Gut Microbiome Modification through Dietary Intervention in Patients with Colorectal Cancer: Protocol for a Prospective, Interventional, Controlled, Randomized Clinical Trial in Patients with Scheduled Surgical Intervention for CRC

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Objectives
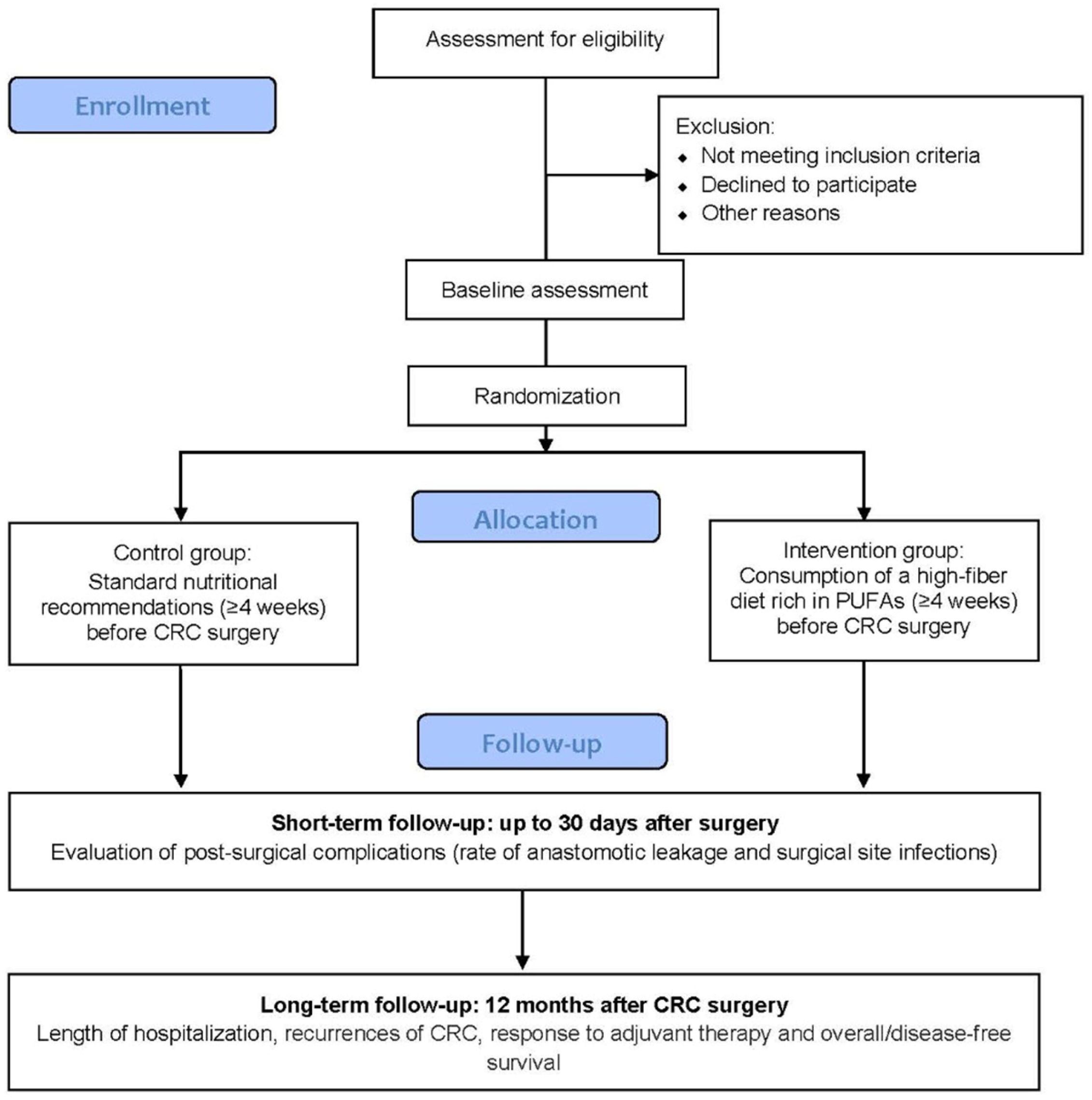
- To determine the change in the gut and intra-tumoral microbiome composition, fecal and serum levels of short-chain fatty acids (SCFAs), and serum inflammation, endotoxemia, and intestinal permeability markers in CRC patients following a high-fiber diet rich in PUFAs in the preoperative phase, in comparison to the control group.
- To evaluate the rate of anastomotic dehiscence and surgical site infections after surgery (30 days of follow-up) in the intervention group, in comparison to the control group.
- To establish the length of hospitalization, recurrences of CRC, response to adjuvant therapy, and overall and disease-free survival after surgery (1 year of follow-up) in the intervention group, in comparison to the control group.
