1. Introduction
Vaccination against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) induces a rapid and strong immunological response in healthy individuals [
1]. Anti-SARS-CoV-2 antibodies are a serological marker of an adequate immune response and correlate with protection against coronavirus disease 2019 (COVID-19) induced by vaccination [
2]. In particular, IgG antibodies correlate with protection from death and hospitalization due to COVID-19 [
3,
4]. Two doses of vaccine usually induce sufficient antibodies for protection against the SARS-CoV-2 Alpha and Delta variant, whereas three doses are required to induce protection against the Omicron variant in healthy individuals [
5].
Kidney transplant recipients (KTR) show a secondary immunodeficiency caused by the intake of immunosuppressive medication [
6] and chronic kidney disease [
7]. Reduced immunogenicity of SARS-CoV-2 vaccines leads to a low rate of sufficient serological response and lower levels of antibodies in KTR [
8,
9,
10]. Specifically, only 19–54% of KTR showed sufficient response after two doses of the vaccine [
8,
11,
12]. Similarly, only 42% of KTR exhibited vaccination response after a third dose of the vaccine, while seroconversion reached 95% in dialysis patients and 98% in medical personnel [
10,
12,
13]. The result is a lack of protection against COVID-19 in KTR as compared with healthy individuals [
14,
15]. A third vaccination was recommended early on for KTR in order to increase immune response [
16]. Further, repeated vaccinations under modulated immunosuppression effectively increase protection, yet a substantial number of patients do not reach protective antibody levels [
12,
17,
18].
Vaccine effectiveness after two and three doses of the vaccine vanishes over time even in healthy individuals, limiting the duration of protection [
1]. Six months after a third vaccination, seroconversion remains positive in 98% healthy controls, but only in 87% of KTR and 91% of dialysis patients [
19]. Whether the limited immune response in KTR leads to a faster reduction in protection after three, four, and five doses of vaccine is not fully understood [
18].
In the current study, we assess the course of anti-SARS-CoV-2 antibodies over time in KTR who show serological response after receiving two to five doses of SARS-CoV-2 vaccines. We evaluate the serological response with two different Ig assays. Finally, we correlate measurements between IgG and IgA assays.
2. Materials and Methods
Kidney transplant recipients treated and followed at our institution received repeated doses of SARS-CoV-2 vaccines in case of sustained non-response to vaccination against SARS-CoV-2 [
17]. Data from up to five doses of vaccine were included in this analysis. Basic immunization was performed with two doses; the third, fourth, and fifth immunizations were performed with one dose of BNT162b2 (Comirnaty, BioNTech, Mainz, Germany/Pfizer; New York City, NY, USA), mRNA-1273 (Spikevax, Moderna Biotech, Cambridge, MA, USA), ChAdOx1-S (AZD1222, AstraZeneca, Cambridge, UK) or Ad26.COV2.S (Johnson & Johnson, Janssen, Beerse, Belgium) in different combinations. We obtained written and informed consent into off-label use for vaccine doses four and five from all patients.
At routine visits, serological response following vaccinations was measured using different assays either alone or in parallel:
An anti-SARS-CoV-2 enzyme-linked immunosorbent assays (ELISA) for the detection of IgG antibodies against the S1 domain of the SARS-CoV-2 spike (S) protein in serum according to the instructions of the manufacturer (Anti-SARS-CoV-2-ELISA (IgG), EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany) [
20]. Processing and measurement were done using the fully automated ‘Immunomat’ (Institut Virion\Serion GmbH, Würzburg, Germany). Results were determined by comparing the obtained signals of the patient samples with the previously obtained cut-off value of the calibrator. As suggested by the manufacturer, we considered samples with a cut-off index ≥ 1.1 positive for IgG and IgA.
An electrochemiluminescence immunoassay (ECLIA, Elecsys, Anti-SARS-CoV-2, Roche Diagnostics GmbH, Mannheim, Germany) for the detection of human immunoglobulins, including IgG, IgA, and IgM against the spike receptor binding (RBD) domain protein. Results were determined by comparing the obtained signals of the patient samples with the previously obtained cut-off value of the calibrator. As suggested by the manufacturer and as recommended by Caillard et al [
18], we considered samples with a cut-off index ≥ 264 U/mL positive. The standard maximum level determined was >2500 U/mL. With regard to the following analyses, we defined the maximum measurement of >2500 U/mL as equal to 2500 U/mL and removed measurements that were only performed to a maximum dilution of >250 U/mL from the dataset.
We retrospectively analyzed serological response to all basic immunizations; the third, fourth, and fifth immunizations were performed between 27 December 2020 and 31 December 2021. We included serological data of COVID-naïve and previously non-responding adult kidney transplant recipients who received at least one SARS-CoV-2 vaccination after kidney transplantation into the analysis. Conversely, any positive SARS-CoV-2 RNA PCR, positive anti-SARS-CoV-2-N-protein antibodies, positive anti-SARS-CoV-2 Ig, or administration of monoclonal anti-SARS-CoV-2-S-protein antibody therapy before the serological sample lead to the exclusion of the respective following serological data. Samples performed within less than 14 days after vaccination were not included.
The primary outcome was the course of serological response within the vaccination interval, hence being after the respective vaccination and before any further vaccination. The secondary outcomes were the correlations of serological measurements between the two aforementioned anti-SARS-CoV-2 Ig ELISA (IgG) and ECLIA (total Ig) assays and the anti-SARS-CoV-2 IgA ELISA assay.
For the analysis of the course of anti-SARS-CoV-2 Ig after vaccination, we only included patients who showed a positive serological response to the respective vaccination. We assigned all serological samples to periods with regard to their time distance to the date of vaccination: First period at 2–6 weeks (14 to 41 days), second period at 6–12 weeks (42 to 83 days), and third period at 12–40 weeks (84 to 279 days) after vaccination. We evaluated the results of the two different anti-SARS-CoV-2 Ig assays separately. In the case of multiple samples in the same patient within the same period in the same vaccination interval, we kept only the first sample. We paired the data from the first period with the data from the second and third period, respectively, in all patients with available anti-SARS-CoV-2 Ig samples in the respective pairs of periods. Finally, we compared the level of anti-SARS-CoV-2 Ig at the first period with the level at the second and third period, respectively. We performed two-sided Wilcoxon signed-rank tests to test for differences between the periods.
To correlate serological measurements between the two anti-SARS-CoV-2 Ig assays (IgG ELISA and IgG ECLIA) as well as between Ig and the anti-SARS-CoV-2 IgA assay (IgA ELISA), we compared pairs of data that came from the same patient at the same date in graphical analysis. To determine the statistical relationship between the assay’s results, we calculated the Pearson product-moment correlation coefficient for parametric or Kendall rank correlation test for non-parametric data after testing for normality using Shapiro–Wilk normality test.
RStudio v. 1.4.1717 developed by RStudio, Inc., Boston, MA, USA and R version 4.1.1 (10 August 2021) developed by the R Core Team were used to perform the statistical analysis. We applied a significance level alpha = 0.05 for all calculations.
