
Comparison between Fourth-Generation FloTrac/Vigileo System and Continuous Thermodilution Technique for Cardiac Output Estimation after Time Adjustment during Off-Pump Coronary Artery Bypass Graft Surgery: A Retrospective Cohort Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Acquisition and Preprocessing
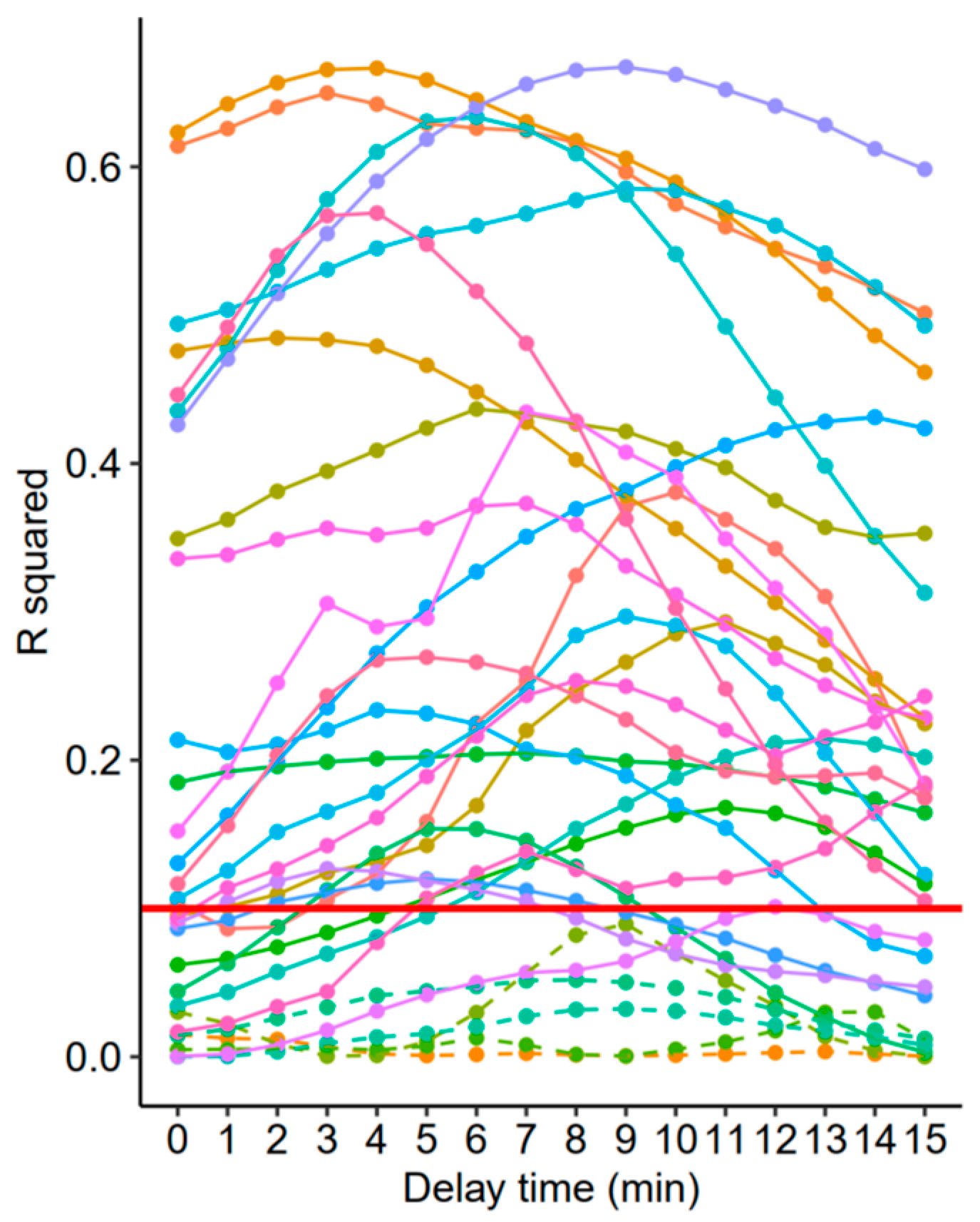
2.3. Time Adjustments
2.4. Sensitivity Analysis
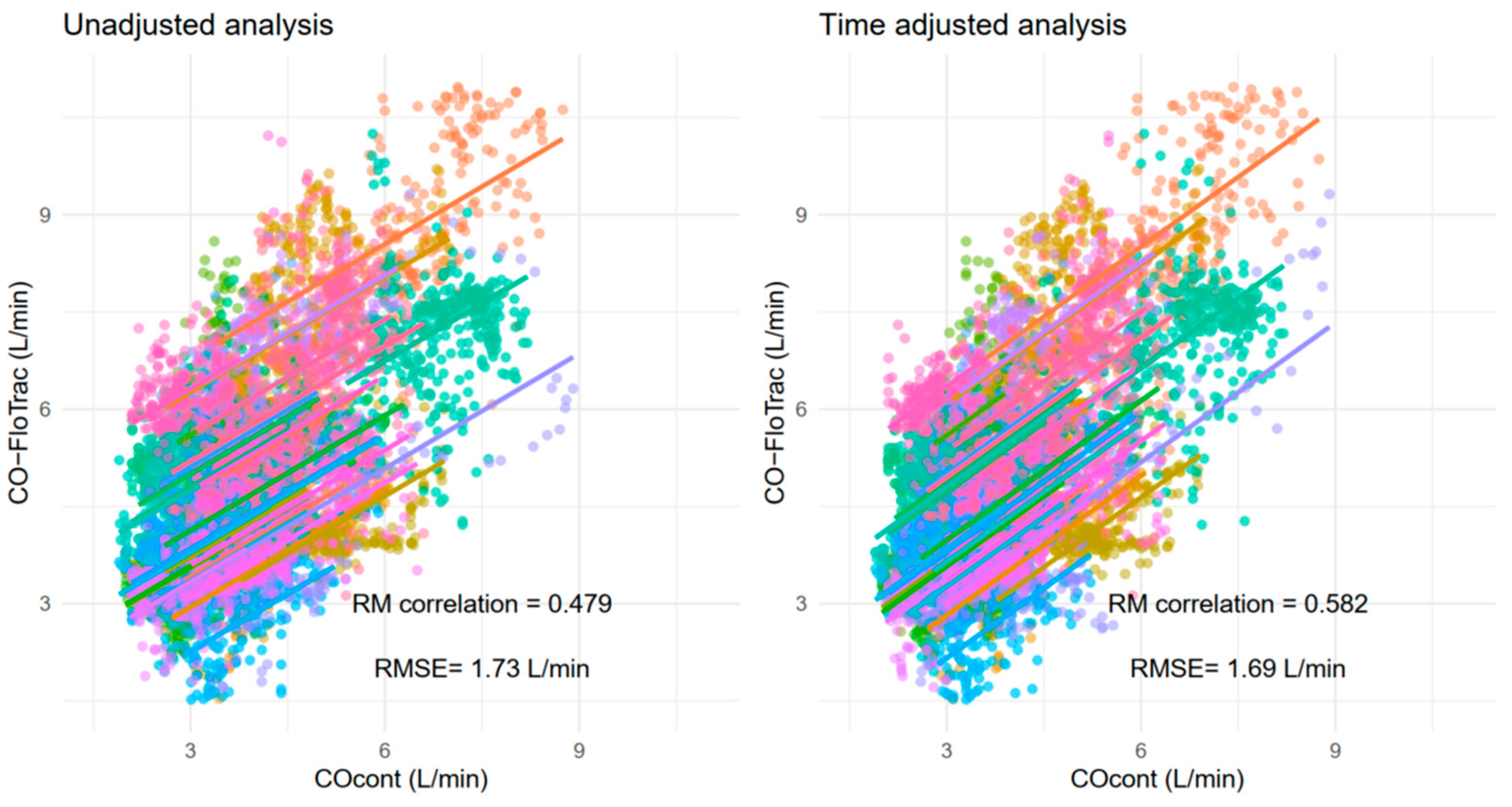
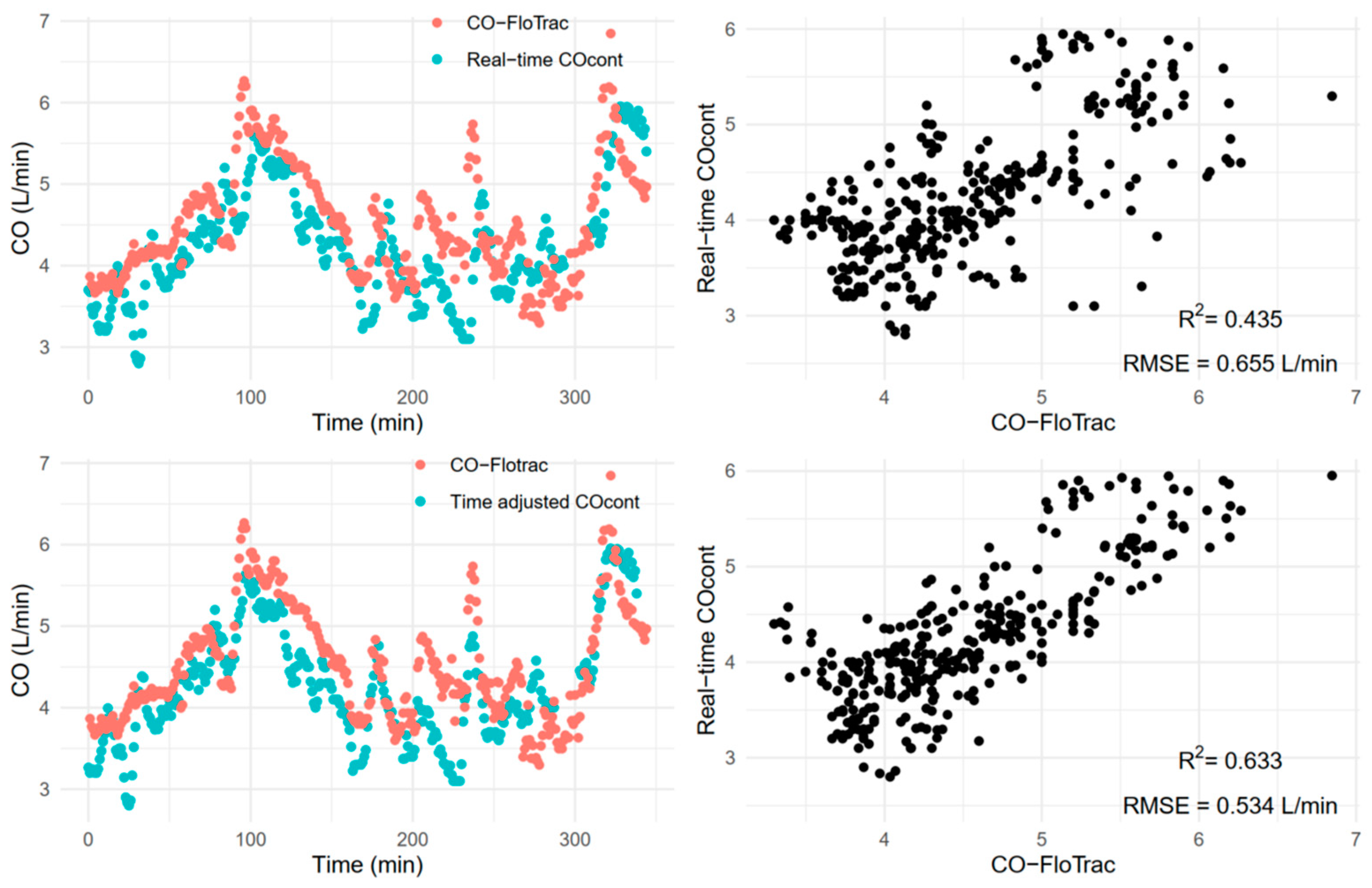
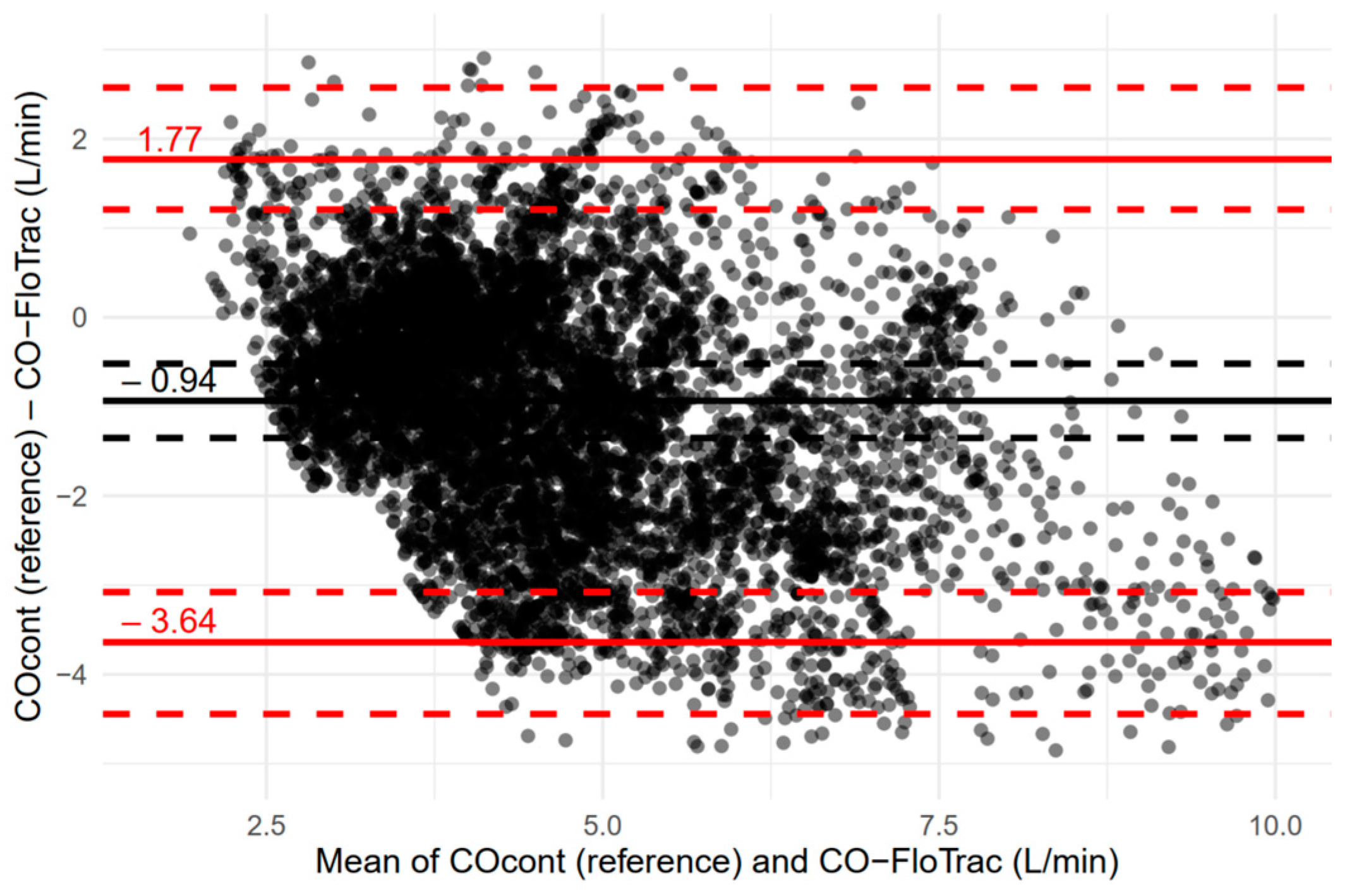
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suehiro, K.; Tanaka, K.; Mikawa, M.; Uchihara, Y.; Matsuyama, T.; Matsuura, T.; Funao, T.; Yamada, T.; Mori, T.; Nishikawa, K. Improved Performance of the Fourth-Generation FloTrac/Vigileo System for Tracking Cardiac Output Changes. J. Cardiothorac. Vasc. Anesth. 2015, 29, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Kusaka, Y.; Ohchi, F.; Minami, T. Evaluation of the Fourth-Generation FloTrac/Vigileo System in Comparison With the Intermittent Bolus Thermodilution Method in Patients Undergoing Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2019, 33, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Hamaguchi, E.; Kubo, N.; Shimokawa, A.; Kanazawa, H.; Ohnishi, Y. The accuracy and trending ability of cardiac index measured by the fourth-generation FloTrac/Vigileo system™ and the Fick method in cardiac surgery patients. J. Clin. Monit. Comput. 2019, 33, 767–776. [Google Scholar] [CrossRef]
