
Reinforcement of the Standard Therapy with Two Infusions of Convalescent Plasma for Patients with COVID-19: A Randomized Clinical Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
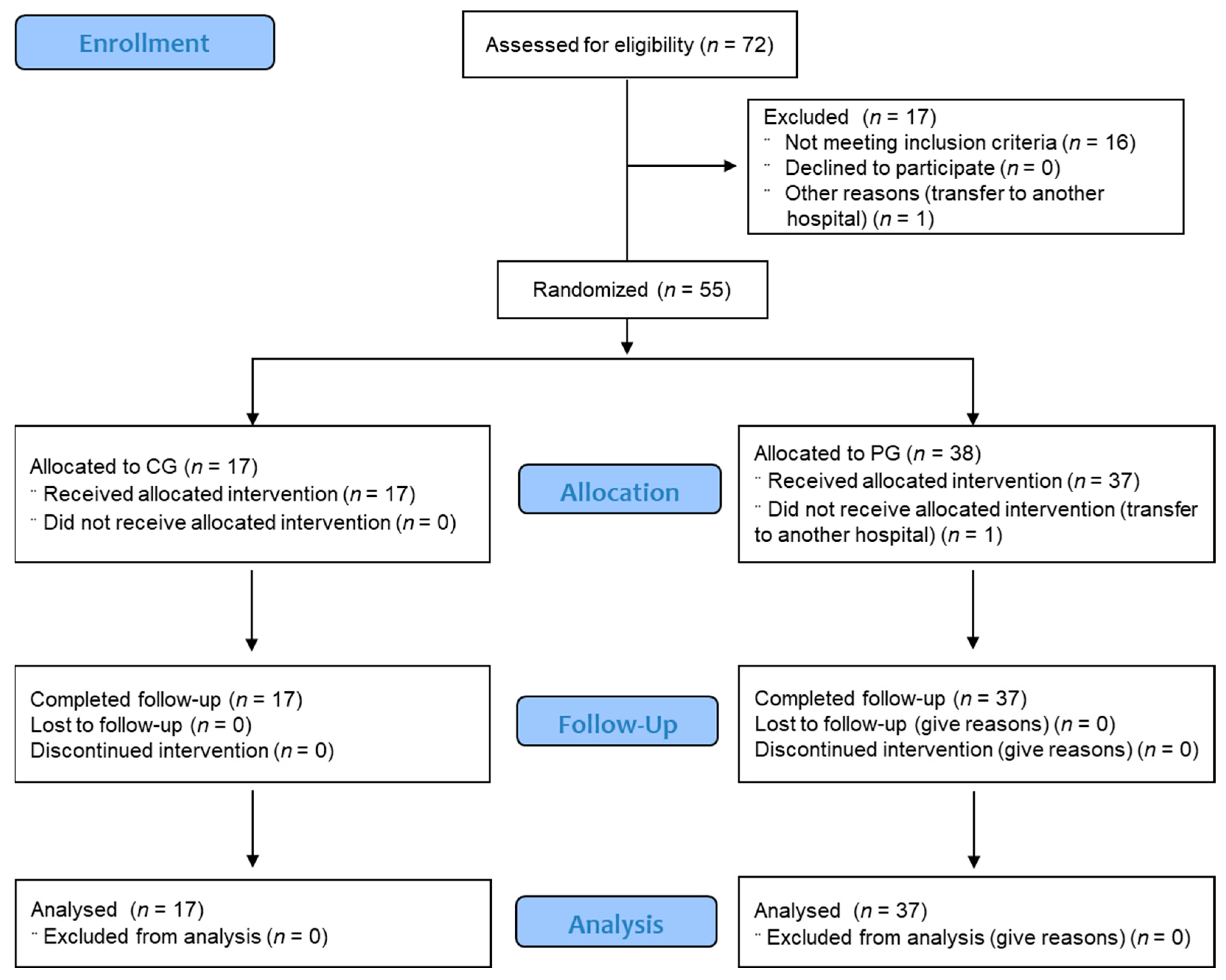
2.1. Trial Design
2.2. Recruitment and Selection Criteria