The institutional ethics committee of Charité–Universitätsmedizin Berlin, Germany approved this retrospective analysis (ethics votum EA1/030/22).
3. Results
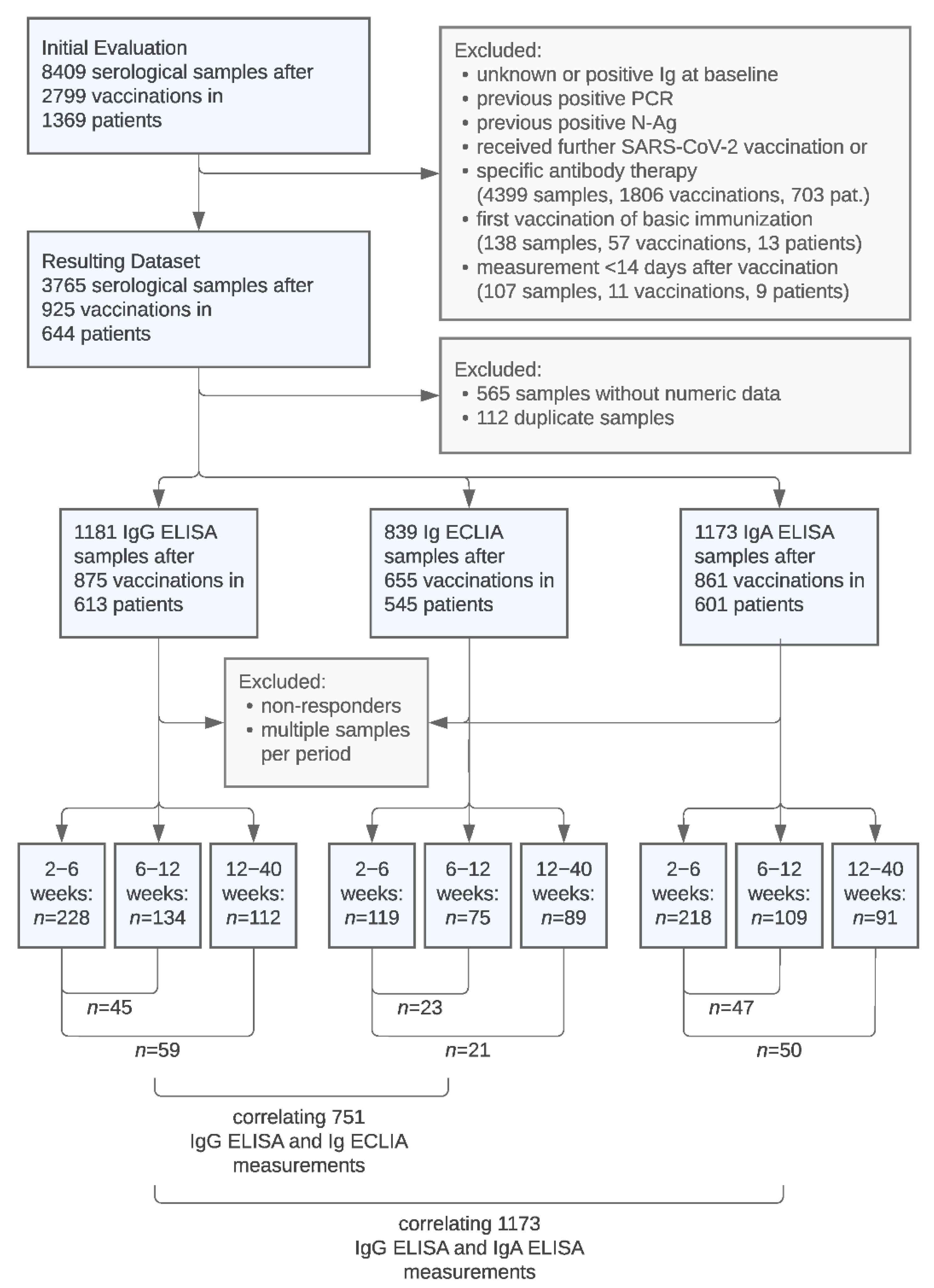
A total of 8409 serological samples after 2799 SARS-CoV-2 vaccinations in 1369 patients were initially evaluated.
Figure 1 illustrates the process of data exclusion and the split into datasets comprised of serological samples performed with the respective IgG ELISA, Ig ECLIA, and IgA ELISA assays.
Figure 1 also presents the amount of paired data used for the following comparison of anti-SARS-CoV-2 IgG levels in different periods and the selection of samples used for correlations between the assays.
Table 1 presents the baseline demographic and immunosuppression data of the 644 included patients and characteristics of the 925 included vaccinations.
Serological samples from the first, second, and third period were performed at a median of 32 days (1 month), 61 days (2 months), and 124 days (4 months), respectively, after the date of vaccination. In vaccine responders, mean Ig levels determined with ELISA and ECLIA showed a large variability. Mean IgG ELISA, Ig ECLIA, and IgA ELISA levels peaked at 1 month and decreased by 14%, 25%, and 17%, respectively, essentially already at 2 months without substantial further decrease at 4 months (
Table 2).