- Ylikauma, L.A.; Ohtonen, P.P.; Erkinaro, T.M.; Vakkala, M.A.; Liisanantti, J.H.; Satta, J.U.; Juvonen, T.S.; Kaakinen, T.I. Bioreactance and fourth-generation pulse contour methods in monitoring cardiac index during off-pump coronary artery bypass surgery. J. Clin. Monit. Comput. 2022, 36, 879–888. [Google Scholar] [CrossRef]
- Nadeau, S.; Noble, W.H. Limitations of cardiac output measurements by thermodilution. Can. Anaesth. Soc. J. 1986, 33, 780–784. [Google Scholar] [CrossRef] [Green Version]
- de Lange, F.; Bootsma, I.T.; Boerma, E.C. Letter to the editor in response to “Agreement between continuous and intermittent pulmonary artery thermodilution for cardiac output measurement in perioperative and intensive care medicine: A systematic review and meta-analysis”. Crit. Care 2021, 25, 215. [Google Scholar] [CrossRef]
- Bootsma, I.T.; Boerma, E.C.; Scheeren, T.W.L.; de Lange, F. The contemporary pulmonary artery catheter. Part 2: Measurements, limitations, and clinical applications. J. Clin. Monit. Comput. 2022, 36, 17–31. [Google Scholar] [CrossRef]
- Aranada, M.; Mihm, F.G.; Garrett, S.; Mihm, M.N.; Pearl, R.G. Continuous Cardiac Output Catheters: Delay in In Vitro Response Time after Controlled Flow Changes. Anesthesiology 1998, 89, 1592–1595. [Google Scholar] [CrossRef]
