
Direct-Acting Antiviral Drugs Reduce Fibromyalgia Symptoms in Patients with Chronic Hepatitis C
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Liver Function Test and Hepatitis C Virus (HCV) Viral Loads
2.3. Serum Levels of Inflammatory Cytokines in CHC Patients
2.4. Evaluation of Concomitant Fibromyalgia in CHC Patients
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
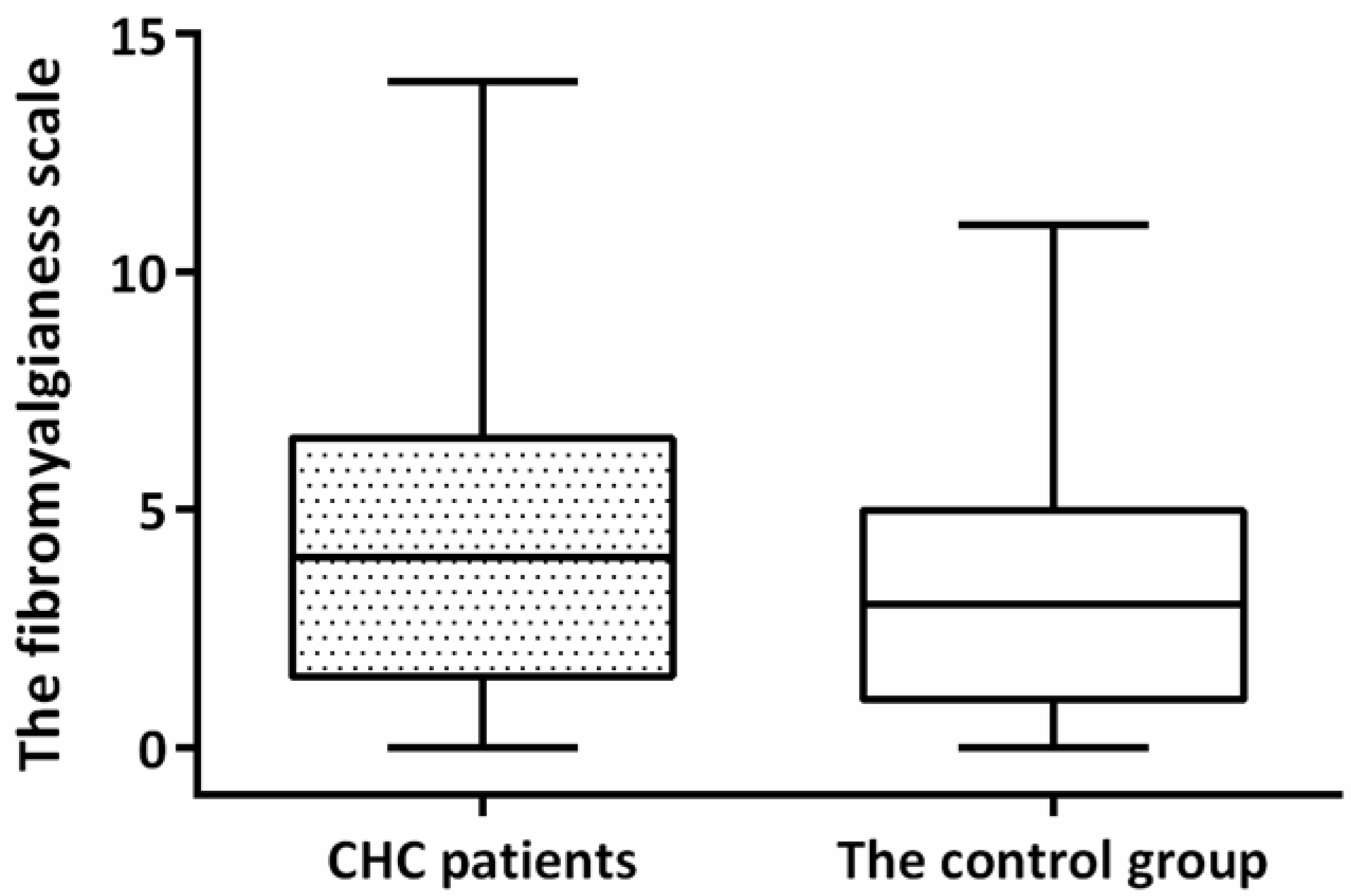
3.2. The Prevalence of FM in CHC Patients and the Control Group at Baseline
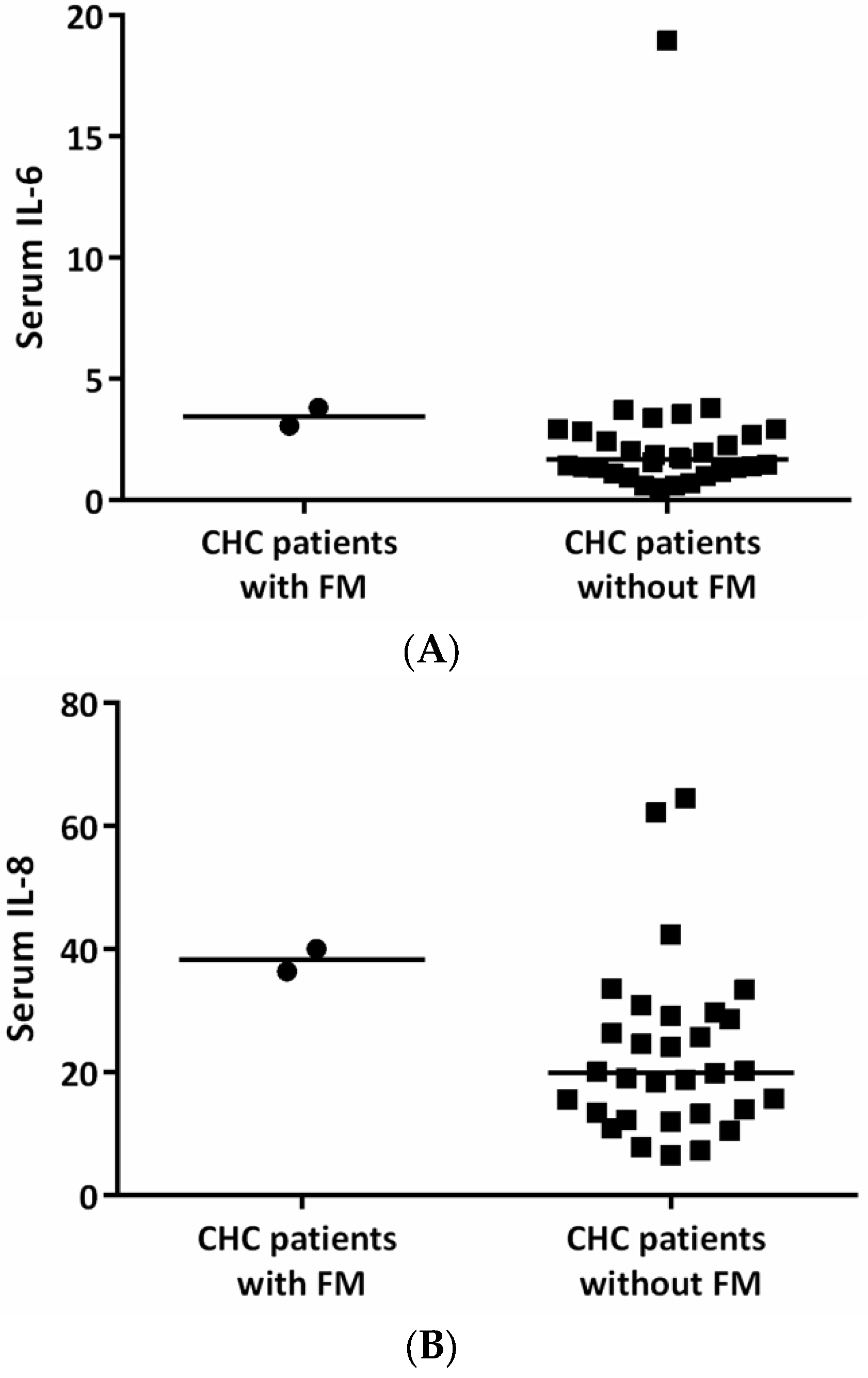
3.3. Factors Associated with FM in CHC Patients at Baseline
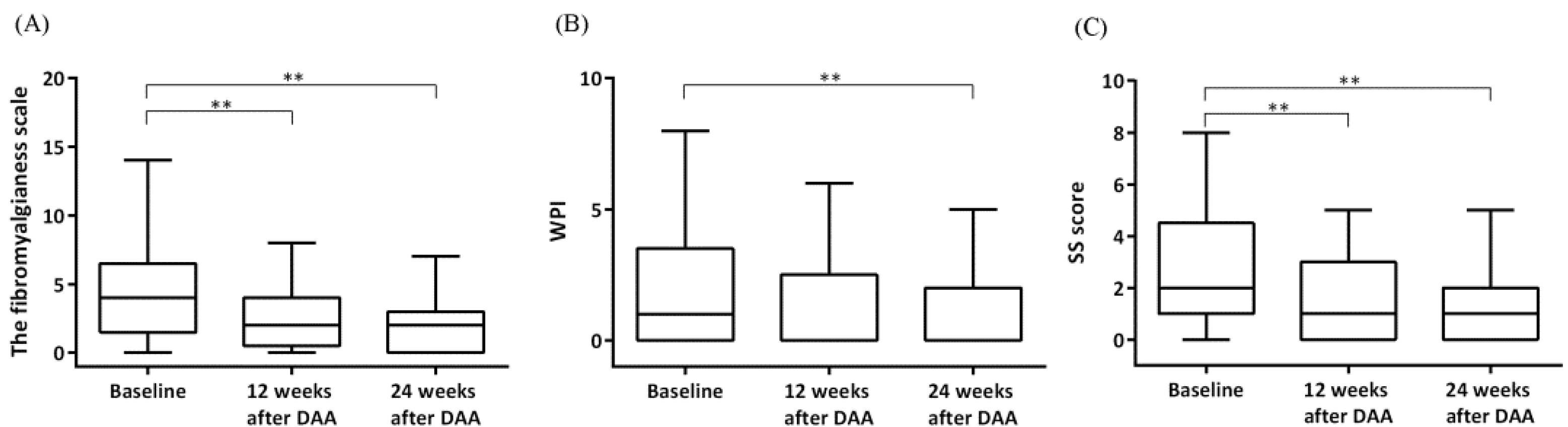
3.4. The Impact of DAA Therapy on FM Symptoms in HCV Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahman, A.; Underwood, M.; Carnes, D. Fibromyalgia. BMJ 2014, 348, g1224. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Hauser, W.; Fluss, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Pinto, I.; Agmon-Levin, N.; Howard, A.; Shoenfeld, Y. Fibromyalgia and cytokines. Immunol. Lett. 2014, 161, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.J.; Linker-Israeli, M.; Hallegua, D.; Silverman, S.; Silver, D.; Weisman, M.H. Cytokines play an aetiopathogenetic role in fibromyalgia: A hypothesis and pilot study. Rheumatology 2001, 40, 743–749. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Perrot, S.; Hauser, W. Comorbid fibromyalgia: A qualitative review of prevalence and importance. Eur. J. Pain 2018, 22, 1565–1576. [Google Scholar] [CrossRef]
- Gupta, N.; Bhatnagar, A.K. Musculoskeletal manifestations of tuberculosis: An observational study. J. Fam. Med. Prim. Care 2018, 7, 538–541. [Google Scholar] [CrossRef]
- Kozanoglu, E.; Canataroglu, A.; Abayli, B.; Colakoglu, S.; Goncu, K. Fibromyalgia syndrome in patients with hepatitis C infection. Rheumatol. Int. 2003, 23, 248–251. [Google Scholar] [CrossRef]
