
Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension in Greece: Data from the Hellenic Pulmonary Hypertension Registry

 ,
,  ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
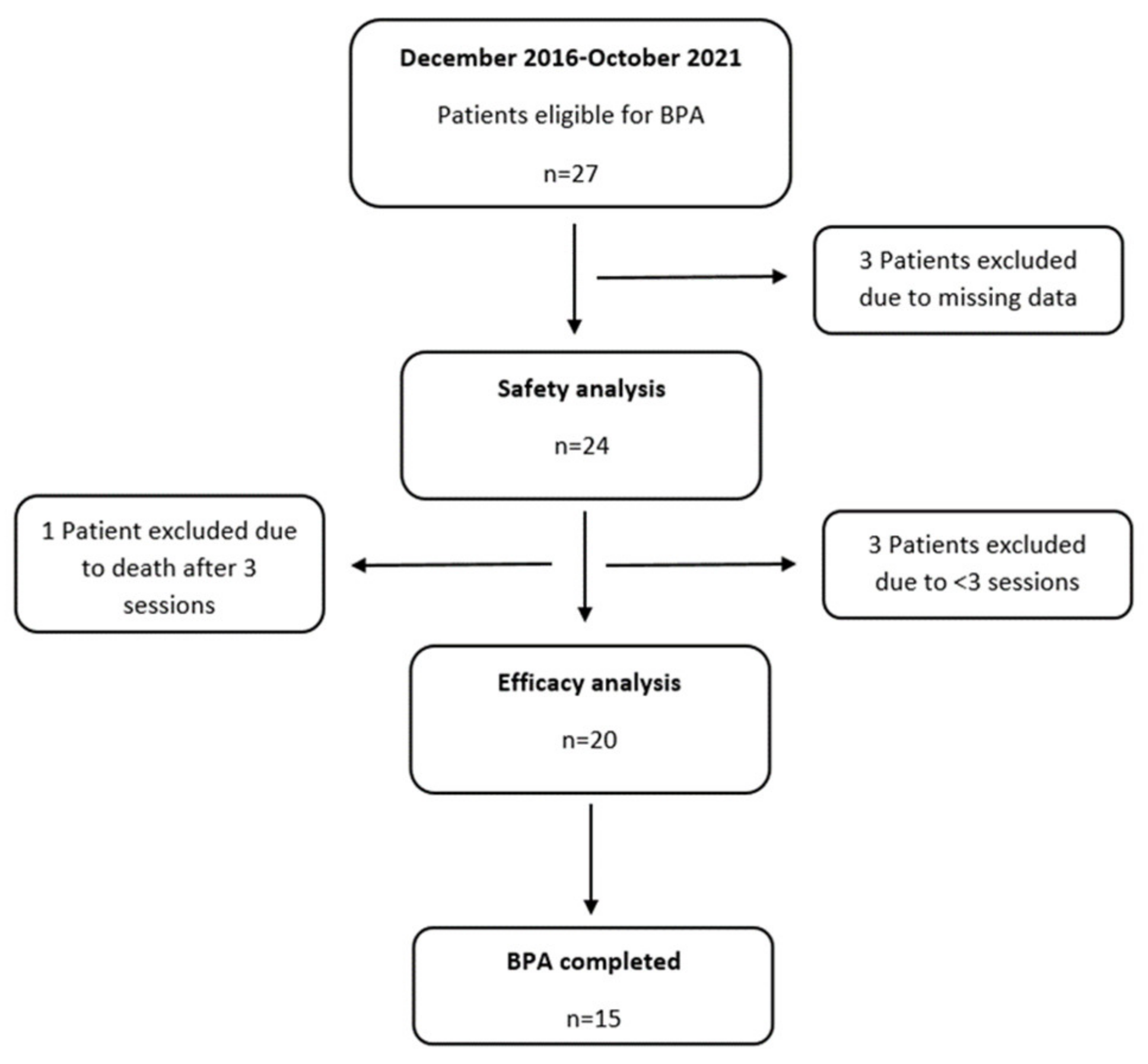
2. Materials and Methods
2.1. Patients’ Characteristics
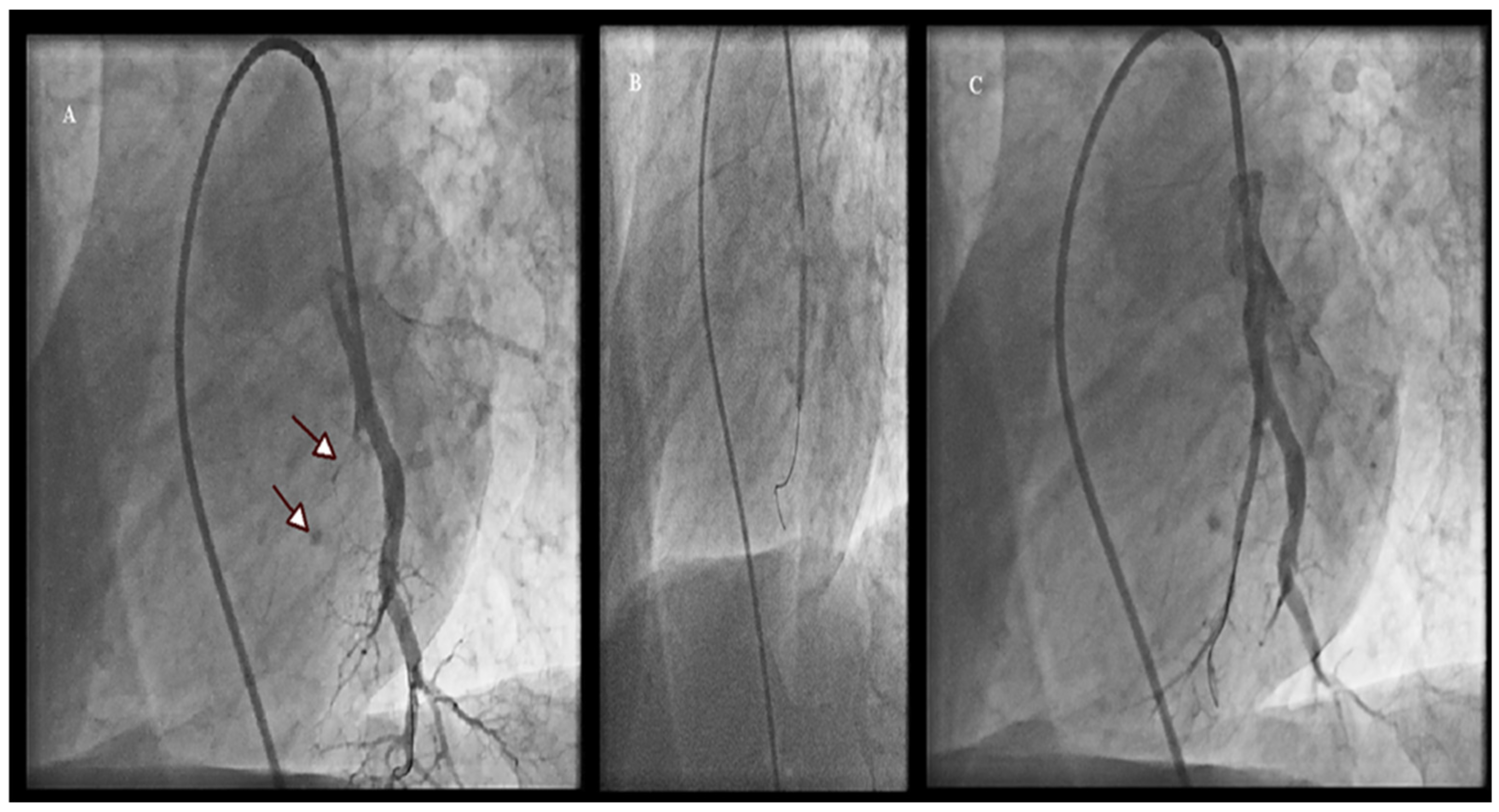
2.2. BPA Procedure
2.3. Definition of Complications Related to BPA
2.4. Statistical Analysis
2.5. Outcomes of BPA
3. Results
3.1. Patient Characteristics
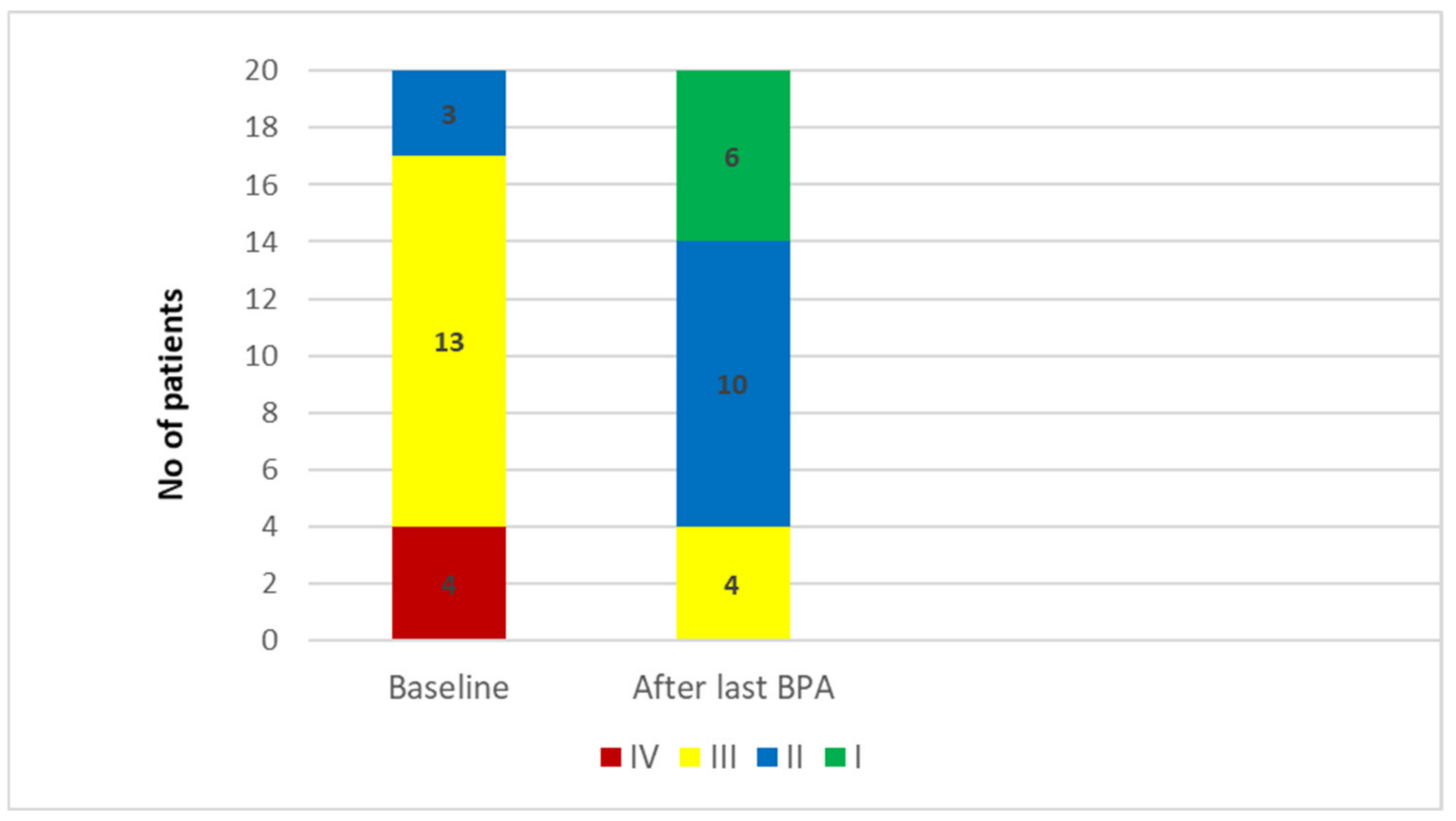
3.2. Effects of BPA
3.3. Safety
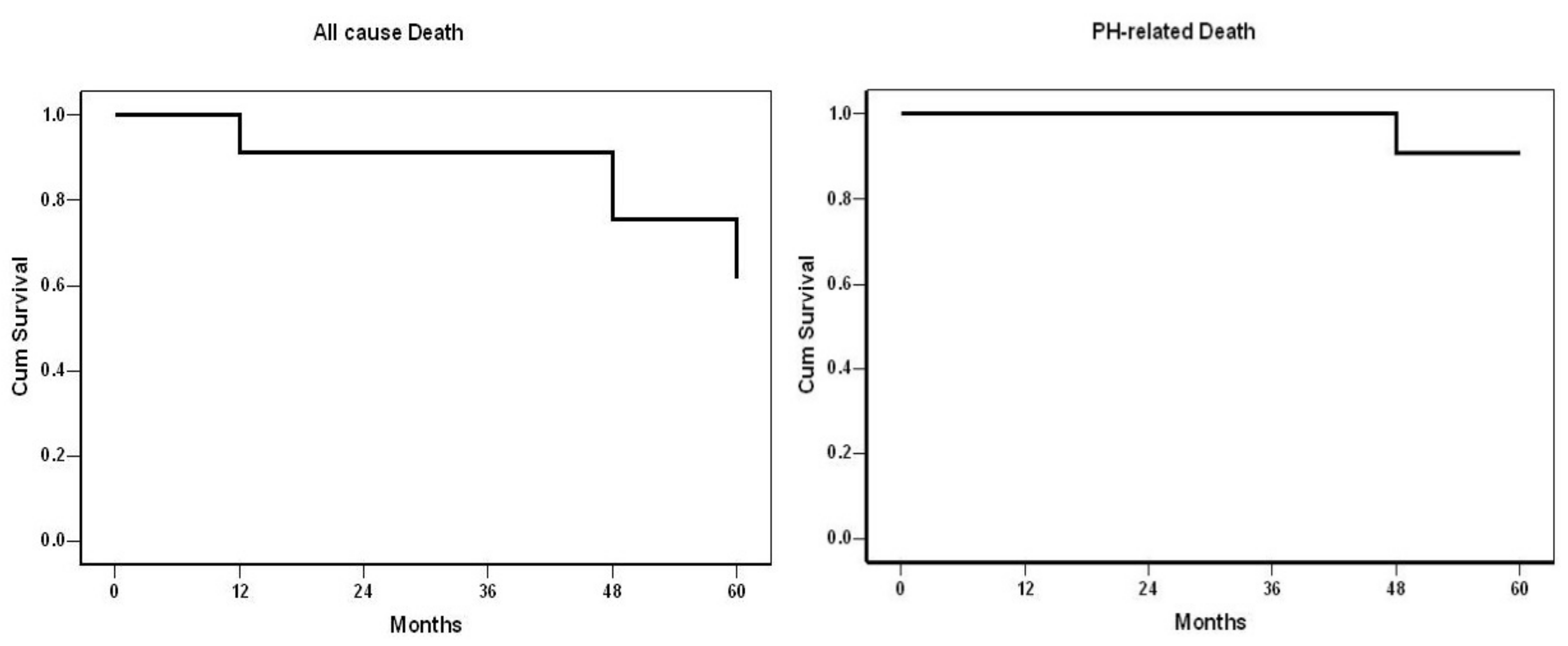
3.4. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoeper, M.M.; Mayer, E.; Simonneau, G.; Rubin, L.J. Chronic thromboembolic pulmonary hypertension. Circulation 2006, 113, 2011–2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef] [PubMed]
- Frost, A.; Badesch, D.; Gibbs, S.; Gopalan, D.; Khanna, D.; Manes, A.; Oudiz, R.; Satoh, T.; Torres, F.; Torbicki, A. Diagnosis of pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghofrani, H.A.; D’Armini, A.M.; Kim, N.H.; Mayer, E.; Simonneau, G. Interventional and pharmacological management of chronic thromboembolic pulmonary hypertension. Respir. Med. 2021, 177, 106293. [Google Scholar] [CrossRef] [PubMed]
- Fukui, S.; Ogo, T.; Morita, Y.; Tsuji, A.; Tateishi, E.; Ozaki, K. Right ventricular reverse remodelling after balloon pulmonary angioplasty. Eur. Respir. J. 2014, 43, 1394–1402. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, A.; Satoh, T.; Fukuda, T.; Sugimura, K.; Fukumoto, Y.; Emoto, N. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: Results of a Multicenter Registry. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e004029. