
Triglyceride-Glucose Index for Early Prediction of Nonalcoholic Fatty Liver Disease: A Meta-Analysis of 121,975 Individuals

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Outcomes of Interest
2.5. Statistical Analysis
2.6. Quality Assessment
3. Results
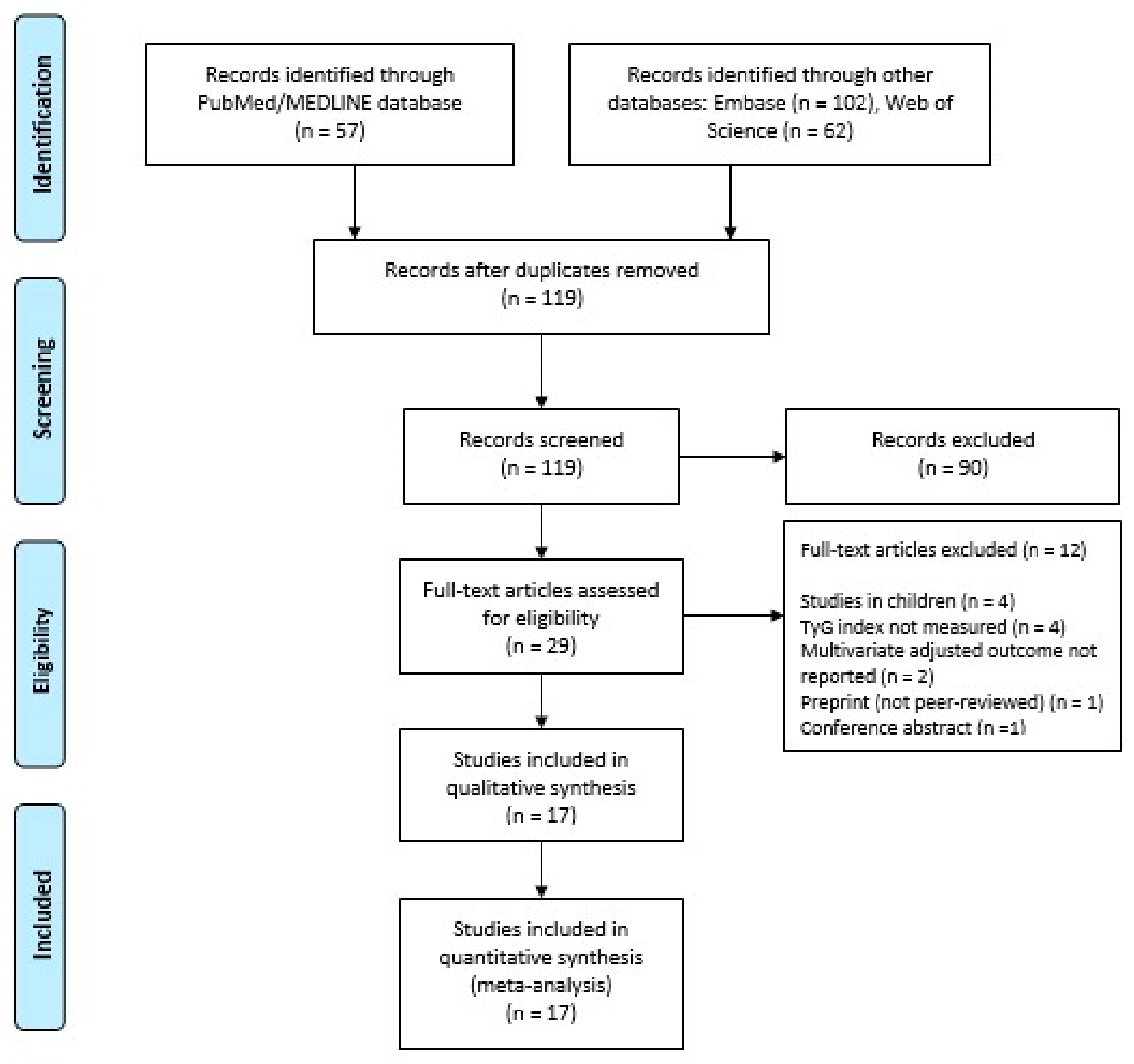
3.1. Study Selection
3.2. Study and Participants’ Characteristics
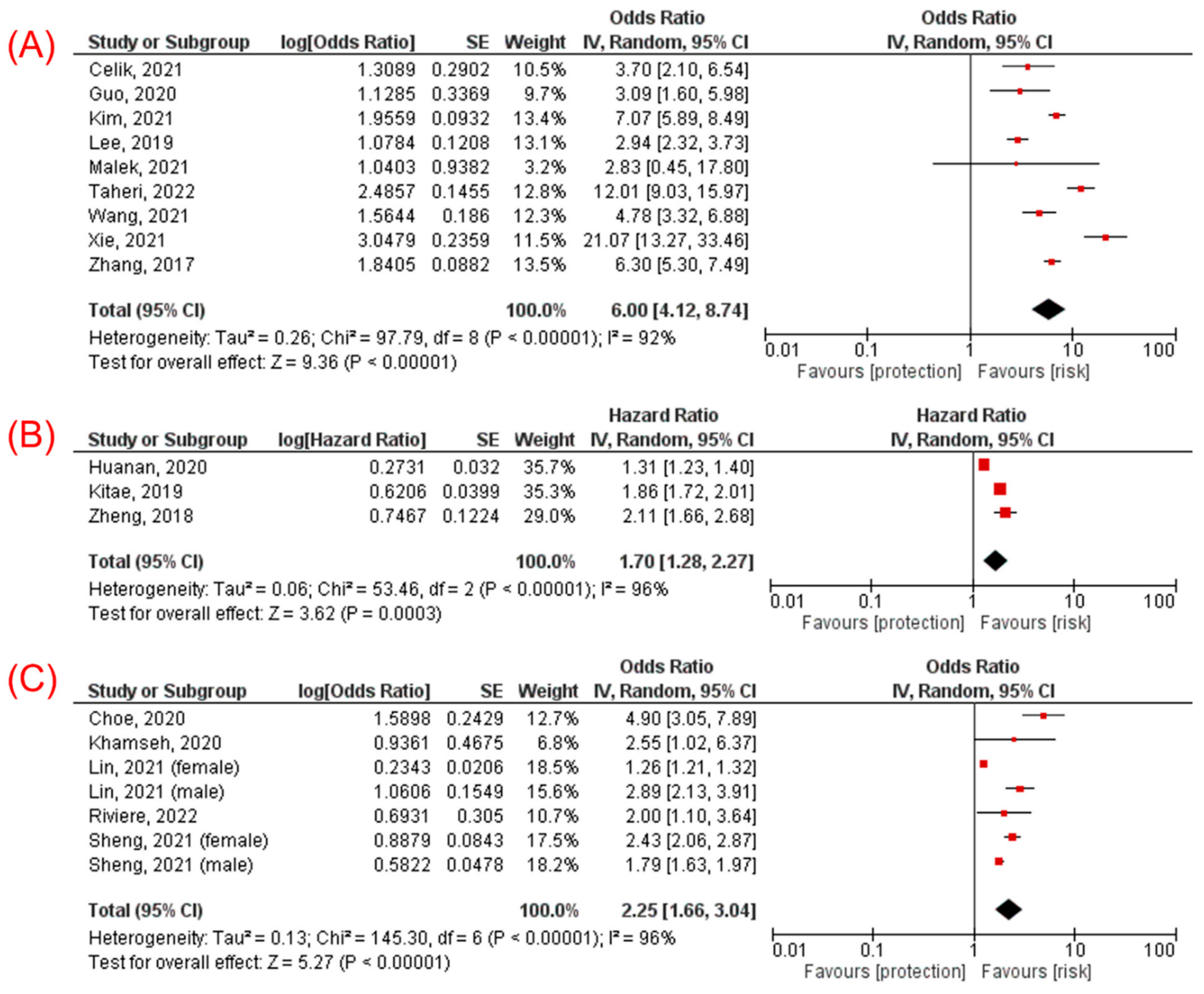
3.3. TyG Index and Incidence of NAFLD
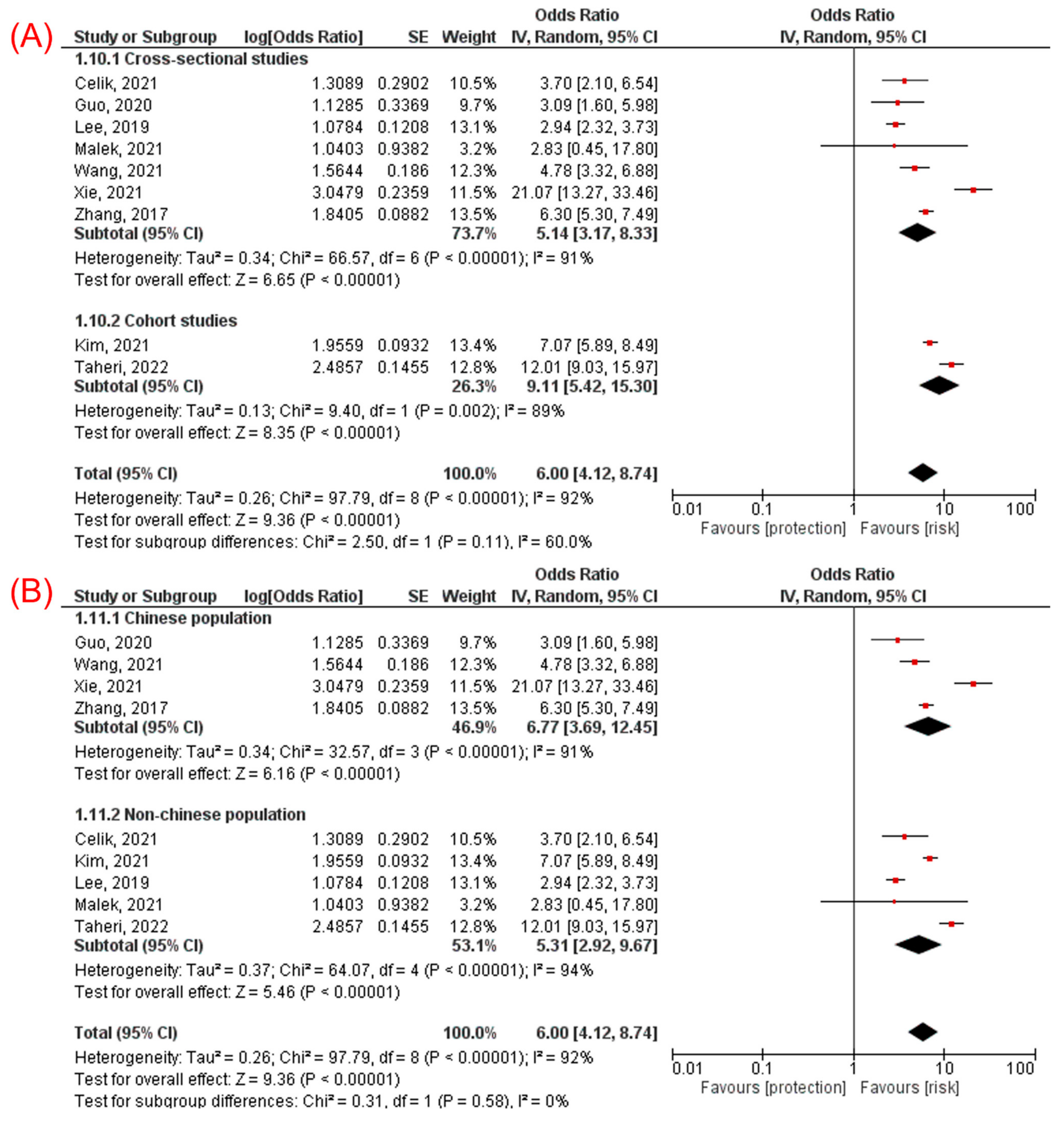
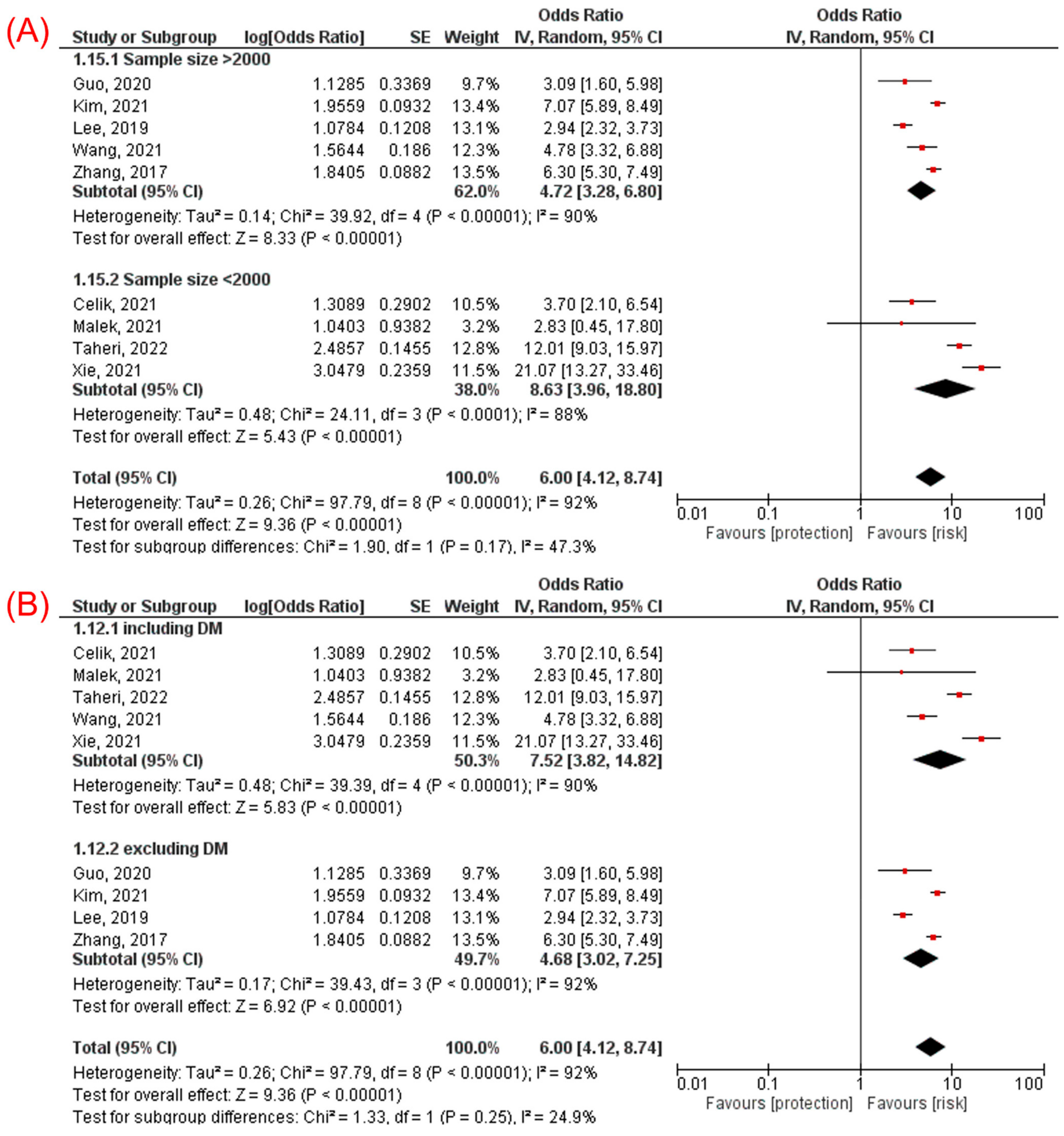
3.3.1. TyG Index Analyzed as a Categorical Variable
3.3.2. TyG Index Analyzed as a Continuous Variable
3.4. Sensitivity Analysis
3.5. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, R.; Priyadarshi, R.N.; Anand, U. Non-alcoholic Fatty Liver Disease: Growing Burden, Adverse Outcomes and Associations. J. Clin. Transl. Hepatol. 2020, 8, 76–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwak, M.S.; Kim, D. Non-alcoholic fatty liver disease and lifestyle modifications, focusing on physical activity. Korean J. Intern. Med. 2018, 33, 64–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhtar, D.H.; Iqbal, U.; Vazquez-Montesino, L.M.; Dennis, B.B.; Ahmed, A. Pathogenesis of Insulin Resistance and Atherogenic Dyslipidemia in Nonalcoholic Fatty Liver Disease. J. Clin. Transl. Hepatol. 2019, 7, 362–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerrero-Romero, F.; Villalobos-Molina, R.; Jiménez-Flores, J.R.; Simental-Mendia, L.E.; Méndez-Cruz, R.; Murguía-Romero, M.; Rodríguez-Morán, M. Fasting Triglycerides and Glucose Index as a Diagnostic Test for Insulin Resistance in Young Adults. Arch. Med. Res. 2016, 47, 382–387. [Google Scholar] [CrossRef]
- Son, D.H.; Lee, H.S.; Lee, Y.J.; Lee, J.H.; Han, J.H. Comparison of triglyceride-glucose index and HOMA-IR for predicting prevalence and incidence of metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 596–604. [Google Scholar] [CrossRef]