- Lazor, M.A.; Pierce, E.T.; Stanley, G.D.; Cass, J.L.; Halpern, E.F.; Bode, R.H., Jr. Evaluation of the accuracy and response time of STAT-mode continuous cardiac output. J. Cardiothorac. Vasc. Anesth. 1997, 11, 432–436. [Google Scholar] [CrossRef]
- Siegel, L.C.; Hennessy, M.M.; Pearl, R.G. Delayed time response of the continuous cardiac output pulmonary artery catheter. Anesth. Analg. 1996, 83, 1173–1177. [Google Scholar] [CrossRef]
- Mukkamala, R.; Kohl, B.A.; Mahajan, A. Comparison of accuracy of two uncalibrated pulse contour cardiac output monitors in off-pump coronary artery bypass surgery patients using pulmonary artery catheter-thermodilution as a reference. BMC Anesth. 2021, 21, 189. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.B.; Kim, T.H.; Roh, Y.J.; Choi, I.C.; Suh, J.H. Comparison of Uncalibrated Arterial Pressure Waveform Analysis with Continuous Thermodilution Cardiac Output Measurements in Patients Undergoing Elective Off-Pump Coronary Artery Bypass Surgery. J. Cardiothorac Vasc. Anesth. 2010, 24, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-C.; Jung, C.-W. Vital Recorder—A free research tool for automatic recording of high-resolution time-synchronised physiological data from multiple anaesthesia devices. Sci. Rep. 2018, 8, 1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakdash, J.Z.; Marusich, L.R. Repeated Measures Correlation. Front. Psychol. 2017, 8, 456. [Google Scholar] [CrossRef] [Green Version]
