
Prognostic Utility of the Modified Glasgow Prognostic Score in Urothelial Carcinoma: Outcomes from a Pooled Analysis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Literature Search Strategy
2.3. Inclusion/Exclusion Criteria
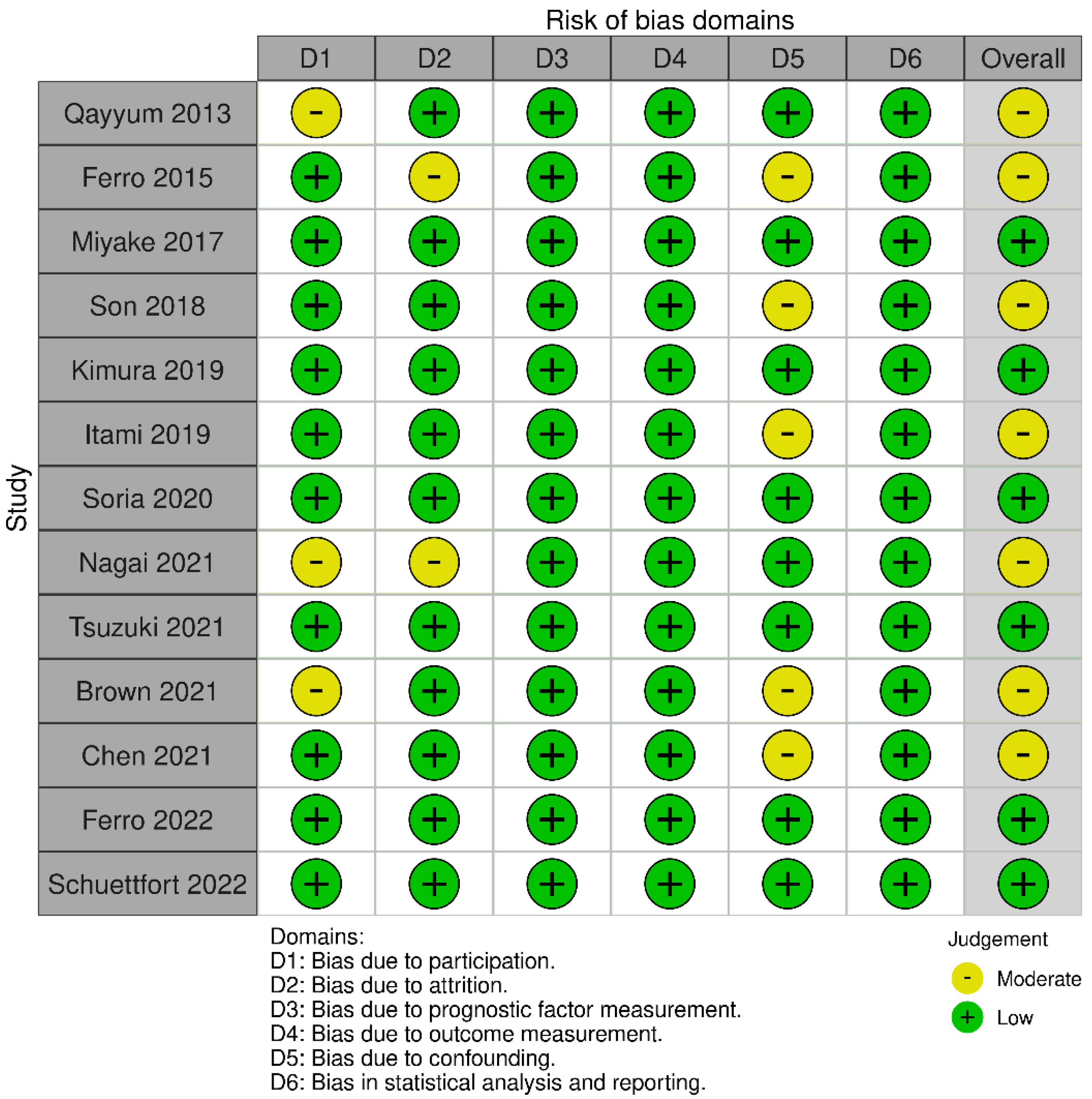
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
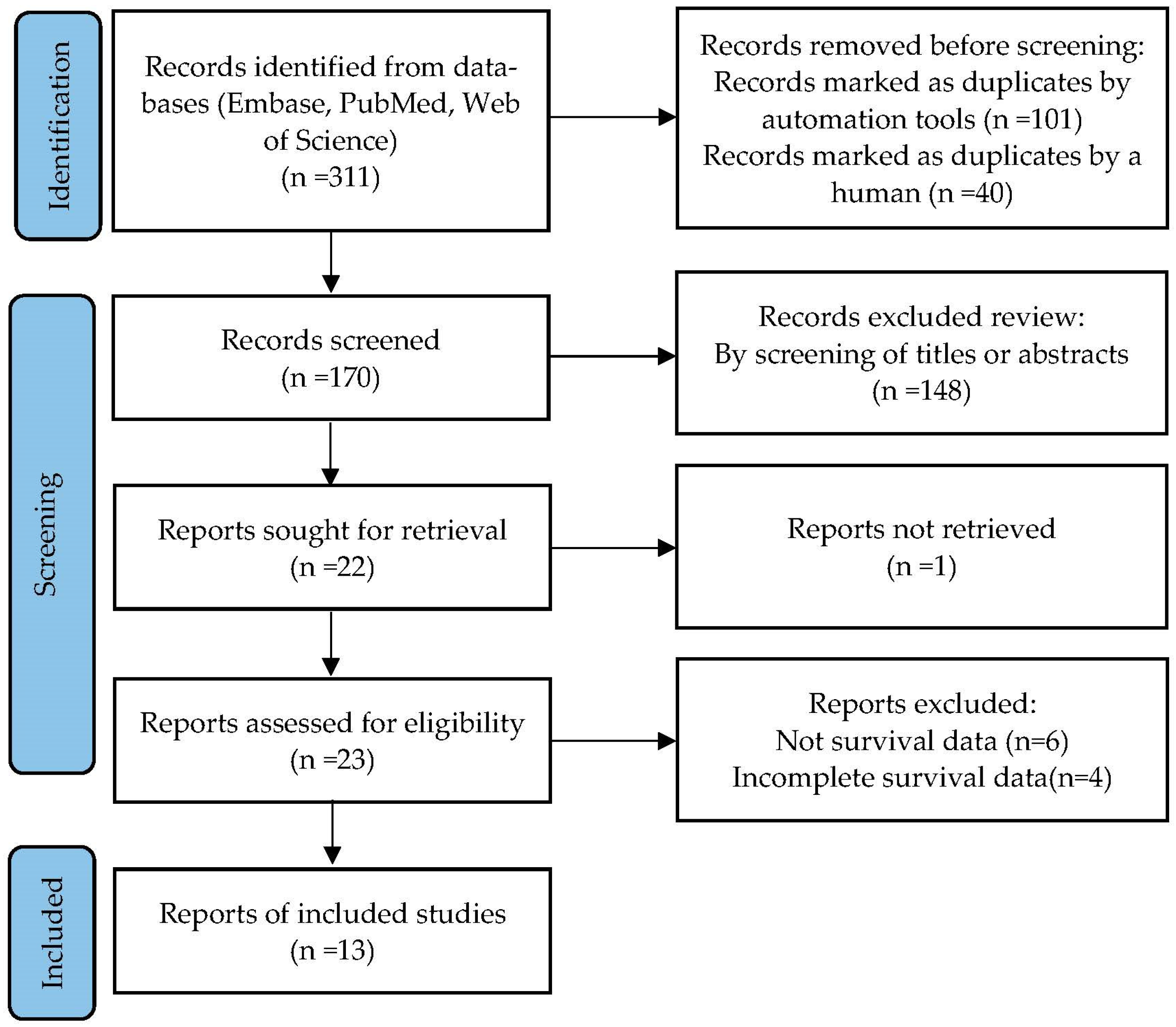
3.1. Study Selection
3.2. Study Characteristics
3.3. mGPS and OS
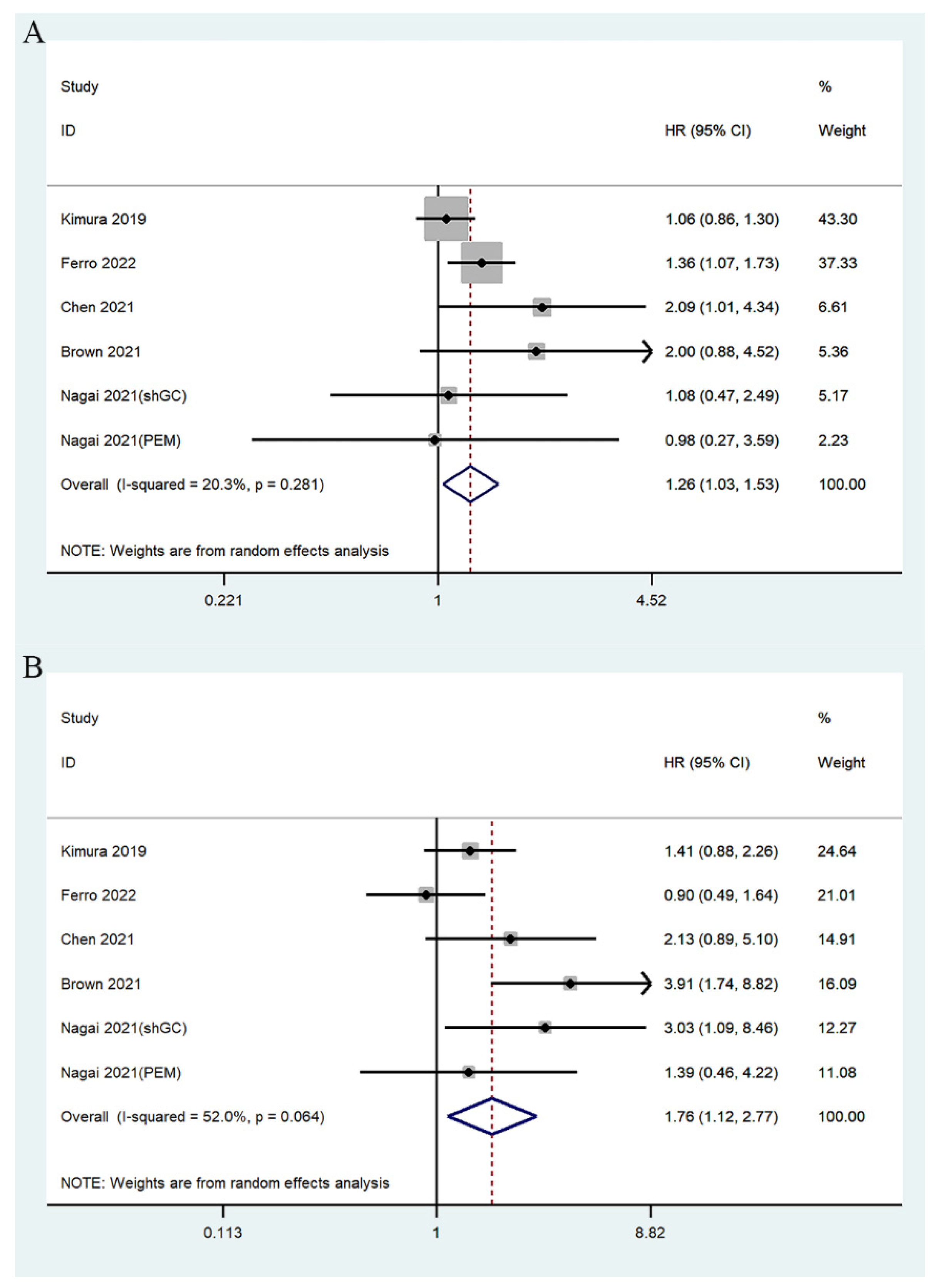
3.4. mGPS and PFS
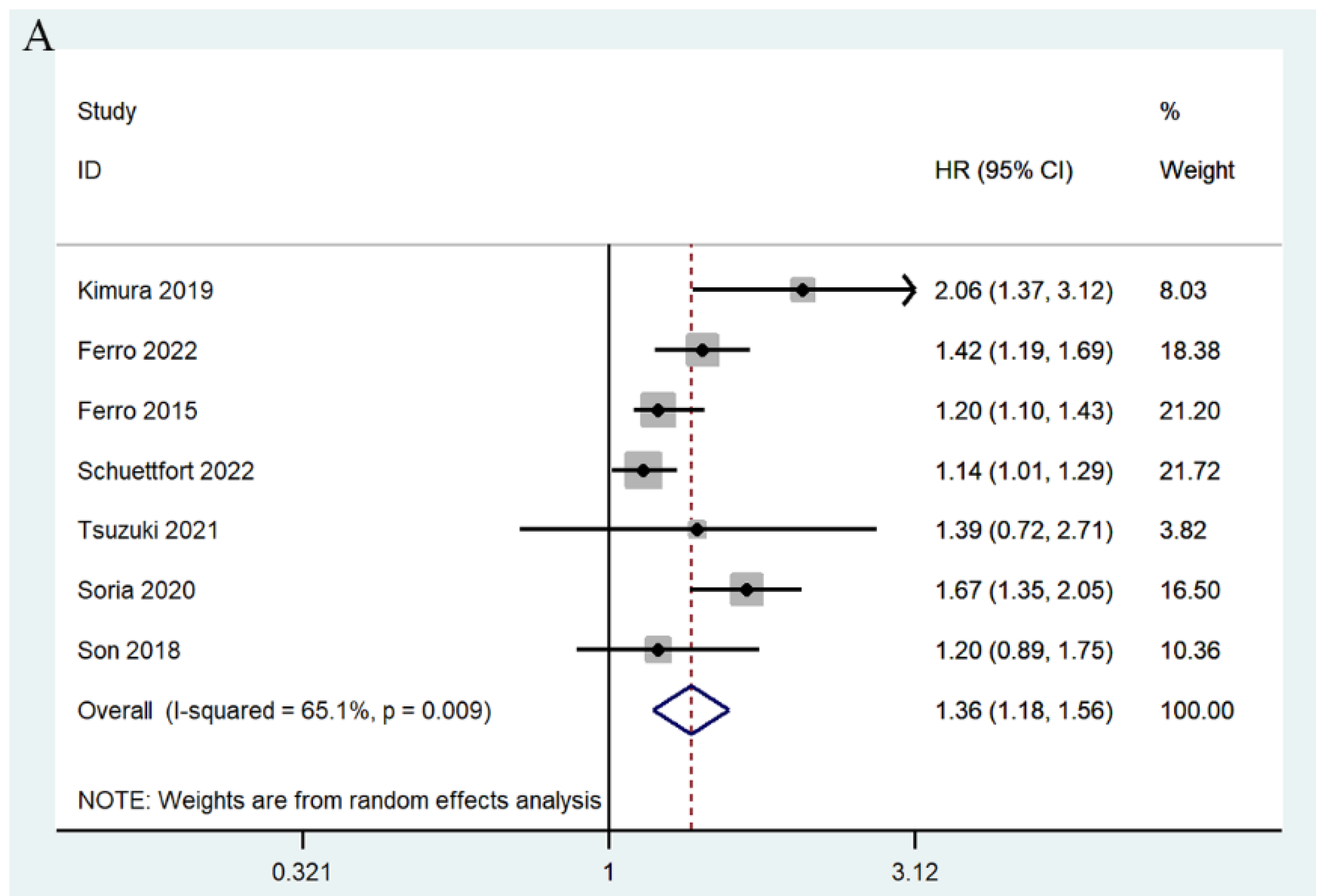
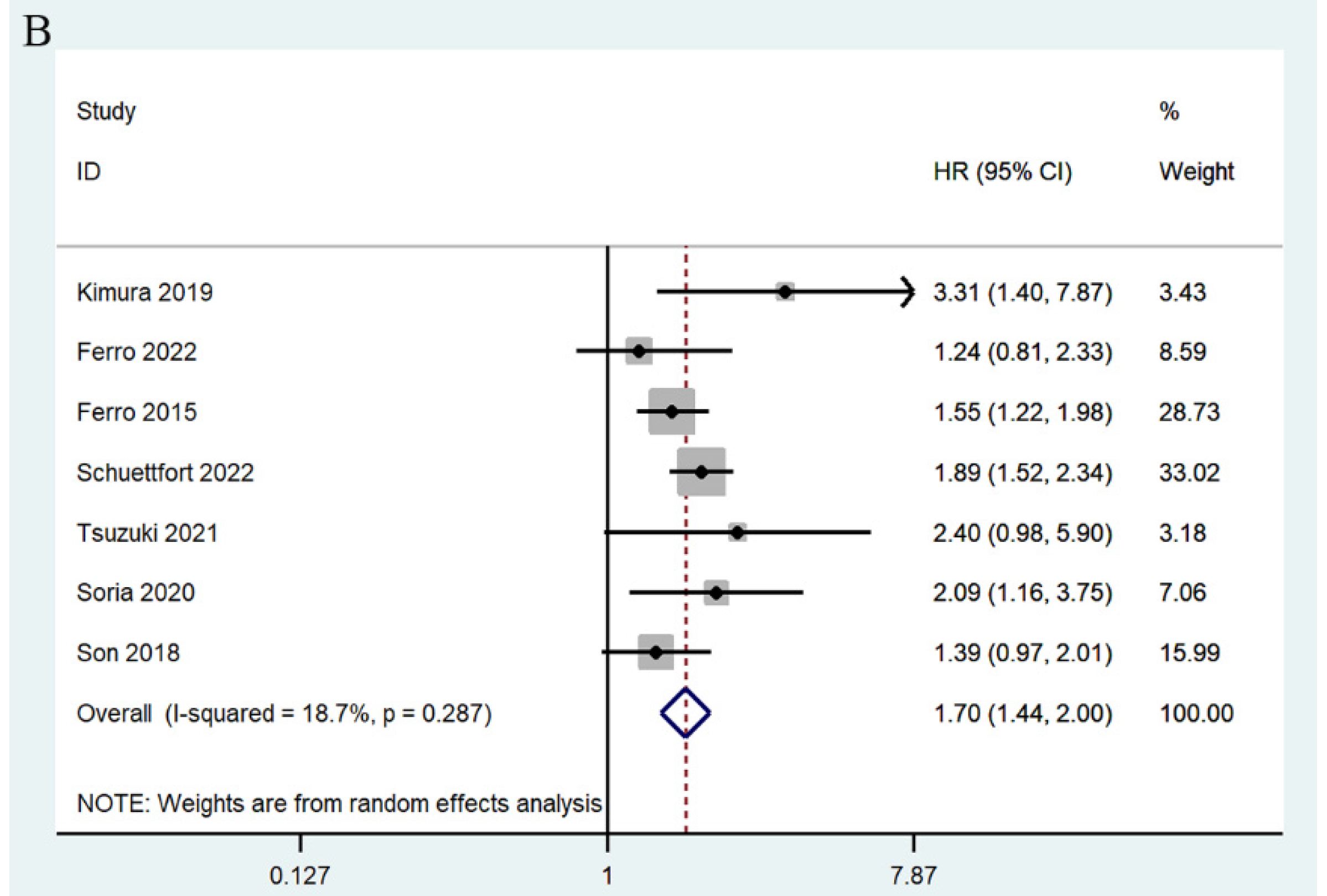
3.5. mGPS and RFS
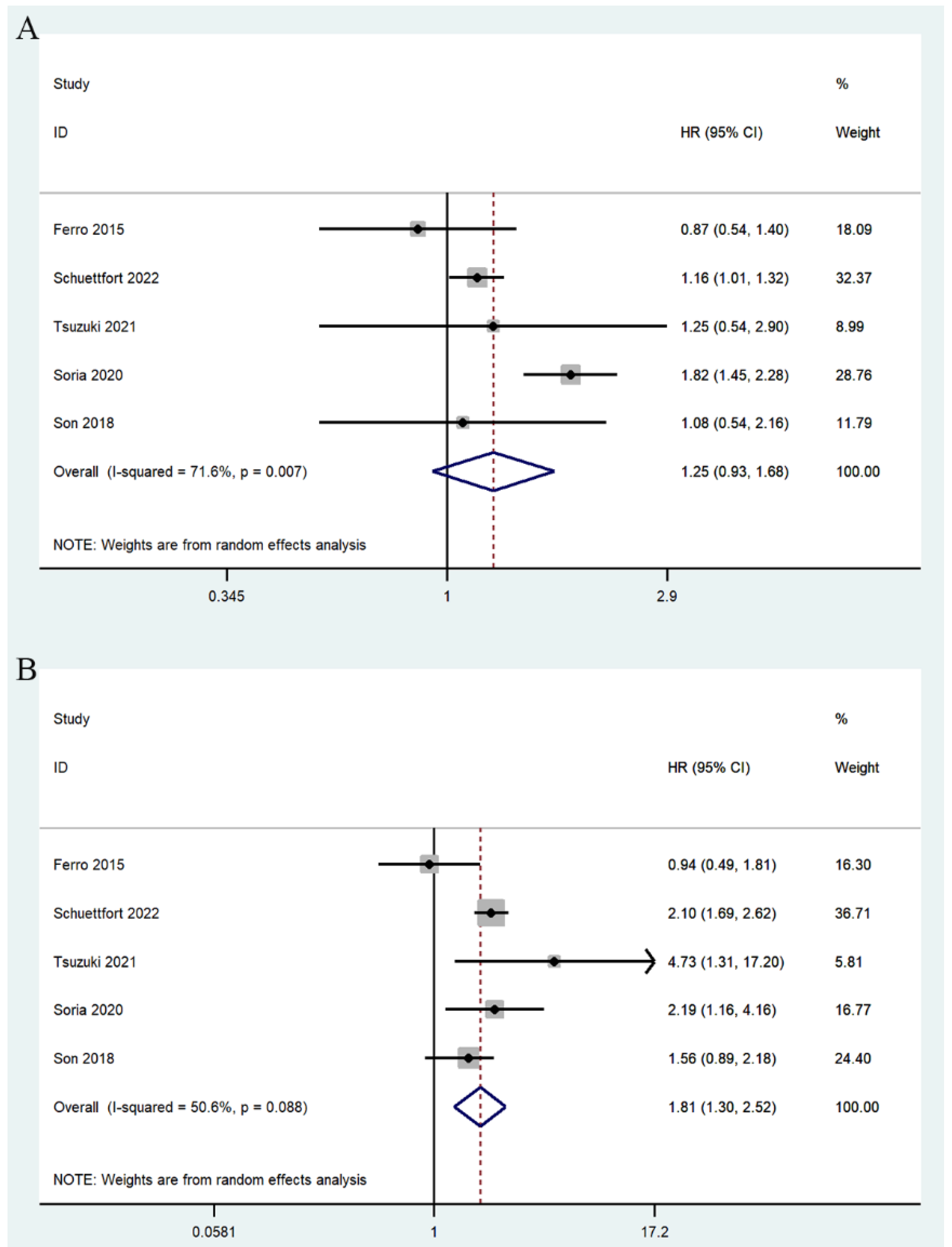
3.6. mGPS and CSS
3.7. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmadi, H.; Duddalwar, V.; Daneshmand, S. Diagnosis and Staging of Bladder Cancer. Hematol Oncol Clin. N. Am 2021, 35, 531–541. [Google Scholar]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2021, 79, 62–79. [Google Scholar]
- Terakawa, T.; Miyake, H.; Muramaki, M.; Takenaka, A.; Hara, I.; Fujisawa, M. Risk Factors for Intravesical Recurrence After Surgical Management of Transitional Cell Carcinoma of the Upper Urinary Tract. Urology 2008, 71, 123–127. [Google Scholar]
- Katims, A.B.; Say, R.; Derweesh, I.; Uzzo, R.; Minervini, A.; Wu, Z.; Abdollah, F.; Sundaram, C.; Ferro, M.; Rha, K.; et al. Risk Factors for Intravesical Recurrence after Minimally Invasive Nephroureterectomy for Upper Tract Urothelial Cancer (ROBUUST Collaboration). J. Urol. 2021, 206, 568–576. [Google Scholar]
- Elawdy, M.M.; Osman, Y.; Taha, D.E.; Zahran, M.H.; El-Halwagy, S.; Garba, M.E.; Harraz, A.M. Risk factors and prognosis of intravesical recurrence after surgical management of upper tract urothelial carcinoma: A 30-year single centre experience. Arab. J. Urol. 2019, 15, 216–222. [Google Scholar]
- Fernandez-Gomez, J.; Madero, R.; Solsona, E.; Unda, M.; Martinez-Piñeiro, L.; Gonzalez, M.; Portillo, J.; Ojea, A.; Pertusa, C.; Rodriguez-Molina, J.; et al. Predicting nonmuscle invasive bladder cancer recurrence and progression in patients treated with bacillus Calmette-Guerin: The CUETO scoring model. J. Urol. 2009, 182, 2195–2203. [Google Scholar]
- Sylvester, R.J.; van der Meijden, A.P.M.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar]
- Fernandez-Gomez, J.; Madero, R.; Solsona, E.; Unda, M.; Martinez-Piñeiro, L.; Ojea, A.; Portillo, J.; Montesinos, M.; Gonzalez, M.; Pertusa, C.; et al. The EORTC Tables Overestimate the Risk of Recurrence and Progression in Patients with Non–Muscle-Invasive Bladder Cancer Treated with Bacillus Calmette-Guérin: External Validation of the EORTC Risk Tables. Eur. Urol. 2011, 60, 423–430. [Google Scholar]