2.3. Randomization and Intervention
Intervention: HP and Plasma Donors
2.4. Clinical and Laboratory Monitoring
2.5. Trial End Points
2.6. Early Trial Termination
2.7. Statistical Analysis
3. Results
3.1. Epidemiological and Baseline Characteristics of the Trial Population
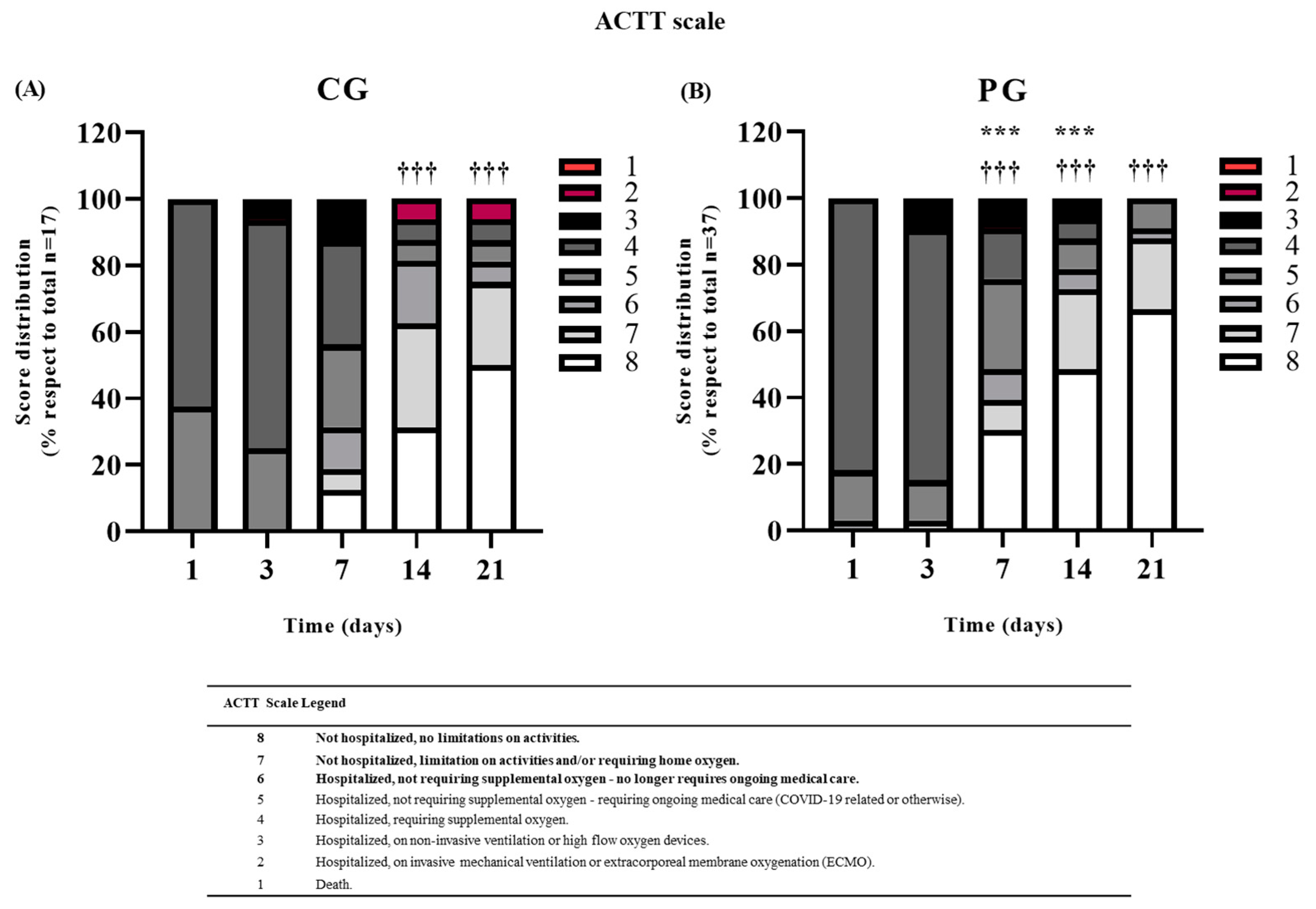