- Garcia, J.B.S.; Moura, S.A.d.M.; Kraychete, D.C.; Castro, A.P.C.R.; Garcia, M.A. Clinical evaluation and prevalence of fibromyalgia in hepatitis C patients. Braz. J. Pain 2019, 2, 308–315. [Google Scholar] [CrossRef]
- Rivera, J.; de Diego, A.; Trinchet, M.; Garcia Monforte, A. Fibromyalgia-associated hepatitis C virus infection. Br. J. Rheumatol. 1997, 36, 981–985. [Google Scholar] [CrossRef]
- Buskila, D.; Shnaider, A.; Neumann, L.; Zilberman, D.; Hilzenrat, N.; Sikuler, E. Fibromyalgia in hepatitis C virus infection. Another infectious disease relationship. Arch. Intern. Med. 1997, 157, 2497–2500. [Google Scholar] [CrossRef]
- Malaguarnera, M.; Di Fazio, I.; Romeo, M.A.; Restuccia, S.; Laurino, A.; Trovato, B.A. Elevation of interleukin 6 levels in patients with chronic hepatitis due to hepatitis C virus. J. Gastroenterol. 1997, 32, 211–215. [Google Scholar] [CrossRef]
- Polyak, S.J.; Khabar, K.S.; Rezeiq, M.; Gretch, D.R. Elevated levels of interleukin-8 in serum are associated with hepatitis C virus infection and resistance to interferon therapy. J. Virol. 2001, 75, 6209–6211. [Google Scholar] [CrossRef]
- Goldenberg, D.L. Do infections trigger fibromyalgia? Arthritis Rheum. 1993, 36, 1489–1492. [Google Scholar] [CrossRef]
- Chen, D.S.; Kuo, G.C.; Sung, J.L.; Lai, M.Y.; Sheu, J.C.; Chen, P.J.; Yang, P.M.; Hsu, H.M.; Chang, M.H.; Chen, C.J.; et al. Hepatitis C virus infection in an area hyperendemic for hepatitis B and chronic liver disease: The Taiwan experience. J. Infect. Dis. 1990, 162, 817–822. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Chen, C.L.; Chen, J.W.; Hsu, N.T.; Wei, S.T.; Hou, S.M.; Lu, S.N.; Chen, P.J. Secular Trends and Geographic Maps of Hepatitis C Virus Infection among 4 Million Blood Donors in Taiwan from 1999 to 2017. Hepatol. Commun. 2020, 4, 1193–1205. [Google Scholar] [CrossRef]
- Flemming, J.A.; Kim, W.R.; Brosgart, C.L.; Terrault, N.A. Reduction in liver transplant wait-listing in the era of direct-acting antiviral therapy. Hepatology 2017, 65, 804–812. [Google Scholar] [CrossRef]
