
Pandemic Preparedness: Maintaining Adequate Immune Fitness by Attaining a Normal, Healthy Body Weight

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Filindassi, V.; Pedrini, C.; Sabadini, C.; Duradoni, M.; Guazzini, A. Impact of COVID-19 First Wave on Psychological and Psychosocial Dimensions: A Systematic Review. COVID 2022, 2, 273–340. [Google Scholar] [CrossRef]
- Guazzini, A.; Pesce, A.; Marotta, L.; Duradoni, M. Through the Second Wave: Analysis of the Psychological and Perceptive Changes in the Italian Population during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1635. [Google Scholar] [CrossRef] [PubMed]
- Vishwakarma, S.; Panigrahi, C.; Barua, S.; Sahoo, M.; Mandliya, S. Food nutrients as inherent sources of immunomodulation during COVID-19 pandemic. Lebensm. Wiss. Technol. 2022, 158, 113154. [Google Scholar] [CrossRef]
- Filgueira, T.O.; Castoldi, A.; Santos, L.E.R.; de Amorim, G.J.; de Fernandes, M.S.S.; Anastácio, W.; Campos, E.Z.; Santos, T.M.; Souto, F.O. The relevance of a physical active lifestyle and physical fitness on immune defense: Mitigating disease burden, with focus on COVID-19 consequences. Front. Immunol. 2021, 12, 587146. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, N.; van der Werf, Y.D.; van der Holst, H.M. The importance of sleep and circadian rhythms for vaccination success and susceptibility to viral infections. Clocks Sleep 2022, 4, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Kiani, P.; Balikji, J.; Kraneveld, A.D.; Garssen, J.; Bruce, G.; Verster, J.C. Pandemic Preparedness: The Importance of Adequate Immune Fitness. J. Clin. Med. 2022, 11, 2442. [Google Scholar] [CrossRef]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe COVID-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- De Lusignan, S.; Dorward, J.; Correa, A.; Jones, N.; Akinyemi, O.; Amirthalingam, G.; Andrews, N.; Byford, R.; Dabrera, G.; Elliot, A.; et al. Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of general practitioners research and surveillance Centre primary care network: A cross-sectional study. Lancet Infect. Dis. 2020, 20, 1034–1042. [Google Scholar] [CrossRef]
- Intensive Care National Audit & Research Centre (ICNARC). Report on COVID-19. 2022. Available online: https://www.icnarc.org/our-audit/audits/cmp/reports (accessed on 8 June 2022).
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M. High prevalence of obesity in severe acute respiratory syndrome Coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Chen, F.; Wang, T.; Luo, F.; Liu, X.; Wu, Q.; He, Q.; Wang, Z.; Liu, Y.; Liu, L.; et al. Obesity and COVID-19 severity in a designated Hospital in Shenzhen, China. Diabetes Care 2020, 43, 1392–1398. [Google Scholar] [CrossRef] [PubMed]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in patients younger than 60 years is a risk factor for COVID-19 hospital admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [Green Version]
- Kompaniyets, L.; Goodman, A.B.; Belay, B.; Freedman, D.S.; Sucosky, M.S.; Lange, S.J.; Gundlapalli, A.V.; Boehmer, T.K.; Blanck, H.M. Body Mass Index and Risk for COVID-19–Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death—United States, March–December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 355–361. [Google Scholar] [CrossRef]
- Zhang, X.; Lewis, A.M.; Moley, J.R.; Brestoff, J.R. A systematic review and meta-analysis of obesity and COVID-19 outcomes. Sci. Rep. 2021, 11, 7193. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (COVID-19). Diabetes Metab. Res. Rev. 2021, 37, e3377. [Google Scholar] [CrossRef]
- Giacomelli, A.; Ridolfo, A.L.; Milazzo, L.; Oreni, L.; Bernacchia, D.; Siano, M.; Bonazzetti, C.; Covizzi, A.; Schiuma, M.; Passerini, M.; et al. 30-day mortality in patients hospitalized with COVID-19 during the first wave of the Italian epidemic: A prospective cohort study. Pharmacol. Res. 2020, 158, 104931. [Google Scholar] [CrossRef]
- Palaiodimos, L.; Kokkinidis, D.G.; Li, W.; Karamanis, D.; Ognibene, J.; Arora, S.; Southern, W.N.; Mantzoros, C.S. Severe obesity, increasing age and male sex are independently associated with worse in- hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 2020, 108, 154262. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 7 June 2020).
