

Systematic Review and Meta-Analysis of Statin Use and Mortality, Intensive Care Unit Admission and Requirement for Mechanical Ventilation in COVID-19 Patients

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
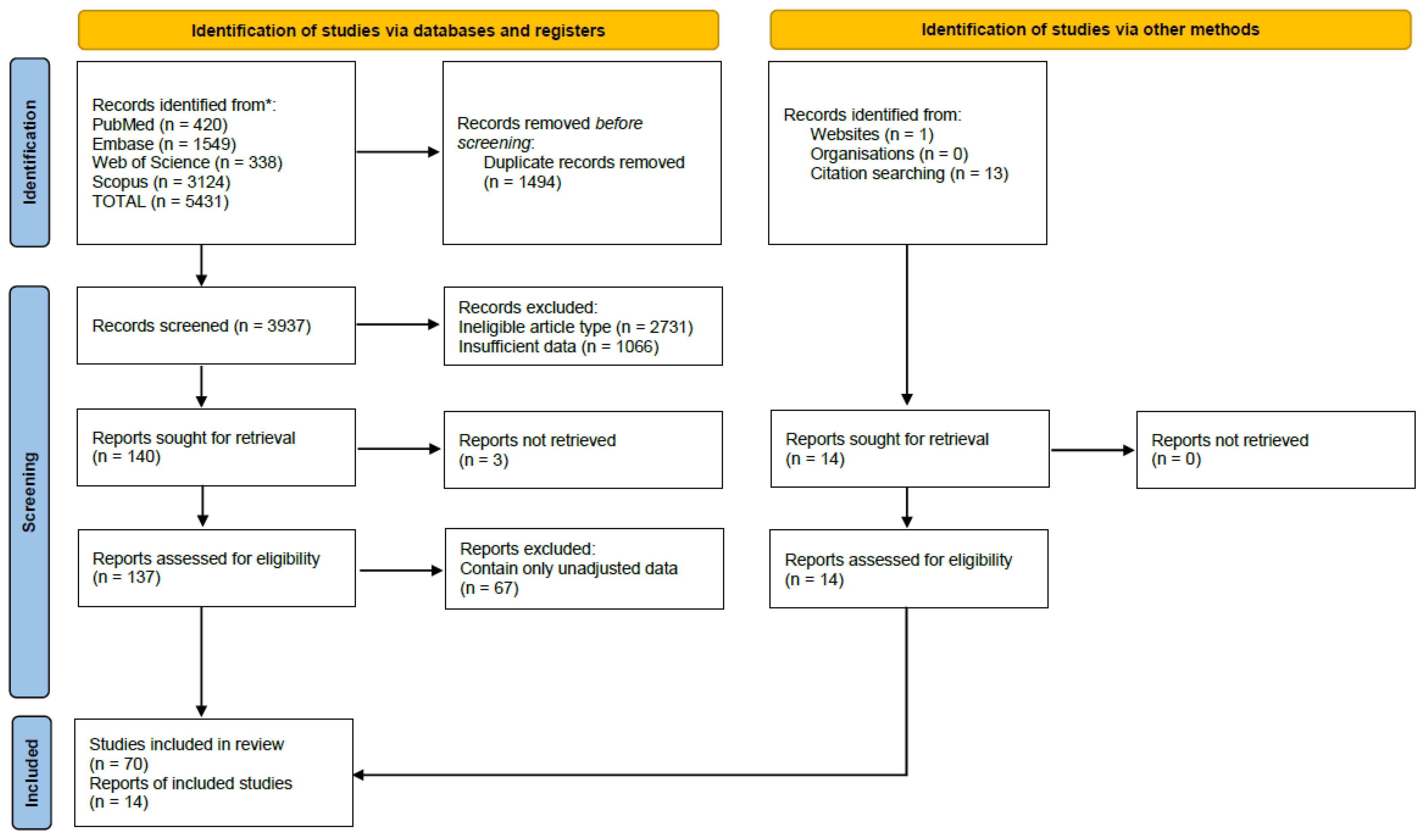
3.1. Literature Search and Study Characteristics
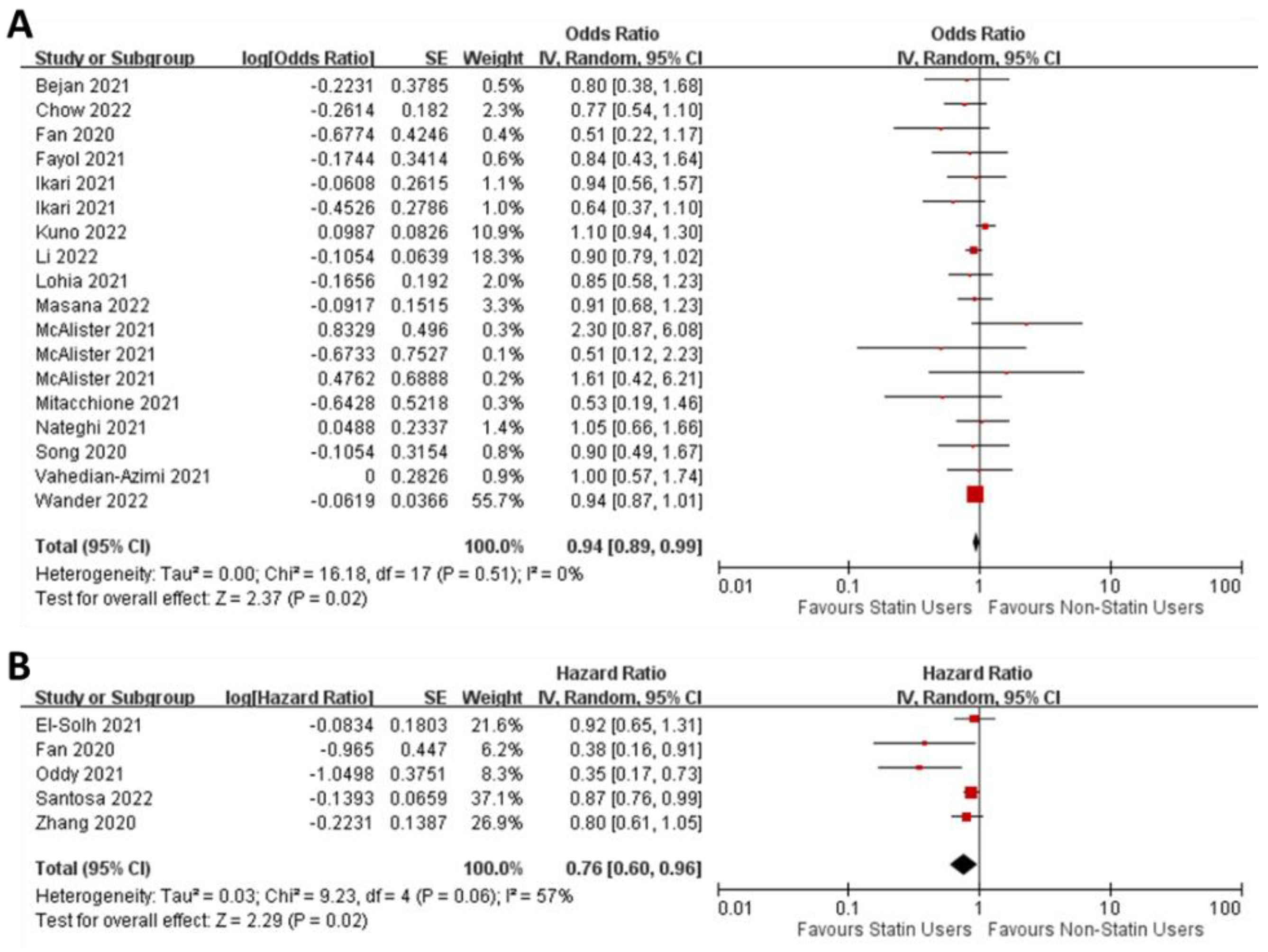
3.2. Effect of Statins on Mortality
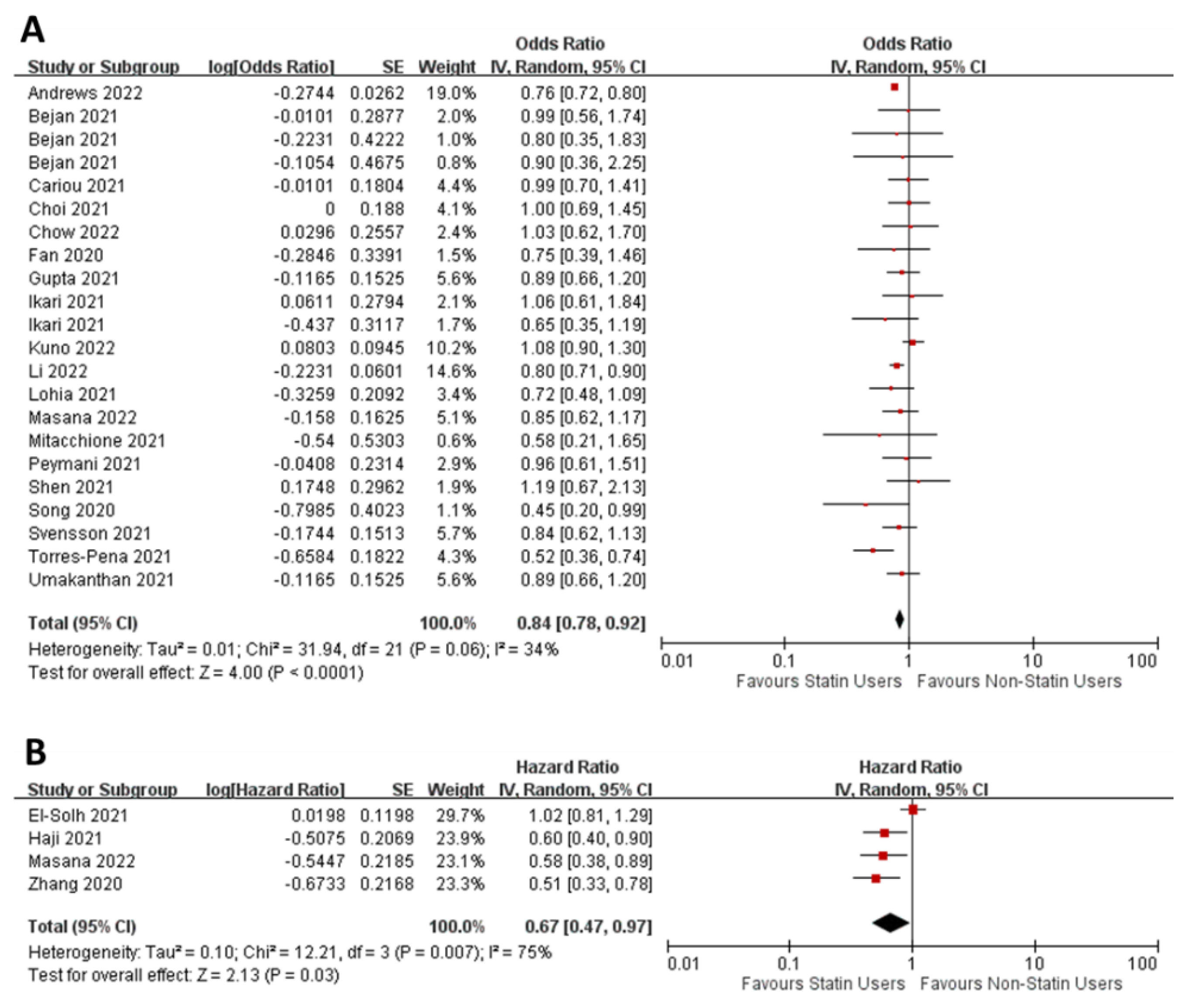
3.3. Effect of Statins on ICU Admission
3.4. Effect of Statins on Requirement of Mechanical Ventilaion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.B.; June, C.H. Cytokine release syndrome in severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab. Res. Rev. 2020, 36, e3319. [Google Scholar] [CrossRef] [PubMed]
- Dehnavi, S.; Sohrabi, N.; Sadeghi, M.; Lansberg, P.; Banach, M.; Al-Rasadi, K.; Johnston, T.P.; Sahebkar, A. Statins and autoimmunity: State-of-the-art. Pharmacol. Ther. 2020, 214, 107614. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M., Jr.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef]
- Ridker, P.M.; Rifai, N.; Clearfield, M.; Downs, J.R.; Weis, S.E.; Miles, J.S.; Gotto, A.M., Jr.; Air Force/Texas Coronary Atherosclerosis Prevention Study, I. Measurement of C-reactive protein for the targeting of statin therapy in the primary prevention of acute coronary events. N. Engl. J. Med. 2001, 344, 1959–1965. [Google Scholar] [CrossRef]
- Chow, R.; Im, J.; Chiu, N.; Chiu, L.; Aggarwal, R.; Lee, J.; Choi, Y.G.; Prsic, E.H.; Shin, H.J. The protective association between statins use and adverse outcomes among COVID-19 patients: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0253576. [Google Scholar] [CrossRef]
- Diaz-Arocutipa, C.; Melgar-Talavera, B.; Alvarado-Yarasca, A.; Saravia-Bartra, M.M.; Cazorla, P.; Belzusarri, I.; Hernandez, A.V. Statins reduce mortality in patients with COVID-19: An updated meta-analysis of 147 824 patients. Int. J. Infect. Dis. 2021, 110, 374–381. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Statin and outcomes of coronavirus disease 2019 (COVID-19): A systematic review, meta-analysis, and meta-regression. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1662–1670. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Statin therapy did not improve the in-hospital outcome of coronavirus disease 2019 (COVID-19) infection. Diabetes Metab. Syndr. 2020, 14, 1613–1615. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Kyriakoulis, I.G.; Nitsotolis, T.; Poulakou, G.; Stergiou, G.S.; Syrigos, K. Statin use and mortality in COVID-19 patients: Updated systematic review and meta-analysis. Atherosclerosis 2021, 330, 114–121. [Google Scholar] [CrossRef]
- Kow, C.S.; Hasan, S.S. Meta-analysis of Effect of Statins in Patients with COVID-19. Am. J. Cardiol. 2020, 134, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Kow, C.S.; Hasan, S.S. The Association Between the Use of Statins and Clinical Outcomes in Patients with COVID-19: A Systematic Review and Meta-analysis. Am. J. Cardiovasc. Drugs 2021, 22, 167–181. [Google Scholar] [CrossRef]
- Permana, H.; Huang, I.; Purwiga, A.; Kusumawardhani, N.Y.; Sihite, T.A.; Martanto, E.; Wisaksana, R.; Soetedjo, N.N.M. In-hospital use of statins is associated with a reduced risk of mortality in coronavirus-2019 (COVID-19): Systematic review and meta-analysis. Pharmacol. Rep. 2021, 73, 769–780. [Google Scholar] [CrossRef]
- Scheen, A.J. Statins and clinical outcomes with COVID-19: Meta-analyses of observational studies. Diabetes Metab. 2021, 47, 101220. [Google Scholar] [CrossRef]
- Vahedian-Azimi, A.; Mohammadi, S.M.; Banach, M.; Beni, F.H.; Guest, P.C.; Al-Rasadi, K.; Jamialahmadi, T.; Sahebkar, A. Improved COVID-19 Outcomes following Statin Therapy: An Updated Systematic Review and Meta-analysis. Biomed. Res. Int. 2021, 2021, 1901772. [Google Scholar] [CrossRef]
- Wu, C.C.; Lee, A.J.; Su, C.H.; Huang, C.Y.; Islam, M.M.; Weng, Y.C. Statin Use Is Associated with a Decreased Risk of Mortality among Patients with COVID-19. J. Clin. Med. 2021, 10, 1450. [Google Scholar] [CrossRef]
- Wu, K.S.; Lin, P.C.; Chen, Y.S.; Pan, T.C.; Tang, P.L. The use of statins was associated with reduced COVID-19 mortality: A systematic review and meta-analysis. Ann. Med. 2021, 53, 874–884. [Google Scholar] [CrossRef]