2.2. Study Design
2.3. Study Setting
2.4. Eligibility Criteria
2.4.1. Inclusion Criteria
- Age between 18–80 years old;
- After the clinical diagnosis of CRC (stage I–III), the doctor has recommended and arranged for CRC surgery.
2.4.2. Exclusion Criteria
- Clinical diagnosis of stage IV CRC;
- Current gastrointestinal illness other than gastroesophageal reflux disease or hemorrhoids;
- Chronic liver or kidney disease;
- History of cardiac disease;
- Positive genetic test for inherited polyposis syndromes (such as familial adenomatous polyps, hereditary non-polyposis colon cancer syndromes, etc.);
- Alcoholism or illicit drug use;
- Antibiotic use within the past 2 months;
- Dietary supplement use including pre- or probiotics within the past month;
- History of intestinal cancer, inflammatory bowel disease, celiac disease, or malabsorptive bariatric surgery;
- Inflammatory or connective tissue disease (such as lupus, scleroderma, rheumatoid arthritis, etc.).
2.5. Consent
2.6. Research Ethics Approval
2.7. Protocol Amendments
2.8. Intervention
2.9. Outcomes
2.10. Participant Timeline
2.11. Sample Size and Recruitment
2.12. Randomization and Blinding
2.13. Data and Sample Collection and Analysis of Variables
2.13.1. Data Collection
2.13.2. Sample Collection and Storage
2.13.3. Analysis of Gut and Intra-Tumoral Microbiota Composition
2.13.4. Analysis of Intestinal Permeability
2.13.5. Determination of Endotoxemia Markers
2.13.6. Determination of Inflammatory Markers
2.13.7. Analysis of SCFAs in Fecal Samples by Gas Chromatography (GC) Coupled with a Flame-Ionization Detector
2.13.8. Analysis of Plasma SCFA Levels by Ultra-High Performance Liquid Chromatography Tandem Mass Spectrometry (UHPLC-MS/MS)
2.13.9. Assessment of Postoperative Follow-Up and Recovery
2.14. Data Management
2.15. Statistical Methods
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hooper, L.V. Bacterial contributions to mammalian gut development. Trends Microbiol. 2004, 12, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.A.; Gahan, C.G. The gut microbiota and the metabolic health of the host. Curr. Opin. Gastroenterol. 2014, 30, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Pedersen, O. Gut microbiota in human metabolic health and disease. Nat. Rev. Microbiol 2021, 19, 55–71. [Google Scholar] [CrossRef] [PubMed]
- Koliarakis, I.; Messaritakis, I.; Nikolouzakis, T.K.; Hamilos, G.; Souglakos, J.; Tsiaoussis, J. Oral bacteria and intestinal dysbiosis in colorectal cancer. Int. J. Mol. Sci. 2019, 20, 4146. [Google Scholar] [CrossRef] [Green Version]
- Durack, J.; Lynch, S.V. The gut microbiome: Relationships with disease and opportunities for therapy. J. Exp. Med. 2019, 216, 20–40. [Google Scholar] [CrossRef] [Green Version]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef]
- Feng, Q.; Liang, S.; Jia, H.; Stadlmayr, A.; Tang, L.; Lan, Z.; Zhang, D.; Xia, H.; Xu, X.; Jie, Z.; et al. Gut microbiome development along the colorectal adenoma-carcinoma sequence. Nat. Commun. 2015, 6, 6528. [Google Scholar] [CrossRef] [Green Version]
- Castellarin, M.; Warren, R.L.; Freeman, J.D.; Dreolini, L.; Krzywinski, M.; Strauss, J.; Barnes, R.; Watson, P.; Allen-Vercoe, E.; Moore, R.A.; et al. Fusobacterium nucleatum infection is prevalent in human colorectal carcinoma. Genome Res. 2012, 22, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Fukuda, M.; Komiyama, Y.; Mitsuyama, K.; Andoh, A.; Aoyama, T.; Matsumoto, Y.; Kanauchi, O. Prebiotic treatment reduced preneoplastic lesions through the downregulation of toll like receptor 4 in a chemo-induced carcinogenic model. J. Clin. Biochem. Nutr. 2011, 49, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Wirbel, J.; Pyl, P.T.; Kartal, E.; Zych, K.; Kashani, A.; Milanese, A.; Fleck, J.S.; Voigt, A.Y.; Palleja, A.; Ponnudurai, R.; et al. Meta-analysis of fecal metagenomes reveals global microbial signatures that are specific for colorectal cancer. Nat. Med. 2019, 25, 679–689. [Google Scholar] [CrossRef] [Green Version]
