
Does Elevated Pre-Treatment Plasma PD-L1 Level Indicate an Increased Tumor Burden and Worse Prognosis in Metastatic Colorectal Cancer?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Clinicopathological and Laboratory Data Measurements
2.3. Statistical Analysis
3. Results
3.1. Baseline Measurements
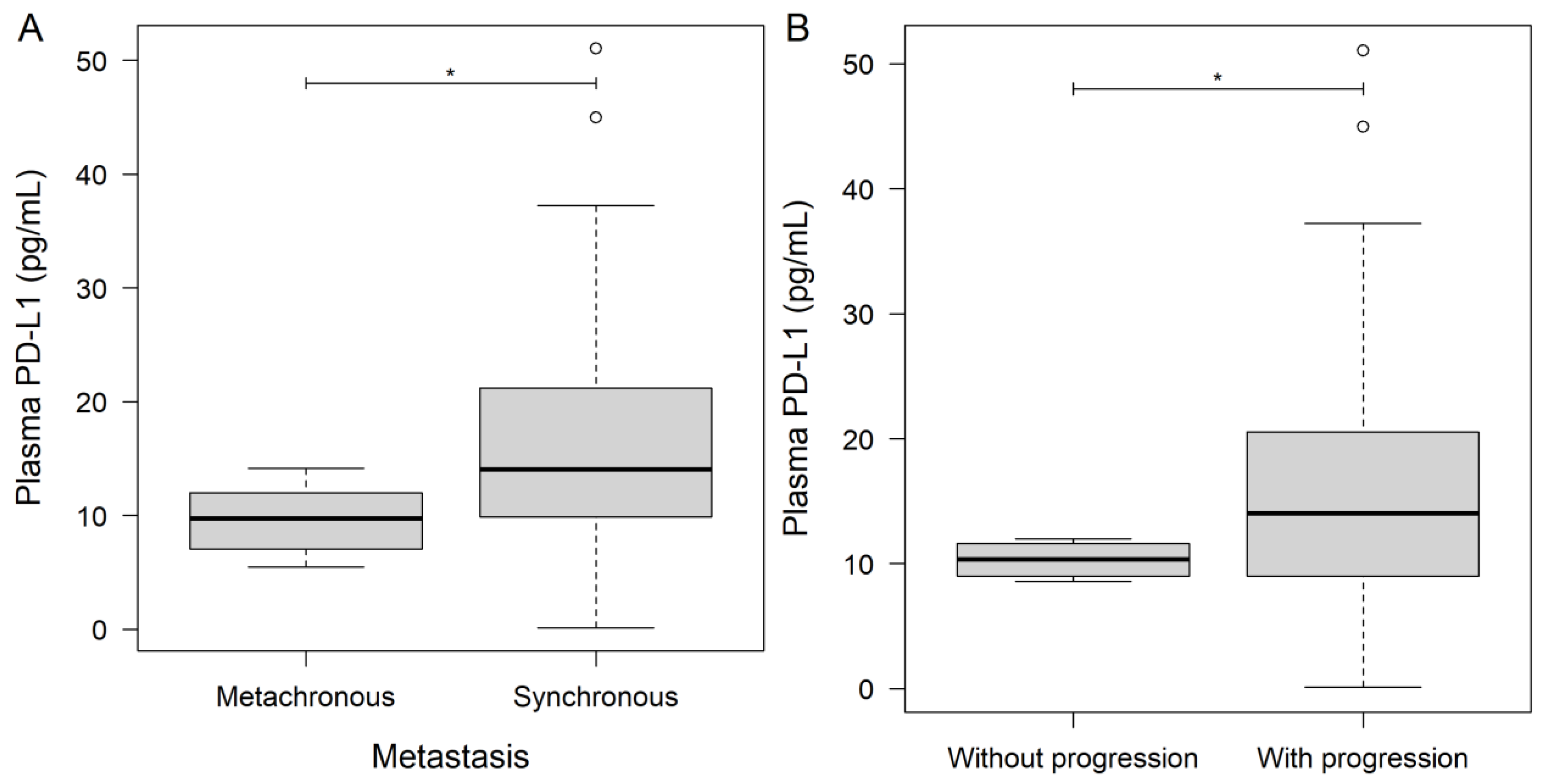
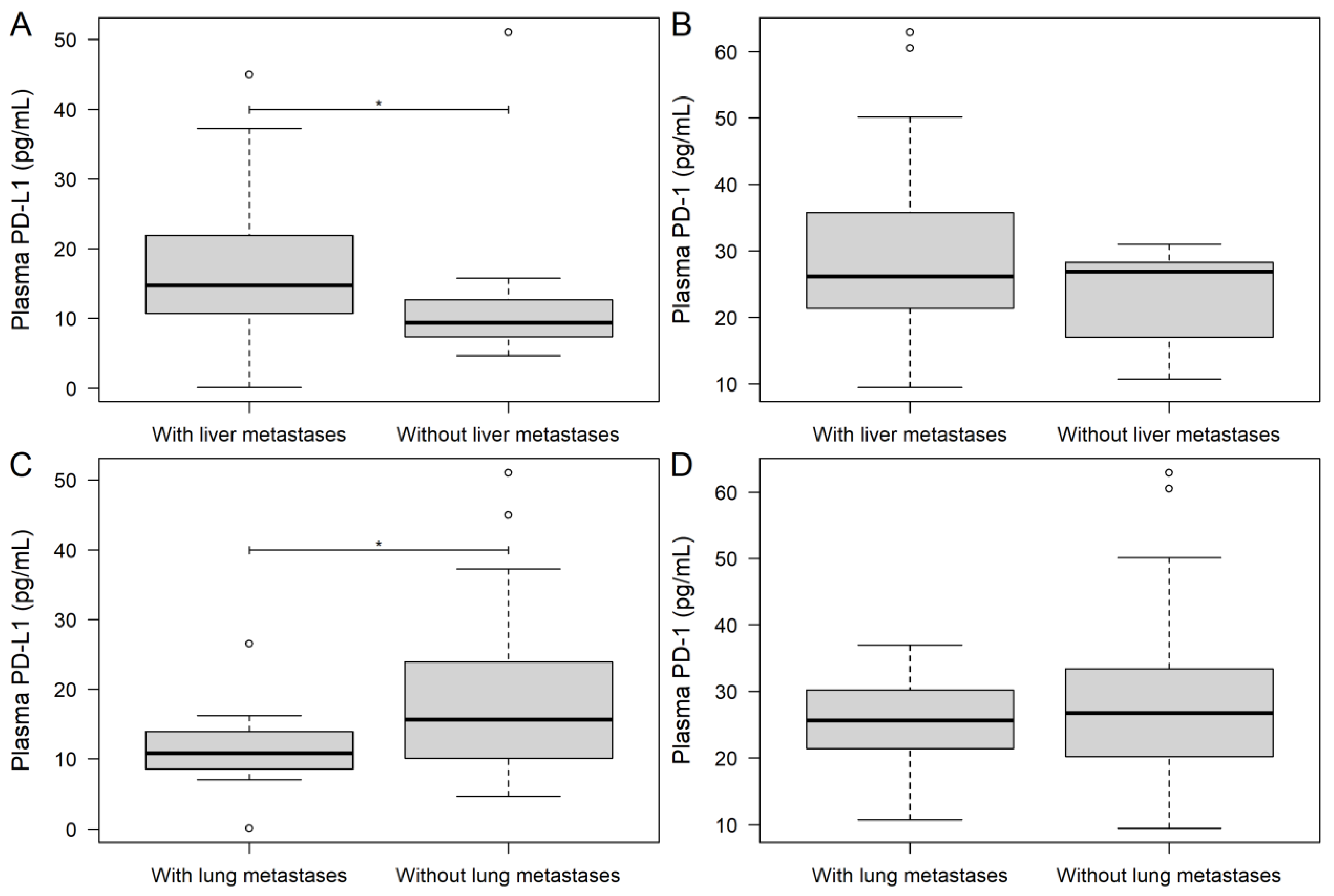
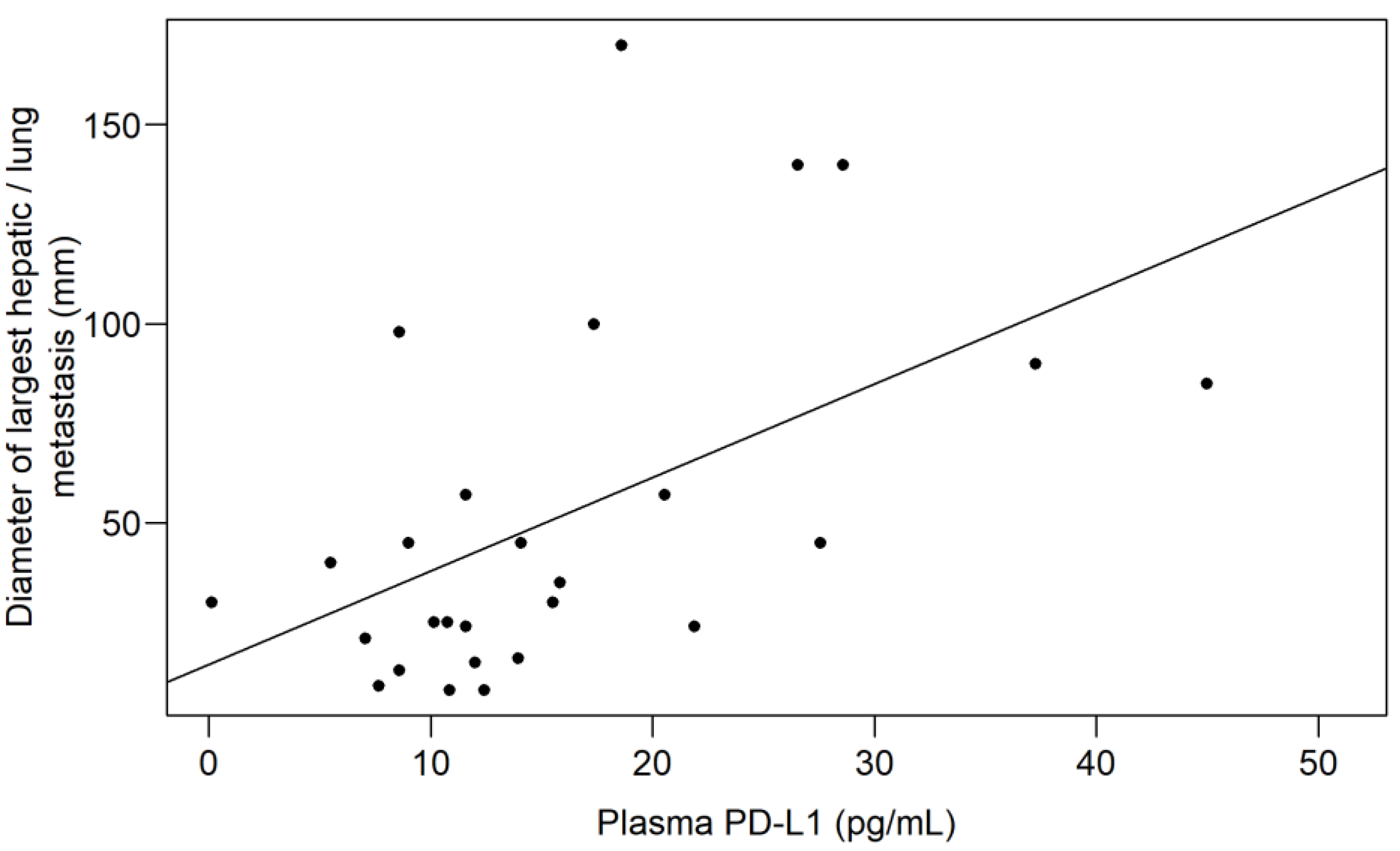
3.2. Investigating the Association between Plasma PD-1/PD-L1 Level and Tumor Burden
3.3. Comparison of Low and High PD-1/PD-L1 Subgroups
3.3.1. Baseline Measurements
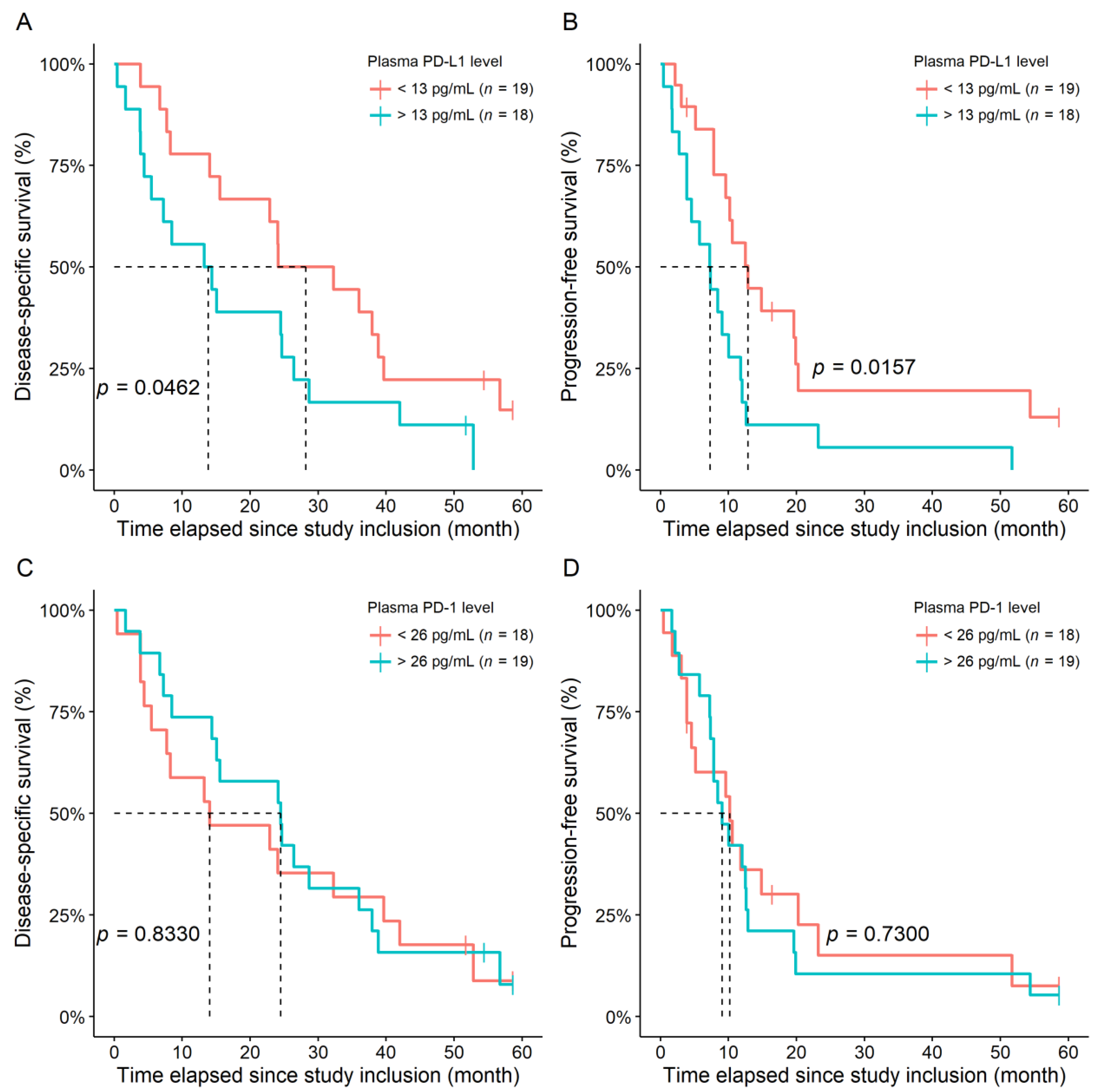
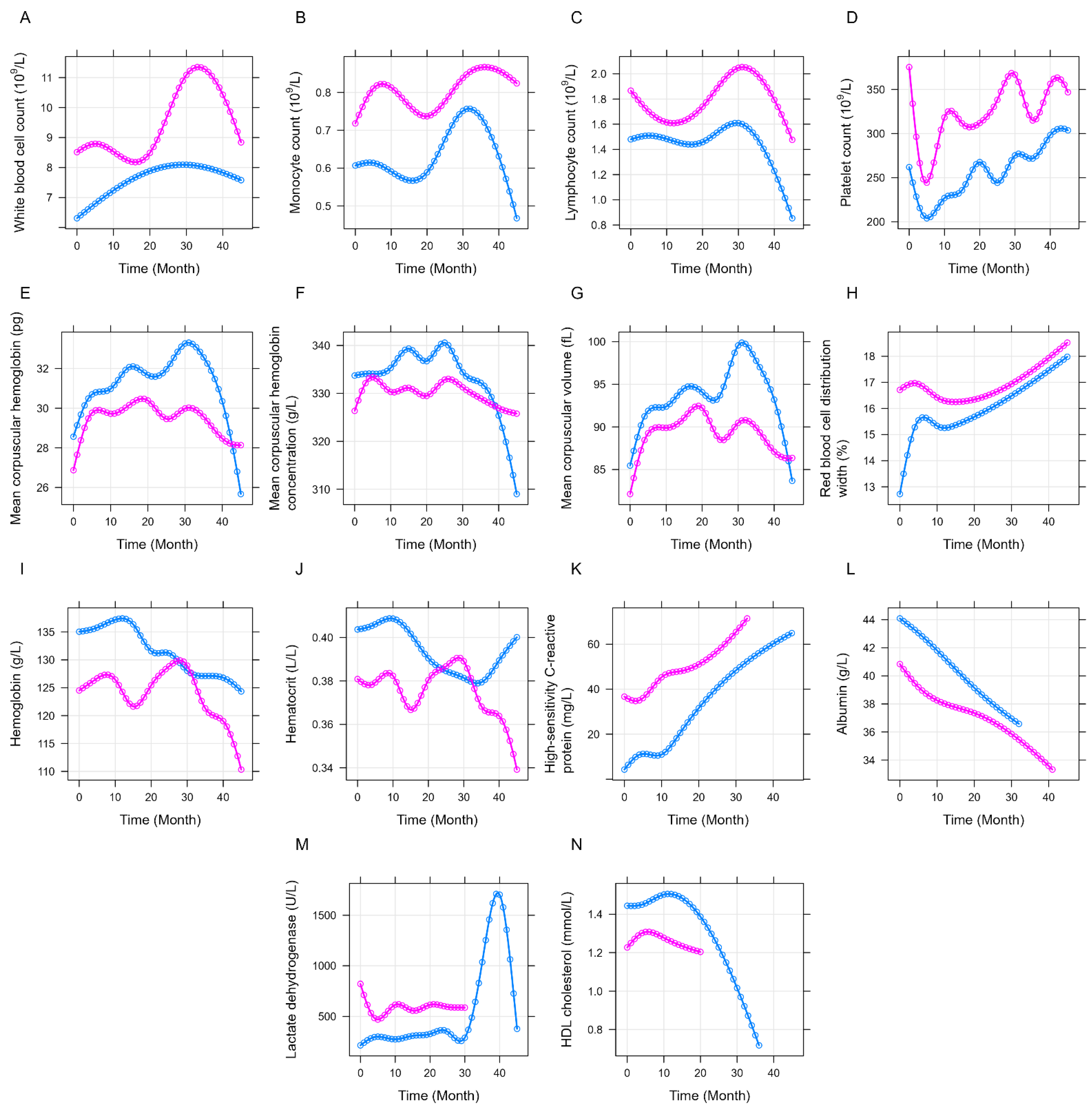
3.3.2. Longitudinal Analysis
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Biller, L.H.; Schrag, D. Diagnosis and Treatment of Metastatic Colorectal Cancer: A Review. JAMA 2021, 325, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Payandeh, Z.; Khalili, S.; Somi, M.H.; Mard-Soltani, M.; Baghbanzadeh, A.; Hajiasgharzadeh, K.; Samadi, N.; Baradaran, B. PD-1/PD-L1-dependent immune response in colorectal cancer. J. Cell Physiol. 2020, 235, 5461–5475. [Google Scholar] [CrossRef] [PubMed]
- Kornepati, A.V.R.; Vadlamudi, R.K.; Curiel, T.J. Programmed death ligand 1 signals in cancer cells. Nat. Rev. Cancer 2022, 22, 174–189. [Google Scholar] [CrossRef]
- Alsaab, H.O.; Sau, S.; Alzhrani, R.; Tatiparti, K.; Bhise, K.; Kashaw, S.K.; Iyer, A.K. PD-1 and PD-L1 Checkpoint Signaling Inhibition for Cancer Immunotherapy: Mechanism, Combinations, and Clinical Outcome. Front. Pharmacol. 2017, 8, 561. [Google Scholar] [CrossRef]
- Zhu, X.; Lang, J. Soluble PD-1 and PD-L1: Predictive and prognostic significance in cancer. Oncotarget 2017, 8, 97671–97682. [Google Scholar] [CrossRef]
- Schildberg, F.A.; Klein, S.R.; Freeman, G.J.; Sharpe, A.H. Coinhibitory Pathways in the B7-CD28 Ligand-Receptor Family. Immunity 2016, 44, 955–972. [Google Scholar] [CrossRef]
- Fife, B.T.; Bluestone, J.A. Control of peripheral T-cell tolerance and autoimmunity via the CTLA-4 and PD-1 pathways. Immunol. Rev. 2008, 224, 166–182. [Google Scholar] [CrossRef]
- Gu, Y.; Morgan, J.; Lewis, D.F.; Cooper, D.B.; McCathran, C.E.; Wang, Y. Maternal soluble PD-1 levels are significantly increased in women with preeclampsia. Am. J. Reprod. Immunol. 2020, 83, e13193. [Google Scholar] [CrossRef]
- Gu, D.; Ao, X.; Yang, Y.; Chen, Z.; Xu, X. Soluble immune checkpoints in cancer: Production, function and biological significance. J. Immunother. Cancer 2018, 6, 132. [Google Scholar] [CrossRef]
- Liu, J.; Peng, X.; Yang, S.; Li, X.; Huang, M.; Wei, S.; Zhang, S.; He, G.; Zheng, H.; Fan, Q.; et al. Extracellular vesicle PD-L1 in reshaping tumor immune microenvironment: Biological function and potential therapy strategies. Cell Commun. Signal. 2022, 20, 14. [Google Scholar] [CrossRef] [PubMed]
- Okuma, Y.; Hosomi, Y.; Nakahara, Y.; Watanabe, K.; Sagawa, Y.; Homma, S. High plasma levels of soluble programmed cell death ligand 1 are prognostic for reduced survival in advanced lung cancer. Lung Cancer 2017, 104, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tominaga, T.; Akiyoshi, T.; Yamamoto, N.; Taguchi, S.; Mori, S.; Nagasaki, T.; Fukunaga, Y.; Ueno, M. Clinical significance of soluble programmed cell death-1 and soluble programmed cell death-ligand 1 in patients with locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy. PLoS ONE 2019, 14, e0212978. [Google Scholar] [CrossRef] [PubMed]