- Toro-Huamanchumo, C.J.; Urrunaga-Pastor, D.; Guarnizo-Poma, M.; Lazaro-Alcantara, H.; Paico-Palacios, S.; Pantoja-Torres, B.; Ranilla-Seguin, V.D.C.; Benites-Zapata, V.A. Triglycerides and glucose index as an insulin resistance marker in a sample of healthy adults. Diabetes Metab. Syndr. 2019, 13, 272–277. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; González-Ortiz, M.; Martínez-Abundis, E.; Ramos-Zavala, M.G.; Hernández-González, S.O.; Jacques-Camarena, O.; Rodríguez-Morán, M. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J. Clin. Endocrinol. Metab. 2010, 95, 3347–3351. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-García, A.; Rodríguez-Gutiérrez, R.; Mancillas-Adame, L.; González-Nava, V.; Díaz González-Colmenero, A.; Solis, R.C.; Álvarez-Villalobos, N.A.; González-González, J.G. Diagnostic Accuracy of the Triglyceride and Glucose Index for Insulin Resistance: A Systematic Review. Int. J. Endocrinol. 2020, 2020, 4678526. [Google Scholar] [CrossRef]
- Simental-Mendía, L.E.; Simental-Mendía, E.; Rodríguez-Hernández, H.; Rodríguez-Morán, M.; Guerrero-Romero, F. The product of triglycerides and glucose as biomarker for screening simple steatosis and NASH in asymptomatic women. Ann. Hepatol. 2016, 15, 715–720. [Google Scholar]
- Zhang, S.; Du, T.; Zhang, J.; Lu, H.; Lin, X.; Xie, J.; Yang, Y.; Yu, X. The triglyceride and glucose index (TyG) is an effective biomarker to identify nonalcoholic fatty liver disease. Lipids Health Dis. 2017, 16, 15. [Google Scholar] [CrossRef] [Green Version]
- Taheri, E.; Pourhoseingholi, M.A.; Moslem, A.; Hassani, A.H.; Mousavi Jarrahi, A.; Asadzadeh Aghdaei, H.; Zali, M.R.; Hatami, B. The triglyceride-glucose index as a clinical useful marker for metabolic associated fatty liver disease (MAFLD): A population-based study among Iranian adults. J. Diabetes Metab. Disord. 2022. [Google Scholar] [CrossRef]
- Khamseh, M.E.; Malek, M.; Abbasi, R.; Taheri, H.; Lahouti, M.; Alaei-Shahmiri, F. Triglyceride Glucose Index and Related Parameters (Triglyceride Glucose-Body Mass Index and Triglyceride Glucose-Waist Circumference) Identify Nonalcoholic Fatty Liver and Liver Fibrosis in Individuals with Overweight/Obesity. Metab. Syndr. Relat. Disord. 2021, 19, 167–173. [Google Scholar] [CrossRef]