3.1. Course of Anti-SARS-CoV-2 Ig after SARS-CoV-2 Vaccination in Paired Samples
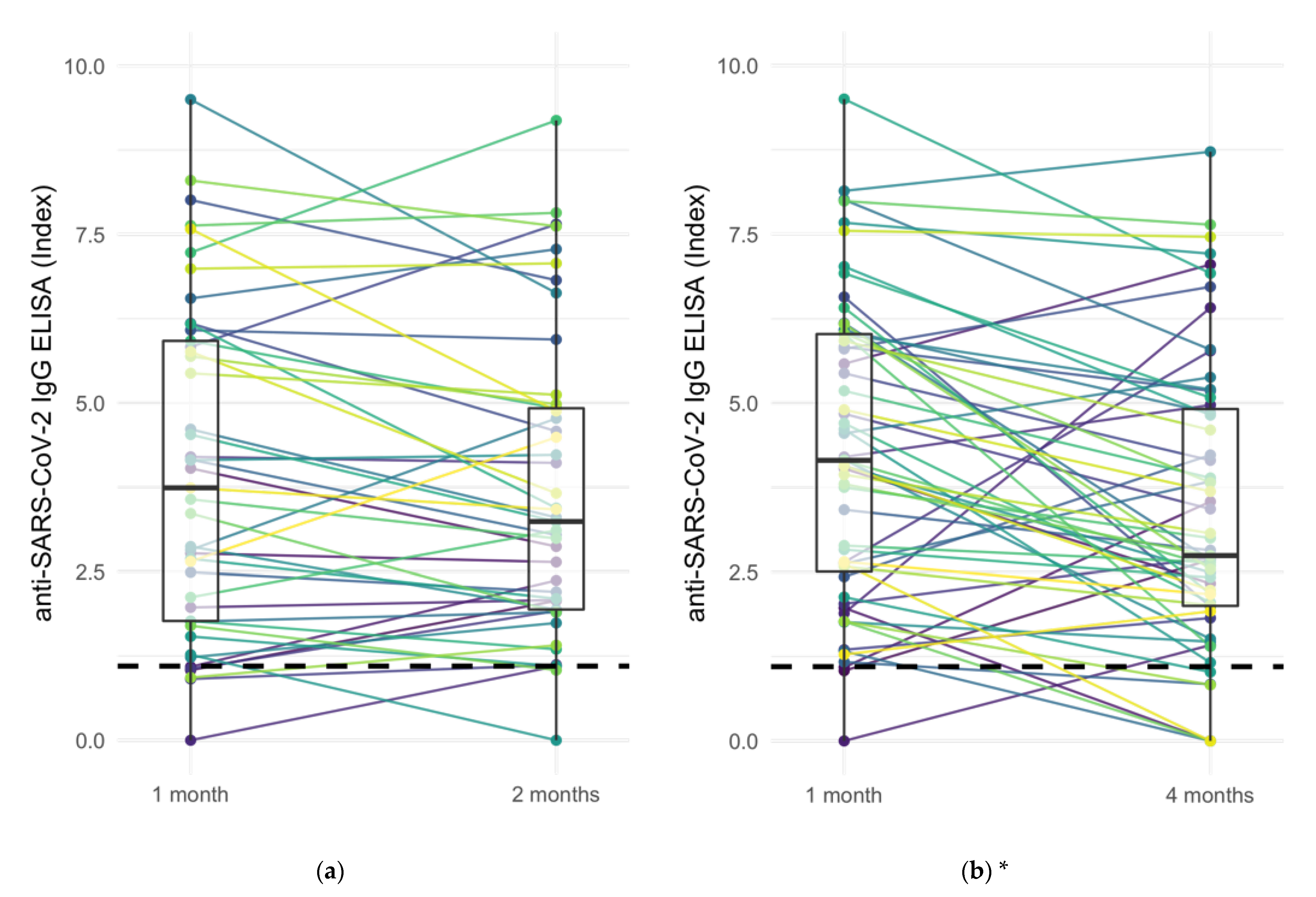
The specific comparison of anti-SARS-CoV-2 Ig levels of responders at 1 month with levels at 2 and 4 months in paired samples from both IgG ELISA and Ig ECLIA assays showed decreasing Ig levels in 77 of 148 (52.0%) of vaccination cases, increasing Ig levels in 26 of 148 (17.6%) cases, and stable Ig levels (±20%) in the remaining 45 cases (30.0%) (
Figure 2). In 18 out of 137 paired samples (12.2%) with positive Ig levels at 1 month, Ig levels were determined below the respective cut-off at a later period.
The decrease of anti-SARS-CoV-2 Ig levels between 1 and 4 months in both ELISA and ECLIA Ig assays was significant according to two-sided Wilcoxon signed-rank test (ELISA: p < 0.001, ECLIA: p = 0.005). The comparison of anti-SARS-CoV-2 Ig levels between 1 and 2 months, however, was only significant in ECLIA samples but not in ELISA (ELISA: p = 0.12, ECLIA: p < 0.05).
Responders with increasing Ig levels after vaccination were more frequently observed to be younger, non-diabetic, and receiving mycophenolic acid and belatacept immunosuppression (
Table 3).
3.2. Correlation of Anti-SARS-CoV-2 IgG ELISA and Ig ECLIA
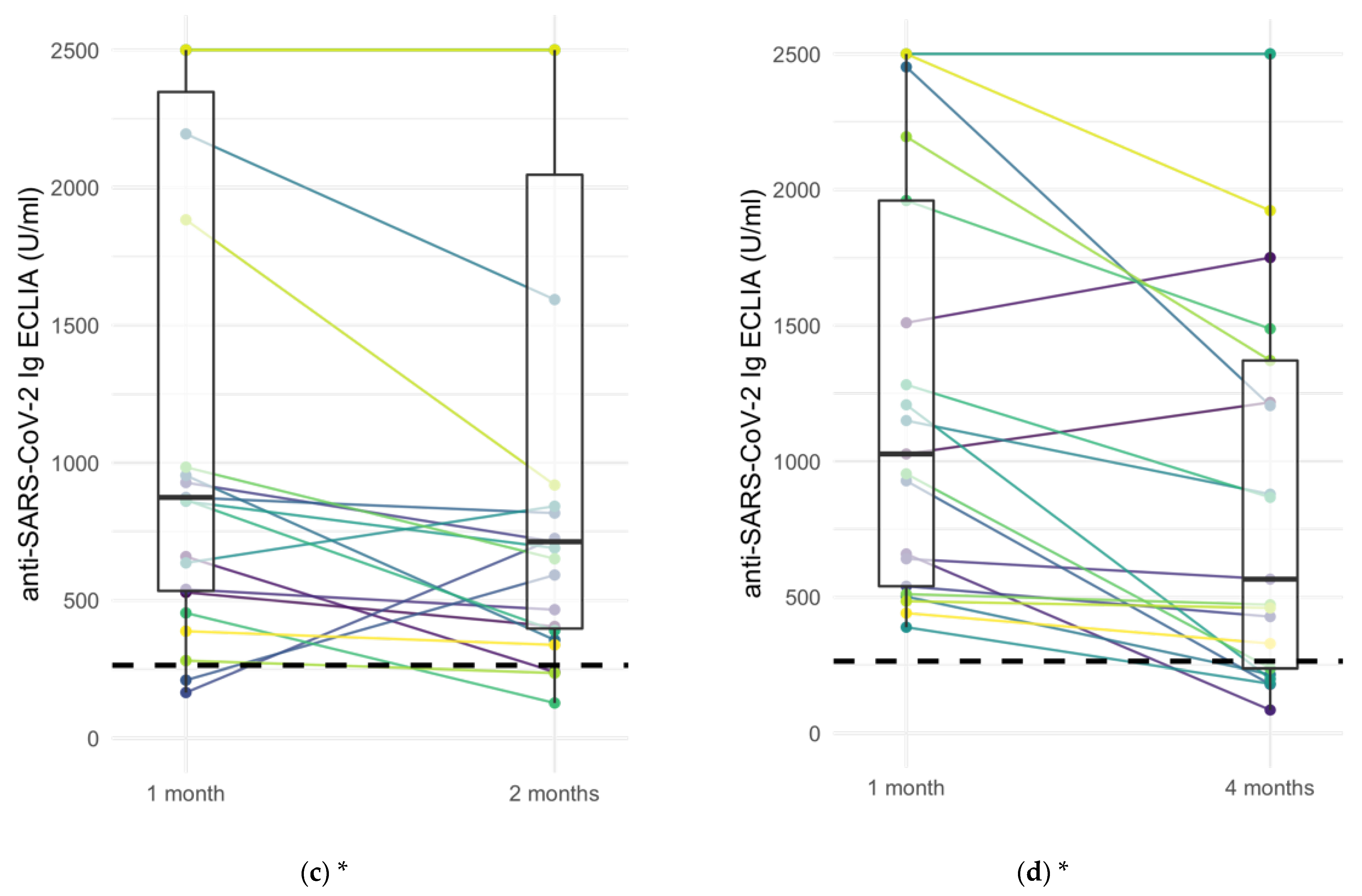
Correlation of 751 anti-SARS-CoV-2 IgG ELISA with Ig ECLIA assay results showed a strong positive association between the two tests (
Figure 3) (Kendall’s tau-b correlation coefficient = 0.784,
p < 0.001). Despite the strong positive correlation, we observed cases that were positive in ELISA and negative in ECLIA (97 of 751; 12.8%) and vice versa (2 of 751; 0.2%) (
Table 4).