- Xylinas, E.; Kent, M.; Kluth, L.; Pycha, A.; Comploj, E.; Svatek, R.S.; Lotan, Y.; Trinh, Q.D.; Karakiewicz, P.I.; Holmang, S.; et al. Accuracy of the EORTC risk tables and of the CUETO scoring model to predict outcomes in non-muscle-invasive urothelial carcinoma of the bladder. Br. J. Cancer 2013, 109, 1460–1466. [Google Scholar]
- Chung, J.-W.; Kim, J.W.; Lee, E.H.; Chun, S.Y.; Park, D.J.; Byeon, K.H.; Choi, S.H.; Lee, J.N.; Kim, B.S.; Tae, H.; et al. Prognostic Significance of the Neutrophil-to-Lymphocyte Ratio in Patients with Non-Muscle Invasive Bladder Cancer treated with Intravesical Bacillus Calmette–Guérin and the Relationship with the CUETO Scoring Model. Urol. J. 2021, 18, 6765. [Google Scholar]
- Hauth, F.; Roberts, H.J.; Hong, T.S.; Duda, D.G. Leveraging Blood-Based Diagnostics to Predict Tumor Biology and Extend the Application and Personalization of Radiotherapy in Liver Cancers. Int. J. Mol. Sci. 2022, 23, 1926. [Google Scholar]
- Schuurbiers, M.; Huang, Z.; Saelee, S.; Javey, M.; de Visser, L.; van den Broek, D.; Monkhorst, K.; Heuvel Mvd Lovejoy, A.F.; Klass, D. Biological and technical factors in the assessment of blood-based tumor mutational burden (bTMB) in patients with NSCLC. J. ImmunoTherapy Cancer 2022, 10, e004064. [Google Scholar]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, Inflammation, and Cancer. Cell 2010, 140, 883–899. [Google Scholar]
- Ni, X.-C.; Yi, Y.; Fu, Y.-P.; He, H.-W.; Cai, X.-Y.; Wang, J.-X.; Zhou, J.; Cheng, Y.-F.; Jin, J.-J.; Fan, J.; et al. Prognostic Value of the Modified Glasgow Prognostic Score in Patients Undergoing Radical Surgery for Hepatocellular Carcinoma. Medicine 2015, 94, e1486. [Google Scholar]
- Chen, Z.; Nonaka, H.; Onishi, H.; Nakatani, E.; Sato, Y.; Funayama, S.; Watanabe, H.; Komiyama, T.; Kuriyama, K.; Marino, K.; et al. Modified Glasgow Prognostic Score is predictive of prognosis for non-small cell lung cancer patients treated with stereotactic body radiation therapy: A retrospective study. J. Radiat. Res. 2021, 62, 457–464. [Google Scholar]
- Golder, A.M.; McMillan, D.C.; Park, J.H.; Mansouri, D.; Horgan, P.G.; Roxburgh, C.S. The prognostic value of combined measures of the systemic inflammatory response in patients with colon cancer: An analysis of 1700 patients. Br. J. Cancer 2021, 124, 1828–1835. [Google Scholar]
- Ferro, M.; De Cobelli, O.; Buonerba, C.; Di Lorenzo, G.; Capece, M.; Bruzzese, D.; Autorino, R.; Bottero, D.; Cioffi, A.; Matei, D.V.; et al. Modified Glasgow Prognostic Score is Associated with Risk of Recurrence in Bladder Cancer Patients After Radical Cystectomy. Medicine 2015, 94, e1861. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar]