- Huanan, C.; Sangsang, L.; Amoah, A.N.; Yacong, B.; Xuejiao, C.; Zhan, S.; Guodong, W.; Jian, H.; Songhe, S.; Quanjun, L. Relationship between triglyceride glucose index and the incidence of non-alcoholic fatty liver disease in the elderly: A retrospective cohort study in China. BMJ Open 2020, 10, e039804. [Google Scholar] [CrossRef]
- Guo, W.; Lu, J.; Qin, P.; Li, X.; Zhu, W.; Wu, J.; Xu, N.; Zhang, Q. The triglyceride-glucose index is associated with the severity of hepatic steatosis and the presence of liver fibrosis in non-alcoholic fatty liver disease: A cross-sectional study in Chinese adults. Lipids Health Dis. 2020, 19, 218. [Google Scholar] [CrossRef] [PubMed]
- Malek, M.; Khamseh, M.E.; Chehrehgosha, H.; Nobarani, S.; Alaei-Shahmiri, F. Triglyceride glucose-waist to height ratio: A novel and effective marker for identifying hepatic steatosis in individuals with type 2 diabetes mellitus. Endocrine 2021, 74, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Çelik, M.; Ahbab, S.; Hoca, E.; Ataoglu, H.E. The Assessment of Insulin Resistance and Triglyceride/Glucose Index in Nonalcoholic Fatty Liver Disease. South Clin. Ist. Eurasia 2021, 32, 381–387. [Google Scholar]
- Choe, A.R.; Ryu, D.R.; Kim, H.Y.; Lee, H.A.; Lim, J.; Kim, J.S.; Lee, J.K.; Kim, T.H.; Yoo, K. Noninvasive indices for predicting nonalcoholic fatty liver disease in patients with chronic kidney disease. BMC Nephrol. 2020, 21, 50. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Cho, Y.K.; Kim, E.H.; Lee, M.J.; Jung, C.H.; Park, J.Y.; Kim, H.K.; Lee, W.J. Triglyceride Glucose-Waist Circumference Is Superior to the Homeostasis Model Assessment of Insulin Resistance in Identifying Nonalcoholic Fatty Liver Disease in Healthy Subjects. J. Clin. Med. 2021, 11, 41. [Google Scholar] [CrossRef]
- Kitae, A.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. The Triglyceride and Glucose Index Is a Predictor of Incident Nonalcoholic Fatty Liver Disease: A Population-Based Cohort Study. Can. J. Gastroenterol. Hepatol. 2019, 2019, 5121574. [Google Scholar] [CrossRef] [Green Version]