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Matsuoka, Y.; Onishi, H.; Yanaka, K.; Emoto, N.; Nakai, H. The role of balloon pulmonary angioplasty and pulmonary endarterectomy: Is chronic thromboembolic pulmonary hypertension still a life-threatening disease? Int. J. Cardiol. 2021, 326, 170–177. [Google Scholar] [CrossRef]
- Arvanitaki, A.; Boutsikou, M.; Anthi, A.; Apostolopoulou, S.; Avgeropoulou, A.; Demerouti, E.; Farmakis, D.; Feloukidis, C.; Giannakoulas, G.; Karvounis, H.; et al. Epidemiology and initial management of pulmonary arterial hypertension: Real-world data from the Hellenic urrO pin urrO pinon rEgistry (HOPE). Pulm. Circ. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Demerouti, E.; Karyofyllis, P.; Voudris, V.; Boutsikou, M.; Anastasiadis, G.; Anthi, A.; Arvanitaki, A.; Athanassopoulos, G.; Avgeropoulou, A.; Brili, S.; et al. Real-World Data from the Hellenic Pulmonary Hypertension Registry (HOPE). J. Clin. Med. 2021, 10, 4547. [Google Scholar] [CrossRef]
- Kim, N.H.; Delcroix, M.; Jais, X.; Madani, M.M.; Matsubara, H.; Mayer, E.; Ogo, T.; Tapson, V.F.; Ghofrani, H.A.; Jenkins, D.P. Chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801915. [Google Scholar] [CrossRef]
- Ogawa, A.; Matsubara, H. After the Dawn—Balloon Pulmonary Angioplasty for Patients With Chronic Thromboembolic Pulmonary Hypertension. Circ. J. 2018, 82, 1222–1230. [Google Scholar] [CrossRef] [Green Version]
- Inami, T.; Kataoka, M.; Shimura, N. Pressure-wire-guided percutaneous transluminal pulmonary angioplasty: A breakthrough in catheter-interventional therapy for chronic thromboembolic pulmonary hypertension. JACC Cardiovasc. Interv. 2014, 7, 1297–1306. [Google Scholar] [CrossRef] [Green Version]