- Costantini, A.; Julie, C.; Dumenil, C.; Helias-Rodzewicz, Z.; Tisserand, J.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Emile, J.F.; et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. Oncoimmunology 2018, 7, e1452581. [Google Scholar] [CrossRef]
- Krafft, U.; Olah, C.; Reis, H.; Kesch, C.; Darr, C.; Grunwald, V.; Tschirdewahn, S.; Hadaschik, B.; Horvath, O.; Kenessey, I.; et al. High Serum PD-L1 Levels Are Associated with Poor Survival in Urothelial Cancer Patients Treated with Chemotherapy and Immune Checkpoint Inhibitor Therapy. Cancers 2021, 13, 2548. [Google Scholar] [CrossRef]
- Montemagno, C.; Hagege, A.; Borchiellini, D.; Thamphya, B.; Rastoin, O.; Ambrosetti, D.; Iovanna, J.; Rioux-Leclercq, N.; Porta, C.; Negrier, S.; et al. Soluble forms of PD-L1 and PD-1 as prognostic and predictive markers of sunitinib efficacy in patients with metastatic clear cell renal cell carcinoma. Oncoimmunology 2020, 9, 1846901. [Google Scholar] [CrossRef]
- Omura, Y.; Toiyama, Y.; Okugawa, Y.; Yin, C.; Shigemori, T.; Kusunoki, K.; Kusunoki, Y.; Ide, S.; Shimura, T.; Fujikawa, H.; et al. Prognostic impacts of tumoral expression and serum levels of PD-L1 and CTLA-4 in colorectal cancer patients. Cancer Immunol. Immunother. 2020, 69, 2533–2546. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef]
- Schwandt, A.; Denkinger, M.; Fasching, P.; Pfeifer, M.; Wagner, C.; Weiland, J.; Zeyfang, A.; Holl, R.W. Comparison of MDRD, CKD-EPI, and Cockcroft-Gault equation in relation to measured glomerular filtration rate among a large cohort with diabetes. J. Diabetes Complicat. 2017, 31, 1376–1383. [Google Scholar] [CrossRef]
- Jessup, J.; Goldberg, R.; Asare, E.; Benson, A.; Brierley, J.; Chang, G.; Chen, V.; Compton, C.; De Nardi, P.; Goodman, K.; et al. Colon and Rectum. In AJCC Cancer Staging Manual, 8th ed.; Amin, M., Edge, S., Greene, F., Byrd, D., Brookland, R., Washington, M., Gershenwald, J., Compton, C., Hess, K., Sullivan, D., et al., Eds.; Springer International Publishing: Chicago, IL, USA, 2018; pp. 251–274. [Google Scholar]
- Baran, B.; Mert Ozupek, N.; Yerli Tetik, N.; Acar, E.; Bekcioglu, O.; Baskin, Y. Difference between Left-Sided and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterol. Res. 2018, 11, 264–273. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.; Monette, G. Generalized Collinearity Diagnostics. JASA 1992, 87, 178–183. [Google Scholar] [CrossRef]
- Grambsch, P.M.; Therneau, T.M. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 1994, 81, 515–526. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Ren, X.; Li, Y.; Nishimura, C.; Zang, X. Crosstalk between the B7/CD28 and EGFR pathways: Mechanisms and therapeutic opportunities. Genes Dis. 2022, 9, 1181–1193. [Google Scholar] [CrossRef]
- Ganesh, K.; Stadler, Z.K.; Cercek, A.; Mendelsohn, R.B.; Shia, J.; Segal, N.H.; Diaz, L.A., Jr. Immunotherapy in colorectal cancer: Rationale, challenges and potential. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 361–375. [Google Scholar] [CrossRef]
- Boukouris, A.E.; Theochari, M.; Stefanou, D.; Papalambros, A.; Felekouras, E.; Gogas, H.; Ziogas, D.C. Latest evidence on immune checkpoint inhibitors in metastatic colorectal cancer: A 2022 update. Crit. Rev. Oncol. Hematol. 2022, 173, 103663. [Google Scholar] [CrossRef]
- Weng, J.; Li, S.; Zhu, Z.; Liu, Q.; Zhang, R.; Yang, Y.; Li, X. Exploring immunotherapy in colorectal cancer. J. Hematol. Oncol. 2022, 15, 95. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, Z.; An, Y.; Liu, Y.; Wei, Q.; Xu, F.; Yao, H.; Zhang, Z. Clinical benefits of PD-1/PD-L1 inhibitors in patients with metastatic colorectal cancer: A systematic review and meta-analysis. World J. Surg. Oncol. 2022, 20, 93. [Google Scholar] [CrossRef] [PubMed]