- Rivière, B.; Jaussent, A.; Macioce, V.; Faure, S.; Builles, N.; Lefebvre, P.; Géraud, P.; Picot, M.C.; Rebuffat, S.; Renard, E.; et al. The triglycerides and glucose (TyG) index: A new marker associated with nonalcoholic steatohepatitis (NASH) in obese patients. Diabetes Metab. 2022, 48, 101345. [Google Scholar] [CrossRef]
- Lee, S.B.; Kim, M.K.; Kang, S.; Park, K.; Kim, J.H.; Baik, S.J.; Nam, J.S.; Ahn, C.W.; Park, J.S. Triglyceride Glucose Index Is Superior to the Homeostasis Model Assessment of Insulin Resistance for Predicting Nonalcoholic Fatty Liver Disease in Korean Adults. Endocrinol. Metab. 2019, 34, 179–186. [Google Scholar] [CrossRef]
- Lin, I.T.; Lee, M.Y.; Wang, C.W.; Wu, D.W.; Chen, S.C. Gender Differences in the Relationships among Metabolic Syndrome and Various Obesity-Related Indices with Nonalcoholic Fatty Liver Disease in a Taiwanese Population. Int. J. Environ. Res. Public Health 2021, 18, 857. [Google Scholar] [CrossRef]
- Wang, J.; Su, Z.; Feng, Y.; Xi, R.; Liu, J.; Wang, P. Comparison of several blood lipid-related indexes in the screening of non-alcoholic fatty liver disease in women: A cross-sectional study in the Pearl River Delta region of southern China. BMC Gastroenterol. 2021, 21, 482. [Google Scholar] [CrossRef]
- Xie, F.; Pei, Y.; Zhou, Q.; Cao, D.; Wang, Y. Comparison of obesity-related indices for identifying nonalcoholic fatty liver disease: A population-based cross-sectional study in China. Lipids Health Dis. 2021, 20, 132. [Google Scholar] [CrossRef]
- Zheng, R.; Du, Z.; Wang, M.; Mao, Y.; Mao, W. A longitudinal epidemiological study on the triglyceride and glucose index and the incident nonalcoholic fatty liver disease. Lipids Health Dis. 2018, 17, 262. [Google Scholar] [CrossRef]