- Ejiri, K.; Ogawa, A.; Fujii, S.; Ito, H.; Matsubara, H. Vascular Injury Is a Major Cause of Lung Injury After Balloon Pulmonary Angioplasty in Patients With Chronic Thromboembolic Pulmonary Hypertension. Circ. Cardiovasc. Interv. 2018, 11, e005884. [Google Scholar] [CrossRef] [Green Version]
- Jönsson, A.K.; Schill, J.; Olsson, H.; Spigset, O.; Hägg, S. Venous Thromboembolism During Treatment with Antipsychotics: A Review of Current Evidence. CNS Drugs 2018, 32, 47–64. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, W.C.; Jansa, P.; Huang, W.C.; Nižnanský, M.; Omara, M.; Lindner, J. Residual pulmonary hypertension after pulmonary endarterectomy: A meta-analysis. J. Thorac. Cardiovasc. Surg. 2018, 156, 1275–1287. [Google Scholar] [CrossRef]
- Jansa, P.; Heller, S.; Svoboda, M.; Pad’our, M.; Ambrož, D.; Dytrych, V.; Širanec, M.; Kovárník, T.; Felšoci, M.; Hutyra, M.; et al. Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension: Impact on Clinical and Hemodynamic Parameters, Quality of Life and Risk Profile. J. Clin. Med. 2020, 9, 3608. [Google Scholar] [CrossRef]
- Guth, S.; D’Armini, A.M.; Delcroix, M.; Nakayama, K.; Fadel, E.; Hoole, S.P.; Jenkins, D.P.; Kiely, D.G.; Kim, N.H.; Lang, I.M.; et al. Current strategies for managing chronic thromboembolic pulmonary hypertension: Results of the worldwide prospective CTEPH Registry. ERJ Open Res. 2021, 7, 00850–02020. [Google Scholar] [CrossRef]
- Jamieson, S.W.; Kapelanski, D.P.; Sakakibara, N. Pulmonary endarterectomy: Experience and lessons learned in 1500 cases. Ann. Thorac. Surg. 2003, 76, 1457–1462. [Google Scholar] [CrossRef]