- Kanwal, F.; Kramer, J.; Asch, S.M.; Chayanupatkul, M.; Cao, Y.; El-Serag, H.B. Risk of Hepatocellular Cancer in HCV Patients Treated With Direct-Acting Antiviral Agents. Gastroenterology 2017, 153, 996–1005.e1. [Google Scholar] [CrossRef]
- Cacoub, P.; Saadoun, D. Extrahepatic Manifestations of Chronic HCV Infection. N. Engl. J. Med. 2021, 384, 1038–1052. [Google Scholar] [CrossRef]
- Bonacci, M.; Lens, S.; Marino, Z.; Londono, M.C.; Rodriguez-Tajes, S.; Sanchez-Tapias, J.M.; Ramos-Casals, M.; Hernandez-Rodriguez, J.; Forns, X. Long-Term Outcomes of Patients With HCV-Associated Cryoglobulinemic Vasculitis After Virologic Cure. Gastroenterology 2018, 155, 311–315.e6. [Google Scholar] [CrossRef]
- Ferrari, R.; Russell, A.S. A questionnaire using the modified 2010 American College of Rheumatology criteria for fibromyalgia: Specificity and sensitivity in clinical practice. J. Rheumatol. 2013, 40, 1590–1595. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Hauser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: A modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J. Rheumatol. 2011, 38, 1113–1122. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Hauser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Wolfe, F.; Walitt, B.T.; Rasker, J.J.; Katz, R.S.; Hauser, W. The Use of Polysymptomatic Distress Categories in the Evaluation of Fibromyalgia (FM) and FM Severity. J. Rheumatol. 2015, 42, 1494–1501. [Google Scholar] [CrossRef]
- Bennett, R.M.; Friend, R.; Jones, K.D.; Ward, R.; Han, B.K.; Ross, R.L. The Revised Fibromyalgia Impact Questionnaire (FIQR): Validation and psychometric properties. Arthritis Res. Ther. 2009, 11, R120. [Google Scholar] [CrossRef]
- Zuckerman, E.; Keren, D.; Rozenbaum, M.; Toubi, E.; Slobodin, G.; Tamir, A.; Naschitz, J.E.; Yeshurun, D.; Rosner, I. Hepatitis C virus-related arthritis: Characteristics and response to therapy with interferon alpha. Clin. Exp. Rheumatol. 2000, 18, 579–584. [Google Scholar]