- Sternea, J.A.C.; Gavaghanb, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar]
- Qayyum, T.; McArdle, P.; Hilmy, M.; Going, J.; Orange, C.; Seywright, M.; Horgan, P.; Underwood, M.; Edwards, J. A Prospective Study of the Role of Inflammation in Bladder Cancer. Curr. Urol. 2013, 6, 189–193. [Google Scholar]
- Miyake, M.; Morizawa, Y.; Hori, S.; Marugami, N.; Iida, K.; Ohnishi, K.; Gotoh, D.; Tatsumi, Y.; Nakai, Y.; Inoue, T.; et al. Integrative Assessment of Pretreatment Inflammation-, Nutrition-, and Muscle-Based Prognostic Markers in Patients with Muscle-Invasive Bladder Cancer Undergoing Radical Cystectomy. Oncology 2017, 93, 259–269. [Google Scholar]
- Kimura, S.; D’ Andrea, D.; Soria, F.; Foerster, B.; Abufaraj, M.; Vartolomei, M.D.; Iwata, T.; Karakiewicz, P.I.; Rink, M.; Gust, K.M.; et al. Prognostic value of modified Glasgow Prognostic Score in non–muscle-invasive bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2019, 37, e119–e179. [Google Scholar]
- Son, S.; Hwang, E.-C.; Jung, S.-I.; Kwon, D.-D.; Choi, S.-H.; Kwon, T.-G.; Noh, J.-H.; Kim, M.-K.; Seo, I.-Y.; Kim, C.-S.; et al. Prognostic value of preoperative systemic inflammation markers in localized upper tract urothelial cell carcinoma: A large, multicenter cohort analysis. Minerva Urol. Nephrol. 2018, 70, 300–309. [Google Scholar]
- Itami, Y.; Miyake, M.; Tatsumi, Y.; Gotoh, D.; Hori, S.; Morizawa, Y.; Iida, K.; Ohnishi, K.; Nakai, Y.; Inoue, T.; et al. Preoperative predictive factors focused on inflammation-, nutrition-, and muscle-status in patients with upper urinary tract urothelial carcinoma undergoing nephroureterectomy. Int. J. Clin. Oncol. 2019, 24, 533–545. [Google Scholar]
- Soria, F.; Giordano, A.; D’Andrea, D.; Moschini, M.; Rouprêt, M.; Margulis, V.; Karakiewicz, P.I.; Briganti, A.; Bensalah, K.; Mathieu, R.; et al. Prognostic value of the systemic inflammation modified Glasgow prognostic score in patients with upper tract urothelial carcinoma (UTUC) treated with radical nephroureterectomy: Results from a large multicenter international collaboration. Urol. Oncol. Semin. Orig. Investig. 2020, 38, e602–e611. [Google Scholar]
- Tsuzuki, S.; Kimura, S.; Fukuokaya, W.; Yanagisawa, T.; Hata, K.; Miki, J.; Kimura, T.; Abe, H.; Egawa, S. Modified Glasgow prognostic score is a pre-surgical prognostic marker of disease mortality in upper urinary tract urothelial carcinoma. Jpn. J. Clin. Oncol. 2021, 51, 138–144. [Google Scholar]