3.2. Primary EndPoint
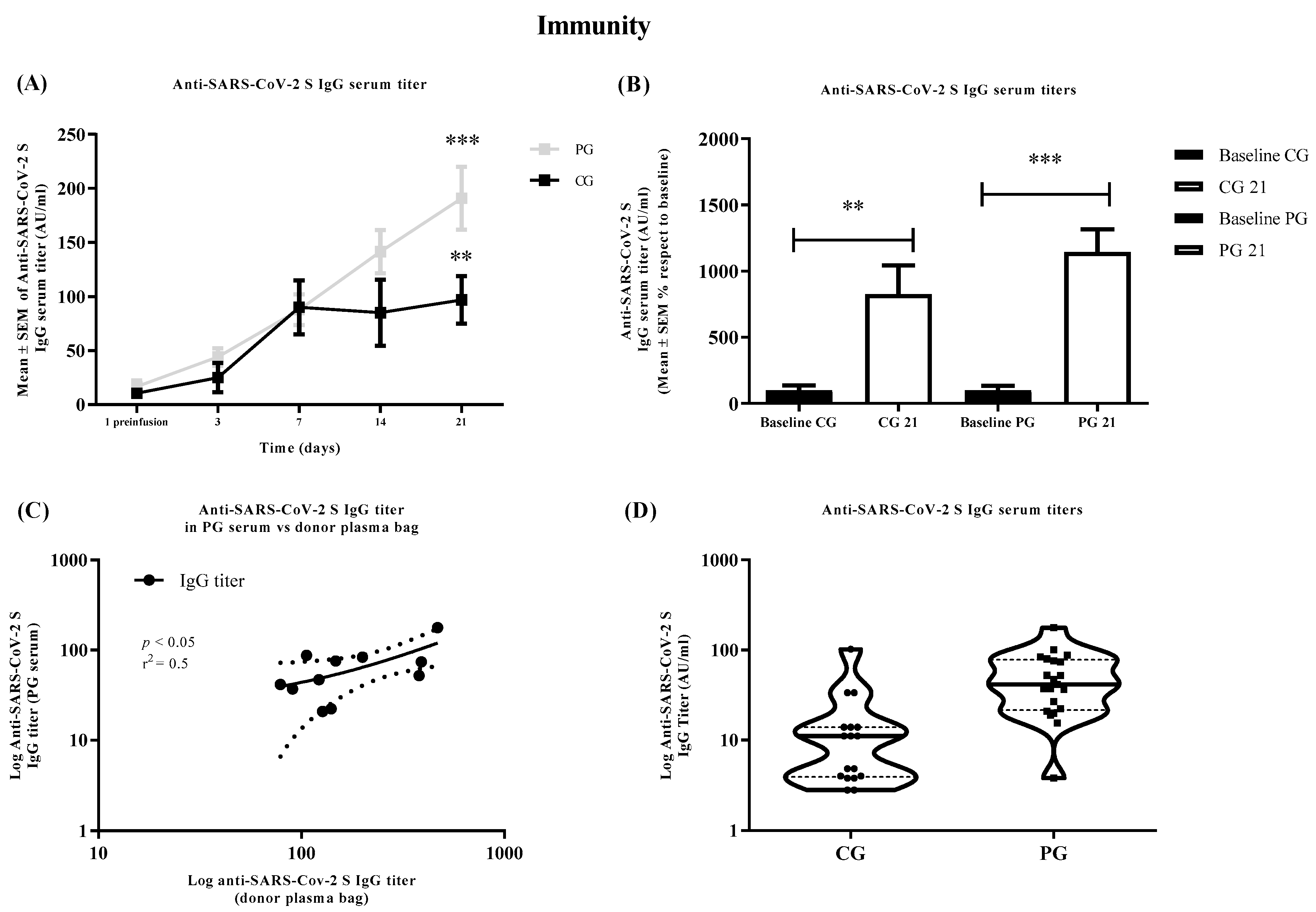
3.3. Immunity
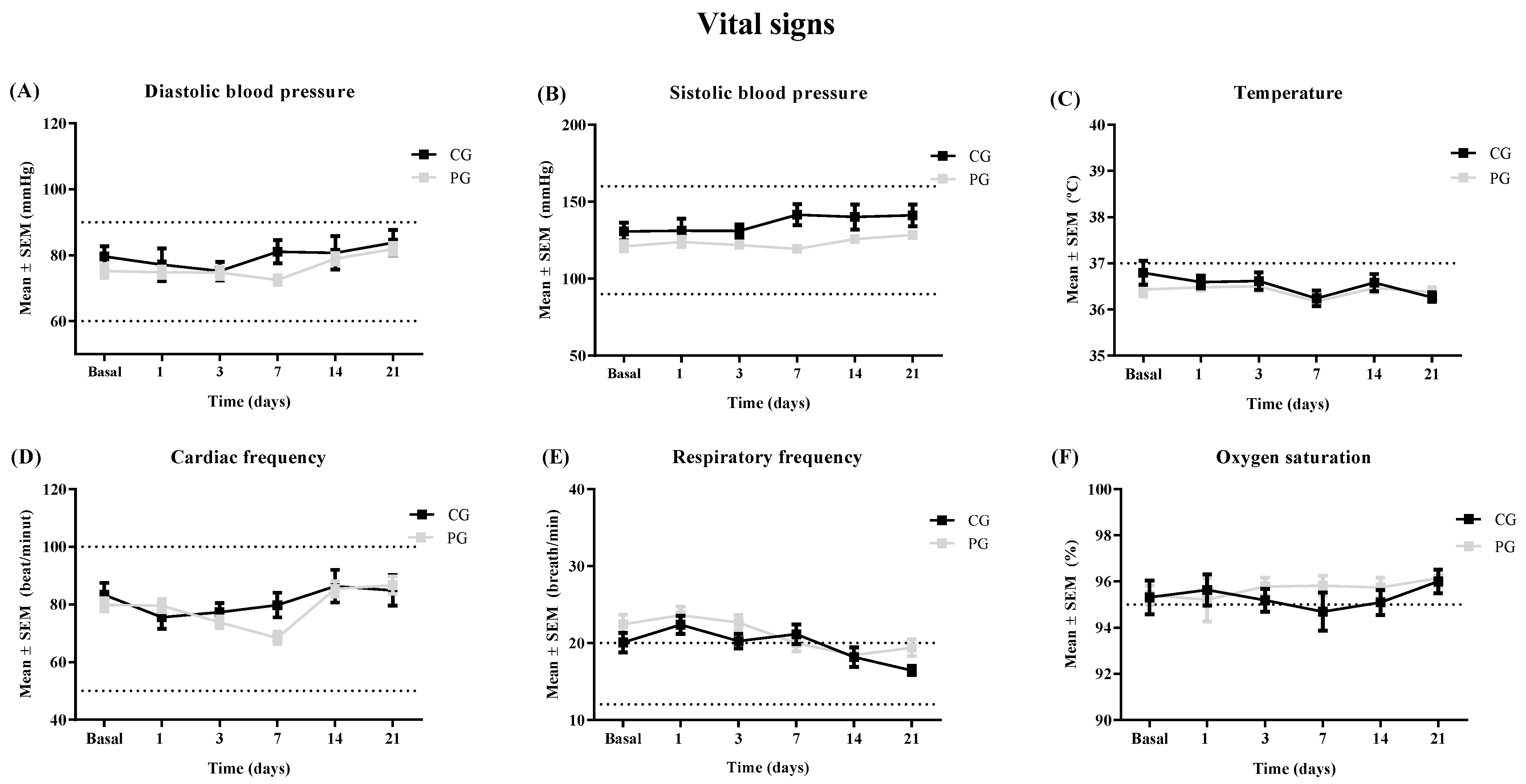
3.4. Follow-Up Clinical Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAEE | adverse effect |
| BMI | body mass index |
| CG | control group |
| ECMO | extracorporeal membrane oxygenation |
| HP | hyperimmune plasma |
| MOH | Mateu Orfila Hospital |
| PG | plasma group |
| RHM | Regional Hospital of Manacor |
| SEM | standard error of the mean |
| SOFA | Sequential Organ Failure Assessment score |
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 18 May 2022).