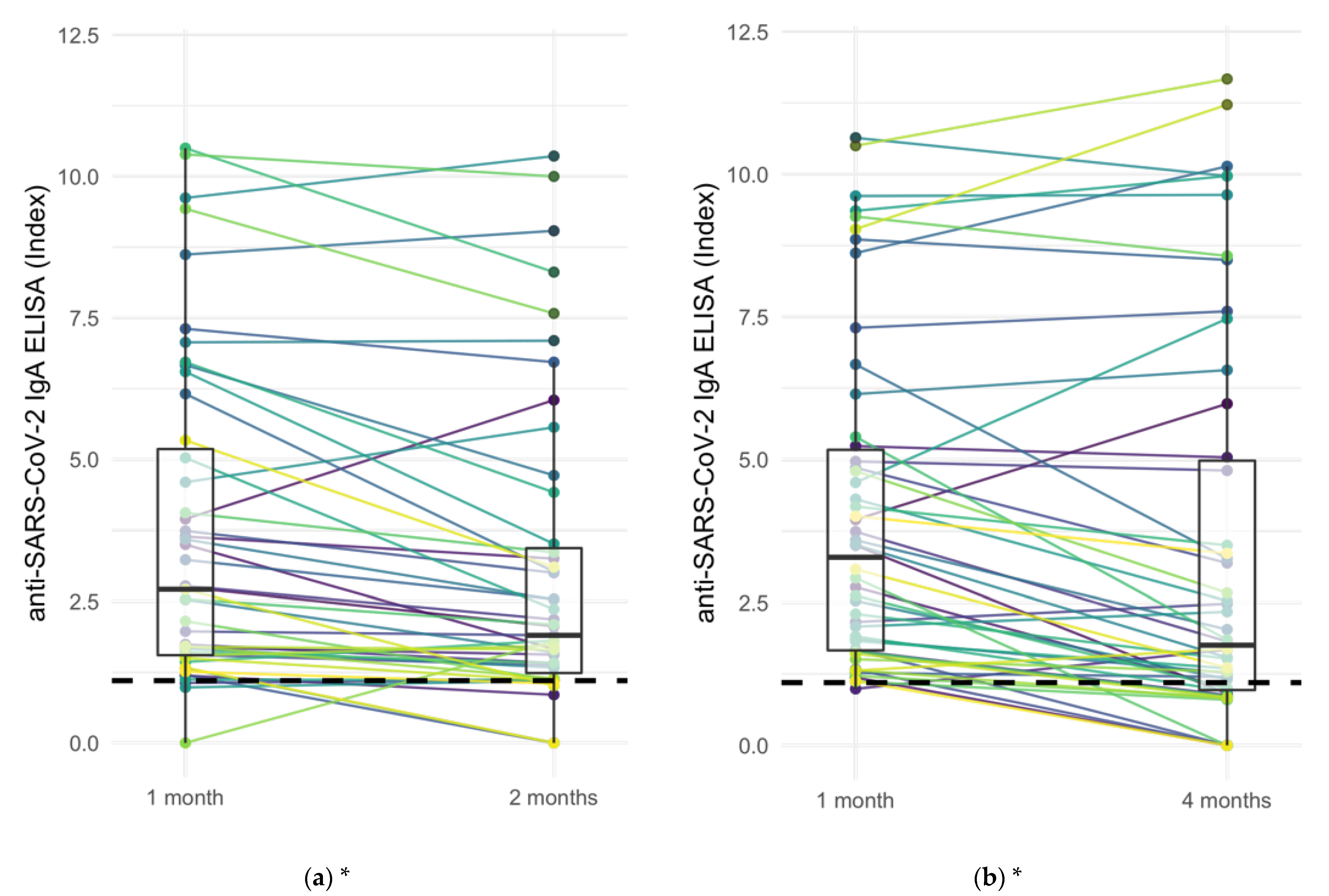
3.3. Course of Anti-SARS-CoV-2 IgA after SARS-CoV-2 Vaccination in Paired Samples
Anti-SARS-CoV-2 IgA levels of IgA-responders at 1 month with levels at 2 months and 4 months in paired samples from IgA ELISA assays showed decreasing IgA levels in 50 of 97 (51.5%) of cases, increasing IgA levels in 9 of 97 (9.2%) cases, and stable Ig levels (±20%) in the remaining 38 cases (39.2%) (
Figure 4). Twenty-one of 97 (21.6%) became negative. The decrease of anti-SARS-CoV-2 Ig levels between 1 and 2 months as well as between 1 and 4 months was significant according to two-sided Wilcoxon signed-rank test (
p < 0.001 for both).