- Yetmar, Z.A.; Chesdachai, S.; Kashour, T.; Riaz, M.; Gerberi, D.J.; Badley, A.D.; Berbari, E.F.; Tleyjeh, I.M. Prior Statin Use and Risk of Mortality and Severe Disease From Coronavirus Disease 2019: A Systematic Review and Meta-analysis. Open Forum Infect. Dis. 2021, 8, ofab284. [Google Scholar] [CrossRef] [PubMed]
- Zein, A.; Sulistiyana, C.S.; Khasanah, U.; Wibowo, A.; Lim, M.A.; Pranata, R. Statin and mortality in COVID-19: A systematic review and meta-analysis of pooled adjusted effect estimates from propensity-matched cohorts. Postgrad. Med. J. 2022, 98, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Banerjee, M.; Yadav, U.; Bhattacharjee, S. Statin use and clinical outcomes in patients with COVID-19: An updated systematic review and meta-analysis. Postgrad. Med. J. 2022, 98, 354–359. [Google Scholar] [CrossRef]
- Vahedian-Azimi, A.; Mohammadi, S.M.; Heidari Beni, F.; Banach, M.; Guest, P.C.; Jamialahmadi, T.; Sahebkar, A. Improved COVID-19 ICU admission and mortality outcomes following treatment with statins: A systematic review and meta-analysis. Arch. Med. Sci. 2021, 17, 579–595. [Google Scholar] [CrossRef]
- Vahedian-Azimi, A.; Rahimibashar, F.; Najafi, A.; Kidde, J.; Shahriary, A.; Shojaei, S.; Pourhoseingholi, M.A.; Jamialahmadi, T.; Sahebkar, A. Association of In-hospital Use of Statins, Aspirin, and Renin-Angiotensin-Aldosterone Inhibitors with Mortality and ICU Admission Due to COVID-19. In Identification of Biomarkers, New Treatments, and Vaccines for COVID-19; Guest, P.C., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 205–214. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- EPOC. EPOC Resources for Review Authors. Available online: https://epoc.cochrane.org/epoc-resources-review-authors (accessed on 3 August 2022).
- The Cochrane Collaboration. Review Manager (RevMan); Version 5.4; Cochrane: London, UK, 2020. [Google Scholar]
- Ageno, W.; De Candia, E.; Iacoviello, L.; Di Castelnuovo, A. Protective effect of oral anticoagulant drugs in atrial fibrillation patients admitted for COVID-19: Results from the CORIST study. Thromb. Res. 2021, 203, 138–141. [Google Scholar] [CrossRef]
- Al Sulaiman, K.; Aljuhani, O.; Korayem, G.; Altebainawi, A.; Al Harbi, S.; Shaya, A.; Badreldin, H.; Kensara, R.; Harthi, A.; Alghamdi, J.; et al. Statins’ safety and impact on the clinical outcomes in COVID-19 critically ill patients: A Multicenter, Cohort Study. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Andrews, L.; Goldin, L.; Shen, Y.; Korwek, K.; Kleja, K.; Poland, R.E.; Guy, J.; Sands, K.E.; Perlin, J.B. Discontinuation of atorvastatin use in hospital is associated with increased risk of mortality in COVID-19 patients. J. Hosp. Med. 2022, 17, 169–175. [Google Scholar] [CrossRef]
- Aparisi, A.; Amat-Santos, I.J.; Lopez Otero, D.; Marcos-Mangas, M.; Gonzalez-Juanatey, J.R.; San Roman, J.A. Impact of statins in patients with COVID-19. Rev. Esp. Cardiol. 2021, 74, 637–640. [Google Scholar] [CrossRef]
- Basu, A.; Agwu, J.C.; Barlow, N.; Lee, B. Hypertension is the major predictor of poor outcomes among inpatients with COVID-19 infection in the UK: A retrospective cohort study. BMJ Open 2021, 11, e047561. [Google Scholar] [CrossRef]
- Bejan, C.A.; Cahill, K.N.; Staso, P.J.; Choi, L.; Peterson, J.F.; Phillips, E.J. DrugWAS: Drug-wide Association Studies for COVID-19 Drug Repurposing. Clin. Pharmacol. Ther. 2021, 110, 1537–1546. [Google Scholar] [CrossRef] [PubMed]
- Bifulco, M.; Ciccarelli, M.; Bruzzese, D.; Dipasquale, A.; Lania, A.G.; Mazziotti, G.; Gazzerro, P. The benefit of statins in SARS-CoV-2 patients: Further metabolic and prospective clinical studies are needed. Endocrine 2021, 71, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Bui, A.N.; Tyan, K.; Giobbie-Hurder, A.; Klein, I.A.; Manos, M.P.; Zubiri, L.; Reynolds, K.; Grover, S.; Weinhouse, G.L.; Ott, P.A.; et al. Impact of COVID-19 on Patients with Cancer Receiving Immune Checkpoint Inhibitors. J. Immunother. Precis. Oncol. 2021, 4, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Byttebier, G.; Belmans, L.; Alexander, M.; Saxberg, B.E.H.; De Spiegeleer, B.; De Spiegeleer, A.; Devreker, N.; Van Praet, J.T.; Vanhove, K.; Reybrouck, R.; et al. Hospital mortality in COVID-19 patients in Belgium treated with statins, ACE inhibitors and/or ARBs. Hum. Vaccin. Immunother. 2021, 17, 2841–2850. [Google Scholar] [CrossRef] [PubMed]