- Baraibar, I.; Mirallas, O.; Saoudi, N.; Ros, J.; Salva, F.; Tabernero, J.; Elez, E. Combined Treatment with Immunotherapy-Based Strategies for MSS Metastatic Colorectal Cancer. Cancers 2021, 13, 6311. [Google Scholar] [CrossRef] [PubMed]
- Galbraith, N.J.; Wood, C.; Steele, C.W. Targeting Metastatic Colorectal Cancer with Immune Oncological Therapies. Cancers 2021, 13, 3566. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, M.W.; Bledsoe, J.R.; Morales-Oyarvide, V.; Huynh, T.G.; Mino-Kenudson, M. PD-L1 expression in colorectal cancer is associated with microsatellite instability, BRAF mutation, medullary morphology and cytotoxic tumor-infiltrating lymphocytes. Mod. Pathol. 2016, 29, 1104–1112. [Google Scholar] [CrossRef]
- Tintelnot, J.; Stein, A. Immunotherapy in colorectal cancer: Available clinical evidence, challenges and novel approaches. World J. Gastroenterol. 2019, 25, 3920–3928. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.; Bang, J.H.; Nam, A.R.; Park, J.E.; Jin, M.H.; Bang, Y.J.; Oh, D.Y. Dynamics of Soluble Programmed Death-Ligand 1 (sPDL1) during Chemotherapy and Its Prognostic Implications in Cancer Patients: Biomarker Development in Immuno-oncology. Cancer Res. Treat. 2019, 51, 832–840. [Google Scholar] [CrossRef]
- Ha, H.; Nam, A.R.; Bang, J.H.; Park, J.E.; Kim, T.Y.; Lee, K.H.; Han, S.W.; Im, S.A.; Kim, T.Y.; Bang, Y.J.; et al. Soluble programmed death-ligand 1 (sPDL1) and neutrophil-to-lymphocyte ratio (NLR) predicts survival in advanced biliary tract cancer patients treated with palliative chemotherapy. Oncotarget 2016, 7, 76604–76612. [Google Scholar] [CrossRef]
- Oh, S.Y.; Kim, S.; Keam, B.; Kim, T.M.; Kim, D.W.; Heo, D.S. Soluble PD-L1 is a predictive and prognostic biomarker in advanced cancer patients who receive immune checkpoint blockade treatment. Sci. Rep. 2021, 11, 19712. [Google Scholar] [CrossRef]
- Park, W.; Bang, J.H.; Nam, A.R.; Jin, M.H.; Seo, H.; Kim, J.M.; Oh, K.S.; Kim, T.Y.; Oh, D.Y. Prognostic Value of Serum Soluble Programmed Death-Ligand 1 and Dynamics during Chemotherapy in Advanced Gastric Cancer Patients. Cancer Res. Treat. 2021, 53, 199–206. [Google Scholar] [CrossRef]
- Dong, M.P.; Enomoto, M.; Thuy, L.T.T.; Hai, H.; Hieu, V.N.; Hoang, D.V.; Iida-Ueno, A.; Odagiri, N.; Amano-Teranishi, Y.; Hagihara, A.; et al. Clinical significance of circulating soluble immune checkpoint proteins in sorafenib-treated patients with advanced hepatocellular carcinoma. Sci. Rep. 2020, 10, 3392. [Google Scholar] [CrossRef]
- Mocan, T.; Ilies, M.; Nenu, I.; Craciun, R.; Horhat, A.; Susa, R.; Minciuna, I.; Rusu, I.; Mocan, L.P.; Seicean, A.; et al. Serum levels of soluble programmed death-ligand 1 (sPD-L1): A possible biomarker in predicting post-treatment outcomes in patients with early hepatocellular carcinoma. Int. Immunopharmacol. 2021, 94, 107467. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, K.M.; Ross-Macdonald, P.; Yuan, L.; Song, L.; Veras, E.; Wind-Rotolo, M.; McDermott, D.F.; Stephen Hodi, F.; Choueiri, T.K.; Freeman, G.J. Soluble PD-L1 as an early marker of progressive disease on nivolumab. J. Immunother. Cancer 2022, 10, e003527. [Google Scholar] [CrossRef] [PubMed]
- Swiderska, J.; Kozlowski, M.; Nowak, K.; Rychlicka, M.; Branecka-Wozniak, D.; Kwiatkowski, S.; Pius-Sadowska, E.; Machalinski, B.; Cymbaluk-Ploska, A. Clinical Relevance of Soluble Forms of Immune Checkpoint Molecules sPD-1, sPD-L1, and sCTLA-4 in the Diagnosis and Prognosis of Ovarian Cancer. Diagnostics 2022, 12, 189. [Google Scholar] [CrossRef]