- Argiles, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol 2020, 31, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, J.E.; Schumacher, J.; Kent, K.C.; Heise, C.P.; Greenberg, C.C. Associations of Specific Postoperative Complications with Outcomes After Elective Colon Resection: A Procedure-Targeted Approach Toward Surgical Quality Improvement. JAMA Surg. 2017, 152, e164681. [Google Scholar] [CrossRef] [PubMed]
- Ohigashi, S.; Sudo, K.; Kobayashi, D.; Takahashi, T.; Nomoto, K.; Onodera, H. Significant changes in the intestinal environment after surgery in patients with colorectal cancer. J. Gastrointest. Surg. 2013, 17, 1657–1664. [Google Scholar] [CrossRef] [PubMed]
- Alam, A.; Neish, A. Role of gut microbiota in intestinal wound healing and barrier function. Tissue Barriers 2018, 6, 1539595. [Google Scholar] [CrossRef] [PubMed]
- Veettil, S.K.; Wong, T.Y.; Loo, Y.S.; Playdon, M.C.; Lai, N.M.; Giovannucci, E.L.; Chaiyakunapruk, N. Role of Diet in Colorectal Cancer Incidence: Umbrella Review of Meta-analyses of Prospective Observational Studies. JAMA Netw. Open 2021, 4, e2037341. [Google Scholar] [CrossRef]
- Scheppach, W. Effects of short chain fatty acids on gut morphology and function. Gut 1994, 35, S35–S38. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.S.; Nishihara, R.; Cao, Y.; Song, M.; Mima, K.; Qian, Z.R.; Nowak, J.A.; Kosumi, K.; Hamada, T.; Masugi, Y.; et al. Association of Dietary Patterns with Risk of Colorectal Cancer Subtypes Classified by Fusobacterium nucleatum in Tumor Tissue. JAMA Oncol. 2017, 3, 921–927. [Google Scholar] [CrossRef] [Green Version]
- Costantini, L.; Molinari, R.; Farinon, B.; Merendino, N. Impact of Omega-3 Fatty Acids on the Gut Microbiota. Int. J. Mol. Sci. 2017, 18, 2645. [Google Scholar] [CrossRef] [Green Version]
- Parolini, C. Effects of fish n-3 PUFAs on intestinal microbiota and immune system. Mar. Drugs 2019, 17, 374. [Google Scholar] [CrossRef] [Green Version]
- Watson, H.; Mitra, S.; Croden, F.C.; Taylor, M.; Wood, H.M.; Perry, S.L.; Spencer, J.A.; Quirke, P.; Toogood, G.J.; Lawton, C.L.; et al. A randomized trial of the effect of omega-3 polyunsaturated fatty acid supplements on the human intestinal microbiota. Gut 2018, 67, 1974–1983. [Google Scholar] [CrossRef]
- Zazpe, I.; Santiago, S.; de la Fuente-Arrillaga, C.; Núñez-Cordoba, J.M.; Bes-Rastrollo, M.; Martínez-González, M.A. Paper-Based versus web-based versions of self-administered questionnaires, including food frequency questionnaires: Prospective cohort study. JMIR Public Health Surveill. 2019, 5, e11997. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Alcoholado, L.; Laborda-Illanes, A.; Otero, A.; Ordoñez, R.; Gonzalez-Gonzalez, A.; Plaza-Andrades, I.; Ramos-Molina, B.; Gomez-Millan, J.; Queipo-Ortuño, M.I. Relationships of gut microbiota composition, short-chain fatty acids and polyamines with the pathological response to neoadjuvant radiochemotherapy in colorectal patients. Int. J. Mol. Sci. 2021, 22, 9549. [Google Scholar] [CrossRef] [PubMed]
- Fritsch, J.; Garces, L.; Quintero, M.A.; Pignac-Kobinger, J.; Santander, A.M.; Fernández, I.; Ban, Y.J.; Kwon, D.; Phillips, M.C.; Knight, K.; et al. Low-fat, high-fiber diet reduces markers of inflammation and dysbiosis and improves quality of life in patients with ulcerative colitis. Clin. Gastroenterol. Hepatol. 2021, 19, 1189–1199.e30. [Google Scholar] [CrossRef]