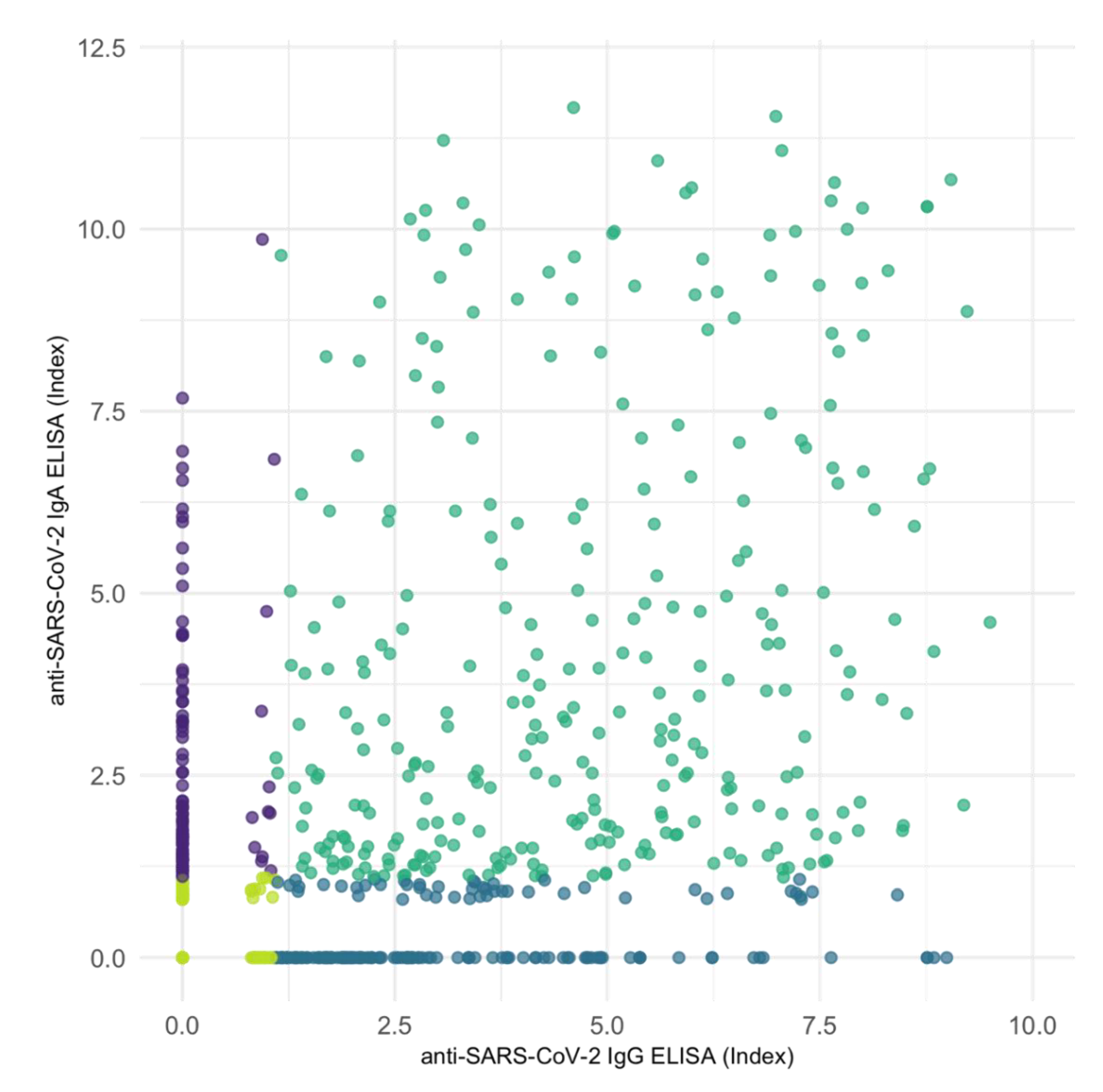
3.4. Correlation of Anti-SARS-CoV-2 IgG and IgA
Correlation of all 1.173 anti-SARS-CoV-2 IgG ELISA with corresponding IgA ELISA assay results showed a moderate positive association between the two variables (
Figure 5) (Kendall’s tau-b correlation coefficient = 0.499,
p < 0.001). However, IgA and IgG assays determined differing results in 266 of 1173 cases (
Table 5). We found only a weak correlation when limiting the analysis to data pairs with positive measurements in at least one (tau = 0.141,
p < 0.001) or in both the compared IgG and IgA assay (tau = 0.176,
p < 0.001).
In cases with divergent results, the percentage of IgG only vs. IgA only positive measurements increased with time after the vaccination (
Figure 6 and
Supplementary Figure S1).
In both assays, variable distribution did not follow a normal distribution according to Shapiro–Wilk normality test.
4. Discussion
The current study presents the first systematic analysis of anti-SARS-CoV-2 Ig antibody course after vaccination in a large cohort of previously nonresponding KTR who were subsequently receiving up to five doses of vaccine.
While it is known that rates of serological non-responders are inadequately high among KTR [
9,
12,
16], we were able to show that levels of humoral protection decrease early also in responding KTR irrespective of the type of Ig and the assay used. Loss of antibodies at 2 and 4 months after vaccination occurred in a substantial number of initially responding individuals, presumably resulting in a loss of protection against COVID-19. While it is known that patients receiving MPA have a low vaccination response rate [
17,
21], our results suggest that the use of MPA is also associated with a delay in vaccination response, resulting in increasing Ig levels over time in almost 18% of patients. Most importantly, we noted a high variability in the development of humoral protection over time between KTR. These results support the monitoring of antibody levels and, if required, shorter vaccination intervals in KTR compared with healthy individuals. Effectively, a higher number of vaccine doses is required for kTR to reach protection.
The loss of protective Ig levels over time is more pronounced in KTR than in healthy individuals who are able to generate a detectable immune response over a period of more than 6 months [
22,
23]. Contrary to patients receiving hemodialysis who show high response rates after two doses of the vaccine, [
24] KTR do require repeated doses to elicit a sufficient humoral response. Still, the decrease of mean Ig levels in both hemodialysis patients and KTR might be comparable [
24]. Similar to our results, Weigert et al. reported a 25% decrease in IgG from 42 to 140 days after vaccination. In both populations, loss of protection does occur faster and more frequently than in healthy individuals.
It should be noted that the used Ig level cut-offs are indicative of protection against SARS-CoV-2 variants before the Delta variant. Although we cannot determine any clear cut-off values, loss of protection against Delta and Omicron variants will be more severe as these variants have been shown to require a higher level of humoral response for protection [
5]. Even though humoral response correlates with protection from disease, specific neutralizing antibodies and T cell response are important factors that we did not cover in this analysis.
The correlation of two different anti-SARS-CoV-2 Ig assays, namely one IgG and one total Ig assay, in our population, revealed that despite a strong positive correlation between the assays’ results, a relevant number of individuals presented with diverging results. This observation reflects some differences in sensitivity between both assays. Whether this should impact clinical practice and trigger the use of multiple assays, preference of one assay over the other cannot be concluded from our analysis.
IgA response was described to dominate the early neutralizing antibody response in SARS-CoV-2 cases [
25]. Serum IgA has been interpreted as a proxy of salivary IgA, and low serum IgA levels have been correlated with breakthrough infections [
26]. Correlation of IgG and IgA assay results indicates that these lead to consistent interpretations of results in a majority of cases. However, in about a quarter of cases we observed diverging results, and moreover, the level of IgG and IgA antibodies did not correlate well in positive cases. In previous studies, KTR with positivity in either one of the assays were classified as responders, which might have led to an overinterpretation of vaccine response in KTR [
10].
Due to the study’s retrospective design, methodological limitations arise. However, the applied selection criteria for sample data account for the risk of selection bias. In a large number of patients at our institution, repeated serological measurements were not performed, thus resulting in the exclusion of singular samples. Hence, limiting the comparison of Ig levels between intervals to paired data samples decreased the size of the dataset but also reduced the risk selection bias due to singular samples that might not have been followed up due to confounding reasons. Despite the limitations, our analysis provides the first data of different assays and time course of the serological response in a large number of KTR.
5. Conclusions
Large individual variability in serological response and loss of serological response after 4 months in 21% of patients support the utility of regular serological monitoring and might argue for the consideration of shorter and individualized vaccination intervals in KTR.