- Cabezon Villalba, G.; Amat-Santos, I.J.; Duenas, C.; Lopez Otero, D.; Catala, P.; Aparisi, A.; Lopez-Pais, J.; Cacho Antonio, C.E.; Candela, J.; Antunez Muinos, P.; et al. Impact of the presence of heart disease, cardiovascular medications and cardiac events on outcome in COVID-19. Cardiol. J. 2021, 28, 360–368. [Google Scholar] [CrossRef]
- Chacko, S.R.; DeJoy, R.; Lo, K.B.; Albano, J.; Peterson, E.; Bhargav, R.; Gu, F.; Salacup, G.; Pelayo, J.; Azmaiparashvili, Z.; et al. Association of Pre-Admission Statin Use With Reduced In-Hospital Mortality in COVID-19. Am. J. Med. Sci. 2021, 361, 725–730. [Google Scholar] [CrossRef]
- Cho, D.-H.; Choi, J.; Gwon, J.G. Atorvastatin Reduces the Severity of COVID-19: A Nationwide, Total Population-Based, Case-Control Study. COVID 2022, 2, 398–406. [Google Scholar] [CrossRef]
- Choi, D.; Chen, Q.; Goonewardena, S.N.; Pacheco, H.; Mejia, P.; Smith, R.L.; Rosenson, R.S. Efficacy of Statin Therapy in Patients with Hospital Admission for COVID-19. Cardiovasc. Drugs Ther. 2021. [Google Scholar] [CrossRef]
- Chow, R.; Lee, J.; Noh, H.; Lee, J.; Simone II, C.B.; Shin, H.J.; Choi, Y.-G. The association between statin and COVID-19 adverse outcomes: National COVID-19 cohort in South Korea. Ann. Palliat. Med. 2022, 11, 1297–1307. [Google Scholar] [CrossRef]
- Daniels, L.B.; Ren, J.; Kumar, K.; Bui, Q.M.; Zhang, J.; Zhang, X.; Sawan, M.A.; Eisen, H.; Longhurst, C.A.; Messer, K. Relation of prior statin and anti-hypertensive use to severity of disease among patients hospitalized with COVID-19: Findings from the American Heart Association’s COVID-19 Cardiovascular Disease Registry. PLoS ONE 2021, 16, e0254635. [Google Scholar] [CrossRef]
- De Spiegeleer, A.; Van Migerode, J.; Bronselaer, A.; Wynendaele, E.; Peelman, M.; Vandaele, F.; Byttebier, G.; De Tre, G.; Belmans, L.; Van De Wiele, C.; et al. Statin Intake and All-Cause Mortality among Older Nursing Home Residents. Gerontology 2022, 68, 407–411. [Google Scholar] [CrossRef] [PubMed]
- El-Solh, A.A.; Lawson, Y.; El-Solh, D.A. All-cause mortality in COVID-19 patients receiving statin therapy: Analysis of veterans affairs database cohort study. Intern. Emerg. Med. 2021, 17, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Espana, P.P.; Bilbao, A.; Garcia-Gutierrez, S.; Lafuente, I.; Anton-Ladislao, A.; Villanueva, A.; Uranga, A.; Legarreta, M.J.; Aguirre, U.; Quintana, J.M.; et al. Predictors of mortality of COVID-19 in the general population and nursing homes. Intern. Emerg. Med. 2021, 16, 1487–1496. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Guo, T.; Yan, F.; Gong, M.; Zhang, X.A.; Li, C.; He, T.; Luo, H.; Zhang, L.; Chen, M.; et al. Association of Statin Use With the In-Hospital Outcomes of 2019-Coronavirus Disease Patients: A Retrospective Study. Front. Med. 2020, 7, 584870. [Google Scholar] [CrossRef]
- Greco, S.; D’Amuri, A.; Giorgini, E.; Luciani, F.; Lopreiato, M.; Fortunato, V.; Scopa, A.; Vestita, G.; Capatti, E.; Passaro, A. Role of Statins in Coronavirus-Related Disease (COVID-19): A Retrospective Cohort Study in Northern Italy. High. Blood Press Cardiovasc. Prev. 2021, 28, 355–364. [Google Scholar] [CrossRef]
- Gupta, A.; Madhavan, M.V.; Poterucha, T.J.; DeFilippis, E.M.; Hennessey, J.A.; Redfors, B.; Eckhardt, C.; Bikdeli, B.; Platt, J.; Nalbandian, A.; et al. Association between antecedent statin use and decreased mortality in hospitalized patients with COVID-19. Nat. Commun. 2021, 12, 1325. [Google Scholar] [CrossRef]
- Ikari, Y.; Matsue, Y.; Torii, S.; Hasegawa, M.; Aihara, K.; Kuroda, S.; Sano, T.; Kitai, T.; Yonetsu, T.; Kohsaka, S.; et al. Association Between Statin Use Prior to Admission and Lower Coronavirus Disease 2019 (COVID-19) Severity in Patients With Cardiovascular Disease or Risk Factors. Circ. J. 2021, 85, 939–943. [Google Scholar] [CrossRef]
- Kabootari, M.; Habibi Tirtashi, R.; Hasheminia, M.; Bozorgmanesh, M.; Khalili, D.; Akbari, H.; Roshandel, G.; Hadaegh, F. Clinical features, risk factors and a prediction model for in-hospital mortality among diabetic patients infected with COVID-19: Data from a referral centre in Iran. Public Heal. 2022, 202, 84–92. [Google Scholar] [CrossRef]
- Kuno, T.; So, M.; Iwagami, M.; Takahashi, M.; Egorova, N.N. The association of statins use with survival of patients with COVID-19. J. Cardiol. 2022, 79, 494–500. [Google Scholar] [CrossRef]
