
Pathogenesis and Management of Brugada Syndrome: Recent Advances and Protocol for Umbrella Reviews of Meta-Analyses in Major Arrhythmic Events Risk Stratification

 ,
,  ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
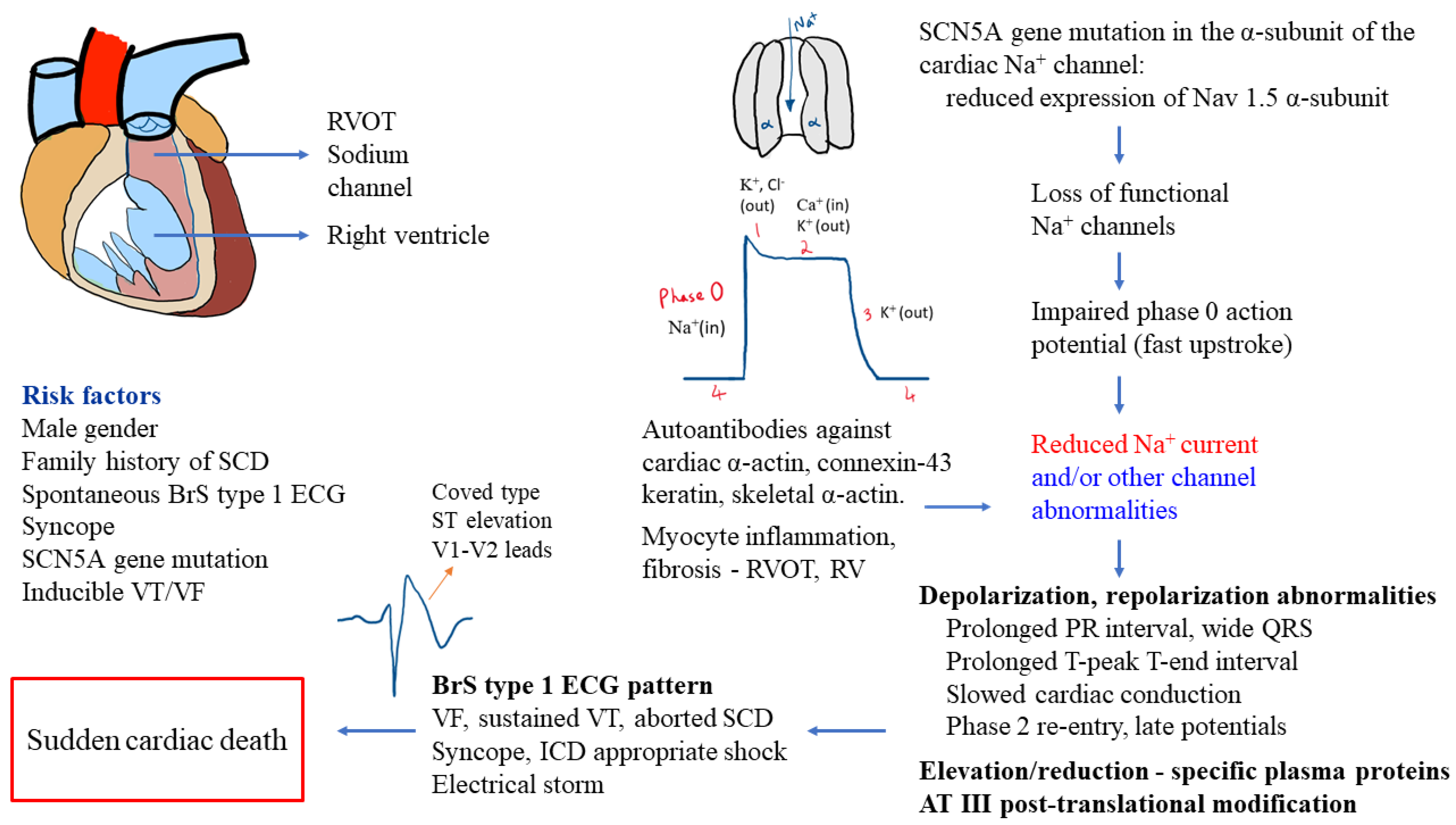
2. Pathogenesis of BrS
3. Diagnostics and Risk Stratification
3.1. Diagnostics in BrS
3.2. Risk Stratification in BrS
4. Treatment of Patients with BrS
5. Protocol for Umbrella Reviews of Meta-Analyses in MAE Risk Stratification in BrS
5.1. Major Questions of Umbrella Reviews
- What is the association between MAE and clinical factors such as positive family history of SCD in BrS individuals based on an integrative evaluation of previous meta-analyses?