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/jcm11123291/s1, Figure S1. 266 cases where IgA and IgG assays determined differing results (only IgG positive vs. only IgA positive measurements) and their relative frequency over time.
Author Contributions
Conceptualization, S.R., B.O., K.B. and E.S.; methodology, S.R., B.O., K.B. and E.S.; formal analysis, S.R. and B.O.; investigation, A.J., C.H., N.K., B.Z., F.B., M.C., U.W., B.E., J.H. and F.H.; resources, K.B.; data curation, S.R., B.O., A.J., C.H., B.E., J.H., F.G. and M.M.; writing—original draft preparation, S.R., B.O. and E.S.; writing—review and editing, K.B., A.J., N.K., B.Z., F.B., M.C., U.W., B.E., J.H. and F.H.; visualization, S.R.; supervision, E.S. and K.B.; project administration, E.S. and K.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Charité–Universitätsmedizin Berlin (protocol code of the ethics votum: EA1/030/22, date of approval 10 March 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to their containing personal information that could compromise the privacy of involved patients.
Acknowledgments
E.S. is a participant in the BIH-Charité Clinician Scientist Program funded by the Charité—Universitätsmedizin Berlin and the Berlin Institute of Health.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by COVID-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. Available online: https://www.nature.com/articles/s41591-021-01540-1 (accessed on 18 February 2022). [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. Available online: https://www.nature.com/articles/s41591-021-01377-8 (accessed on 18 February 2022). [CrossRef] [PubMed]
- Gruell, H.; Vanshylla, K.; Tober-Lau, P.; Hillus, D.; Schommers, P.; Lehmann, C.; Kurth, F.; Sander, L.E.; Klein, F. mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. Nat. Med. 2022, 28, 477–480. Available online: https://www.nature.com/articles/s41591-021-01676-0 (accessed on 1 March 2022).
- Phadke, V.K.; Scanlon, N.; Jordan, S.C.; Rouphael, N.G. Immune Responses to SARS-CoV-2 in Solid Organ Transplant Recipients. Curr. Transplant. Rep. 2021, 8, 127–139. Available online: https://pubmed.ncbi.nlm.nih.gov/33688459/ (accessed on 18 February 2022). [CrossRef]
- Steiger, S.; Rossaint, J.; Zarbock, A.; Anders, H.J. Secondary Immunodeficiency Related to Kidney Disease (SIDKD)—Definition, Unmet Need, and Mechanisms. J. Am. Soc. Nephrol. 2022, 33, 259–278. Available online: https://jasn.asnjournals.org/content/33/2/259 (accessed on 3 March 2022). [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. Available online: https://jamanetwork.com/journals/jama/fullarticle/2779852 (accessed on 18 February 2022). [CrossRef]
- Schrezenmeier, E.; Rincon-Arevalo, H.; Stefanski, A.L.; Potekhin, A.; Staub-Hohenbleicher, H.; Choi, M.; Bachmann, F.; Proβ, V.; Hammett, C.; Schrezenmeier, H.; et al. B and t cell responses after a third dose of SARS-CoV-2 vaccine in kidney transplant recipients. J. Am. Soc. Nephrol. 2021, 32, 3027–3033. Available online: https://jasn.asnjournals.org/content/32/12/3027 (accessed on 18 February 2022). [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health-Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Fujieda, K.; Tanaka, A.; Kikuchi, R.; Takai, N.; Saito, S.; Yasuda, Y.; Fujita, T.; Kato, M.; Furuhashi, K.; Maruyama, S. Antibody response to double SARS-CoV-2 mRNA vaccination in Japanese kidney transplant recipients. Sci. Rep. 2022, 12, 6850. Available online: https://www.nature.com/articles/s41598-022-10510-7 (accessed on 1 June 2022). [CrossRef] [PubMed]
- Osmanodja, B.; Ronicke, S.; Budde, K.; Jens, A.; Hammett, C.; Koch, N.; Seelow, E.; Waiser, J.; Zukunft, B.; Bachmann, F.; et al. Serological Response to Three, Four and Five Doses of SARS-CoV-2 Vaccine in Kidney Transplant Recipients. J. Clin. Med. 2022, 11, 2565. [Google Scholar] [CrossRef] [PubMed]
- Reindl-Schwaighofer, R.; Heinzel, A.; Mayrdorfer, M.; Jabbour, R.; Hofbauer, T.M.; Merrelaar, A.; Eder, M.; Regele, F.; Doberer, K.; Spechtl, P.; et al. Comparison of SARS-CoV-2 Antibody Response 4 Weeks After Homologous vs Heterologous Third Vaccine Dose in Kidney Transplant Recipients: A Randomized Clinical Trial. JAMA Intern. Med. 2022, 182, 165–171. Available online: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2787200 (accessed on 1 June 2022). [CrossRef] [PubMed]
- Reischig, T.; Kacer, M.; Vlas, T.; Drenko, P.; Kielberger, L.; Machova, J.; Topolcan, O.; Kucera, R.; Kormunda, S. Insufficient response to mRNA SARS-CoV-2 vaccine and high incidence of severe COVID-19 in kidney transplant recipients during pandemic. Am. J. Transplant. 2022, 22, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Osmanodja, B.; Mayrdorfer, M.; Halleck, F.; Choi, M.; Budde, K. Undoubtedly, kidney transplant recipients have a higher mortality due to COVID-19 disease compared to the general population. Transpl. Int. 2021, 34, 769–771. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Schrezenmeier, E.; Rincon-Arevalo, H.; Jens, A.; Stefanski, A.L.; Hammett, C.; Osmanodja, B.; Koch, N.; Zukunft, B.; Beck, J.; Oellerich, M.; et al. Temporary hold of mycophenolate boosts SARS-CoV-2 vaccination-specific humoral and cellular immunity in kidney transplant recipients. medRxiv 2022. [CrossRef]
- Caillard, S.; Thaunat, O. COVID-19 vaccination in kidney transplant recipients. Nat. Rev. Nephrol. 2021, 17, 785–787. Available online: https://www.nature.com/articles/s41581-021-00491-7 (accessed on 18 February 2022). [CrossRef]
- Stumpf, J.; Schwöbel, J.; Lindner, T.; Anders, L.; Siepmann, T.; Karger, C.; Hüther, J.; Martin, H.; Müller, P.; Faulhaber-Walter, R.; et al. Risk of strong antibody decline in dialysis and transplant patients after SARS-CoV-2mRNA vaccination: Six months data from the observational Dia-Vacc study. Lancet Reg. Health–Eur. 2022, 17, 100371. Available online: http://www.thelancet.com/article/S2666776222000643/fulltext (accessed on 18 February 2022). [CrossRef]
- Jahrsdörfer, B.; Kroschel, J.; Ludwig, C.; Corman, V.M.; Schwarz, T.; Körper, S.; Rojewski, M.; Lotfi, R.; Weinstock, C.; Drosten, C.; et al. Independent Side-by-Side Validation and Comparison of 4 Serological Platforms for SARS-CoV-2 Antibody Testing. J. Infect. Dis. 2021, 223, 796–801. Available online: https://academic.oup.com/jid/article/223/5/796/5926414 (accessed on 18 February 2022). [CrossRef]