- Lee, H.Y.; Ahn, J.; Park, J.; Kyung Kang, C.; Won, S.H.; Wook Kim, D.; Park, J.H.; Chung, K.H.; Joh, J.S.; Bang, J.H.; et al. Beneficial Effect of Statins in COVID-19-Related Outcomes-Brief Report: A National Population-Based Cohort Study. Arterioscler. Thromb. Vasc. Biol. 2021, 41, e175–e182. [Google Scholar] [CrossRef]
- Li, W.; Rios, S.; Nagraj, S.; Hajra, A.; Saralidze, T.; Varrias, D.; Mathai, S.V.; Novakovic, M.; Hupart, K.H.; Miles, J.A.; et al. Statin Use in Hospitalized Patients with COVID-19: A Comprehensive Analysis of the New York City Public Hospital System. Am. J. Med. 2022, 135, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Lohia, P.; Kapur, S.; Benjaram, S.; Mir, T. Association between antecedent statin use and severe disease outcomes in COVID-19: A retrospective study with propensity score matching. J. Clin. Lipidol. 2021, 15, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Luo, P.; Qiu, L.; Liu, Y.; Liu, X.L.; Zheng, J.L.; Xue, H.Y.; Liu, W.H.; Liu, D.; Li, J. Metformin Treatment Was Associated with Decreased Mortality in COVID-19 Patients with Diabetes in a Retrospective Analysis. Am. J. Trop. Med. Hyg. 2020, 103, 69–72. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, Y.; Li, S.; Yang, H.; Li, H.; Cao, Z.; Xu, F.; Sun, L.; Wang, Y. Sex Differences in Association Between Anti-Hypertensive Medications and Risk of COVID-19 in Middle-Aged and Older Adults. Drugs Aging 2021, 38, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Mallow, P.J.; Belk, K.W.; Topmiller, M.; Hooker, E.A. Outcomes of Hospitalized COVID-19 Patients by Risk Factors: Results from a United States Hospital Claims Database. J. Health Econ. Outcomes Res. 2020, 7, 165–174. [Google Scholar] [CrossRef]
- Maric, I.; Oskotsky, T.; Kosti, I.; Le, B.; Wong, R.J.; Shaw, G.M.; Sirota, M.; Stevenson, D.K. Decreased Mortality Rate among COVID-19 Patients Prescribed Statins: Data from Electronic Health Records in the US. Front. Med. 2021, 8, 639804. [Google Scholar] [CrossRef]
- Masana, L.; Correig, E.; Rodriguez-Borjabad, C.; Anoro, E.; Arroyo, J.A.; Jerico, C.; Pedragosa, A.; Miret, M.; Naf, S.; Pardo, A.; et al. Effect of statin therapy on SARS-CoV-2 infection-related mortality in hospitalized patients. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 157–164. [Google Scholar] [CrossRef]
- McAlister, F.A.; Wang, T.; Wang, X.; Chu, A.; Goodman, S.G.; Diepen, S.V.; Jackevicius, C.A.; Kaul, P.; Udell, J.; Ko, D.T.; et al. Statins and SARS-CoV-2 Infection: Results of a P.Popu.ulation-Based Prospective Cohort Study of 469 749 Adults From 2 Canadian Provinces. J. Am. Hear. Assoc. 2021, 10, e022330. [Google Scholar] [CrossRef]
- Mehra, M.R.; Desai, S.S.; Kuy, S.; Henry, T.D.; Patel, A.N. Retraction: Cardiovascular Disease, Drug Therapy, and Mortality in COVID-19. N. Engl. J. Med. 2020, 382, 2582. [Google Scholar] [CrossRef]
- Meintrup, D.; Borgmann, S.; Seidl, K.; Stecher, M.; Jakob, C.E.M.; Pilgram, L.; Spinner, C.D.; Rieg, S.; Isberner, N.; Hower, M.; et al. Specific Risk Factors for Fatal Outcome in Critically Ill COVID-19 Patients: Results from a European Multicenter Study. J. Clin. Med. 2021, 10, 3855. [Google Scholar] [CrossRef] [PubMed]
- Merzon, E.; Green, I.; Vinker, S.; Golan-Cohen, A.; Gorohovski, A.; Avramovich, E.; Frenkel-Morgenstern, M.; Magen, E. The use of aspirin for primary prevention of cardiovascular disease is associated with a lower likelihood of COVID-19 infection. FEBS J. 2021, 288, 5179–5189. [Google Scholar] [CrossRef]
- Mitacchione, G.; Schiavone, M.; Curnis, A.; Arca, M.; Antinori, S.; Gasperetti, A.; Mascioli, G.; Severino, P.; Sabato, F.; Caracciolo, M.M.; et al. Impact of prior statin use on clinical outcomes in COVID-19 patients: Data from tertiary referral hospitals during COVID-19 pandemic in Italy. J. Clin. Lipidol. 