- Vizza, C.D.; Lang, I.M.; Badagliacca, R.; Benza, R.L.; Rosenkranz, S.; White, R.J.; Adir, Y.; Andreassen, A.K.; Balasubramanian, V.; Bartolome, S.; et al. Aggressive Afterload Lowering to Improve the RV: A New Target for Medical Therapy in PAH? Am. J. Respir. Crit. Care Med. 2021. [Google Scholar] [CrossRef]
- Olsson, K.M.; Wiedenroth, C.B.; Kamp, J.C. Balloon pulmonary angioplasty for inoperable patients with chronic thromboembolic pulmonary hypertension: The initial German experience. Eur. Respir. J. 2017, 49, 1602409. [Google Scholar] [CrossRef]
- Brenot, P.; Jaïs, X.; Alonso, T.C.G.; Gerardin, B.; Mussot, S.; Mercier, O.; Fabre, D.; Parent, F.; Jevnikar, M.; Montani, D.; et al. French experience of balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1802095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kataoka, M.; Inami, T.; Hayashida, K. Percutaneous transluminal pulmonary angioplasty for the treatment of chronic thromboembolic pulmonary hypertension. Circ. Cardiovasc. Interv. 2012, 5, 756–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minatsuki, S.; Takahara, M.; Kiyosue, A.; Kodera, S.; Hatano, M.; Ando, J.; Komuro, I. Characteristics and in-hospital outcomes of patients undergoing balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: A time-trend analysis from the Japanese nationwide registry. Open Heart 2021, 8, e001721. [Google Scholar] [CrossRef] [PubMed]
- Mizoguchi, H.; Ogawa, A.; Munemasa, M. Refined balloon pulmonary angioplasty for inoperable patients with chronic thromboembolic pulmonary hypertension. Circ. Cardiovasc. Interv. 2012, 5, 748–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimokawahara, H.; Ogawa, A.; Matsubara, H. Balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: Advances in patient and lesion selection urrO pin. Pulm. Med. 2021, 27, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Minatsuki, S.; Hatano, M.; Maki, H.; Takimoto, H.; Morita, H.; Komuro, I. Analysis of Oxygenation in Chronic Thromboembolic Pulmonary Hypertension Using Dead Space Ratio and Intrapulmonary Shunt Ratio. Int. Heart J. 2019, 60, 1137–1141. [Google Scholar] [CrossRef] [Green Version]
- Bazmpani, M.A.; Arvanitaki, A.; Toumpourleka, M.; Pitsiou, G.; Panagiotidou, E.; Mouratoglou, S.A.; Sianos, G.; Hadjimiltiades, S.; Pitsis, A.; Mayer, E.; et al. Epidemiology and management of chronic thromboembolic pulmonary hypertension: Experience from two expert centers. Hellenic. J. Cardiol. 2018, 59, 16–23. [Google Scholar] [CrossRef]
- Lang, I.; Meyer, B.C.; Ogo, T.; Matsubara, H.; Kurzyna, M.; Ghofrani, H.A.; Mayer, E.; Brenot, P. Balloon pulmonary angioplasty in chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2017, 26, 160119. [Google Scholar] [CrossRef] [Green Version]
- Kriechbaum, S.D.; Wiedenroth, C.B.; Hesse, M.L.; Ajnwojner, R.; Keller, T.; Sebastian Wolter, J.; Haas, M.; Roller, F.C.; Breitheck-er, A.; Rieth, A.J.; et al. Development of renal function during staged balloon pulmonary angioplasty for inoperable chronic thromboembolic pulmonary hypertension. Scand. J. Clin. Lab. Investig. 2019, 79, 268–275. [Google Scholar] [CrossRef]
- Riedel, M.; Stanek, V.; Widimsky, J.; Prerovsky, I. Longterm follow-up of patients with pulmonary thromboembolism. Late prog-nosis and evolution of hemodynamic and respiratory data. Chest 1982, 81, 151–158. [Google Scholar] [CrossRef]