- Verhaegen, A.A.; Van Gaal, L.F. Drugs that Affect Body Weight, Body Fat Distribution, and Metabolism. In Endotext; Feingold, K.R., Ed.; MDText.com, Inc.: Portland, OR, USA, 2019. [Google Scholar]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- Karatzi, K.; Poulia, K.-A.; Papakonstantinou, E.; Zampelas, A. The impact of nutritional and lifestyle changes on body weight, body composition and cardiometabolic risk factors in children and adolescents during the pandemic of COVID-19: A systematic review. Children 2021, 8, 1130. [Google Scholar] [CrossRef]
- Huang, C.J.; Zourdos, M.C.; Jo, E.; Ormsbee, M.J. Influence of physical activity and nutrition on obesity-related immune function. Sci. World J. 2013, 2013, 752071. [Google Scholar] [CrossRef] [PubMed]
- Quetelet, A.A. Treatise on Man and the Development of His Faculties; Burt Franklin: New York, NY, USA, 2005. [Google Scholar]
- Keys, A.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; Taylor, H.L. Indices of relative weight and adiposity. J. Chronic Dis. 1972, 25, 329–343. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Organization BMI Classification. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 1 November 2020).
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Observatory Data Repository. Overweight/Obesity. 2017. Available online: https://apps.who.int/gho/data/node.main.A896?lang=en (accessed on 8 June 2022).
- Talbot, H.; Coleman, L.; Crimin, K.; Zhu, Y.; Rock, M.; Meece, J.; Shay, D.; Belongia, E.; Griffin, M. Association between obesity and vulnerability and serologic response to influenza vaccination in older adults. Vaccine 2012, 30, 3937–3943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frydrych, L.M.; Bian, G.; O’Lone, D.E.; Ward, P.A.; Delano, M. Obesity and type 2 diabetes mellitus drive immune dysfunction, infection development, and sepsis mortality. J. Leukoc. Biol. 2018, 104, 525–534. [Google Scholar] [CrossRef]
- Dixon, A.E.; Peters, U. The effect of obesity on lung function. Expert Rev. Respir. Med. 2018, 12, 755–767. [Google Scholar] [CrossRef]
- Watanabe, M.; Caruso, D.; Tuccinardi, D.; Risi, R.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Tarallo, M.; Strigari, L.; Manfrini, S.; et al. Visceral fat shows the strongest association with the need of intensive Care in Patients with COVID-19. Metab. Clin. Exp. 2020, 111, 154319. [Google Scholar] [CrossRef]