- How can ECG changes such as QRS complexes prolongation, fQRS, AV conduction delay, T-peak to T-end (Tpe) interval, and prolonged QTc interval be used to predict life-threatening ventricular arrhythmias in patients with BrS?
- What role does EPS, PVS, genetic studies, and features of sodium channel blocker challenge have on predicting MAE and sudden fatalities in BrS?
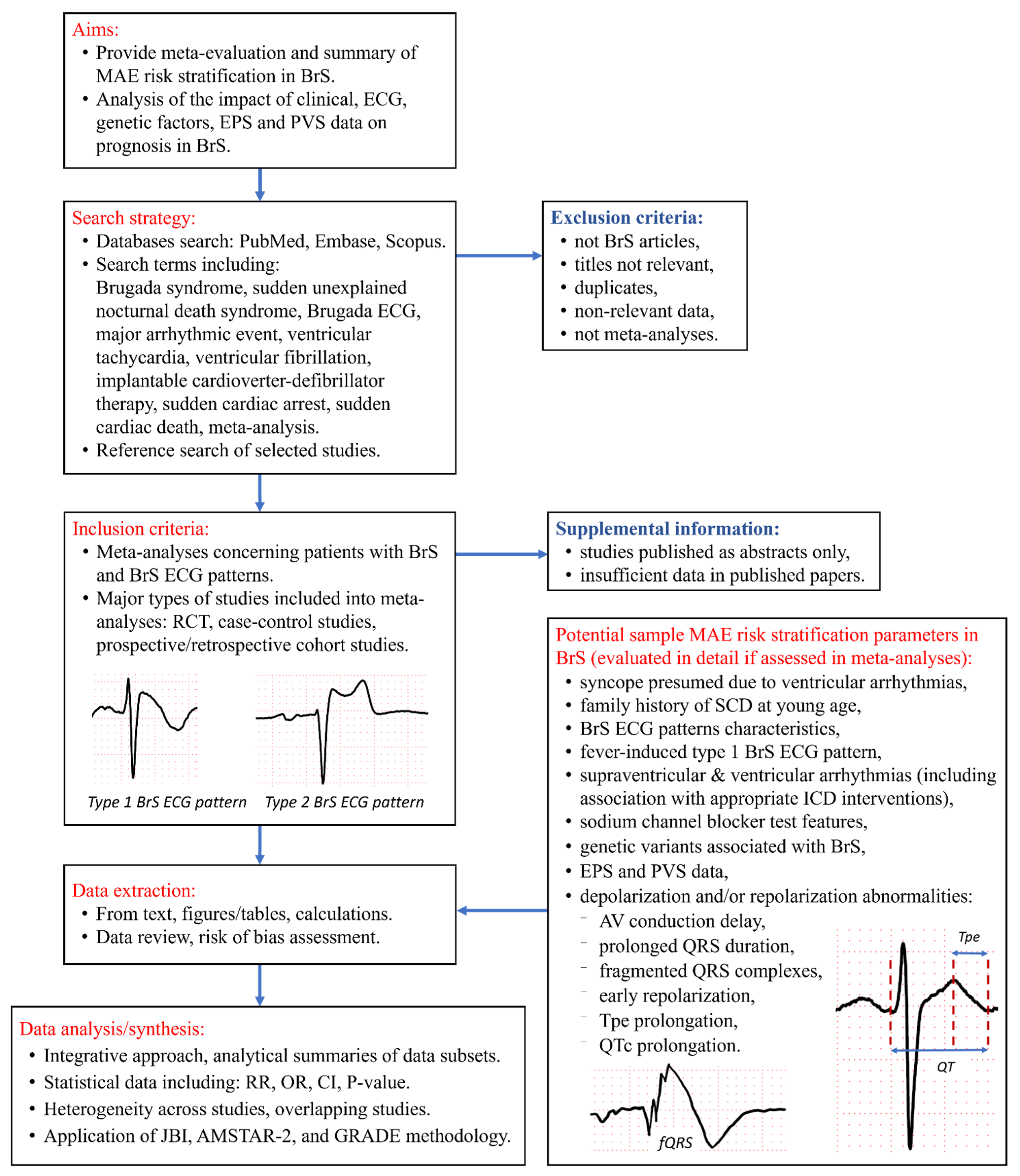
5.2. Aims of Umbrella Reviews
5.3. Type and Method of Review
5.4. Search Strategy and Study Selection
5.5. Inclusion Criteria
5.6. Exclusion Criteria
- older versions of updated meta-analyses;
- publications which included smaller number of studies or smaller number of patients on the same risk stratification tool [71].
5.7. Participants/Population
5.8. Types of Interventions or Exposures
- clinical factors such as fever-induced BrS ECG pattern, syncope, and positive SCD family history;
- spontaneous and drug-induced type-1 BrS ECG pattern;
- supraventricular and ventricular arrhythmias—including appropriate ICD therapy,
- depolarization and/or repolarization abnormalities due to factors such as atrioventricular conduction delay, prolonged QRS duration, fQRS, early repolarization, late potentials, and Tpe interval prolongation;
- abnormal EPS and/or PVS;
- genetic variants associated with BrS.
5.9. Planned Umbrella Reviews Include
- Analysis of clinical (i.e., previous syncope) and ECG factors, including ECG parameters such as prolonged QRS duration, atrioventricular conduction delay, Tpe, fQRS, QTc prolongation, late potentials, arrhythmias, fever-induced type 1 BrS ECG pattern, and the impact of sodium channel blocker challenge features for MAE risk stratification in BrS.
- Evaluation of the influence of genetic factors, and family history of BrS or SCD at young age, on life-threatening ventricular arrhythmias.
- Analysis of EPS and PVS for MAE risk stratification in BrS.
5.10. Context
5.11. Types of Studies
5.12. Condition or Domain Being Studied
5.13. Main Outcomes
- Evaluation of association between multiple potential MAE risk stratification parameters and MAE in individuals with BrS (e.g., listed in Figure 2).
- Application of meta-evaluation results to facilitate evidence-based diagnosis and treatment approaches in order to mitigate the risk of SCD and improve the quality of life in BrS patients and their relatives.