2021, 15, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Monserrat Villatoro, J.; Mejia-Abril, G.; Diaz Garcia, L.; Zubiaur, P.; Jimenez Gonzalez, M.; Fernandez Jimenez, G.; Cancio, I.; Arribas, J.R.; Suarez Fernandez, C.; Mingorance, J.; et al. A Case-Control of Patients with COVID-19 to Explore the Association of Previous Hospitalisation Use of Medication on the Mortality of COVID-19 Disease: A Propensity Score Matching Analysis. Pharmaceuticals 2022, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Nateghi, S.; Gomari, M.M.; Hosamirudsari, H.; Behnoush, B.; Razmjoofard, A.; Azimi, G.; Ordookhani, S.; Jafarpour, A.; Faraji, N. A historical cohort study to investigation of statins safety in COVID-19 hospitalized patients. Therapie 2021, 77, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, C.J.; Wooster, L.; Sigurslid, H.H.; Li, R.H.; Jiang, W.; Tian, W.; Lino Cardenas, C.L.; Malhotra, R. Estimating risk of mechanical ventilation and in-hospital mortality among adult COVID-19 patients admitted to Mass General Brigham: The VICE and DICE scores. EClinicalMedicine 2021, 33, 100765. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.A.; Jeon, Y.T. Statin Therapy and the Risk of COVID-19: A Cohort Study of the National Health Insurance Service in South Korea. J. Pers. Med. 2021, 11, 116. [Google Scholar] [CrossRef]
- Pazoki, M.; Chichagi, F.; Hadadi, A.; Kafan, S.; Montazeri, M.; Kazemian, S.; Aminorroaya, A.; Ebrahimi, M.; Ashraf, H.; Hazaveh, M.M.; et al. Association of clinical characteristics, antidiabetic and cardiovascular agents with diabetes mellitus and COVID-19: A 7-month follow-up cohort study. J. Diabetes Metab. Disord. 2021, 20, 1545–1555. [Google Scholar] [CrossRef]
- Philipose, Z.; Smati, N.; Wong, C.S.J.; Aspey, K.; Mendall, M. Obesity, old age and frailty are the true risk factors for COVID-19 mortality and not chronic disease or ethnicity in Croydon. medRxiv 2020. [Google Scholar] [CrossRef]
- Ramachandran, P.; Perisetti, A.; Gajendran, M.; Jean-Louis, F.; Bansal, P.; Dwivedi, A.K.; Goyal, H. Pre-hospitalization proton pump inhibitor use and clinical outcomes in COVID-19. Eur. J. Gastroenterol. Hepatol. 2022, 34, 137–141. [Google Scholar] [CrossRef]
- Ramos-Rincon, J.M.; Perez-Belmonte, L.M.; Carrasco-Sanchez, F.J.; Jansen-Chaparro, S.; De-Sousa-Baena, M.; Bueno-Fonseca, J.; Perez-Aguilar, M.; Arevalo-Canas, C.; Bacete Cebrian, M.; Mendez-Bailon, M.; et al. Cardiometabolic Therapy and Mortality in Very Old Patients With Diabetes Hospitalized due to COVID-19. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, e102–e109. [Google Scholar] [CrossRef]
- Rosenthal, N.; Cao, Z.; Gundrum, J.; Sianis, J.; Safo, S. Risk Factors Associated With In-Hospital Mortality in a US National Sample of Patients With COVID-19. JAMA Netw. Open 2020, 3, e2029058. [Google Scholar] [CrossRef] [PubMed]
- Soldevila, L.; Valerio-Sallent, L.; Roure, S.; Perez-Quilez, O.; Mas, M.A.; Miralles, R.; Lopez-Munoz, I.; Estrada, O.; Valles, X. Drug exposure may have a substantial influence on COVID-19 prognosis among residents of long-term care facilities: An exploratory analysis. Int. J. Infect. Dis. 2021, 109, 192–194. [Google Scholar] [CrossRef]
- Song, S.L.; Hays, S.B.; Panton, C.E.; Mylona, E.K.; Kalligeros, M.; Shehadeh, F.; Mylonakis, E. Statin Use Is Associated with Decreased Risk of Invasive Mechanical Ventilation in COVID-19 Patients: A Preliminary Study. Pathogens 2020, 9, 759. [Google Scholar] [CrossRef] [PubMed]
- Terlecki, M.; Wojciechowska, W.; Klocek, M.; Olszanecka, A.; Stolarz-Skrzypek, K.; Grodzicki, T.; Malecki, M.; Katra, B.; Garlicki, A.; Bociaga-Jasik, M.; et al. Association between cardiovascular disease, cardiovascular drug therapy, and in-hospital outcomes in patients with COVID-19: Data from a large single-center registry in Poland. Kardiol. Pol. 2021, 79, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Tignanelli, C.J.; Bramante, C.T.; Dutta, N.; Tamariz, L.; Usher, M.G.; Ikramuddin, S. Metabolic surgery may protect against admission for COVID-19 in persons with nonalcoholic fatty liver disease. Surg. Obes. Relat. Dis. 2021, 17, 1780–1786. [Google Scholar] [CrossRef]
- Torres-Pena, J.D.; Perez-Belmonte, L.M.; Fuentes-Jimenez, F.; Lopez Carmona, M.D.; Perez-Martinez, P.; Lopez-Miranda, J.; Carrasco Sanchez, F.J.; Vargas Nunez, J.A.; Del Corral Beamonte, E.; Magallanes Gamboa, J.O.; et al. Prior Treatment with Statins is Associated with Improved Outcomes of Patients with COVID-19: Data from the SEMI-COVID-19 Registry. Drugs 2021, 81, 685–695. [Google Scholar] [CrossRef]
- Umakanthan, S.; Senthil, S.; John, S.; Madhavan, M.K.; Das, J.; Patil, S.; Rameshwaram, R.; Cintham, A.; Subramaniam, V.; Yogi, M.; et al. The protective role of statins in COVID-19 patients: A retrospective observational study. Transl. Med. Commun. 2021, 6, 22. [Google Scholar] [CrossRef]