- Yang, Y.; Ding, L.; Zou, X.; Shen, Y.; Hu, D.; Hu, X.; Li, Z.; Kamel, I.R. Visceral adiposity and high intramuscular fat deposition independently predict critical illness in patients with Sars-CoV-2. Obesity 2020, 28, 2040–2048. [Google Scholar] [CrossRef]
- De Frel, D.L.; Atsma, D.E.; Pijl, H.; Seidell, J.C.; Leenen, P.J.M.; Dik, W.A.; van Rossum, E.F.C. The impact of obesity and lifestyle on the immune system and susceptibility to infections such as COVID-19. Front. Nutr. 2020, 7, 597600. [Google Scholar] [CrossRef]
- Lavská, S.; Horváthová, M.; Szabová, M.; Nemessányi, T.; Jahnová, E.; Tulinská, J.; Líšková, A.; Wsolová, L.; Staruchová, M.; Volkovová, K. Association between the human immune response and body mass index. Hum. Immunol. 2012, 73, 480–485. [Google Scholar] [CrossRef]
- Yu, J.-Y.; Choi, W.-J.; Lee, H.-S.; Lee, J.-W. Relationship between inflammatory markers and visceral obesity in obese and overweight Korean adults. Medicine 2019, 98, e14740. [Google Scholar] [CrossRef] [PubMed]
- Otten, L.; De Kruijff, D.; Mackus, M.; Garssen, J.; Verster, J. Attention Deficit Hyperactivity Disorder (ADHD) and the dietary intake of fiber and fats. Eur. Neuropsychopharmacol. 2016, 26, S726. [Google Scholar] [CrossRef]
- Mackus, M.; de Kruijff, D.; Otten, L.S.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Differential gender effects in the relationship between perceived immune functioning and autism spectrum disorder scores. Int. J. Environ. Res. Public Health 2017, 14, E409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernstrand, A.M.; Bury, D.; Garssen, J.; Verster, J.C. Dietary intake of fibers: Differential effects in men and women on general health and perceived immune functioning. Food Nutr. Res. 2017, 61, 1297053. [Google Scholar] [CrossRef] [Green Version]
- Becht, N.N.; Hoepel, S.J.W.; Garssen, J.; Verster, J.C. Perceived immune fitness, depression, and dietary zinc intake. In Proceedings of the Poster presented at ECNP Congress, Vienna, Austria, 15–18 October 2022. [Google Scholar]
- Van Lantman, M.S.; Otten, L.S.; Mackus, M.; de Kruijff, D.; van de Loo, A.J.A.E.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Mental resilience, perceived immune functioning, and health. J. Multidiscip. Healthc. 2017, 10, 107–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huls, H.; Abdulahad, S.; Mackus, M.; Van de Loo, A.J.A.E.; Roehrs, T.; Roth, T.; Verster, J.C. Inclusion and Exclusion Criteria of Clinical Trials for Insomnia. J. Clin. Med. 2018, 7, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baars, T.; Berge, A.C.; Garssen, J.; Verster, J.C. Effect of raw milk consumption on perceived health, mood and immune functioning among US adults with a poor and normal health: A retrospective questionnaire based study. Complement. Ther. Med. 2019, 47, 102196. [Google Scholar] [CrossRef]