- Kantauskaite, M.; Mueller, L.; Hillebrandt, J.; Lamberti, J.L.; Fischer, S.; Kolb, T.; Ivens, K.; Koch, M.; Andree, M.; Lübke, N.; et al. Immune response to third SARS-CoV-2 vaccination in seronegative kidney transplant recipients: Possible improvement by mycophenolate mofetil reduction. medRxiv 2022. [CrossRef]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef] [PubMed]
- Tober-Lau, P.; Schwarz, T.; Vanshylla, K.; Hillus, D.; Gruell, H.; Suttorp, N.; Landgraf, I.; Kappert, K.; Seybold, J.; Drosten, C.; et al. Long-term immunogenicity of BNT162b2 vaccination in older people and younger health-care workers. Lancet Respir. Med. 2021, 9, e104–e105. [Google Scholar] [CrossRef]
- Weigert, A.; Bergman, M.-L.; Gonçalves, L.A.; Godinho, I.; Duarte, N.; Abrantes, R.; Borges, P.; Brennand, A.; Malheiro, V.; Matoso, P.; et al. Longitudinal Analysis of Antibody Responses to the mRNA BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis: A 6-Month Follow-Up. Front. Med. 2021, 8, 2623. [Google Scholar] [CrossRef]
- Sterlin, D.; Mathian, A.; Miyara, M.; Mohr, A.; Anna, F.; Claër, L.; Quentric, P.; Fadlallah, J.; Devilliers, H.; Ghillani, P.; et al. IgA dominates the early neutralizing antibody response to SARS-CoV-2. Sci. Transl. Med. 2021, 13, 2223. [Google Scholar] [CrossRef]
- Sheikh-Mohamed, S.; Isho, B.; Chao, G.Y.; Zuo, M.; Cohen, C.; Lustig, Y.; Nahass, G.R.; Salomon-Shulman, R.E.; Blacker, G.; Fazel-Zarandi, M.; et al. Systemic and mucosal IgA responses are variably induced in response to SARS-CoV-2 mRNA vaccination and are associated with protection against subsequent infection. Mucosal. Immunol. 2022. [CrossRef]
Figure 1.
Flow diagram of evaluated, excluded, and included serological sample data.
Figure 1.
Flow diagram of evaluated, excluded, and included serological sample data.
Figure 2.
Comparison of anti-SARS-CoV-2 Ig levels at different intervals based on ELISA IgG and ECLIA Ig assays: (a) ELISA at 1 month vs. 2 months, (b) ELISA at 1 month vs. 4 months, (c) ECLIA at 1 month vs. 2 months, and (d) ECLIA at 1 month vs. 4 months. Wilcoxon signed-rank test showed a significant decrease between 1 and 4 months (ELISA: p < 0.001, ECLIA: p = 0.005). Dashed line: positivity cut-off at 1.1 index or 264 U/mL, respectively. Boxplots’ line, lower and upper hinge: median, first, and third quartile. * Indicating statistical significance (p-values < 0.05) in Wilcoxon signed-rank test.
Figure 2.
Comparison of anti-SARS-CoV-2 Ig levels at different intervals based on ELISA IgG and ECLIA Ig assays: (a) ELISA at 1 month vs. 2 months, (b) ELISA at 1 month vs. 4 months, (c) ECLIA at 1 month vs. 2 months, and (d) ECLIA at 1 month vs. 4 months. Wilcoxon signed-rank test showed a significant decrease between 1 and 4 months (ELISA: p < 0.001, ECLIA: p = 0.005). Dashed line: positivity cut-off at 1.1 index or 264 U/mL, respectively. Boxplots’ line, lower and upper hinge: median, first, and third quartile. * Indicating statistical significance (p-values < 0.05) in Wilcoxon signed-rank test.
Figure 3.
Correlation scatter plot of 751 serological samples performed with anti-SARS-CoV-2 IgG ELISA and Ig ECLIA assays showing a strong positive association in Kendall rank correlation test (tau = 0.784, p < 0.001). Violet: 97 samples determined as positive in ELISA but negative in ECLIA. Blue: Two samples determined as positive in ECLIA but negative in ELISA. Dark green and light green: congruent results determined as positive or negative, respectively. Black line: linear correlation.
Figure 3.
Correlation scatter plot of 751 serological samples performed with anti-SARS-CoV-2 IgG ELISA and Ig ECLIA assays showing a strong positive association in Kendall rank correlation test (tau = 0.784, p < 0.001). Violet: 97 samples determined as positive in ELISA but negative in ECLIA. Blue: Two samples determined as positive in ECLIA but negative in ELISA. Dark green and light green: congruent results determined as positive or negative, respectively. Black line: linear correlation.
Figure 4.
Comparison of anti-SARS-CoV-2 IgA levels at different intervals based on ELISA IgA assay: (a) IgA at 1 month vs. 2 months, (b) IgA at 1 month vs. 4 months. Wilcoxon signed-rank test showed a significant decrease between 1 and 2 months (p < 0.001) as well as between 1 and 4 months (p < 0.001). Dashed line: positivity cut-off at 1.1 index. Boxplots’ line, lower and upper hinge: median, first, and third quartile. * Indicating statistical significance (p-values < 0.05) in Wilcoxon signed-rank test.
Figure 4.
Comparison of anti-SARS-CoV-2 IgA levels at different intervals based on ELISA IgA assay: (a) IgA at 1 month vs. 2 months, (b) IgA at 1 month vs. 4 months. Wilcoxon signed-rank test showed a significant decrease between 1 and 2 months (p < 0.001) as well as between 1 and 4 months (p < 0.001). Dashed line: positivity cut-off at 1.1 index. Boxplots’ line, lower and upper hinge: median, first, and third quartile. * Indicating statistical significance (p-values < 0.05) in Wilcoxon signed-rank test.
Figure 5.
Correlation scatter plot of serological samples performed with anti-SARS-CoV-2 IgG ELISA and IgA ELISA assays. Correlation shows a moderate positive association in Kendall rank correlation test (tau = 0.499, p < 0.001). Violet: samples determined positive in IgA but negative in IgG assays. Blue: samples determined negative in IgA but positive in IgG assays. Dark green and light green: congruent results determined as positive or negative, respectively.
Figure 5.
Correlation scatter plot of serological samples performed with anti-SARS-CoV-2 IgG ELISA and IgA ELISA assays. Correlation shows a moderate positive association in Kendall rank correlation test (tau = 0.499, p < 0.001). Violet: samples determined positive in IgA but negative in IgG assays. Blue: samples determined negative in IgA but positive in IgG assays. Dark green and light green: congruent results determined as positive or negative, respectively.
Figure 6.