- Ferri, C.; Marzo, E.; Longombardo, G.; Lombardini, F.; La Civita, L.; Vanacore, R.; Liberati, A.M.; Gerli, R.; Greco, F.; Moretti, A. Interferon-alpha in mixed cryoglobulinemia patients: A randomized, crossover-controlled trial. Blood 1993, 81, 1132–1136. [Google Scholar] [CrossRef]
- Misiani, R.; Bellavita, P.; Fenili, D.; Vicari, O.; Marchesi, D.; Sironi, P.L.; Zilio, P.; Vernocchi, A.; Massazza, M.; Vendramin, G.; et al. Interferon alfa-2a therapy in cryoglobulinemia associated with hepatitis C virus. N. Engl. J. Med. 1994, 330, 751–756. [Google Scholar] [CrossRef]
- Ghany, M.G.; Morgan, T.R.; AASLD-IDSA Hepatitis C Guidance Panel. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases-Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Lauletta, G.; Russi, S.; Pavone, F.; Vacca, A.; Dammacco, F. Direct-acting antiviral agents in the therapy of hepatitis C virus-related mixed cryoglobulinaemia: A single-centre experience. Arthritis Res. Ther. 2017, 19, 74. [Google Scholar] [CrossRef]
- Saadoun, D.; Thibault, V.; Si Ahmed, S.N.; Alric, L.; Mallet, M.; Guillaud, C.; Izzedine, H.; Plaisier, A.; Fontaine, H.; Costopoulos, M.; et al. Sofosbuvir plus ribavirin for hepatitis C virus-associated cryoglobulinaemia vasculitis: VASCUVALDIC study. Ann. Rheum. Dis. 2016, 75, 1777–1782. [Google Scholar] [CrossRef] [PubMed]
- Shahin, A.A.; Zayed, H.S.; Said, M.; Amer, S.A. Efficacy and safety of sofosbuvir-based, interferon-free therapy: The Management of rheumatologic extrahepatic manifestations associated with chronic hepatitis C virus infection. Z. Rheumatol. 2018, 77, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Kida, T.; Umemura, A.; Kaneshita, S.; Sagawa, R.; Inoue, T.; Toyama, S.; Wada, M.; Kohno, M.; Oda, R.; Inaba, T.; et al. Effectiveness and safety of chronic hepatitis C treatment with direct-acting antivirals in patients with rheumatic diseases: A case-series. Mod. Rheumatol. 