- Tiako Meyo, M.; Jouinot, A.; Giroux-Leprieur, E.; Fabre, E.; Wislez, M.; Alifano, M.; Leroy, K.; Boudou-Rouquette, P.; Tlemsani, C.; Khoudour, N.; et al. Predictive Value of Soluble PD-1, PD-L1, VEGFA, CD40 Ligand and CD44 for Nivolumab Therapy in Advanced Non-Small Cell Lung Cancer: A Case-Control Study. Cancers 2020, 12, 473. [Google Scholar] [CrossRef]
- Ohkuma, R.; Ieguchi, K.; Watanabe, M.; Takayanagi, D.; Goshima, T.; Onoue, R.; Hamada, K.; Kubota, Y.; Horiike, A.; Ishiguro, T.; et al. Increased Plasma Soluble PD-1 Concentration Correlates with Disease Progression in Patients with Cancer Treated with Anti-PD-1 Antibodies. Biomedicines 2021, 9, 1929. [Google Scholar] [CrossRef] [PubMed]
- Kovaleva, O.V.; Rashidova, M.A.; Gratchev, A.N.; Maslennikov, V.V.; Boulitcheva, I.V.; Gershtein, E.S.; Korotkova, E.A.; Sokolov, N.Y.; Delektorskaya, V.V.; Mamedli, Z.Z.; et al. Immunosuppression Factors PD-1, PD-L1, and IDO1 and Colorectal Cancer. Dokl. Biochem. Biophys. 2021, 497, 66–70. [Google Scholar] [CrossRef]
- Lushnikova, A.; Bohr, J.; Wickbom, A.; Munch, A.; Sjoberg, K.; Hultgren, O.; Wiren, A.; Hultgren Hornquist, E. Patients with Microscopic Colitis Have Altered Levels of Inhibitory and Stimulatory Biomarkers in Colon Biopsies and Sera Compared to Non-inflamed Controls. Front. Med. 2021, 8, 727412. [Google Scholar] [CrossRef]
- Akhmaltdinova, L.; Sirota, V.; Zhumaliyeva, V.; Babenko, D.; Kadyrova, I.; Tauesheva, Z.; Taizhanova, D.; Ibraeva, A.; Maratkyzy, M.; Turmukhambetova, A. Inflammatory Serum Biomarkers in Colorectal Cancer in Kazakhstan Population. Int. J. Inflamm. 2020, 2020, 9476326. [Google Scholar] [CrossRef]
- Chen, X.; Du, Z.; Huang, M.; Wang, D.; Fong, W.P.; Liang, J.; Fan, L.; Wang, Y.; Yang, H.; Chen, Z.; et al. Circulating PD-L1 is associated with T cell infiltration and predicts prognosis in patients with CRLM following hepatic resection. Cancer Immunol. Immunother. 2022, 71, 661–674. [Google Scholar] [CrossRef]
- Muneoka, K.; Shirai, Y.; Sasaki, M.; Honma, S.; Sakata, J.; Kanda, J.; Wakabayashi, H.; Wakai, T.; Miyazaki, M. Selection of Chemotherapy Regimen on the Basis of Monitoring NLR and Soluble PD-L1 during CRC Chemotherapy. Gan Kagaku Ryoho 2018, 45, 1159–1163. [Google Scholar]
- Sun, J.; Qiu, M.Z.; Mei, T.; Gao, Y.; Chang, B.; Zhang, Y.; Wang, F.H.; Li, S. Dynamic monitoring of serum soluble programmed cell death ligand 1 as a response predictor to chemotherapy in metastatic or recurrent gastrointestinal cancer. Transl. Cancer Res. 2020, 9, 2434–2448. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.L.; Yang, C.Y.; Huang, Y.L.; Wu, C.T.; Yang, P.C. High PD-L1 expression is associated with stage IV disease and poorer overall survival in 186 cases of small cell lung cancers. Oncotarget 2017, 8, 18021–18030. [Google Scholar] [CrossRef] [PubMed]
- Shan, T.; Chen, S.; Wu, T.; Yang, Y.; Li, S.; Chen, X. PD-L1 expression in colon cancer and its relationship with clinical prognosis. Int. J. Clin. Exp. Pathol. 2019, 12, 1764–1769. [Google Scholar] [PubMed]
- Niu, M.; Liu, Y.; Yi, M.; Jiao, D.; Wu, K. Biological Characteristics and Clinical Significance of Soluble PD-1/PD-L1 and Exosomal PD-L1 in Cancer. Front. Immunol. 2022, 13, 827921. [Google Scholar] [CrossRef] [PubMed]
- Asanuma, K.; Nakamura, T.; Hayashi, A.; Okamoto, T.; Iino, T.; Asanuma, Y.; Hagi, T.; Kita, K.; Nakamura, K.; Sudo, A. Soluble programmed death-ligand 1 rather than PD-L1 on tumor cells effectively predicts metastasis and prognosis in soft tissue sarcomas. Sci. Rep. 2020, 10, 9077. [Google Scholar] [CrossRef]
