr. Surg. 2014, 49, 688–693. [Google Scholar] [CrossRef]
- Brown, B.P.; Clark, M.T.; Wise, R.L.; Timsina, L.R.; Reher, T.A.; Vandewalle, R.J.; Brown, J.J.; Saenz, Z.M.; Gray, B.W. A Multifactorial Severity Score for Left Congenital Diaphragmatic Hernia in a High-Risk Population Using Fetal Magnetic Resonance Imaging. Pediatr. Radiol. 2019, 49, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Cordier, A.-G.; Russo, F.M.; Deprest, J.; Benachi, A. Prenatal Diagnosis, Imaging, and Prognosis in Congenital Diaphragmatic Hernia. Semin. Perinatol. 2019, 44, 51163. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, H.; Kotani, T.; Miura, M.; Ito, Y.; Hirako, S.; Nakano, T.; Imai, K.; Kikkawa, F. Observed-to-Expected MRI Fetal Lung Volume Can Predict Long-Term Lung Morbidity in Infants with Congenital Diaphragmatic Hernia. J. Matern. Fetal Neonatal Med. 2017, 30, 1509–1513. [Google Scholar] [CrossRef] [PubMed]
- Trachsel, D.; Selvadurai, H.; Bohn, D.; Langer, J.C.; Coates, A.L. Long-Term Pulmonary Morbidity in Survivors of Congenital Diaphragmatic Hernia. Pediatr. Pulmonol. 2005, 39, 433–439. [Google Scholar] [CrossRef]
- Cauley, R.P.; Potanos, K.; Fullington, N.; Bairdain, S.; Sheils, C.A.; Finkelstein, J.A.; Graham, D.A.; Wilson, J.M. Pulmonary Support on Day of Life 30 Is a Strong Predictor of Increased 1 and 5-Year Morbidity in Survivors of Congenital Diaphragmatic Hernia. J. Pediatr. Surg. 2015, 50, 849–855. [Google Scholar] [CrossRef]
- Basek, P.; Bajrami, S.; Straub, D.; Moeller, A.; Baenziger, O.; Wildhaber, J.; Bernet, V. The Pulmonary Outcome of Long-Term Survivors after Congenital Diaphragmatic Hernia Repair. Swiss Med. Weekly 2008, 138, 173–179. [Google Scholar] [CrossRef]
- Fisher, J.C.; Jefferson, R.A.; Arkovitz, M.S.; Stolar, C.J.H. Redefining Outcomes in Right Congenital Diaphragmatic Hernia. J. Pediatr. Surg. 2008, 43, 373–379. [Google Scholar] [CrossRef]
- Schaible, T.; Kohl, T.; Reinshagen, K.; Brade, J.; Neff, K.W.; Stressig, R.; Büsing, K.A. Right- versus Left-Sided Congenital Diaphragmatic Hernia: Postnatal Outcome at a Specialized Tertiary Care Center. Pediatr. Crit. Care Med. 2012, 13, 66–71. [Google Scholar] [CrossRef]
- Pinton, A.; Boubnova, J.; Becmeur, F.; Kuhn, P.; Senat, M.-V.; Stirnemann, J.; Capelle, M.; Rosenblatt, J.; Massardier, J.; Vaast, P.; et al. Is Laterality of Congenital Diaphragmatic Hernia a Reliable Prognostic Factor? French National Cohort Study. Prenat. Diagn. 2020, 40, 949–957. [Google Scholar] [CrossRef]


{kind=link}
| Features and Characteristics | Value |
|---|---|
| Observed/expected FLV (%) | 29 [26–38] |
| Median GW | 36 [31–40] |
| Prematurity | 2 (20) |
| Male | 3 (30) |
| Time of death: | |
| Before 24 h of life | 1 (10) |
| After 24 h of life, without hospital discharge | 6 (60) |
| Between hospital discharge and 2 years of age | 3 (30) |
| Features and Characteristics | Value |
|---|---|
| Observed/expected FLV (%) | 39 [33–49] |
| Median GW | 39 [38 + 5–40] |
| Prematurity | 4 (9) |
| Male | 28 (60) |
| Intrathoracic liver herniation | 16 (34) |
| Patch repair | 15 (32) |
| Median total O2 duration (days) | 14 [5–34] |
| Median mechanical ventilation duration (days) | 5 [3–9] |
| HFO | 9 (19) |
| Median HFO duration (days) | 4 [3–7] |
| ECMO | 2 (4) |
| CLD | 13 (28) |
| Features and Characteristics | Value | o/e FLV | p |
|---|---|---|---|
| ICS daily treatment < consecutive months | |||
| Yes | 16 (34) | 33% [28–41] | 0.027 |
| No | 31 (66) | 44% [34–58] | |
| ≥1 hospitalization for acute respiratory illness | |||
| Yes | 13 (28) | 34% [32–41] | 0.082 |
| No | 34 (72) | 42% [33–52] | |
| Outcome | |||
| Favorable | 28 (60) | 45% [35–59] | 0.024 |
| Unfavorable | 19 (40) | 34% [29–42] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerbelle, V.; Le Duc, K.; Lejeune, S.; Mur, S.; Lerisson, H.; Drumez, E.; Sfeir, R.; Bigot, J.; Verpillat, P.; Boukhris, R.; et al. Fetal Lung Volume Appears to Predict Respiratory Morbidity in Congenital Diaphragmatic Hernia. J. Clin. Med. 2023, 12, 1508. https://doi.org/10.3390/jcm12041508
Cerbelle V, Le Duc K, Lejeune S, Mur S, Lerisson H, Drumez E, Sfeir R, Bigot J, Verpillat P, Boukhris R, et al. Fetal Lung Volume Appears to Predict Respiratory Morbidity in Congenital Diaphragmatic Hernia. Journal of Clinical Medicine. 2023; 12(4):1508. https://doi.org/10.3390/jcm12041508
Chicago/Turabian StyleCerbelle, Valentine, Kévin Le Duc, Stephanie Lejeune, Sébastien Mur, Héloise Lerisson, Elodie Drumez, Rony Sfeir, Julien Bigot, Pauline Verpillat, Riadh Boukhris, and et al. 2023. "Fetal Lung Volume Appears to Predict Respiratory Morbidity in Congenital Diaphragmatic Hernia" Journal of Clinical Medicine 12, no. 4: 1508. https://doi.org/10.3390/jcm12041508