- Delcroix, M.; Lang, I.; Pepke-Zaba, J.; Jansa, P.; D’Armini, A.M.; Snijder, R.; Bresser, P.; Torbicki, A.; Mellemkjaer, S.; Lewczuk, J.; et al. Long-Term Outcome of Patients with Chronic Thromboembolic Pulmonary Hypertension: Results From an International Prospective Registry. Circulation 2016, 133, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Darocha, S.; Roik, M.; Kopeć, G.; Araszkiewicz, A.; Furdal, M.; Lewandowski, M.; Jacheć, W.; Grabka, M.; Banaszkiewicz, M.; Pietrasik, A.; et al. Balloon pulmonary angioplasty in chronic thromboembolic pulmonary hypertension: A multicentre registry. EuroIntervention 2022, 17, 1104–1111. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | 53 ± 17 |
| Females (n, %) | 19 (79.2) |
| WHO FC I/II/III/IV (%) | 0/12.5/62.5/25 |
| NTproBNP (pg/mL) | 669 (IQR 153–1938) |
| Previous PEA (n, %) | 6 (25) |
| Haemodynamics | |
| Systolic PAP (mmHg) | 84.5 ± 23.5 |
| Mean PAP (mmHg) | 51.3 ± 12.6 |
| Mean RAP (mmHg) | 10.7 ± 4.0 |
| PCWP (mmHg) | 11.0 ± 2.7 |
| CI (L/min/m2) | 2.30 ± 0.64 |
| PVR (WU) | 10.66 ± 4.59 |
| SaO2 (%) | 89.6 ± 4.6 |
| SvO2 (%) | 60.9 ± 8.3 |
| Heart Rate | 82 ± 9 |
| PH therapy | |
| ERA (n, %) | 9 (37.5) |
| PDE5-I (n, %) | 1 (4.2) |
| sGC stimulator (n, %) | 14 (58.3) |
| Oral IP receptor agonist (n, %) | 1 (4.2) |
| IV epoprostenol | 1 (4.2) |
| Sc treprostinil | 2 (8.3) |
| Inhaled Iloprost | 1 (4.2) |
| None/single/double/triple (%) | 20.8/45.8/25.0/8.3 |
| Home Oxygen (n, %) | 21 (87.5) |
| Associated Conditions | |
| Splenectomy (n, %) | 6 (25) |
| Hemoglobinopathies (n, %) | 4 (16.7) |
| Myeloproliferative disorder (n, %) | 2 (8.3) |
| Thrombophilic disorder (n, %) | 5 (20.8) |
| V/A shunt/Pacemaker (n, %) | 2 (8.3) |
| APS (n, %) | 2 (8.3) |
| Psychiatric disorder (n, %) | 1 (4.2.) |
| Baseline | After BPA | Change (%) | p-Value | |
|---|---|---|---|---|
| RAP (mmHg) | 10.4 ± 4.0 | 6.5 ± 3.0 | −37 | <0.001 |
| Systolic PAP (mmHg) | 82.8 ± 25.3 | 44.6 ± 13.2 | −46 | <0.001 |