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. Jama 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Şimşek-Yavuz, S.; Komsuoğlu Çelikyurt, F.I. An update of anti-viral treatment of COVID-19. Turkish J. Med. Sci. 2021, 51, 3372–3390. [Google Scholar] [CrossRef] [PubMed]
- Stasi, C.; Fallani, S.; Voller, F.; Silvestri, C. Treatment for COVID-19: An overview. Eur. J. Pharmacol. 2020, 889, 173644. [Google Scholar] [CrossRef]
- Gold, J.A.W.; Rossen, L.M.; Ahmad, F.B.; Sutton, P.; Li, Z.; Salvatore, P.P.; Coyle, J.P.; DeCuir, J.; Baack, B.N.; Durant, T.M.; et al. Race, Ethnicity, and Age Trends in Persons Who Died from COVID-19—United States, May–August 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1517. [Google Scholar] [CrossRef]
- Joyner, M.J.; Wright, R.S.; Fairweather, D.; Senefeld, J.W.; Bruno, K.A.; Klassen, S.A.; Carter, R.E.; Klompas, A.M.; Wiggins, C.C.; Shepherd, J.R.A.; et al. Early safety indicators of COVID-19 convalescent plasma in 5000 patients. J. Clin. Investig. 2020, 130, 4791–4797. [Google Scholar] [CrossRef]
- Chung, J.Y.; Thone, M.N.; Kwon, Y.J. COVID-19 vaccines: The status and perspectives in delivery points of view. Adv. Drug Deliv. Rev. 2021, 170, 1–25. [Google Scholar] [CrossRef]
- Cheng, Y.; Wong, R.; Soo, Y.O.Y.; Wong, W.S.; Lee, C.K.; Ng, M.H.L.; Chan, P.; Wong, K.C.; Leung, C.B.; Cheng, G. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 44–46. [Google Scholar] [CrossRef]
- Ko, J.H.; Seok, H.; Cho, S.Y.; Ha, Y.E.; Baek, J.Y.; Kim, S.H.; Kim, Y.J.; Park, J.K.; Chung, C.R.; Kang, E.S.; et al. Challenges of convalescent plasma infusion therapy in Middle East respiratory coronavirus infection: A single centre experience. Antivir. Ther. 2018, 23, 617–622. [Google Scholar] [CrossRef]
- Li, L.; Zhang, W.; Hu, Y.; Tong, X.; Zheng, S.; Yang, J.; Kong, Y.; Ren, L.; Wei, Q.; Mei, H.; et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients with Severe and Life-threatening COVID-19: A Randomized Clinical Trial. Jama 2020, 324, 460–470. [Google Scholar] [CrossRef]
- Arciuolo, R.J.; Jablonski, R.R.; Zucker, J.R.; Rosen, J.B. Effectiveness of Measles Vaccination and Immune Globulin Post-Exposure Prophylaxis in an Outbreak Setting—New York City, 2013. Clin. Infect. Dis. 2017, 65, 1843–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de Sanidad. Documento Técnico Manejo Clínico del COVID-19: Atención Hospitalaria; Ministerio de Sanidad Gobierno de España: Madrid, Spain, 2020. [Google Scholar]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Final Report. N. Engl. J. Med. 2020, 383, 2085–2098. [Google Scholar] [CrossRef] [PubMed]
- Shih, W.J.; Shen, X.; Zhang, P.; Xie, T. Remdesivir is effective for moderately severe patients: A re-analysis of the first double-blind, placebo-controlled, randomized trial on remdesivir for treatment of severe covid-19 patients conducted in wuhan city. Open Access J. Clin. Trials 2020, 12, 15–21. [Google Scholar] [CrossRef]
- World Health Organization. WHO R&D Blueprint: Novel Coronavirus: Outline of Trial Designs for Experimental Therapeutics; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Libster, R.; Pérez Marc, G.; Wappner, D.; Coviello, S.; Bianchi, A.; Braem, V.; Esteban, I.; Caballero, M.T.; Wood, C.; Berrueta, M.; et al. Early High-Titer Plasma Therapy to Prevent Severe Covid-19 in Older Adults. N. Engl. J. Med. 2021, 384, 610–618. [Google Scholar] [CrossRef]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Convalescent plasma in patients admitted to hospital with COVID-19 (RECOVERY): A randomised controlled, open-label, platform trial. Lancet 2021, 397, S0140–S6736. [Google Scholar] [CrossRef]