- Baars, T.; Berge, C.; Garssen, J.; Verster, J. The impact of raw fermented milk products on perceived health and mood among Dutch adults. Nutr. Food Sci. 2019, 49, 1195–1206. [Google Scholar] [CrossRef]
- Sulzer, T.A.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Early life exposome pressure on later life immune fitness: A layman’s perspective. Eur. Neuropsychopharmacol. 2019, 29, S204–S205. [Google Scholar] [CrossRef]
- Van de Loo, A.J.A.E.; Kerssemakers, N.; Scholey, A.; Garssen, J.; Kraneveld, A.D.; Verster, J.C. Perceived immune fitness, individual strength, and hangover severity. Int. J. Environ. Res. Public Health 2020, 17, 4039. [Google Scholar] [CrossRef]
- Verster, J.; Arnoldy, L.; van de Loo, A.; Kraneveld, A.; Garssen, J.; Scholey, A. The Impact of Having a Holiday or Work in Fiji on Perceived Immune Fitness. Tour. Hosp. 2021, 2, 95–112. [Google Scholar] [CrossRef]
- Kiani, P.; Merlo, A.; Saeed, H.; Benson, S.; Bruce, G.; Hoorn, R.; Kraneveld, A.; van de Loo, A.; Severeijns, N.; Sips, A.; et al. Immune fitness, and the psychosocial and health consequences of the COVID-19 pandemic lockdown in The Netherlands: Methodology and design of the CLOFIT study. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 199–218. [Google Scholar] [CrossRef] [PubMed]
- Versprille, L.J.F.; van de Loo, A.J.A.E.; Mackus, M.; Arnoldy, L.; Sulzer, T.A.L.; Vermeulen, S.A.; Abdulahad, S.; Huls, H.; Baars, T.; Kraneveld, A.D.; et al. Development and validation of the Immune Status Questionnaire (ISQ). Int. J. Environ. Res. Public Health 2019, 16, E4743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, I. Chi-squared and Fisher-Irwin tests of two-by-two tables with small sample recommendations. Stat. Med. 2007, 26, 3661–3675. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.T.E. The analysis of 2 × 2 contingency tables—Yet again. Stat. Med. 2011, 30, 890. [Google Scholar] [CrossRef]
- Merlo, A.; Severeijns, N.R.; Benson, S.; Scholey, A.; Garssen, J.; Bruce, G.; Verster, J.C. Mood and changes in alcohol consumption in young adults during COVID-19 lockdown: A model explaining associations with perceived immune fitness and experiencing COVID-19 symptoms. Int. J. Environ. Res. Public Health 2021, 18, 10028. [Google Scholar] [CrossRef]