- Wander, P.L.; Lowy, E.; Beste, L.A.; Tulloch-Palomino, L.; Korpak, A.; Peterson, A.C.; Kahn, S.E.; Danaei, G.; Boyko, E.J. Associations of statin use with 30-day adverse outcomes among 4 801 406 US Veterans with and without SARS-CoV-2: An observational cohort study. BMJ Open 2022, 12, e058363. [Google Scholar] [CrossRef]
- Wargny, M.; Potier, L.; Gourdy, P.; Pichelin, M.; Amadou, C.; Benhamou, P.Y.; Bonnet, J.B.; Bordier, L.; Bourron, O.; Chaumeil, C.; et al. Predictors of hospital discharge and mortality in patients with diabetes and COVID-19: Updated results from the nationwide CORONADO study. Diabetologia 2021, 64, 778–794. [Google Scholar] [CrossRef]
- Yetmar, Z.A.; Challener, D.W.; Tleyjeh, I.M.; Sohail, M.R.; Cerhan, J.R.; Badley, A.D.; O’Horo, J.C. Association Between Chronic Statin Use and 30-Day Mortality in Hospitalized Patients With COVID-19. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 442–446. [Google Scholar] [CrossRef]
- Zhang, X.J.; Qin, J.J.; Cheng, X.; Shen, L.; Zhao, Y.C.; Yuan, Y.; Lei, F.; Chen, M.M.; Yang, H.; Bai, L.; et al. In-Hospital Use of Statins Is Associated with a Reduced Risk of Mortality among Individuals with COVID-19. Cell Metab. 2020, 32, 176–187.e174. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Zhao, L.; Wu, G.; Hu, C.; Wu, C.; Xu, M.; Dong, H.; Zhang, Q.; Wang, G.; Yu, B.; et al. Impact of renin-angiotensin system inhibitors use on mortality in severe COVID-19 patients with hypertension: A retrospective observational study. J. Int. Med. Res. 2020, 48, 300060520979151. [Google Scholar] [CrossRef] [PubMed]
- An, C.; Lim, H.; Kim, D.W.; Chang, J.H.; Choi, Y.J.; Kim, S.W. Machine learning prediction for mortality of patients diagnosed with COVID-19: A nationwide Korean cohort study. Sci. Rep. 2020, 10, 18716. [Google Scholar] [CrossRef] [PubMed]
- Ayeh, S.K.; Abbey, E.J.; Khalifa, B.A.A.; Nudotor, R.D.; Osei, A.D.; Chidambaram, V.; Osuji, N.; Khan, S.; Salia, E.L.; Oduwole, M.O.; et al. Statins use and COVID-19 outcomes in hospitalized patients. PLoS ONE 2021, 16, e0256899. [Google Scholar] [CrossRef] [PubMed]
- Bergqvist, R.; Ahlqvist, V.H.; Lundberg, M.; Hergens, M.P.; Sundstrom, J.; Bell, M.; Magnusson, C. HMG-CoA reductase inhibitors and COVID-19 mortality in Stockholm, Sweden: A registry-based cohort study. PLoS Med. 2021, 18, e1003820. [Google Scholar] [CrossRef]
- Buenen, A.G.; Sinkeldam, M.; Maas, M.L.; Verdonschot, M.; Wever, P.C. Prior use of anticoagulation is associated with a better survival in COVID-19. J. Thromb. Thrombolysis 2021, 52, 1207–1211. [Google Scholar] [CrossRef]
- Butt, J.H.; Gerds, T.A.; Schou, M.; Kragholm, K.; Phe.elps, M.; Havers-Borgersen, E.; Yafasova, A.; Gislason, G.H.; Torp-Pedersen, C.; Kober, L.; et al. Association between statin use and outcomes in patients with coronavirus disease 2019 (COVID-19): A nationwide cohort study. BMJ Open 2020, 10, e044421. [Google Scholar] [CrossRef]
- Castagna, F.; Xue, X.; Saeed, O.; Kataria, R.; Puius, Y.A.; Patel, S.R.; Garcia, M.J.; Racine, A.D.; Sims, D.B.; Jorde, U.P. Hospital bed occupancy rate is an independent risk factor for COVID-19 inpatient mortality: A pandemic epicentre cohort study. BMJ Open 2022, 12, e058171. [Google Scholar] [CrossRef]
- Fung, K.W.; Baik, S.H.; Baye, F.; Zheng, Z.; Huser, V.; McDonald, C.J. Effect of common maintenance drugs on the risk and severity of COVID-19 in elderly patients. PLoS ONE 2022, 17, e0266922. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Haji Aghajani, M.; Moradi, O.; Azhdari Tehrani, H.; Amini, H.; Pourheidar, E.; Hatami, F.; Rabiei, M.M.; Sistanizad, M. Promising effects of atorvastatin on mortality and need for mechanical ventilation in patients with severe COVID-19; a retrospective cohort study. Int. J. Clin. Pract. 2021, 75, e14434. [Google Scholar] [CrossRef] [PubMed]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Kouhpeikar, H.; Khosaravizade Tabasi, H.; Khazir, Z.; Naghipour, A.; Mohammadi Moghadam, H.; Forouzanfar, H.; Abbasifard, M.; Kirichenko, T.V.; Reiner, Z.; Banach, M.; et al. Statin Use in COVID-19 Hospitalized Patients and Outcomes: A Retrospective Study. Front. Cardiovasc. Med. 2022, 9, 820260. [Google Scholar] [CrossRef] [PubMed]