- Han, B.; Dong, L.; Zhou, J.; Yang, Y.; Guo, J.; Xuan, Q.; Gao, K.; Xu, Z.; Lei, W.; Wang, J.; et al. The clinical implication of soluble PD-L1 (sPD-L1) in patients with breast cancer and its biological function in regulating the function of T lymphocyte. Cancer Immunol. Immunother. 2021, 70, 2893–2909. [Google Scholar] [CrossRef]
- Cubillos-Zapata, C.; Martinez-Garcia, M.A.; Campos-Rodriguez, F.; Sanchez de la Torre, M.; Nagore, E.; Martorell-Calatayud, A.; Hernandez Blasco, L.; Chiner Vives, E.; Abad-Capa, J.; Montserrat, J.M.; et al. Soluble PD-L1 is a potential biomarker of cutaneous melanoma aggressiveness and metastasis in obstructive sleep apnoea patients. Eur. Respir. J. 2019, 53, 1801298. [Google Scholar] [CrossRef]
- Larrinaga, G.; Solano-Iturri, J.D.; Errarte, P.; Unda, M.; Loizaga-Iriarte, A.; Perez-Fernandez, A.; Echevarria, E.; Asumendi, A.; Manini, C.; Angulo, J.C.; et al. Soluble PD-L1 Is an Independent Prognostic Factor in Clear Cell Renal Cell Carcinoma. Cancers 2021, 13, 667. [Google Scholar] [CrossRef]
- Vikerfors, A.; Davidsson, S.; Frey, J.; Jerlstrom, T.; Carlsson, J. Soluble PD-L1 in Serum and Urine in Urinary Bladder Cancer Patients. Cancers 2021, 13, 5841. [Google Scholar] [CrossRef]
- Bakács, T.; Lee, J.; Moreno, M.B.; Zacharchuk, C.M.; Cole, M.S.; Tso, J.Y.; Paik, C.H.; Ward, J.M.; Segal, D.M. A bispecific antibody prolongs survival in mice bearing lung metastases of syngeneic mammary adenocarcinoma. Int. Immunol. 1995, 7, 947–955. [Google Scholar] [CrossRef]
- Kleef, R.; Moss, R.; Szasz, A.M.; Bohdjalian, A.; Bojar, H.; Bakacs, T. Complete Clinical Remission of Stage IV Triple-Negative Breast Cancer Lung Metastasis Administering Low-Dose Immune Checkpoint Blockade in Combination with Hyperthermia and Interleukin-2. Integr. Cancer Ther. 2018, 17, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Agulnik, J.; Kasymjanova, G.; Fiset, P.O.; Camilleri-Broet, S.; Redpath, M.; Cohen, V.; Small, D.; Pepe, C.; Sakr, L.; et al. The metastatic site does not influence PD-L1 expression in advanced non-small cell lung carcinoma. Lung Cancer 2019, 132, 36–38. [Google Scholar] [CrossRef] [PubMed]
- Rozenblit, M.; Huang, R.; Danziger, N.; Hegde, P.; Alexander, B.; Ramkissoon, S.; Blenman, K.; Ross, J.S.; Rimm, D.L.; Pusztai, L. Comparison of PD-L1 protein expression between primary tumors and metastatic lesions in triple negative breast cancers. J. Immunother. Cancer 2020, 8, e001558. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yin, X.; Zhang, H.; Sun, G.; Yang, Y.; Chen, J.; Zhu, X.; Zhao, P.; Zhao, J.; Liu, J.; et al. Differential expressions of PD-1, PD-L1 and PD-L2 between primary and metastatic sites in renal cell carcinoma. BMC Cancer 2019, 19, 360. [Google Scholar] [CrossRef]
- Liu, C.; Li, X. Stage-Dependent Changes in Albumin, NLR, PLR, and AFR are Correlated with Shorter Survival in Patients with Gastric Cancer. Clin. Lab. 2019, 65, e190132. [Google Scholar] [CrossRef]
- Ding, X.; Zhang, W.; Li, S.; Yang, H. The role of cholesterol metabolism in cancer. Am. J. Cancer Res. 2019, 9, 219–227. [Google Scholar]
- Rojko, L.; Megyesfalvi, Z.; Czibula, E.; Reiniger, L.; Teglasi, V.; Szegedi, Z.; Szallasi, Z.; Dome, B.; Moldvay, J. Longitudinal analysis of complete blood count parameters in advanced-stage lung cancer patients. Thorac. Cancer 2020, 11, 3193–3204. [Google Scholar] [CrossRef]
- Faubert, B.; Solmonson, A.; DeBerardinis, R.J. Metabolic reprogramming and cancer progression. Science 2020, 368, eaaw5473. [Google Scholar] [CrossRef]