- Brown, J.T.; Liu, Y.; Shabto, J.M.; Martini, D.J.; Ravindranathan, D.; Hitron, E.E.; Russler, G.A.; Caulfield, S.; Yantorni, L.B.; Joshi, S.S.; et al. Baseline Modified Glasgow Prognostic Score Associated with Survival in Metastatic Urothelial Carcinoma Treated with Immune Checkpoint Inhibitors. Oncologist 2021, 26, 397–405. [Google Scholar]
- Chen, J.; Hao, L.; Zhang, S.; Zhang, Y.; Dong, B.; Zhang, Q.; Han, C. Preoperative Fibrinogen–Albumin Ratio, Potential Prognostic Factors for Bladder Cancer Patients Undergoing Radical Cystectomy: A Two-Center Study. Cancer Manag. Res. 2021, 13, 3181–3192. [Google Scholar]
- Schuettfort, V.M.; Gust, K.; D’Andrea, D.; Quhal, F.; Mostafaei, H.; Laukhtina, E.; Mori, K.; Rink, M.; Abufaraj, M.; Karakiewicz, P.I.; et al. Impact of the preoperative modified Glasgow Prognostic Score on disease outcome after radical cystectomy for urothelial carcinoma of the bladder. Minerva Urol. Nephrol. 2022, 74, 302–312. [Google Scholar]
- Nagai, T.; Naiki, T.; Isobe, T.; Sugiyama, Y.; Etani, T.; Iida, K.; Nozaki, S.; Noda, Y.; Shimizu, N.; Tasaki, Y.; et al. Modified Glasgow Prognostic Score 2 as a Prognostic Marker in Patients with Metastatic Urothelial Carcinoma. Vivo 2021, 35, 2793–2800. [Google Scholar]
- Ferro, M.; Tătaru, O.S.; Musi, G.; Lucarelli, G.; Abu Farhan, A.R.; Cantiello, F.; Damiano, R.; Hurle, R.; Contieri, R.; Busetto, G.M.; et al. Modified Glasgow Prognostic Score as a Predictor of Recurrence in Patients with High Grade Non-Muscle Invasive Bladder Cancer Undergoing Intravesical Bacillus Calmette–Guerin Immunotherapy. Diagnostics 2022, 12, 586. [Google Scholar]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Syn. Meth. 2021, 12, 55–61. [Google Scholar]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non–muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar]
- Mastroianni, R.; Brassetti, A.; Krajewski, W.; Zdrojowy, R.; Salhi, Y.A.; Anceschi, U.; Bove, A.M.; Carbone, A.; De Nunzio, C.; Fuschi, A.; et al. Assessing the Impact of the Absence of Detrusor Muscle in Ta Low-grade Urothelial Carcinoma of the Bladder on Recurrence-free Survival. Eur. Urol. Focus 2021, 7, 1324–1331. [Google Scholar]
- Cicione, A.; Manno, S.; Ucciero, G.; Cantiello, F.; Damiano, R.; Lima, E.; Posti, A.; Balloni, F.; De Nunzio, C. A larger detrusor wall thickness increases the risk of non muscle invasive bladder cancer recurrence and progression: Result from a multicenter observational study. Minerva Urol. E Nefrol. Ital. J. Urol. Nephrol. 2018, 70, 310–318. [Google Scholar]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Linares Espinós, E.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar]