2020, 30, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Poynard, T.; Cacoub, P.; Ratziu, V.; Myers, R.P.; Dezailles, M.H.; Mercadier, A.; Ghillani, P.; Charlotte, F.; Piette, J.C.; Moussalli, J.; et al. Fatigue in patients with chronic hepatitis C. J. Viral. Hepat. 2002, 9, 295–303. [Google Scholar] [CrossRef]
- Evon, D.M.; Wahed, A.S.; Johnson, G.; Khalili, M.; Lisker-Melman, M.; Fontana, R.J.; Sarkar, S.; Reeve, B.B.; Hoofnagle, J.H. Fatigue in Patients with Chronic Hepatitis B Living in North America: Results from the Hepatitis B Research Network (HBRN). Dig. Dis. Sci. 2016, 61, 1186–1196. [Google Scholar] [CrossRef]
- Kallman, J.; O’Neil, M.M.; Larive, B.; Boparai, N.; Calabrese, L.; Younossi, Z.M. Fatigue and health-related quality of life (HRQL) in chronic hepatitis C virus infection. Dig. Dis. Sci. 2007, 52, 2531–2539. [Google Scholar] [CrossRef]
- Hassoun, Z.; Willems, B.; Deslauriers, J.; Nguyen, B.N.; Huet, P.M. Assessment of fatigue in patients with chronic hepatitis C using the Fatigue Impact Scale. Dig. Dis. Sci. 2002, 47, 2674–2681. [Google Scholar] [CrossRef]
- Sarkar, S.; Jiang, Z.; Evon, D.M.; Wahed, A.S.; Hoofnagle, J.H. Fatigue before, during and after antiviral therapy of chronic hepatitis C: Results from the Virahep-C study. J. Hepatol. 2012, 57, 946–952. [Google Scholar] [CrossRef]
- Fagundes, R.N.; Ferreira, L.; Pace, F.H.L. Health-related quality of life and fatigue in patients with chronic hepatitis C with therapy with direct-acting antivirals agents interferon-free. PLoS ONE 2020, 15, e0237005. [Google Scholar] [CrossRef]
- Heeren, M.; Sojref, F.; Schuppner, R.; Worthmann, H.; Pflugrad, H.; Tryc, A.B.; Pasedag, T.; Weissenborn, K. Active at night, sleepy all day-sleep disturbances in patients with hepatitis C virus infection. J. Hepatol. 2014, 60, 732–740. [Google Scholar] [CrossRef]