- Lala, A.; Johnson, K.W.; Januzzi, J.L.; Russak, A.J.; Paranjpe, I.; Richter, F.; Zhao, S.; Somani, S.; Van Vleck, T.; Vaid, A.; et al. Prevalence and Impact of Myocardial Injury in Patients Hospitalized With COVID-19 Infection. J. Am. Coll. Cardiol. 2020, 76, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Memel, Z.N.; Lee, J.J.; Foulkes, A.S.; Chung, R.T.; Thaweethai, T.; Bloom, P.P. Association of Statins and 28-Day Mortality Rates in Patients Hospitalized With Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Infect. Dis. 2022, 225, 19–29. [Google Scholar] [CrossRef]
- Oddy, C.; McCaul, J.; Keeling, P.; Allington, J.; Senn, D.; Soni, N.; Morrison, H.; Mawella, R.; Samuel, T.; Dixon, J. Pharmacological Predictors of Morbidity and Mortality in COVID-19. J. Clin. Pharmacol. 2021, 61, 1286–1300. [Google Scholar] [CrossRef]
- Peymani, P.; Dehesh, T.; Aligolighasemabadi, F.; Sadeghdoust, M.; Kotfis, K.; Ahmadi, M.; Mehrbod, P.; Iranpour, P.; Dastghaib, S.; Nasimian, A.; et al. Statins in patients with COVID-19: A retrospective cohort study in Iranian COVID-19 patients. Transl. Med. Commun. 2021, 6, 3. [Google Scholar] [CrossRef]
- Rey, J.R.; Merino Llorens, J.L.; Iniesta Manjavacas, A.M.; Rodriguez, S.O.R.; Castrejon-Castrejon, S.; Arbas-Redondo, E.; Poveda-Pinedo, I.D.; Tebar-Marquez, D.; Severo-Sanchez, A.; Rivero-Santana, B.; et al. Influence of statin treatment in a cohort of patients admitted for COVID-19. Med. Clin. 2022, 158, 586–595. [Google Scholar] [CrossRef]
- Saeed, O.; Castagna, F.; Agalliu, I.; Xue, X.; Patel, S.R.; Rochlani, Y.; Kataria, R.; Vukelic, S.; Sims, D.B.; Alvarez, C.; et al. Statin Use and In-Hospital Mortality in Patients With Diabetes Mellitus and COVID-19. J. Am. Heart Assoc. 2020, 9, e018475. [Google Scholar] [CrossRef]
- Santosa, A.; Franzen, S.; Natman, J.; Wettermark, B.; Parmryd, I.; Nyberg, F. Protective effects of statins on COVID-19 risk, severity and fatal outcome: A nationwide Swedish cohort study. Sci. Rep. 2022, 12, 12047. [Google Scholar] [CrossRef]
- Shen, L.; Qiu, L.; Wang, L.; Huang, H.; Liu, D.; Xiao, Y.; Liu, Y.; Jin, J.; Liu, X.; Wang, D.W.; et al. Statin Use and In-hospital Mortality in Patients with COVID-19 and Coronary Heart Disease. Sci. Rep. 2021, 11, 23874. [Google Scholar] [CrossRef] [PubMed]
- Vila-Corcoles, A.; Satue-Gracia, E.; Vila-Rovira, A.; de Diego-Cabanes, C.; Forcadell-Peris, M.J.; Hospital-Guardiola, I.; Ochoa-Gondar, O.; Basora-Gallisa, J. COVID19-related and all-cause mortality risk among middle-aged and older adults across the first epidemic wave of SARS-CoV-2 infection: A population-based cohort stuJune 2020.dy in Southern Catalonia, Spain, March. BMC Public Health 2021, 21, 1795. [Google Scholar] [CrossRef] [PubMed]
- Volff, M.; Tonon, D.; Bommel, Y.; Peres, N.; Lagier, D.; Agard, G.; Jacquier, A.; Bartoli, A.; Carvelli, J.; Max, H.; et al. Factors Associated with 90-Day Mortality in Invasively Ventilated Patients with COVID-19 in Marseille, France. J. Clin. Med. 2021, 10, 5650. [Google Scholar] [CrossRef]
- Fayol, A.; Livrozet, M.; Pereira, H.; Diehl, J.-L.; Lebeaux, D.; Arlet, J.-B.; Cholley, B.; Carette, C.; Carves, J.-B.; Czernichow, S.; et al. Cardiometabolic Disorders and the Risk of Critical COVID-19 as Compared to Influenza Pneumonia. J. Clin. Med. 2021, 10, 4618. [Google Scholar] [CrossRef]
- Cariou, B.; Goronflot, T.; Rimbert, A.; Boullu, S.; Le May, C.; Moulin, P.; Pichelin, M.; Potier, L.; Smati, S.; Sultan, A.; et al. Routine use of statins and increased COVID-19 related mortality in inpatients with type 2 diabetes: Results from the CORONADO study. Diabetes Metab. 2021, 47, 101202. [Google Scholar] [CrossRef] [PubMed]
- Svensson, P.; Hofmann, R.; Habel, H.; Jernberg, T.; Nordberg, P. Association between cardiometabolic disease and severe COVID-19: A nationwide case-control study of patients requiring invasive mechanical ventilation. BMJ Open 2021, 11, e044486. [Google Scholar] [CrossRef]
- Sasidhar, M.V.; Chevooru, S.K.; Eickelberg, O.; Hartung, H.P.; Neuhaus, O. Downregulation of monocytic differentiation via modulation of CD147 by 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors. PLoS ONE 2017, 12, e0189701. [Google Scholar] [CrossRef]
- Liang, X.; Yang, L.X.; Guo, R.; Shi, Y.; Hou, X.; Yang, Z.; Zhou, X.; Liu, H. Atorvastatin attenuates plaque vulnerability by downregulation of EMMPRIN expression via COX-2/PGE2 pathway. Exp. Ther. Med. 2017, 13, 835–844. [Google Scholar] [CrossRef]