- Merlo, A.; Hendriksen, P.A.; Severeijns, N.R.; Garssen, J.; Bruce, G.; Verster, J.C. Alcohol consumption patterns during COVID-19 lockdown and their relationship with perceived immune fitness and reported COVID-19 symptoms. Healthcare 2021, 9, 1039. [Google Scholar] [CrossRef]
- Merlo, A.; Severeijns, N.R.; Hendriksen, P.A.; Benson, S.; Scholey, A.; Garssen, J.; Bruce, G.; Verster, J.C. Alcohol consumption on the heaviest drinking occasion and hangovers during the first Dutch COVID-19 lockdown. Int. J. Environ. Res. Public Health 2022, 19, 4301. [Google Scholar] [CrossRef]
- Dutra, P.M.L.; Da-Silva, S.A.G.; Mineo, J.R.; Turner, J.E. Editorial: The effects of physical activity and exercise on immune responses to infection. Front. Immunol. 2022, 13, 842568. [Google Scholar] [CrossRef]
- Morey, J.N.; Boggero, I.A.; Scott, A.B.; Segerstrom, S.C. Current directions in stress and human immune function. Curr. Opin. Psychol. 2015, 5, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Gouin, J.P. Chronic stress, immune dysregulation, and health. Am. J. Lifestyle Med. 2011, 5, 476–485. [Google Scholar] [CrossRef]
- Qiu, F.; Liang, C.L.; Liu, H.; Zeng, Y.Q.; Hou, S.; Huang, S.; Lai, X.; Dai, Z. Impacts of cigarette smoking on immune responsiveness: Up and down or upside down? Oncotarget 2017, 8, 268–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minihane, A.M.; Vinoy, S.; Russell, W.R.; Baka, A.; Roche, H.M.; Tuohy, K.M.; Teeling, J.L.; Blaak, E.E.; Fenech, M.; Vauzour, D.; et al. Low-grade inflammation, diet composition and health: Current research evidence and its translation. Br. J. Nutr. 2015, 114, 999–1012. [Google Scholar] [CrossRef] [Green Version]
- Bujtor, M. Can dietary intake protect against low-grade inflammation in children and adolescents? Brain Behav. Immun. Health 2021, 18, 100369. [Google Scholar] [CrossRef] [PubMed]
- Antwi, J.; Appiah, B.; Oluwakuse, B.; Abu, B.A.Z. The Nutrition-COVID-19 interplay: A review. Curr. Nutr. Rep. 2021, 10, 364–374. [Google Scholar] [CrossRef]
- Suardi, C.; Cazzaniga, E.; Graci, S.; Dongo, D.; Palestini, P. Link between viral Iifections, immune system, inflammation and diet. Int. J. Environ. Res. Public Health 2021, 18, 2455. [Google Scholar] [CrossRef]