| mean PAP (mmHg) | 50.8 ± 13.5 | 28.6 ± 8.0 | −44 | <0.001 |
| PVR (WU) | 10.6 ± 4.9 | 4.2 ± 2.7 | −60 | <0.001 |
| CI (L/min/m2) | 2.32 ± 0.68 | 2.56 ± 0.44 | +9 | 0.119 |
| HR | 84 ± 9 | 69 ± 11 | −18 | <0.001 |
| SAO2 | 90.3 ± 4.8 | 95.5 ± 3.6 | +5 | <0.001 |
| SVO2 | 62.4 ± 8.0 | 67.0 ± 6.6 | +7 | 0.003 |
| NTproBNP (pg/mL) (median) | 912 ± 1158 (356) | 220 ± 303 (91) | −76 (−74) | 0.003 |
| WHO FC (mean) (median) | 3.05 ± 0.6 3 | 1.90 ± 0.7 2 | −38 | <0.001 |
| WHO FC I/II/III/IV (%) | 0/15/65/20 | 30/50/20/0 |
| Before BPA | After BPA | p-Value | |
|---|---|---|---|
| Home oxygen therapy | 17 (85) | 7 (35) | 0.003 |
| PH specific drugs | 15 (75) | 11 (55) | 0.320 |
| Parenteral Prostanoids | 3 (15) | 2 (10) | 0.002 |
| Monotherapy | 7 (35) | 7 (35) | |
| Dual combination therapy | 6 (30) | 3 (15) | |
| Triple combination therapy | 2 (10) | 1 (5) |
| Baseline | After BPA | Change (%) | p-Value | |
|---|---|---|---|---|
| mRAP (mmHg) | 10.0 ± 4.2 | 6.6 ± 2.9 | −34 | <0.001 |
| Systolic PAP (mmHg) | 76.8 ± 23.7 | 40.6 ± 11.9 | −47 | <0.001 |
| mean PAP (mmHg) | 47.8 ± 13.5 | 26.4 ± 7.6 | −45 | <0.001 |
| PVR (WU) | 10.0 ± 5.0 | 3.7 ± 2.8 | −63 | <0.001 |
| CI (L/min/m2) | 2.23 ± 0.7 | 2.51 ± 0.36 | +11 | 0.143 |
| HR | 84 ± 10 | 68 ± 12 | −19 | <0.001 |
| SAO2 | 90.4 ± 5.1 | 95.3 ± 4.0 | +5 | 0.001 |
| SVO2 | 63.4 ± 8.2 | 67.3 ± 7.1 | +6 | 0.028 |
| NTproBNP (pg/mL) (median) | 925 ± 1238 (307) | 231 ± 327 (81) | −75 (−74) | 0.012 |
| WHO FC (mean) (median) | 3.0 ± 0.7 3 | 1.9 ± 0.7 2 | −37 | <0.001 |
| WHO FC I/II/III/IV (%) | 0/20/53.3/26.7 | 26.7/53.3/20/0 | ||
| Home Oxygen Therapy (n, %) | 13 (86.7) | 5 (33.3) | 0.001 | |
| Specific PH Treatment (n, %) | 11 (73.3) | 7 (46.7) | 0.041 |