- Wang, K.; Chen, W.; Zhang, Z.; Deng, Y.; Lian, J.Q.; Du, P.; Wei, D.; Zhang, Y.; Sun, X.X.; Gong, L.; et al. CD147-spike protein is a novel route for SARS-CoV-2 infection to host cells. Signal. Transduct. Target. Ther. 2020, 5, 283. [Google Scholar] [CrossRef]
- Albert, M.A.; Danielson, E.; Rifai, N.; Ridker, P.M.; Investigators, P. Effect of statin therapy on C-reactive protein levels: The pravastatin inflammation/CRP evaluation (PRINCE): A randomized trial and cohort study. JAMA 2001, 286, 64–70. [Google Scholar] [CrossRef]
- Parsamanesh, N.; Moossavi, M.; Bahrami, A.; Fereidouni, M.; Barreto, G.; Sahebkar, A. NLRP3 inflammasome as a treatment target in atherosclerosis: A focus on statin therapy. Int. Immunopharmacol. 2019, 73, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Holschermann, H.; Schuster, D.; Parviz, B.; Haberbosch, W.; Tillmanns, H.; Muth, H. Statins prevent NF-kappaB transactivation independently of the IKK-pathway in human endothelial cells. Atherosclerosis 2006, 185, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Ye, B.; Lin, L.; Cai, X.; Huang, W.; Huang, Z. Atorvastatin suppresses NLRP3 inflammasome activation via TLR4/MyD88/NF-kappaB signaling in PMA-stimulated THP-1 monocytes. Biomed. Pharmacother. 2016, 82, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues-Diez, R.R.; Tejera-Munoz, A.; Marquez-Exposito, L.; Rayego-Mateos, S.; Santos Sanchez, L.; Marchant, V.; Tejedor Santamaria, L.; Ramos, A.M.; Ortiz, A.; Egido, J.; et al. Statins: Could an old friend help in the fight against COVID-19? Br. J. Pharmacol. 2020, 177, 4873–4886. [Google Scholar] [CrossRef] [PubMed]
- Onorato, D.; Pucci, M.; Carpene, G.; Henry, B.M.; Sanchis-Gomar, F.; Lippi, G. Protective Effects of Statins Administration in European and North American Patients Infected with COVID-19: A Meta-Analysis. Semin. Thromb. Hemost. 2021, 47, 392–399. [Google Scholar] [CrossRef]
- Beaney, T.; Neves, A.L.; Alboksmaty, A.; Ashrafian, H.; Flott, K.; Fowler, A.; Benger, J.R.; Aylin, P.; Elkin, S.; Darzi, A.; et al. Trends and associated factors for COVID-19 hospitalisation and fatality risk in 2.3 million adults in England. Nat. Commun. 2022, 13, 2356. [Google Scholar] [CrossRef]
- Collard, D.; Nurmohamed, N.S.; Kaiser, Y.; Reeskamp, L.F.; Dormans, T.; Moeniralam, H.; Simsek, S.; Douma, R.; Eerens, A.; Reidinga, A.C.; et al. Cardiovascular risk factors and COVID-19 outcomes in hospitalised patients: A prospective cohort study. BMJ Open 2021, 11, e045482. [Google Scholar] [CrossRef]
- Phadke, M.; Saunik, S. COVID-19 treatment by repurposing drugs until the vaccine is in sight. Drug Dev. Res. 2020, 81, 541–543. [Google Scholar] [CrossRef]
- INSPIRATION-S Investigators. Atorvastatin versus placebo in patients with COVID-19 in intensive care: Randomized controlled trial. BMJ 2022, 376, e068407. [Google Scholar] [CrossRef]
- Gaitan-Duarte, H.G.; Alvarez-Moreno, C.; Rincon-Rodriguez, C.J.; Yomayusa-Gonzalez, N.; Cortes, J.A.; Villar, J.C.; Bravo-Ojeda, J.S.; Garcia-Pena, A.; Adarme-Jaimes, W.; Rodriguez-Romero, V.A.; et al. Effectiveness of rosuvastatin plus colchicine, emtricitabine/tenofovir and combinations thereof in hospitalized patients with COVID-19: A pragmatic, open-label randomized trial. EClinicalMedicine 2022, 43, 101242. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lao, U.-S.; Law, C.-F.; Baptista-Hon, D.T.; Tomlinson, B. Systematic Review and Meta-Analysis of Statin Use and Mortality, Intensive Care Unit Admission and Requirement for Mechanical Ventilation in COVID-19 Patients. J. Clin. Med. 2022, 11, 5454. https://doi.org/10.3390/jcm11185454
Lao U-S, Law C-F, Baptista-Hon DT, Tomlinson B. Systematic Review and Meta-Analysis of Statin Use and Mortality, Intensive Care Unit Admission and Requirement for Mechanical Ventilation in COVID-19 Patients. Journal of Clinical Medicine. 2022; 11(18):5454. https://doi.org/10.3390/jcm11185454
Chicago/Turabian StyleLao, Ut-Sam, Chak-Fun Law, Daniel T. Baptista-Hon, and Brian Tomlinson. 2022. "Systematic Review and Meta-Analysis of Statin Use and Mortality, Intensive Care Unit Admission and Requirement for Mechanical Ventilation in COVID-19 Patients" Journal of Clinical Medicine 11, no. 18: 5454. https://doi.org/10.3390/jcm11185454