- Salazar, E.; Perez, K.K.; Ashraf, M.; Chen, J.; Castillo, B.; Christensen, P.A.; Eubank, T.; Bernard, D.W.; Eagar, T.N.; Long, S.W.; et al. Treatment of Coronavirus Disease 2019 (COVID-19) Patients with Convalescent Plasma. Am. J. Pathol. 2020, 190, 1680–1690. [Google Scholar] [CrossRef]
- Avendaño-Solà, C.; Ramos-Martínez, A.; Muñez-Rubio, E.; Ruiz-Antorán, B.; de Molina, R.M.; Torres, F.; Fernández-Cruz, A.; Callejas-Díaz, A.; Calderón, J.; Payares-Herrera, C.; et al. Convalescent Plasma for COVID-19: A multicenter, randomized clinical trial. medRxiv 2020. [Google Scholar] [CrossRef]
- Rojas, M.; Rodríguez, Y.; Monsalve, D.M.; Acosta-Ampudia, Y.; Camacho, B.; Gallo, J.E.; Anaya, J.M. Convalescent plasma in Covid-19: Possible mechanisms of action. Autoimmun. Rev. 2020, 19, 102554. [Google Scholar] [CrossRef]
- Jorda, A.; Kussmann, M.; Kolenchery, N.; Siller-Matula, J.M.; Zeitlinger, M.; Jilma, B.; Gelbenegger, G. Convalescent Plasma Treatment in Patients with Covid-19: A Systematic Review and Meta-Analysis. Front. Immunol. 2022, 13, 817829. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Burgos Pratx, L.D.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vázquez, C.; Savoy, N.; Giunta, D.H.; Pérez, L.G.; Sánchez, M.d.L.; et al. A Randomized Trial of Convalescent Plasma in Covid-19 Severe Pneumonia. N. Engl. J. Med. 2021, 384, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Faqihi, F.; Alharthy, A.; Abdulaziz, S.; Balhamar, A.; Alomari, A.; AlAseri, Z.; Tamim, H.; Alqahtani, S.A.; Kutsogiannis, D.J.; Brindley, P.G.; et al. Therapeutic plasma exchange in patients with life-threatening COVID-19: A randomised controlled clinical trial. Int. J. Antimicrob. Agents 2021, 57, 106334. [Google Scholar] [CrossRef] [PubMed]
- Estcourt, L.J.; Turgeon, A.F.; McQuilten, Z.K.; McVerry, B.J.; Al-Beidh, F.; Annane, D.; Arabi, Y.M.; Arnold, D.M.; Beane, A.; Bégin, P.; et al. Effect of Convalescent Plasma on Organ Support-Free Days in Critically Ill Patients with COVID-19: A Randomized Clinical Trial. JAMA 2021, 326, 1690–1702. [Google Scholar] [PubMed]
- Salazar, E.; Christensen, P.A.; Graviss, E.A.; Nguyen, D.T.; Castillo, B.; Chen, J.; Lopez, B.V.; Eagar, T.N.; Yi, X.; Zhao, P.; et al. Treatment of Coronavirus Disease 2019 Patients with Convalescent Plasma Reveals a Signal of Significantly Decreased Mortality. Am. J. Pathol. 2020, 190, 2290–2303. [Google Scholar] [CrossRef]
- Balcells, M.E.; Rojas, L.; Le Corre, N.; Martínez-Valdebenito, C.; Ceballos, M.E.; Ferrés, M.; Chang, M.; Vizcaya, C.; Mondaca, S.; Huete, Á.; et al. Early versus deferred anti-SARS-CoV-2 convalescent plasma in patients admitted for COVID-19: A randomized phase II clinical trial. PLoS Med. 2021, 18, e1003415. [Google Scholar] [CrossRef]
- Liu, S.T.H.; Lin, H.M.; Baine, I.; Wajnberg, A.; Gumprecht, J.P.; Rahman, F.; Rodriguez, D.; Tandon, P.; Bassily-Marcus, A.; Bander, J.; et al. Convalescent plasma treatment of severe COVID-19: A propensity score–matched control study. Nat. Med. 2020, 26, 1708–1713. [Google Scholar] [CrossRef]