- De Nunzio, C.; Cicione, A.; Leonardo, F.; Rondoni, M.; Franco, G.; Cantiani, A.; Tubaro, A.; Leonardo, C. Extraperitoneal radical cystectomy and ureterocutaneostomy in octogenarians. Int. Urol. Nephrol. 2010, 43, 663–667. [Google Scholar]
- De Nunzio, C.; Cicione, A.; Izquierdo, L.; Lombardo, R.; Tema, G.; Lotrecchiano, G.; Minervini, A.; Simone, G.; Cindolo, L.; D’Orta, C.; et al. Multicenter Analysis of Postoperative Complications in Octogenarians After Radical Cystectomy and Ureterocutaneostomy: The Role of the Frailty Index. Clin. Genitourin. Cancer 2019, 17, 402–407. [Google Scholar]
- Mastroianni, R.; Ferriero, M.; Tuderti, G.; Anceschi, U.; Bove, A.M.; Brassetti, A.; Misuraca, L.; Zampa, A.; Torregiani, G.; Ghiani, E.; et al. Open Radical Cystectomy versus Robot-Assisted Radical Cystectomy with Intracorporeal Urinary Diversion: Early Outcomes of a Single-Center Randomized Controlled Trial. J. Urol. 2022, 207, 982–992. [Google Scholar]
- Mastroianni, R.; Tuderti, G.; Anceschi, U.; Bove, A.M.; Brassetti, A.; Ferriero, M.; Zampa, A.; Giannarelli, D.; Guaglianone, S.; Gallucci, M.; et al. Comparison of Patient-reported Health-related Quality of Life Between Open Radical Cystectomy and Robot-assisted Radical Cystectomy with Intracorporeal Urinary Diversion: Interim Analysis of a Randomised Controlled Trial. Eur. Urol. Focus 2022, 8, 465–471. [Google Scholar]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar]
- Miyama, Y.; Kaneko, G.; Nishimoto, K.; Yasuda, M. Lower neutrophil-to-lymphocyte ratio and positive programmed cell death ligand-1 expression are favorable prognostic markers in patients treated with pembrolizumab for urothelial carcinoma. Cancer Med. 2022. [Google Scholar] [CrossRef]
- Sari Motlagh, R.; Schuettfort, V.M.; Mori, K.; Katayama, S.; Rajwa, P.; Aydh, A.; Grossmann, N.C.; Laukhtina, E.; Pradere, B.; Mostafai, H.; et al. Prognostic impact of insulin-like growth factor-I and its binding proteins, insulin-like growth factor-I binding protein-2 and -3, on adverse histopathological features and survival outcomes after radical cystectomy. Int. J. Urol. 2022, 29, 676–683. [Google Scholar]
- Jan, H.-C.; Hu, C.-Y.; Yang, W.-H.; Ou, C.-H. Combination of Platelet-Lymphocyte Ratio and Monocyte-Lymphocyte Ratio as a New Promising Prognostic Factor in Upper Tract Urothelial Carcinoma with Large Tumor Sizes > 3 cm. Clin. Genitourin. Cancer 2020, 18, e484–e500. [Google Scholar]
- Sjödahl, G.; Abrahamsson, J.; Holmsten, K.; Bernardo, C.; Chebil, G.; Eriksson, P.; Johansson, I.; Kollberg, P.; Lindh, C.; Lövgren, K.; et al. Different Responses to Neoadjuvant Chemotherapy in Urothelial Carcinoma Molecular Subtypes. Eur. Urol. 2022, 81, 523–532. [Google Scholar]