5.14. Planned Measures of Effect
5.15. Data Extraction (Selection and Coding)
5.16. Risk of Bias (Quality) Assessment
5.17. Strategy for Data Analysis/Synthesis
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sieira, J.; Brugada, P. The definition of the Brugada syndrome. Eur. Heart J. 2017, 38, 3029–3034. [Google Scholar] [CrossRef] [PubMed]
- Matusik, P.T. Insights into channelopathies: Progress in clinical practice and research. J. Electrocardiol. 2017, 50, 534–535. [Google Scholar] [CrossRef] [PubMed]
- Brugada, P.; Brugada, J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: A distinct clinical and electrocardiographic syndrome: A multicenter report. J. Am. Coll. Cardiol. 1992, 20, 1391–1396. [Google Scholar] [CrossRef]
- Havakuk, O.; Viskin, S. A tale of 2 diseases: The history of long-QT syndrome and Brugada syndrome. J. Am. Coll. Cardiol. 2016, 67, 100–108. [Google Scholar] [CrossRef] [Green Version]
- Matusik, P.T.; Pudło, J.; Rydlewska, A.; Podolec, J.; Lelakowski, J.; Podolec, P. Brugada syndrome: Current diagnostics, epidemiology, genetic data and novel mechanisms (RCD code: V-1A.1). J. Rare Cardiovasc. Dis. 2017, 3, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Vutthikraivit, W.; Rattanawong, P.; Putthapiban, P.; Sukhumthammarat, W.; Vathesatogkit, P.; Ngarmukos, T.; Thakkinstian, A. Worldwide prevalence of Brugada syndrome: A systematic review and meta-analysis. Acta Cardiol. Sin. 2018, 34, 267–277. [Google Scholar] [CrossRef]
- Rattanawong, P.; Kewcharoen, J.; Kanitsoraphan, C.; Vutthikraivit, W.; Putthapiban, P.; Prasitlumkum, N.; Mekraksakit, P.; Mekritthikrai, R.; Chung, E.H. The utility of drug challenge testing in Brugada syndrome: A systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 2020, 31, 2474–2483. [Google Scholar] [CrossRef]
- Bernardo, M.; Tiyyagura, S.R. A case of type I and II Brugada phenocopy unmasked in a patient with normal baseline electrocardiogram (ECG). Am. J. Case Rep. 2018, 19, 21–24. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, D.; Pieroni, M.; Fatah, M.; Charpentier, F.; Cunningham, K.S.; Spears, D.A.; Chatterjee, D.; Suna, G.; Bos, J.M.; Ackerman, M.J.; et al. An autoantibody profile detects Brugada syndrome and identifies abnormally expressed myocardial proteins. Eur. Heart J. 2020, 41, 2878A–2890A. [Google Scholar] [CrossRef]
- Roterberg, G.; El-Battrawy, I.; Veith, M.; Liebe, V.; Ansari, U.; Lang, S.; Zhou, X.; Akin, I.; Borggrefe, M. Arrhythmic events in Brugada syndrome patients induced by fever. Ann. Noninvasive Electrocardiol. 2019, 25, 135–140. [Google Scholar] [CrossRef]
- Mizusawa, Y.; Wilde, A.A.M. Brugada syndrome. Circ. Arrhythm Electrophysiol. 2012, 5, 606–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rattanawong, P.; Kewcharoen, J.; Techorueangwiwat, C.; Kanitsoraphan, C.; Mekritthikrai, R.; Prasitlumkum, N.; Puttapiban, P.; Mekraksakit, P.; Vutthikraivit, W.; Sorajja, D. Wide QRS complex and the risk of major arrhythmic events in Brugada syndrome patients: A systematic review and meta-analysis. J. Arrhythmia 2019, 36, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.; Tian, L.; Ke, J.; Sun, Y.; Wu, R.; Zhu, J.; Ke, Q. Risk factors for cardiac events in patients with Brugada syndrome: A PRISMA-compliant meta-analysis and systematic review. Medicine 2016, 95, e4214. [Google Scholar] [CrossRef] [PubMed]
- Antzelevitch, C.; Brugada, P.; Borggrefe, M.; Brugada, J.; Brugada, R.; Corrado, D.; Gussak, I.; LeMarec, H.; Nademanee, K.; Riera, A.R.P.; et al. Brugada syndrome: Report of the second consensus conference. Circulation 2005, 111, 659–670. [Google Scholar] [CrossRef] [Green Version]