- Zou, G.Y. Confidence interval estimation for the Bland-Altman limits of agreement with multiple observations per individual. Stat. Methods Med. Res. 2013, 22, 630–642. [Google Scholar] [CrossRef]
- Critchley, L.A.; Critchley, J.A. A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J. Clin. Monit. Comput. 1999, 15, 85–91. [Google Scholar] [CrossRef]
- Kouz, K.; Michard, F.; Bergholz, A.; Vokuhl, C.; Briesenick, L.; Hoppe, P.; Flick, M.; Schön, G.; Saugel, B. Agreement between continuous and intermittent pulmonary artery thermodilution for cardiac output measurement in perioperative and intensive care medicine: A systematic review and meta-analysis. Crit. Care 2021, 25, 125. [Google Scholar] [CrossRef]
- Saugel, B.; Grothe, O.; Wagner, J.Y. Tracking Changes in Cardiac Output: Statistical Considerations on the 4-Quadrant Plot and the Polar Plot Methodology. Anesth. Analg. 2015, 121, 514–524. [Google Scholar] [CrossRef]
- Cho, Y.J.; Koo, C.H.; Kim, T.K.; Hong, D.M.; Jeon, Y. Comparison of cardiac output measures by transpulmonary thermodilution, pulse contour analysis, and pulmonary artery thermodilution during off-pump coronary artery bypass surgery: A subgroup analysis of the cardiovascular anaesthesia registry at a single tertiary centre. J. Clin. Monit. Comput. 2016, 30, 771–782. [Google Scholar] [CrossRef]
- Argueta, E.; Berdine, G.; Pena, C.; Nugent, K.M. FloTrac® monitoring system: What are its uses in critically ill medical patients? Am. J. Med. Sci. 2015, 349, 352–356. [Google Scholar] [CrossRef]