- Chiang, P.-J.; Xu, T.; Cha, T.-L.; Tsai, Y.-T.; Liu, S.-Y.; Wu, S.-T.; Meng, E.; Tsao, C.-W.; Kao, C.-C.; Chen, C.-L.; et al. Programmed Cell Death Ligand 1 Expression in Circulating Tumor Cells as a Predictor of Treatment Response in Patients with Urothelial Carcinoma. Biology 2021, 10, 674. [Google Scholar]
- Vlachostergios, P.J. The interplay of cell cycle and DNA repair gene alterations in upper tract urothelial carcinoma: Predictive and prognostic implications. Precis. Clin. Med. 2020, 3, 153–160. [Google Scholar]
- Wang, Y.; Wang, K.; Ni, J.; Zhang, H.; Yin, L.; Zhang, Y.; Shi, H.; Zhang, T.; Zhou, N.; Mao, W.; et al. Combination of C-Reactive Protein and Neutrophil-to-Lymphocyte Ratio as a Novel Prognostic Index in Patients with Bladder Cancer After Radical Cystectomy. Front. Oncol. 2021, 11, 762470. [Google Scholar]
- Saito, H.; Kono, Y.; Murakami, Y.; Shishido, Y.; Kuroda, H.; Matsunaga, T.; Fukumoto Yo Osaki, T.; Ashida, K.; Fujiwara, Y. Postoperative Serum Albumin is a Potential Prognostic Factor for Older Patients with Gastric Cancer. Yonago Acta Med. 2018, 61, 72–78. [Google Scholar]
- He, X.; Li, J.-P.; Liu, X.-H.; Zhang, J.-P.; Zeng, Q.-Y.; Chen, H.; Chen, S.-L. Prognostic value of C-reactive protein/albumin ratio in predicting overall survival of Chinese cervical cancer patients overall survival: Comparison among various inflammation based factors. J. Cancer 2018, 9, 1877–1884. [Google Scholar]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br. J. Cancer 2003, 89, 1028–1030. [Google Scholar]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Comparison of an inflammation-based prognostic score (GPS) with performance status (ECOG) in patients receiving platinum-based chemotherapy for inoperable non-small-cell lung cancer. Br. J. Cancer 2004, 90, 1704–1706. [Google Scholar]
- McMillan, D.C.; Crozier, J.E.M.; Canna, K.; Angerson, W.J.; McArdle, C.S. Evaluation of an inflammation-based prognostic score (GPS) in patients undergoing resection for colon and rectal cancer. Int. J. Color. Dis. 2007, 22, 881–886. [Google Scholar]
- Proctor, M.J.; Talwar, D.; Balmar, S.M.; O’Reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; Morrison, D.S.; McMillan, D.C. The relationship between the presence and site of cancer, an inflammation-based prognostic score and biochemical parameters. Initial results of the Glasgow Inflammation Outcome Study. Br. J. Cancer 2010, 103, 870–876. [Google Scholar]
- Jiang, Y.; Xu, D.; Song, H.; Qiu, B.; Tian, D.; Li, Z.; Ji, Y.; Wang, J. Inflammation and nutrition-based biomarkers in the prognosis of oesophageal cancer: A systematic review and meta-analysis. BMJ Open 2021, 11, e048324. [Google Scholar]