- Sheng, G.; Lu, S.; Xie, Q.; Peng, N.; Kuang, M.; Zou, Y. The usefulness of obesity and lipid-related indices to predict the presence of Non-alcoholic fatty liver disease. Lipids Health Dis. 2021, 20, 134. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Colombo, M.; Cortez-Pinto, H.; Huang, T.T.K.; Miller, V.; Ninburg, M.; Schattenberg, J.M.; Seim, L.; Wong, V.W.S.; Zelber-Sagi, S. NAFLD—sounding the alarm on a silent epidemic. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.P.; Patel, J.; Byrne, C.D. Causes of Mortality in Non-Alcoholic Fatty Liver Disease (NAFLD) and Alcohol Related Fatty Liver Disease (AFLD). Curr. Pharm. Des. 2020, 26, 1079–1092. [Google Scholar] [CrossRef] [PubMed]
- Utzschneider, K.M.; Kahn, S.E. Review: The role of insulin resistance in nonalcoholic fatty liver disease. J. Clin. Endocrinol. Metab. 2006, 91, 4753–4761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonora, E.; Targher, G.; Alberiche, M.; Bonadonna, R.C.; Saggiani, F.; Zenere, M.B.; Monauni, T.; Muggeo, M. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: Studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care 2000, 23, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Kang, B.; Yang, Y.; Lee, E.Y.; Yang, H.K.; Kim, H.S.; Lim, S.Y.; Lee, J.H.; Lee, S.S.; Suh, B.K.; Yoon, K.H. Triglycerides/glucose index is a useful surrogate marker of insulin resistance among adolescents. Int. J. Obes. 2017, 41, 789–792. [Google Scholar] [CrossRef]
- Tutunchi, H.; Naeini, F.; Mobasseri, M.; Ostadrahimi, A. Triglyceride glucose (TyG) index and the progression of liver fibrosis: A cross-sectional study. Clin. Nutr. ESPEN 2021, 44, 483–487. [Google Scholar] [CrossRef]
- Amzolini, A.M.; Forţofoiu, M.C.; Barău Abu-Alhija, A.; Vladu, I.M.; Clenciu, D.; Mitrea, A.; Forţofoiu, M.; Matei, D.; Enăchescu, V.; Predescu, O.I.; et al. Triglyceride and glucose index: A useful tool for non-alcoholic liver disease assessed by liver biopsy in patients with metabolic syndrome? Rom. J. Morphol. Embryol. 2021, 62, 475–480. [Google Scholar] [CrossRef]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: A meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year | Study Design | Country | Participant Characteristics | Exclusion Criteria | Total Participants, n | Male, n (%) | Mean Age, Years | Mean BMI, kg/m2 | Incidence of NAFLD, n (%) | Liver Fibrosis, n (%) | Diagnosis of NAFLD | TyG Index Analysis | Variables Adjusted | Follow-Up Period |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Celik, 2021 [21] | Retrospective CS | Turkey | General population | alcohol abuse, chronic liver disease, acute abdomen, ESRD, sepsis, cancer, and neuropsychiatric diseases | 986 | 232 (23.5) | 55.9 | NR | 470 (47.7) | NR | Ultrasound | Categorized (Step 5a:Step 1a) | Age, ALT, AST, LDL, HDL, DM, and prediabetes | NR |
| Choe, 2020 [22] | CS | Korea | Patients with CKD | alcohol abuse, viral hepatitis, other chronic liver diseases | 819 | 682 (83.3) | 64.6 | 25 | 140 (17.1) | NR | Ultrasound | Continuous | Age, gender, BMI, HTN, DM, HLD, eGFR, log creatinine, RRT, EPO use, log WBC, Hb, PLT, log AST, log ALT, log TB, albumin, log CRP, log TG, TC, HbA1C, log FG | NR |
| Guo, 2020 [14] | CS | China | General population | alcohol abuse, HLD, DM, viral hepatitis, chronic liver disease, hyperthyroidism, kidney disease | 4784 | 3231 (67.5) | 48.96 | 24.9 | 2902 (60.7) | 550 out of 2352 (23.4%) | Ultrasound | Categorized (Q4–Q1) | BMI, HbA1c ALT, AST and GGT | NR |
| Huanan, 2020 [13] | RC | China | General population | alcohol abuse, viral hepatitis, chronic liver disease, including NAFLD | 46,693 | 22,932 (49.1) | 68.1 | 24.82 | 5660 (12.1) | NR | Ultrasound | Categorized (Q4–Q1) | Age, sex, smoking, exercise, SBP, DBP, waist ratio, ALT, AST, T. bili, T. cholesterol, DM | 3.2 years |
| Khamseh, 2020 [12] | CS | Iran | General population | alcohol abuse, DM, viral hepatitis, chronic liver disease, pregnant or breastfeeding women | 184 | NR | 44.7 | 30.5 | 96 (52.2) | NR | Ultrasound | Continuous | Age, gender, hip, SBP, DBP, ALT, AST, cholesterol, HOMA-IR, statin, smoking | NR |
| Kim, 2021 [23] | RC | Korea | General population | alcohol abuse, DM, viral hepatitis, HLD | 10,585 | 6326 (59.8) | 47.8 | 23.6 | 3284 (51.9) | NR | Ultrasound | Categorized (Q4:Q1) | NR | NR |