- Sylman, J.L.; Boyce, H.B.; Mitrugno, A.; Tormoen, G.W.; Thomas, I.C.; Wagner, T.H.; Lee, J.S.; Leppert, J.T.; McCarty, O.J.T.; Mallick, P. A Temporal Examination of Platelet Counts as a Predictor of Prognosis in Lung, Prostate, and Colon Cancer Patients. Sci. Rep. 2018, 8, 6564. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, H.; Jiang, J.; Cao, X.; Liu, Q. Early decrease in postoperative serum albumin predicts severe complications in patients with colorectal cancer after curative laparoscopic surgery. World J. Surg. Oncol. 2018, 16, 192. [Google Scholar] [CrossRef]
- Mair, M.J.; Pajenda, S.; Ilhan-Mutlu, A.; Steindl, A.; Kiesel, B.; Widhalm, G.; Dieckmann, K.; Feldmann, K.; Hainfellner, J.; Marosi, C.; et al. Soluble PD-L1 is associated with local and systemic inflammation markers in primary and secondary brain tumours. ESMO Open 2020, 5, e000863. [Google Scholar] [CrossRef] [PubMed]
- Hinterleitner, C.; Strahle, J.; Malenke, E.; Hinterleitner, M.; Henning, M.; Seehawer, M.; Bilich, T.; Heitmann, J.; Lutz, M.; Mattern, S.; et al. Platelet PD-L1 reflects collective intratumoral PD-L1 expression and predicts immunotherapy response in non-small cell lung cancer. Nat. Commun. 2021, 12, 7005. [Google Scholar] [CrossRef] [PubMed]
- Darga, E.P.; Dolce, E.M.; Fang, F.; Kidwell, K.M.; Gersch, C.L.; Kregel, S.; Thomas, D.G.; Gill, A.; Brown, M.E.; Gross, S.; et al. PD-L1 expression on circulating tumor cells and platelets in patients with metastatic breast cancer. PLoS ONE 2021, 16, e0260124. [Google Scholar] [CrossRef] [PubMed]
- Baranyai, Z.; Josa, V.; Toth, A.; Szilasi, Z.; Tihanyi, B.; Zarand, A.; Harsanyi, L.; Szallasi, Z. Paraneoplastic thrombocytosis in gastrointestinal cancer. Platelets 2016, 27, 269–275. [Google Scholar] [CrossRef]
- Herold, Z.; Herold, M.; Lohinszky, J.; Dank, M.; Somogyi, A. Personalized Indicator Thrombocytosis Shows Connection to Staging and Indicates Shorter Survival in Colorectal Cancer Patients with or without Type 2 Diabetes. Cancers 2020, 12, 556. [Google Scholar] [CrossRef]
- Yang, Q.; Feng, M.; Ma, X.; Li, H.; Xie, W. Gene expression profile comparison between colorectal cancer and adjacent normal tissues. Oncol. Lett. 2017, 14, 6071–6078. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | Average ± SD or No. of Obs. |
|---|---|
| Age (years) | 60.95 ± 10.99 |
| Male:female ratio | 24:13 (64.9%:35.1%) |
| Primary tumor resection 1 | 26 (70.3%) |
| AJCC staging [21] at the time of primary tumor removal surgery: | |
| 2 (5.4%) |
| 4 (10.8%) |
| 31 (83.8%) |
| Regional lymph node metastasis | 33 (89.2%) |
| Distant metastases: | |
| 31:6 (83.8%:16.2%) |
| |
| 4:22 (10.8%:59.5%) |
| 13 (35.1%) |
| 2 (5.4%) |
| 14 (37.8%) |
| 10 (27.0%) |
| 13 (35.1%) |
| 12 (32.4%) |
| 25 (67.6%) |
| 51.67 ± 44.66 |
| RAS (wild:mutant) 2 | 19:13 (51.4%:35.1%) |
| Location of the tumor [22] | |
| 28 (75.7%) |
| 9 (24.3%) |
| Final lineage of chemotherapy | |
| 14 (37.8%) |
| 10 (27.0%) |
| 13 (35.1%) |
| Medical history | |
| 6 (27.0%) |
| 24 (64.9%) |
| 5 (13.5%) |
| 4 (10.8%) |
| 4 (10.8%) |
| Parameter | Disease-Specific Survival | Progression-Free Survival | ||
|---|---|---|---|---|
| Age (years) | 0.3825 | 0.3284 | 0.8433 | 0.6069 |
| PD-1 (pg/mL) | 0.2499 | – | 0.1652 | – |
| PD-L1 (pg/mL) | – | 0.0932 | – | 0.0215 |
| Sex (male vs. female) | 0.3173 | 0.1289 | 0.1953 | 0.0598 |
| Sidedness (left-sided vs. right-sided) | 0.1544 | 0.3149 | 0.3324 | 0.4389 |
| Lineage of chemotherapy | ||||
| 0.5425 | 0.6244 | 0.4332 | 0.3344 |
| 0.4964 | 0.4270 | 0.3320 | 0.3635 |
| Type 2 diabetes mellitus (none vs. present) | 0.1435 | 0.0601 | 0.7066 | 0.2831 |
| Hypertension (none vs. present) | 0.4842 | 0.5690 | 0.4708 | 0.6070 |