- Biruete, A.; Cross, T.W.L.; Allen, J.M.; Kistler, B.M.; de Loor, H.; Evenepoel, P.; Fahey, G.C., Jr.; Bauer, L.; Swanson, K.S.; Wilund, K.R. Effect of dietary inulin supplementation on the gut microbiota composition and derived metabolites of individual undergoing hemodialysis: A pilot study. J. Ren. Nutr. 2021, 31, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, L.; Spencer, S.P.; Perelman, D.; Van Treuren, W.; Han, S.; Yu, F.B.; Sonnenburg, E.D.; Fischbach, M.A.; Meyer, T.W.; Sonnenburg, J.L. Impact of a 7-day homogeneous diet on interpersonal variation in human gut microbiomes and metabolomes. Cell Host Microbe 2022, 30, 863–874.e4. [Google Scholar] [CrossRef]
- Vetrani, C.; Maukonen, J.; Bozzeto, L.; Della Pepa, G.; Vitale, M.; Costabile, G.; Riccardi, G.; Albarosa Rivellese, A.; Saarela, M.; Annuzzi, G. Diets naturally rich in polyphenols and/or long-chain n-3 polyunsaturate fatty acids differently affect microbiota composition in high-cardiometabolic-risk individuals. Acta Diabetol. 2020, 57, 853–860. [Google Scholar] [CrossRef]
- Kjølbæk, L.; Benítez-Páez, A.; Gómez Del Pulgar, E.M.; Brahe, L.K.; Liebisch, G.; Matysik, S.; Rampelli, S.; Vermeiren, J.; Brigidi, P.; Larsen, L.H.; et al. Arabinoxylan oligosaccharides and polyunsaturated fatty acid effects on gut microbiota and metabolic markers in overweight individuals with signs of metabolic syndrome: A randomized cross-over trial. Clin. Nutr. 2020, 39, 67–79. [Google Scholar] [CrossRef]


{kind=link}
| STUDY PERIOD | |||||||
|---|---|---|---|---|---|---|---|
| Enrolment | Allocation | Post-Allocation | Close-Out | ||||
| TIMEPOINT | t−1 | t0 | t1 | t2 | t3 | t4 | t5 |
| ENROLLMENT: | |||||||
| Eligibility screen | X | ||||||
| Informed consent | X | ||||||
| Inclusion criteria | X | ||||||
| Exclusion criteria | X | ||||||
| Allocation | X | ||||||
| INTERVENTIONS: | |||||||
| High-fiber diet rich in PUFAs | X | X | |||||
| Standard nutritional recommendation | X | X | |||||
| ASSESSMENTS: | |||||||
| Anthropometric measurements | X | ||||||
| Medication | X | ||||||
| Food Frequency Questionnaire (FFQs) | X | ||||||
| Tumor biopsies | X | X | X | ||||
| Fecal samples | X | X | X | ||||
| Blood samples | X | X | X | ||||
| Anastomotic leak | X | ||||||
| Surgical site infections | X | ||||||
| CRC recurrence | X | ||||||
| Response to adjuvant therapy | X | ||||||
| Disease-free survival | X | ||||||
| Quality of life questionnaire | X | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Sánchez, M.A.; Núñez-Sánchez, M.Á.; Balaguer-Román, A.; Oliva-Bolarín, A.; Pujante-Gilabert, G.; Hernández-Agüera, Q.; Mesa-López, M.J.; Egea-Valenzuela, J.; Queipo-Ortuño, M.I.; Ruiz-Alcaraz, A.J.; et al. Gut Microbiome Modification through Dietary Intervention in Patients with Colorectal Cancer: Protocol for a Prospective, Interventional, Controlled, Randomized Clinical Trial in Patients with Scheduled Surgical Intervention for CRC. J. Clin. Med. 2022, 11, 3613. https://doi.org/10.3390/jcm11133613
Martínez-Sánchez MA, Núñez-Sánchez MÁ, Balaguer-Román A, Oliva-Bolarín A, Pujante-Gilabert G, Hernández-Agüera Q, Mesa-López MJ, Egea-Valenzuela J, Queipo-Ortuño MI, Ruiz-Alcaraz AJ, et al. Gut Microbiome Modification through Dietary Intervention in Patients with Colorectal Cancer: Protocol for a Prospective, Interventional, Controlled, Randomized Clinical Trial in Patients with Scheduled Surgical Intervention for CRC. Journal of Clinical Medicine. 2022; 11(13):3613. https://doi.org/10.3390/jcm11133613
Chicago/Turabian StyleMartínez-Sánchez, María Antonia, María Ángeles Núñez-Sánchez, Andrés Balaguer-Román, Alba Oliva-Bolarín, Gabriel Pujante-Gilabert, Quiteria Hernández-Agüera, María José Mesa-López, Juan Egea-Valenzuela, María Isabel Queipo-Ortuño, Antonio José Ruiz-Alcaraz, and et al. 2022. "Gut Microbiome Modification through Dietary Intervention in Patients with Colorectal Cancer: Protocol for a Prospective, Interventional, Controlled, Randomized Clinical Trial in Patients with Scheduled Surgical Intervention for CRC" Journal of Clinical Medicine 11, no. 13: 3613. https://doi.org/10.3390/jcm11133613