- Martinez-Ferran, M.; De La Guía-Galipienso, F.; Sanchis-Gomar, F.; Pareja-Galeano, H. Metabolic impacts of confinement during the COVID-19 pandemic due to modified diet and physical activity habits. Nutrients 2020, 12, 1549. [Google Scholar] [CrossRef]
- McMillan, L.; Owen, L.; Kras, M.; Scholey, A. Behavioural effects of a 10-day Mediterranean diet. Results from a pilot study evaluating mood and cognitive performance. Appetite 2011, 56, 143–147. [Google Scholar] [CrossRef]
- Martinez-Lacoba, R.; Pardo-Garcia, I.; Amo-Saus, E.; Escribano-Sotos, F. Mediterranean diet and health outcomes: A systematic meta-review. Eur. J. Public Health 2018, 28, 955–961. [Google Scholar] [CrossRef] [Green Version]
- Da Scheffer, D.; Latini, A. Exercise-induced immune system response: Antiinflammatory status on peripheral and central organs. Biochim. Biophys. Acta 2020, 1866, 165823. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
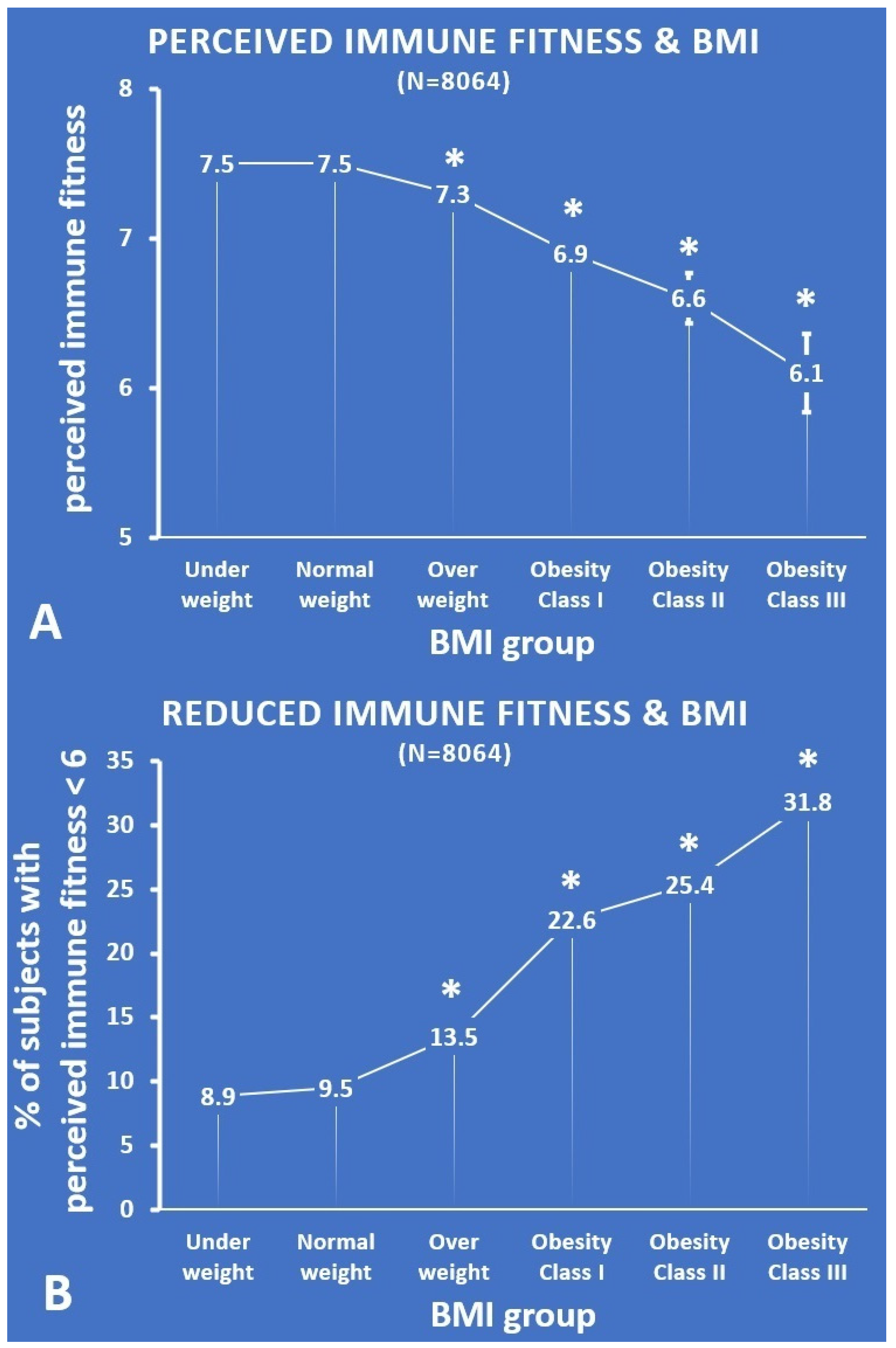
| BMI Group | Under Weight | Normal Weight | Over Weight | Obesity Class I | Obesity Class II | Obesity Class III |
|---|---|---|---|---|---|---|
| N | 361 | 5398 | 1622 | 475 | 142 | 66 |
| Mean (SD) | 7.5 (1.5) | 7.5 (1.5) | 7.3 (1.7) * | 6.9 (2.2) * | 6.6 (2.0) * | 6.1 (2.1) * |
| % < 6 | 8.9 | 9.5 | 13.5 * | 22.6 * | 25.4 * | 31.8 * |
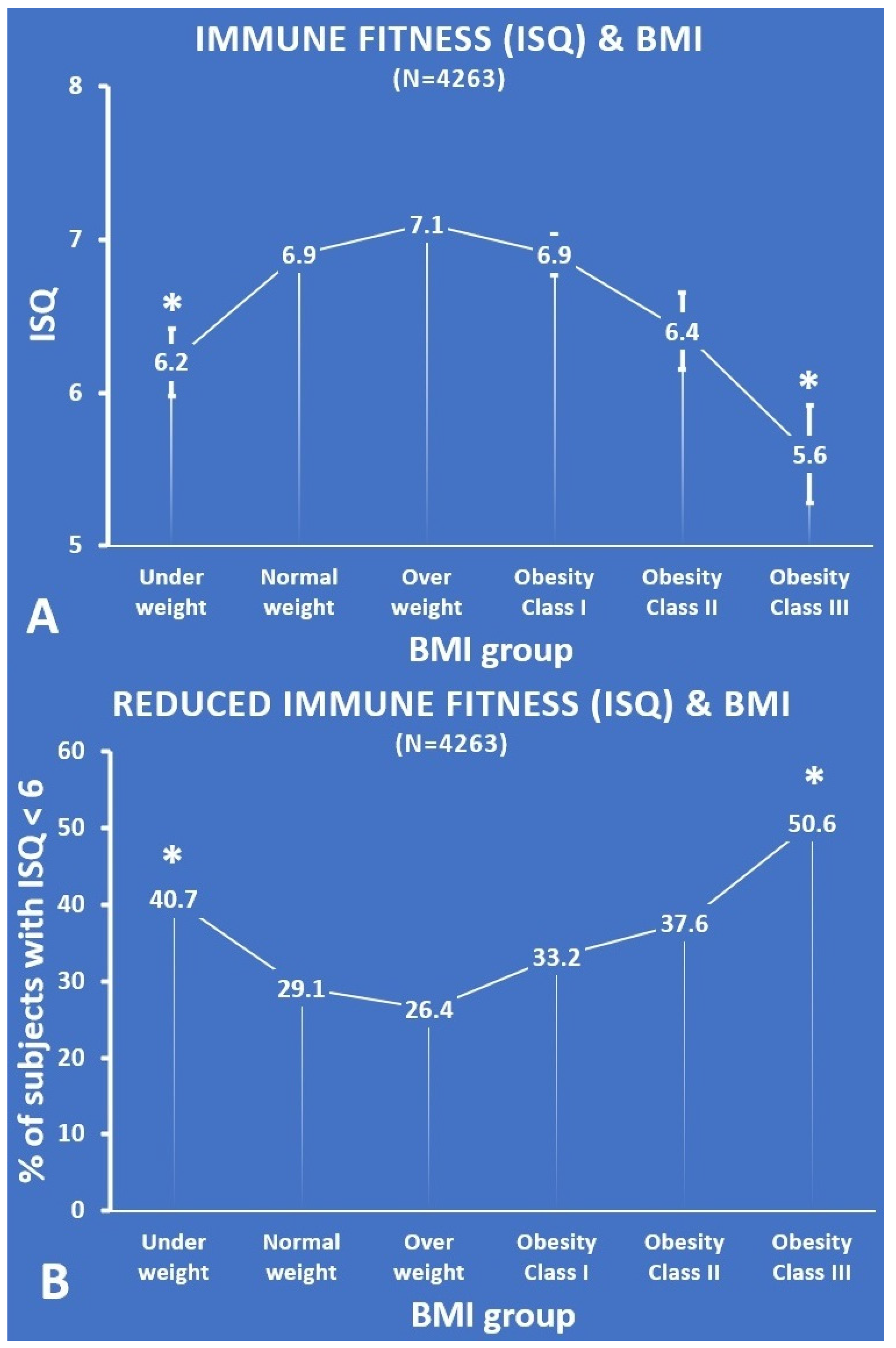
| BMI Group | Under Weight | Normal Weight | Over Weight | Obesity Class I | Obesity Class II | Obesity Class III |
|---|---|---|---|---|---|---|
| N | 130 | 2259 | 1233 | 434 | 138 | 69 |
| Mean (SD) ISQ | 6.2 (2.5) * | 6.9 (2.5) | 7.1 (2.5) * | 6.9 (2.7) | 6.4 (2.9) | 5.6 (2.7) * |
| % < 6 | 40.7 * | 29.1 | 26.4 | 33.2 | 37.6 | 50.6 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiani, P.; Mulder, K.E.W.; Balikji, J.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Pandemic Preparedness: Maintaining Adequate Immune Fitness by Attaining a Normal, Healthy Body Weight. J. Clin. Med. 2022, 11, 3933. https://doi.org/10.3390/jcm11143933
Kiani P, Mulder KEW, Balikji J, Kraneveld AD, Garssen J, Verster JC. Pandemic Preparedness: Maintaining Adequate Immune Fitness by Attaining a Normal, Healthy Body Weight. Journal of Clinical Medicine. 2022; 11(14):3933. https://doi.org/10.3390/jcm11143933
Chicago/Turabian StyleKiani, Pantea, Kiki E. W. Mulder, Jessica Balikji, Aletta D. Kraneveld, Johan Garssen, and Joris C. Verster. 2022. "Pandemic Preparedness: Maintaining Adequate Immune Fitness by Attaining a Normal, Healthy Body Weight" Journal of Clinical Medicine 11, no. 14: 3933. https://doi.org/10.3390/jcm11143933