- Wu, D.; Wang, X.; Sh, G.; Sun, H.; Ge, G. Prognostic and clinical significance of modified glasgow prognostic score in pancreatic cancer: A meta-analysis of 4629 patients. Aging 2021, 13, 1410–1421. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| mGPS | Points Allocated |
|---|---|
| CRP ≤ 10 mg/L and albumin ≥ 35 g/L | 0 |
| CRP > 10 mg/L | 1 |
| CRP > 10 mg/L and albumin < 35 g/L | 2 |
| Author | Year | Country | Study Design | Tumor Type | mGPS Group | Treatment | Sample Size | Age (Years) | Analysis Method | Survival Analysis | Follow-Up (Months) | Quality Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Qayyum et al. [22] | 2013 | United Kingdom | Retrospective | BC | High/low | Non-Surgery | 68 | Median72 (range, 43–93) | Multivariate | CSS | Median47 (range, 1.2–201) | 8 |
| Ferro et al. [17] | 2015 | Italy | Retrospective | BC | 0/1/2 | RC | 1037 | Median70 (range, 42–88) | Multivariate | RFS/OS/CSS | Median22 (range, 3–60) | 9 |
| Miyake et al. [23] | 2017 | Japan | Retrospective | BC | High/low | RC | 117 | Median72 (IQR, 61–77) | Multivariate | OS | Median22 (IQR, 10–64) | 8 |
| Son et al. [25] | 2018 | Korea | Retrospective | UTUC | 0/1/2 | RNU | 1137 | Median69 (IQR, 61–74) | Multivariate | RFS/CSS | Median39.1 (IQR, 18.3–63.8) | 9 |
| Kimura et al. [24] | 2019 | Austria | Retrospective | BC | 0/1/2 | TURB | 1096 | Median67 (IQR, 58–74) | Multivariate | PFS/RFS | Median64.8 (IQR, 26.5–110.9) | 8 |
| Itami et al. [26] | 2019 | Japan | Retrospective | UTUC | High/low | RNU | 125 | Median72 (range, 38–90) | Multivariate | OS | Median51 (range, 6–227) | 8 |
| Soria et al. [27] | 2020 | Italy | Retrospective | UTUC | 0/1/2 | RNU | 2492 | Median69 (IQR, 61–76) | Multivariate | RFS/CSS/OS | Median45 (IQR, 20–81) | 9 |
| Nagai et al. [32] | 2021 | Japan | Retrospective | mUC | High/low | shGC | 68 | - | Multivariate | CSS/PFS | - | 6 |
| Nagai et al. [32] | 2021 | Japan | Retrospective | mUC | High/low | PEM | 74 | - | Multivariate | CSS/PFS | - | 6 |
| Tsuzuki et al. [28] | 2021 | Japan | Retrospective | UTUC | 0/1/2 | RNU | 273 | Median71 (IQR, 63–77) | Multivariate | RFS/CSS/OS | Median36.1 | 8 |
| Brown et al. [29] | 2021 | USA | Retrospective | mUC | 0/1/2 | ICIs | 53 | Median70 (range, 32–86) | Multivariate | PFS/OS | Median27.1 | 8 |
| Chen et al. [30] | 2021 | China | Retrospective | BC | 0/1/2 | RC | 267 | - | Univariate | PFS/OS | - | 8 |
| Ferro et al. [33] | 2022 | Italy | Retrospective | BC | 0/1/2 | BCG | 1382 | Mean69.87 (IQR, 60.16–79.58) | Multivariate | PFS/RFS | Median44 (IQR, 36–58) | 9 |