| Sessions (n = 180) (n, %) | Patients (n = 24) (n, %) | |
|---|---|---|
| Overall complications | 37 (20.6) | 10 (41.7) |
| Asymptomatic Lung Injury | 4 (2.2) | 4 (16.7) |
| Symptomatic Lung Injury | 2 (1.1) | 2 (8.3) |
| Hemoptysis | 18 (10) | 6 (25) |
| Dissection | 3 (1.7) | 2 (8.3) |
| Pulmonary Artery perforation | 5 (2.8) | 4 (8.3) |
| Pulmonary Artery Rapture | 0 | 0 |
| Renal dysfunction | 0 | 0 |
| Allergic reaction (shock) | 2 (1.1) | 2 (16.6) |
| NIPPV | 2 (1.1) | 2 (16.6) |
| Intubation | 0 | 0 |
| ECMO | 0 | 0 |
| Death | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karyofyllis, P.; Demerouti, E.; Giannakoulas, G.; Anthi, A.; Arvanitaki, A.; Athanassopoulos, G.; Feloukidis, C.; Iakovou, I.; Kostelidou, T.; Mitrouska, I.; et al. Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension in Greece: Data from the Hellenic Pulmonary Hypertension Registry. J. Clin. Med. 2022, 11, 2211. https://doi.org/10.3390/jcm11082211
Karyofyllis P, Demerouti E, Giannakoulas G, Anthi A, Arvanitaki A, Athanassopoulos G, Feloukidis C, Iakovou I, Kostelidou T, Mitrouska I, et al. Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension in Greece: Data from the Hellenic Pulmonary Hypertension Registry. Journal of Clinical Medicine. 2022; 11(8):2211. https://doi.org/10.3390/jcm11082211
Chicago/Turabian StyleKaryofyllis, Panagiotis, Eftychia Demerouti, George Giannakoulas, Anastasia Anthi, Alexandra Arvanitaki, George Athanassopoulos, Christos Feloukidis, Ioannis Iakovou, Theodora Kostelidou, Ioanna Mitrouska, and et al. 2022. "Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension in Greece: Data from the Hellenic Pulmonary Hypertension Registry" Journal of Clinical Medicine 11, no. 8: 2211. https://doi.org/10.3390/jcm11082211