- Kim, D.H.; Yoo, J.Y.; Lee, S.Y.; Kim, Y.J.; Lee, S.R.; Park, S.Y. Effects of pulse pressure alterations on cardiac output measurements derived from analysis of arterial pressure waveform. Anesth. Pain Med. 2016, 11, 280–284. [Google Scholar] [CrossRef] [Green Version]
- Heijne, A.; Krijtenburg, P.; Bremers, A.; Scheffer, G.J.; Malagon, I.; Slagt, C. Four different methods of measuring cardiac index during cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Korean. J. Anesth. 2021, 74, 120–133. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Age (years) | 65.0 ± 10.6 |
| Sex (F/M) | 5/25 |
| Height (cm) | 164.2 ± 8.2 |
| Weight (kg) | 68.7 ± 11.2 |
| BMI (kg/m2) | 25.4 ± 3.0 |
| Comorbidities | |
| • DM | 18 (60.0) |
| • HTN | 20 (66.7) |
| • Chronic kidney disease | 4 (13.3) |
| ■ No hemodialysis | 2 (6.7) |
| ■ On hemodialysis | 2 (6.7) |
| Left ventricular ejection fraction (%) | |
| • ≥40 | 26 (86.7) |
| • <40 | 4 (13.3) |
| Surgery type | |
| • Conventional | 22 (73.3) |
| • Minimally invasive | 8 (26.7) |
| Intraoperative fluid intake | |
| • Crystalloid (mL) | 2943.8 ± 1342.1 |
| • Colloid (mL) | 0.0 (0.0, 500.0) |
| Transfusion (mL) * | 773.0 (248.0, 1386.0) |
| • PRBC (unit) | 1 (0, 3) |
| • FFP (unit) | 0 (0, 0) |
| • Salvaged blood (mL) | 304.5 (100.0, 1032.0) |
| Vasopressor infusion | 28 (93.3) |