| Schuettfort et al. [31] | 2022 | Austria | Retrospective | BC | 0/1/2 | RC | 4335 | Median67 (IQR, 60–73) | Multivariate | RFS/OS/CSS | Median41 (IQR, 18.3–60.8) | 9 |
| Outcome | Variable | No. of Studies | Model | HR (95% CI) | p | Heterogeneity | |
|---|---|---|---|---|---|---|---|
| I2 (%) | p | ||||||
| OS (1/0) | All | 6 | Random | 1.33 (1.12, 1.58) | 0.001 | 45.4 | 0.103 |
| Ethnicity | Caucasian | 4 | Random | 1.29 (1.07, 1.56) | 0.008 | 58.0 | 0.068 |
| Asian | 2 | Random | 1.69 (1.06, 2.70) | 0.029 | 0.0 | 0.657 | |
| Tumor type | BC | 3 | Random | 1.16 (1.06, 1.28) | 0.002 | 0.0 | 0.368 |
| mUC | 1 | - | 2.42 (1.01, 5.80) | 0.048 | - | - | |
| UTUC | 2 | Random | 1.47 (1.22, 1.76) | 0.000 | 0.0 | 0.891 | |
| Sample size | ≤1500 | 4 | Random | 1.44 (1.09, 1.90) | 0.009 | 3.8 | 0.374 |
| >1500 | 2 | Random | 1.28 (1.01, 1.61) | 0.004 | 78.9 | 0.029 | |
| Treatment | Surgery | 5 | Random | 1.29 (1.10, 1.51) | 0.001 | 41.5 | 0.145 |
| Non-Surgery | 1 | - | 2.42 (1.01, 5.80) | 0.048 | - | - | |
| OS (2/0) | All | 6 | Random | 2.02 (1.43, 2.84) | 0.000 | 49.3 | 0.079 |
| Ethnicity | Caucasian | 4 | Random | 1.99 (1.29, 3.06) | 0.002 | 65.6 | 0.033 |
| Asian | 2 | Random | 2.26 (1.13, 4.54) | 0.022 | 49.3 | 0.079 | |
| Tumor type | BC | 3 | Random | 1.78 (1.42, 2.23) | 0.000 | 12.4 | 0.319 |
| mUC | 1 | - | 6.37 (2.46, 16.49) | 0.000 | - | - | |
| UTUC | 2 | Random | 2.08 (1.15, 3.77) | 0.015 | 8.4 | 0.296 | |
| Sample size | ≤1500 | 4 | Random | 2.47 (1.15, 5.31) | 0.020 | 69.3 | 0.021 |
| >1500 | 2 | Random | 1.91 (1.59, 2.28) | 0.000 | 0.0 | 0.802 | |
| Treatment | Surgery | 5 | Random | 1.85 (1.56, 2.18) | 0.000 | 0.0 | 0.474 |
| Non-Surgery | 1 | - | 6.37 (2.46, 16.49) | 0.000 | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, D.; Li, J.; Lin, T.; Tan, P.; Zhang, J.; Xiong, Q.; Jiang, J.; Li, Y.; Zhang, P.; Wei, Q. Prognostic Utility of the Modified Glasgow Prognostic Score in Urothelial Carcinoma: Outcomes from a Pooled Analysis. J. Clin. Med. 2022, 11, 6261. https://doi.org/10.3390/jcm11216261
Tan D, Li J, Lin T, Tan P, Zhang J, Xiong Q, Jiang J, Li Y, Zhang P, Wei Q. Prognostic Utility of the Modified Glasgow Prognostic Score in Urothelial Carcinoma: Outcomes from a Pooled Analysis. Journal of Clinical Medicine. 2022; 11(21):6261. https://doi.org/10.3390/jcm11216261
Chicago/Turabian StyleTan, Daqing, Jinze Li, Tianhai Lin, Ping Tan, Jiapeng Zhang, Qiao Xiong, Jinjiang Jiang, Yifan Li, Peng Zhang, and Qiang Wei. 2022. "Prognostic Utility of the Modified Glasgow Prognostic Score in Urothelial Carcinoma: Outcomes from a Pooled Analysis" Journal of Clinical Medicine 11, no. 21: 6261. https://doi.org/10.3390/jcm11216261