Correlation scatter plots of serological samples performed with anti-SARS-CoV-2 IgG ELISA and IgA ELISA assays, split by number of vaccine dose (second, third, fourth, or fifth vaccination for the individual) and time after vaccination. Violet: samples determined positive in IgA but negative in IgG assays. Blue: samples determined negative in IgA but positive in IgG assays. Dark green and light green: congruent results determined as positive or negative, respectively.
Figure 6.
Correlation scatter plots of serological samples performed with anti-SARS-CoV-2 IgG ELISA and IgA ELISA assays, split by number of vaccine dose (second, third, fourth, or fifth vaccination for the individual) and time after vaccination. Violet: samples determined positive in IgA but negative in IgG assays. Blue: samples determined negative in IgA but positive in IgG assays. Dark green and light green: congruent results determined as positive or negative, respectively.
Table 1.
Baseline characteristics of the included patients and SARS-CoV-2 vaccinations.
Table 1.
Baseline characteristics of the included patients and SARS-CoV-2 vaccinations.
| Patient Characteristics | |
| Total patients | 644 |
| Female/male patients | 237/407 (36.8%/63.2%) |
| Median age in years (IQR) | 59.1 (48.4–67.8) |
| Median transplant age in years (IQR) | 8.2 (3.1–13.7) |
| Diabetes | 134 (20.8%) |
| Body mass index kg/m2 (mean) | 25.4 |
| Number of immunosuppressive drugs (mean) | 2.60 |
| Tacrolimus | 460 (71.4%) |
| Cyclosporine A | 112 (17.4%) |
| Mycophenolic acid | 575 (89.3%) |
| Steroids | 415 (64.4%) |
| Belatacept | 52 (8.1%) |
| Azathioprin | 4 (0.6%) |
| mTORi * | 7 (1.1%) |
| low positive antibodies at baseline ** | 70 (7.6%) |
| Vaccination Characteristics | |
| Total vaccinations | 925 |
| Basic immunizations | 48 (5.2%) |
| Third vaccinations | 586 (63.4%) |
| Fourth vaccinations | 254 (27.5%) |
| Fifth vaccinations | 37 (4.0%) |
| BNT162b2 *** | 571 (61.7%) |
| mRNA-1273 *** | 159 (17.2%) |
| ChAdOx1-S *** | 159 (17.2%) |
| Ad26.COV2.S *** | 36 (3.9%) |
Table 2.
Mean anti-SARS-CoV-2 IgG, Ig, and IgA levels in responders after basic immunization, and in those who had taken a third, fourth, or fifth dose who were previously non-responding. Samples at different intervals relate to the respective IgG, Ig, and IgA assays. In comparison, non-responders exhibited IgG/Ig/IgA levels below the respective cut-offs (i.e., index ≥ 1.1 and ≥264 U/mL, respectively).
Table 2.
Mean anti-SARS-CoV-2 IgG, Ig, and IgA levels in responders after basic immunization, and in those who had taken a third, fourth, or fifth dose who were previously non-responding. Samples at different intervals relate to the respective IgG, Ig, and IgA assays. In comparison, non-responders exhibited IgG/Ig/IgA levels below the respective cut-offs (i.e., index ≥ 1.1 and ≥264 U/mL, respectively).
| Assay | 1 Month | 2 Months | 4 Months |
|---|
| Anti-SARS-CoV-2 IgG ELISA | | | |
| Number of samples | 228 | 134 | 112 |
| Median time after vaccination, days (IQR) | 31 (28–35) | 57 (48–70) | 116 (98–144) |
| Mean IgG level, index (±sd) | 4.26 (±2.25) | 3.65 (±2.15) | 3.66 (±2.21) |
| Anti-SARS-CoV-2 Ig ECLIA | | | |
| Number of samples | 119 | 75 | 89 |
| Median time after vaccination, days (IQR) | 31 (28–35) | 61 (52–71) | 123 (99–147) |
| Mean Ig level, U/mL (±sd) | 1548 (±881) | 1202 (±889) | 1145 (±818) |
| Anti-SARS-CoV-2 IgA ELISA | | | |
| Number of samples | 218 | 109 | 91 |
| Median time after vaccination, days (IQR) | 31 (28–35) | 60 (50–71) | 112 (99–138) |
| Mean IgA level, index (±sd) | 3.87 (±2.72) | 3.34 (±2.85) | 3.21 (±3.09) |
Table 3.
Comparison of baseline characteristics of patients with anti-SARS-CoV-2 Ig levels increasing vs. decreasing by at least 20% from 1 to 2 or 4 months after vaccination in paired samples. p-values according to two sample t-test.
Table 3.
Comparison of baseline characteristics of patients with anti-SARS-CoV-2 Ig levels increasing vs. decreasing by at least 20% from 1 to 2 or 4 months after vaccination in paired samples. p-values according to two sample t-test.
| Patient Characteristics | Increasing Ig Level | Decreasing Ig Level | p-Value |
|---|
| Number of patients | 22 | 47 | - |
| Female/male patients | 15/7 (68%/32%) | 26/21 (55%/45%) | - |
| Median age in years (IQR) | 41.1 (33.3–54.4) | 60.2 (49.5–71.1) | <0.001 * |
| Median transplant age in years (IQR) | 5.7 (3.7–8.5) | 7.0 (3.4–11.2) | 0.15 |
| Diabetes | 3 (13.6%) | 11 (23.4%) | 0.32 |
| Body mass index (mean) | 24.5 | 25.5 | 0.54 |
| Number of immunosuppressive drugs (mean) | 2.5 | 2.2 | 0.059 |
| Tacrolimus | 17 (77.3%) | 35 (74.5%) | 0.80 |
| Cyclosporine A | 2 (9.1%) | 9 (19.1%) | 0.24 |
| Mycophenolic acid | 21 (95.5%) | 21 (44.6%) | <0.001 * |
| Steroids | 11 (50.0%) | 37 (78.7%) | 0.027 * |
| Belatacept | 2 (9.1%) | 2 (4.2%) | 0.49 |
Table 4.
Correlation table of 751 anti-SARS-CoV-2 IgG ELISA and Ig ECLIA assay results.
Table 4.
Correlation table of 751 anti-SARS-CoV-2 IgG ELISA and Ig ECLIA assay results.
| Assay | IgG ELISA |
|---|
| | | Positive | Negative | Total |
|---|
| Ig ECLIA | positive | 260 | 2 | 262 |
| negative | 97 | 392 | 489 |
| total | 357 | 394 | 751 |
Table 5.
Correlation table of anti-SARS-CoV-2 IgG ELISA and IgA ELISA samples.
Table 5.
Correlation table of anti-SARS-CoV-2 IgG ELISA and IgA ELISA samples.
| Assay | IgG ELISA |
|---|
| | | Positive | Negative | Total |
|---|
| IgA ELISA | positive | 298 | 96 | 394 |
| negative | 174 | 605 | 779 |
| total | 472 | 701 | 1173 |
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}