| Inotrope infusion | 21 (70.0) |
| Recorded time (h) | 5.7 ± 1.4 |
| COcont (L/min) | 3.8 (3.2, 4.7) |
| CO-FloTrac (L/min) | 4.8 (3.8, 6.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, C.; Lee, S.; Oh, P.; Chung, W.; Ko, Y.; Yoon, S.-H.; Kim, Y.-H.; Ji, S.-M.; Hong, B. Comparison between Fourth-Generation FloTrac/Vigileo System and Continuous Thermodilution Technique for Cardiac Output Estimation after Time Adjustment during Off-Pump Coronary Artery Bypass Graft Surgery: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 6093. https://doi.org/10.3390/jcm11206093
Oh C, Lee S, Oh P, Chung W, Ko Y, Yoon S-H, Kim Y-H, Ji S-M, Hong B. Comparison between Fourth-Generation FloTrac/Vigileo System and Continuous Thermodilution Technique for Cardiac Output Estimation after Time Adjustment during Off-Pump Coronary Artery Bypass Graft Surgery: A Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(20):6093. https://doi.org/10.3390/jcm11206093
Chicago/Turabian StyleOh, Chahyun, Soomin Lee, Pyeonghwa Oh, Woosuk Chung, Youngkwon Ko, Seok-Hwa Yoon, Yoon-Hee Kim, Sung-Mi Ji, and Boohwi Hong. 2022. "Comparison between Fourth-Generation FloTrac/Vigileo System and Continuous Thermodilution Technique for Cardiac Output Estimation after Time Adjustment during Off-Pump Coronary Artery Bypass Graft Surgery: A Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 20: 6093. https://doi.org/10.3390/jcm11206093