- Acosta-Ampudia, Y.; Monsalve, D.M.; Rojas, M.; Rodríguez, Y.; Gallo, J.E.; Salazar-Uribe, J.C.; Santander, M.J.; Cala, M.P.; Zapata, W.; Zapata, M.I.; et al. COVID-19 convalescent plasma composition and immunological effects in severe patients. J. Autoimmun. 2021, 118, 102598. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epidemiological and Baseline Parameters | PG (n = 37) | CG (n = 17) | Epidemiological and Baseline Parameters | PG (n = 37) | CG (n = 17) |
|---|---|---|---|---|---|
| Age (years) | 58 ± 2 | 59 ± 3 | Concomitant medication | ||
| Sex | Yes | 17/37 (45.9%) | 7/17 (41.2%) | ||
| Women | 14/37 (37%) | 7/17 (41%) | No | 20/37 (54.1%) | 10/37 (58.8%) |
| Men | 23/37 (63%) | 10/17 (59%) | Smoke | ||
| BMI | 30.72 ± 1.24 | 30.34 ± 1.99 | Yes | 2/37 (6%) | 1/17 (6%) |
| No | 30/37 (94%) | 16/17 (94%) | |||
| Abuse drugs | |||||
| Concomitant ilnesses | Yes | 2/37 (6%) | 1/17 (6%) | ||
| Yes | 27/37 (73%) | 14/17 (80%) | No | 30/37 (94%) | 16/17 (94%) |
| No | 10/37 (27%) | 3/17 (20%) | Standard treatment | ||
| Type of disease | Antiinflammatorory | 29/37 (34.1%) | 11/17 (32.3%) | ||
| Cardiac diseases | 32 (86.5) | 16 (94.1) | Antiviral | 14/37 (16.5%) | 5/17 (14.7%) |
| Respiratory diseases | 10 (27) | 6 (35.3) | Antiobiotic | 10/37 (11.8%) | 3/17 (8.8%) |
| Digestive diseases | 3 (8.1) | 3 (17.6) | Anticoagulant | 13/37 (15.3%) | 5/17 (14.7%) |
| Neurological diseases | 8 (21.6) | 5 (29.4) | Oxygen theraphy | 19/37 (22.3%) | 10/17 (29.4%) |
| Psychiatric diseases | 0 (0) | 5 (29.4) | |||
| Nephrological diseases | 8 (21.6) | 3 (17.6) | |||
| Oftalmological diseases | 1 (2.7) | 2 (11.8) | |||
| Dermatological diseases | 0 (0) | 1 (5.9) | |||
| Endocrinological diseases | 36 (97.3) | 15 (88.2) | |||
| Rheumatic/osteoarticular diseases | 5 (13.5) | 5 (29.4) | |||
| Inmunitary diseases | 0 (0) | 1 (5.9) |
| Clinical Parameters | PG (n = 37) | CG (n = 17) |
|---|---|---|
| Stay in hospital (days) | 8.9 ± 0.88 | 10.5 ± 1.84 |
| Time to negativization (days to achieve negative PCR) | 12.4 ± 2.14 | 14.6 ± 1.40 |
| AAEE(n/N total) % | 4/37 (10.8%) | |
| Type of AAEE | ||
| Skin rash (Grade 1) | 1/37 (2.7%) | |
| Left ear hearing los | 1/37 (2.7%) | |
| Mild dizziness | 1/37 (2.7%) | |
| Left hypochondrium pain | 1/37 (2.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bargay-Lleonart, J.; Sarubbo, F.; Arrizabalaga, M.; Guerra, J.M.; Borràs, J.; El Haji, K.; Flexas, M.; Perales, J.; Fernández-Baca, V.; Gallegos, C.; et al. Reinforcement of the Standard Therapy with Two Infusions of Convalescent Plasma for Patients with COVID-19: A Randomized Clinical Trial. J. Clin. Med. 2022, 11, 3039. https://doi.org/10.3390/jcm11113039
Bargay-Lleonart J, Sarubbo F, Arrizabalaga M, Guerra JM, Borràs J, El Haji K, Flexas M, Perales J, Fernández-Baca V, Gallegos C, et al. Reinforcement of the Standard Therapy with Two Infusions of Convalescent Plasma for Patients with COVID-19: A Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(11):3039. https://doi.org/10.3390/jcm11113039
Chicago/Turabian StyleBargay-Lleonart, Joan, Fiorella Sarubbo, Maria Arrizabalaga, José Maria Guerra, Josep Borràs, Khaoulah El Haji, Magdalena Flexas, Jorge Perales, Victoria Fernández-Baca, Carmen Gallegos, and et al. 2022. "Reinforcement of the Standard Therapy with Two Infusions of Convalescent Plasma for Patients with COVID-19: A Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 11: 3039. https://doi.org/10.3390/jcm11113039