| Platelet count (109/L) | 0.0210 | 0.0954 | 0.0074 | 0.0699 |
| Parameter | Disease-Specific Survival | Progression-Free Survival | ||
|---|---|---|---|---|
| Stratified Univariate Model p-Values: | ||||
| PD-1 | PD-L1 | PD-1 | PD-L1 | |
| Location of metastases: | ||||
| 0.0331 | 0.0211 | 0.3240 | 0.0253 |
| 0.0651 | 0.0461 | 0.1710 | 0.0063 |
| 0.1242 | 0.0154 | 0.4060 | 0.0163 |
| 0.4353 | 0.0076 | 0.8480 | 0.0539 |
| 0.0344 | 0.0033 | 0.1670 | 0.0047 |
| 0.1280 | 0.0096 | 0.4040 | 0.0329 |
| Patients with multiple metastatic sites (no vs. yes) | 0.3431 | 0.0011 | 0.7450 | 0.0020 |
| Primary tumor resection (no vs. yes) | 0.0224 | 0.0932 | 0.0625 | 0.0041 |
| RAS (wild vs. mutant) | 0.2800 | 0.0803 | 0.5350 | 0.0050 |
| Multivariate Model p-Values: | ||||
| PD-1 (pg/mL) | 0.1731 | – | 0.4018 | – |
| PD-L1 (pg/mL) | – | 0.0987 | – | 0.0058 |
| Location of metastases: | ||||
| 0.9128 | 0.4816 | 0.2072 | 0.7377 |
| 0.1594 | 0.2623 | 0.9651 | 0.7952 |
| 0.0081 | 0.0077 | 0.0077 | 0.0111 |
| 0.0146 | 0.0050 | 0.0312 | 0.0085 |
| 0.6798 | 0.8232 | 0.6379 | 0.3933 |
| Primary tumor resection (no vs. yes) | 0.0101 | 0.0488 | 0.1605 | 0.1825 |
| RAS (wild vs. mutant) | 0.9388 | 0.6880 | 0.3124 | 0.3753 |
| Parameter | <13 pg/mL (n = 19) | >13 pg/mL (n = 18) | Crude p-Value | Adjusted p-Value |
|---|---|---|---|---|
| Age (years) | 60.47 ± 12.70 | 61.45 ± 9.20 | 0.0000 | |
| PD-1 (pg/mL) | 25.12 ± 6.99 | 30.49 ± 15.40 | 0.6388 | |
| PD-L1 (pg/mL) | 8.77 ± 3.04 | 23.65 ± 10.97 | – | |
| White blood cell count (109/L) | 6.85 ± 196 | 9.24 ± 3.65 | 0.0322 | 0.1329 |
| Lymphocyte count (109/L) | 1.52 ± 0.51 | 1.81 ± 0.59 | 0.4380 | |
| Monocyte count (109/L) | 0.57 ± 0.15 | 0.77 ± 0.30 | 0.0432 | 0.1383 |
| Red blood cell count (1012/L) | 4.66 ± 0.44 | 4.67 ± 0.59 | 0.4380 | |
| Hemoglobin (g/L) | 134.79 ± 18.72 | 124.00 ± 17.89 | 0.3151 | |
| Hematocrit (L/L) | 0.40 ± 0.05 | 0.37 ± 0.05 | 0.0887 | 0.2027 |
| Mean corpuscular volume (fL) | 86.43 ± 6.48 | 83.98 ± 6.46 | 0.4380 | |
| Mean corpuscular hemoglobin (pg) | 28.93 ± 2.83 | 27.84 ± 2.99 | 0.4380 | |
| Mean corpuscular hemoglobin concentration (g/L) | 334.17 ± 10.49 | 330.86 ± 14.07 | 0.5216 | |
| Red blood cell distribution width (%) | 14.91 ± 2.54 | 16.01 ± 2.82 | 0.4737 | |
| Platelet count (109/L) | 257.05 ± 76.71 | 368.39 ± 163.97 | 0.0217 | 0.1257 |
| Aspartate transaminase (U/L) | 26.37 ± 10.28 | 65.50 ± 93.05 | 0.0225 | 0.1257 |
| Alanine transaminase (U/L) | 26.79 ± 17.16 | 44.94 ± 34.98 | 0.0635 | 0.1694 |
| Gamma-glutamyl transferase (U/L) | 72.79 ± 82.78 | 225.83 ± 243.04 | 0.0143 | 0.1257 |
| Lactate dehydrogenase (U/L) | 219.37 ± 66.61 | 943.22 ± 1517.84 | 0.0374 | 0.1329 |
| Alkaline phosphatase (U/L) | 110.68 ± 34.22 | 256.73 ± 245.55 | 0.4380 | |
| Plasma glucose (mmol/L) | 5.30 ± 0.82 | 5.21 ± 0.95 | 0.6717 | |
| Creatinine (µmol/L) | 68.26 ± 12.50 | 64.28 ± 18.12 | 0.4483 | |
| 94.01 ± 13.76 | 96.32 ± 17.59 | 0.4880 | ||
| Total cholesterol (mmol/L) | 5.32 ± 1.07 | 5.99 ± 2.05 | 0.4882 | |
| High-density lipoprotein cholesterol (mmol/L) | 1.42 ± 0.35 | 1.23 ± 0.31 | 0.3151 | |
| Low-density lipoprotein cholesterol (mmol/L) | 3.25 ± 0.76 | 3.90 ± 1.43 | 0.0780 | 0.1919 |
| Triglycerides (mmol/L) | 1.62 ± 0.77 | 1.56 ± 0.46 | 1.0000 | |
| Total protein (g/L) | 73.28 ± 4.21 | 72.88 ± 6.21 | 0.9075 | |
| Albumin (g/L) | 44.69 ± 2.75 | 40.83 ± 4.16 | 0.0138 | 0.1257 |
| High-sensitivity C-reactive protein (mg/L) | 7.01 ± 8.56 | 42.89 ± 57.19 | 0.0015 | 0.0478 |
| Thyroid stimulating hormone (mU/L) | 1.18 ± 0.87 | 1.88 ± 2.25 | 0.4882 | |