| Kitae, 2019 [24] | PC | Japan | General population | alcohol abuse, viral hepatitis, and chronic liver disease including NAFLD | 14,086 | 6823 (48.4) | 40 | 21.2 | 2670 (39.1) | NR | Ultrasound | Categorized (T3:T1) | Age, ALT, BMI, alcohol consumption, exercise, and smoking | 1881 (IQR 2771) days in men and 2198 (IQR 2645) in women |
| Lee, 2019 [26] | CS | Korea | General population | alcohol abuse, hypertriglyceridemia, chronic liver disease, viral hepatitis, cancer, DM, acute inflammation, and renal or infectious disease | 4986 | 2979 (59.7) | 52.63 | 23.82 | 2069 (41.5) | NR | Ultrasound | Categorized (Q4:Q1) | Age, sex, BMI, SBP, TC, HDL, ALT, HTN | NR |
| Lin, 2021 [27] | CS | Taiwan | General population | alcohol abuse and viral hepatitis | 1969 | 764 (38.4) | 55.1 | 25.3 | 826 (42) | NR | Ultrasound | Continuous | Age, AST, ALT, T. Cholesterol, Hemoglobin, GFR, uric acid | NR |
| Malek, 2021 [15] | CS | Iran | Patients with T2DM | alcohol abuse, hepatitis, chronic liver disease, liver masses, and pregnant or breastfeeding women | 175 | 80 (45.7) | 48.3 | 29.55 | 122 (69.7) | NR | Elastography (FibroScan) | Categorized (Q4:Q1) | age, gender | NR |
| Riviere, 2022 [25] | Cohort | France | Patients with obesity | alcohol abuse, DM except T2DM, previous bariatric surgery except LAGB, chronic inflammatory disease and cancer | 238 | 80 (33.6) | 43 | 42 | 160 (67.2) | 68 (28.6%) | Liver biopsy | Continuous | sex, age, BMI, AST, GGT | NR |
| Sheng, 2021 [31] | CS | China | General population | alcohol abuse, chronic liver disease including NAFLD, viral hepatitis, and impaired glucose tolerance | 14,251 | 7411 (52) | 44.6 | 23.45 | 2507 (17.6) | NR | Ultrasound | Continuous | GGT, age, drinking status, HbA1c, TC, smoking status, HDL-C, habit of exercise, and DBP | NR |
| Taheri, 2022 [11] | RC | Iran | General population | alcohol abuse, cancer, IBD, transplant patients, viral hepatitis, chronic liver disease, pregnant or breastfeeding women | 1932 | 756 (39.1) | 48.98 | 28.54 | 968 (50.1) | NR | fatty liver index | Categorized (T1–T3) | age, sex, smoking, physical activity level, WHR, SPB, DBP, ALT, and TC levels | NR |