- Kang, J.H.; Choi, S.E.; Xu, H.; Park, D.J.; Lee, J.K.; Lee, S.S. Comparison of the AAPT Fibromyalgia Diagnostic Criteria and Modified FAS Criteria with Existing ACR Criteria for Fibromyalgia in Korean Patients. Rheumatol. Ther. 2021, 8, 1003–1014. [Google Scholar] [CrossRef]
- Neumann, L.; Buskila, D. Epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2003, 7, 362–368. [Google Scholar] [CrossRef]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology 2021, 60, 2602–2614. [Google Scholar] [CrossRef]
- Chou, P.H.; Tang, K.T.; Chen, Y.H.; Sun, C.W.; Huang, C.M.; Chen, D.Y. Reduced frontal activity during a verbal fluency test in fibromyalgia: A near-infrared spectroscopy study. J. Clin. Neurosci. 2018, 50, 35–40. [Google Scholar] [CrossRef]
- Gracely, R.H.; Ambrose, K.R. Neuroimaging of fibromyalgia. Best Pract. Res. Clin. Rheumatol. 2011, 25, 271–284. [Google Scholar] [CrossRef]
- Charlton, M.R.; Pockros, P.J.; Harrison, S.A. Impact of obesity on treatment of chronic hepatitis C. Hepatology 2006, 43, 1177–1186. [Google Scholar] [CrossRef]
- Kwok, W.C.; Ma, T.F.; Chan, J.W.M.; Pang, H.H.; Ho, J.C.M. A multicenter retrospective cohort study on predicting the risk for amiodarone pulmonary toxicity. BMC Pulm. Med. 2022, 22, 128. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CHC Patients (n = 33) | The Control Group (n = 402) | |
|---|---|---|
| Age, mean (SD) * | 58 (11) | 48 (13) |
| Body mass index, median (IQR) | 24.2 (22.5, 26.8) | 23.7 (21.4, 26.2) |
| Female sex, n (%) | 18 (55) | 185 (46) |
| Rheumatic diseases, n (%) | 1 (3) | 13 (3) |
| Chronic hepatitis C, n (%) | 33 (100) | 2 (0.5) |
| HCV viral load, median (IQR) (IU/mL) | 3.3 × 106 (IQR: 1.5 × 106, 6.5 × 106) | N.A. |
| Direct-acting antiviral drugs, n (%) | ||
| Sofosbuvir-velpatasvir | 24 (73) | N.A. |
| Glecaprevir-pibrentasvir | 6 (18) | N.A. |
| Elbasvir-grazoprevir | 3 (9) | N.A. |
| CHC Patients with Fibromyalgia (n = 2) | CHC Patients without Fibromyalgia (n = 31) | |