| Carcinoembryonic antigen (ng/mL) | 458.10 ± 1916.54 | 220.39 ± 425.38 | 0.0373 | 0.1329 |
| Carbohydrate antigen 19-9 (U/mL) | 266.59 ± 682.01 | 1602.17 ± 4813.00 | 0.4882 |
| Parameter | <26 pg/mL (n = 18) | >26 pg/mL (n = 19) | Crude p-Value | Adjusted p-Value |
|---|---|---|---|---|
| Age (years) | 59.88 ± 11.72 | 61.96 ± 10.48 | 0.8812 | |
| PD-1 (pg/mL) | 19.31 ± 5.21 | 35.71 ± 11.13 | – | |
| PD-L1 (pg/mL) | 16.39 ± 11.54 | 15.64 ± 10.51 | 0.8812 | |
| White blood cell count (109/L) | 8.16 ± 3.80 | 7.87 ± 2.39 | 0.8812 | |
| Lymphocyte count (109/L) | 1.60 ± 0.53 | 1.72 ± 0.59 | 0.8812 | |
| Monocyte count (109/L) | 0.72 ± 0.26 | 0.61 ± 0.23 | 0.5203 | |
| Red blood cell count (1012/L) | 4.41 ± 0.58 | 4.72 ± 0.42 | 0.4799 | |
| Hemoglobin (g/L) | 124.61 ± 19.69 | 134.21 ± 17.29 | 0.5203 | |
| Hematocrit (L/L) | 0.37 ± 0.05 | 0.40 ± 0.04 | 0.5203 | |
| Mean corpuscular volume (fL) | 84.76 ± 6.54 | 85.68 ± 6.61 | 0.8793 | |
| Mean corpuscular hemoglobin (pg) | 28.29 ± 2.89 | 28.50 ± 3.03 | 0.8812 | |
| Mean corpuscular hemoglobin concentration (g/L) | 333.27 ± 12.84 | 331.88 ± 12.08 | 0.8812 | |
| Red blood cell distribution width (%) | 15.41 ± 3.00 | 15.48 ± 2.63 | 0.8812 | |
| Platelet count (109/L) | 342.50 ± 176.18 | 281.58 ± 80.13 | 0.8793 | |
| Aspartate transaminase (U/L) | 59.72 ± 93.02 | 31.84 ± 22.31 | 0.0463 | 0.4242 |
| Alanine transaminase (U/L) | 43.00 ± 31.76 | 28.63 ± 23.68 | 0.5203 | |
| Gamma-glutamyl transferase (U/L) | 144.83 ± 149.40 | 149.53 ± 231.46 | 0.8793 | |
| Lactate dehydrogenase (U/L) | 724.50 ± 1415.71 | 426.58 ± 714.76 | 0.8793 | |
| Alkaline phosphatase (U/L) | 200.12 ± 215.17 | 150.12 ± 132.75 | 0.8793 | |
| Plasma glucose (mmol/L) | 4.97 ± 0.79 | 5.55 ± 0.86 | 0.4799 | |
| Creatinine (µmol/L) | 66.83 ± 17.47 | 65.84 ± 13.63 | 0.8812 | |
| 96.10 ± 17.15 | 94.21 ± 14.31 | 0.8793 | ||
| Total cholesterol (mmol/L) | 5.38 ± 1.23 | 5.90 ± 1.94 | 0.8735 | |
| High-density lipoprotein cholesterol (mmol/L) | 1.29 ± 0.35 | 1.37 ± 0.34 | 0.8793 | |
| Low-density lipoprotein cholesterol (mmol/L) | 3.46 ± 1.05 | 3.68 ± 1.28 | 0.8793 | |
| Triglycerides (mmol/L) | 1.47 ± 0.58 | 1.71 ± 0.66 | 0.8735 | |
| Total protein (g/L) | 71.53 ± 6.07 | 74.57 ± 3.83 | 0.0499 | 0.4242 |
| Albumin (g/L) | 41.44 ± 3.68 | 44.12 ± 3.88 | 0.0417 | 0.4242 |
| High-sensitivity C-reactive protein (mg/L) | 33.49 ± 58.18 | 15.92 ± 21.63 | 0.8793 | |
| Thyroid stimulating hormone (mU/L) | 1.83 ± 2.27 | 1.23 ± 0.85 | 0.8793 | |
| Carcinoembryonic antigen (ng/mL) | 555.18 ± 1961.43 | 140.93 ± 389.14 | 0.8812 | |
| Carbohydrate antigen 19-9 (U/mL) | 1440.29 ± 4841.00 | 419.94 ± 768.91 | 0.9757 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dank, M.; Mühl, D.; Herold, M.; Hornyák, L.; Szasz, A.M.; Herold, Z. Does Elevated Pre-Treatment Plasma PD-L1 Level Indicate an Increased Tumor Burden and Worse Prognosis in Metastatic Colorectal Cancer? J. Clin. Med. 2022, 11, 4815. https://doi.org/10.3390/jcm11164815
Dank M, Mühl D, Herold M, Hornyák L, Szasz AM, Herold Z. Does Elevated Pre-Treatment Plasma PD-L1 Level Indicate an Increased Tumor Burden and Worse Prognosis in Metastatic Colorectal Cancer? Journal of Clinical Medicine. 2022; 11(16):4815. https://doi.org/10.3390/jcm11164815
Chicago/Turabian StyleDank, Magdolna, Dorottya Mühl, Magdolna Herold, Lilla Hornyák, Attila Marcell Szasz, and Zoltan Herold. 2022. "Does Elevated Pre-Treatment Plasma PD-L1 Level Indicate an Increased Tumor Burden and Worse Prognosis in Metastatic Colorectal Cancer?" Journal of Clinical Medicine 11, no. 16: 4815. https://doi.org/10.3390/jcm11164815