| Wang, 2021 [28] | CS | China | General population (women) | alcohol abuse and viral or autoimmune hepatitis | 3239 | None | 58.2 | 25.4 | 2257 (69.7) | NR | Ultrasound | Categorized (Q1–Q4) | Age, medical history, SBP, DBP, BMI, RBC, WBC, PLT, FPG, HbA1c, ALT, AST, ALP, BUN, GGT, TBIL, Cr, BUN, UA | NR |
| Xie, 2021 [29] | CS | China | General population | alcohol abuse and chronic liver disease | 1748 | 1153 (66) | 44.5 | 24.6 | 526 (30.1) | NR | Ultrasound | Categorized (Q1–Q4) | Age and gender | NR |
| Zhang, 2017 [10] | CS | China | General population | alcohol abuse, viral hepatitis, chronic liver disease, DM and HLD | 10,761 | 6758 (62.8) | 49.5 | 23.9 | 4349 (64.4) | NR | Ultrasound | Categorized (Q1–Q4) | Age, gender, ALT | NR |
| Zheng, 2018 [30] | PC | China | General population | alcohol abuse, chronic liver disease, HTN, DM, HLD, and multiple sclerosis | 4539 | 2996 (66) | 41 | 22.7 | 1390 (30.6) | NR | Ultrasound | Categorized (Q4:Q1) | BMI, WC, gender, SBP, age, DBP, TC, TG, Apo-A1, Apo-B, LDL-C, FPG, BUN, Cr, HDL-C, AST, ALT, UA, y-GGT and eGFR | 9 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beran, A.; Ayesh, H.; Mhanna, M.; Wahood, W.; Ghazaleh, S.; Abuhelwa, Z.; Sayeh, W.; Aladamat, N.; Musallam, R.; Matar, R.; et al. Triglyceride-Glucose Index for Early Prediction of Nonalcoholic Fatty Liver Disease: A Meta-Analysis of 121,975 Individuals. J. Clin. Med. 2022, 11, 2666. https://doi.org/10.3390/jcm11092666
Beran A, Ayesh H, Mhanna M, Wahood W, Ghazaleh S, Abuhelwa Z, Sayeh W, Aladamat N, Musallam R, Matar R, et al. Triglyceride-Glucose Index for Early Prediction of Nonalcoholic Fatty Liver Disease: A Meta-Analysis of 121,975 Individuals. Journal of Clinical Medicine. 2022; 11(9):2666. https://doi.org/10.3390/jcm11092666
Chicago/Turabian StyleBeran, Azizullah, Hazem Ayesh, Mohammed Mhanna, Waseem Wahood, Sami Ghazaleh, Ziad Abuhelwa, Wasef Sayeh, Nameer Aladamat, Rami Musallam, Reem Matar, and et al. 2022. "Triglyceride-Glucose Index for Early Prediction of Nonalcoholic Fatty Liver Disease: A Meta-Analysis of 121,975 Individuals" Journal of Clinical Medicine 11, no. 9: 2666. https://doi.org/10.3390/jcm11092666