|---|---|---|
| Age | 55 | 58 (48, 64) |
| Body mass index | 30.5 | 24.2 (21.6, 26.8) |
| Female sex, n (%) | 1 (50) | 17 (55) |
| Serum levels of alanine aminotransferase (U/L) | 172 | 43 (32, 97) |
| Serum levels of aspartate aminotransferase (U/L) | 127 | 42 (26, 69) |
| HCV viral load, mean (SD) (IU/mL) | 1.6 × 106 | 3.8 × 106 (1.5 × 106, 7.7 × 106) |
| Subdomains, n (%) | Baseline | 12 Weeks after DAA Therapy | 24 Weeks after DAA Therapy |
|---|---|---|---|
| Cognitive symptoms | |||
| No | 15 (45) | 19 (58) | 19 (58) |
| Mild | 16 (48) | 12 (36) | 12 (36) |
| Moderate | 2 (6) | 2 (6) | 2 (6) |
| Fatigue | |||
| No | 20 (61) | 22 (67) | 24 (73) * |
| Mild | 9 (27) | 9 (27) | 8 (24) |
| Moderate | 4 (12) | 1 (3) | 1 (3) |
| Severe | 0 (0) | 1 (3) | 0 (0) |
| Waking unrefreshed | |||
| No | 19 (58) | 20 (61) * | 24 (73) * |
| Mild | 6 (18) | 11 (33) | 7 (21) |
| Moderate | 8 (24) | 2 (6) | 2 (6) |
| Headache | 15 (45) | 8 (24) * | 5 (15) * |
| Pain or cramps in lower abdomen | 8 (24) | 1 (3) * | 3 (9) * |
| Depression | 5 (15) | 3 (9) | 2 (6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, K.-T.; Lin, C.-C.; Chen, Y.-H.; Liao, T.-L.; Chen, D.-Y.; Yang, S.-S.; Chen, C.-C. Direct-Acting Antiviral Drugs Reduce Fibromyalgia Symptoms in Patients with Chronic Hepatitis C. J. Clin. Med. 2022, 11, 5327. https://doi.org/10.3390/jcm11185327
Tang K-T, Lin C-C, Chen Y-H, Liao T-L, Chen D-Y, Yang S-S, Chen C-C. Direct-Acting Antiviral Drugs Reduce Fibromyalgia Symptoms in Patients with Chronic Hepatitis C. Journal of Clinical Medicine. 2022; 11(18):5327. https://doi.org/10.3390/jcm11185327
Chicago/Turabian StyleTang, Kuo-Tung, Ching-Chun Lin, Yi-Hsing Chen, Tsai-Ling Liao, Der-Yuan Chen, Sheng-Shun Yang, and Chia-Chang Chen. 2022. "Direct-Acting Antiviral Drugs Reduce Fibromyalgia Symptoms in Patients with Chronic Hepatitis C" Journal of Clinical Medicine 11, no. 18: 5327. https://doi.org/10.3390/jcm11185327