- Alings, M.; Wilde, A. “Brugada” syndrome. clinical data and suggested pathophysiological mechanism. Circulation 1999, 99, 666–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matusik, P.T.; Rydlewska, A.; Pudło, J.; Podolec, J.; Lelakowski, J.; Podolec, P. Brugada syndrome: New concepts and algorithms in management (RCD code: V 1A.1). J. Rare Cardiovasc. Dis. 2018, 3, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Miles, C.; Asimaki, A.; Ster, I.C.; Papadakis, M.; Gray, B.; Westaby, J.; Finocchiaro, G.; Bueno-Beti, C.; Ensam, B.; Basu, J.; et al. Biventricular myocardial fibrosis and sudden death in patients with Brugada syndrome. J. Am. Coll. Cardiol. 2021, 78, 1511–1521. [Google Scholar] [CrossRef]
- Zhang, Z.-H.; Barajas-Martínez, H.; Xia, H.; Li, B.; Capra, J.A.; Clatot, J.; Chen, G.-X.; Chen, X.; Yang, B.; Jiang, H.; et al. Distinct features of probands with early repolarization and Brugada syndromes carrying SCN5A pathogenic variants. J. Am. Coll. Cardiol. 2021, 78, 1603–1617. [Google Scholar] [CrossRef]
- Tse, G.; Lee, S.; Liu, T.; Yuen, H.C.; Wong, I.C.K.; Mak, C.; Mok, N.S.; Wong, W.T. Identification of novel SCN5A single nucleotide variants in Brugada syndrome: A territory-wide study from Hong Kong. Front. Physiol. 2020, 11, 574590. [Google Scholar] [CrossRef]
- Barc, J.; Tadros, R.; Glinge, C.; Chiang, D.Y.; Jouni, M.; Simonet, F.; Jurgens, S.J.; Baudic, M.; Nicastro, M.; Potet, F.; et al. Genome-wide association analyses identify new Brugada syndrome risk loci and highlight a new mechanism of sodium channel regulation in disease susceptibility. Nat. Genet. 2022, 54, 232–239. [Google Scholar] [CrossRef]
- Garcia-Elias, A.; Benito, B. Ion Channel Disorders and Sudden Cardiac Death. Int. J. Mol. Sci. 2018, 19, 692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pranata, R.; Yonas, E.; Chintya, V.; Deka, H.; Raharjo, S.B. Association between PR Interval, First-degree atrioventricular block and major arrhythmic events in patients with Brugada syndrome—Systematic review and meta-analysis. J. Arrhythmia 2019, 35, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.A.; Krishnan, K.; Madias, C.; Trohman, R.G. Combined right ventricular outflow tract epicardial and endocardial late potential ablation for treatment of Brugada storm: A case report and review of the literature. Cardiol. Ther. 2016, 5, 229–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Domenico, M.; Cuda, G.; Scumaci, D.; Grasso, S.; Gaspari, M.; Curcio, A.; Oliva, A.; Ausania, F.; Di Nunzio, C.; Ricciardi, C.; et al. Biomarker discovery by plasma proteomics in familial Brugada Syndrome. Front. Biosci. 2013, 18, 564–571. [Google Scholar] [CrossRef] [Green Version]
- Zumhagen, S.; Zeidler, E.M.; Stallmeyer, B.; Ernsting, M.; Eckardt, L.; Schulze-Bahr, E. Tpeak–Tendinterval and Tpeak–Tend/QT ratio in patients with Brugada syndrome. Europace 2016, 18, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Tse, G.; Gong, M.; Li, C.K.H.; Leung, K.S.K.; Georgopoulos, S.; Bazoukis, G.; Letsas, K.P.; Sawant, A.C.; Mugnai, G.; Wong, M.C.S.; et al. T peak -T end, T peak -T end /QT ratio and T peak -T end dispersion for risk stratification in Brugada syndrome: A systematic review and meta-analysis. J. Arrhythmia 2018, 34, 587–597. [Google Scholar] [CrossRef]
- Tse, G.; Lee, S.; Li, A.; Chang, D.; Li, G.; Zhou, J.; Liu, T.; Zhang, Q. Automated electrocardiogram analysis identifies novel predictors of ventricular arrhythmias in Brugada syndrome. Front. Cardiovasc. Med. 2021, 7, 399. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the european society of cardiology (ESC). Endorsed by: Association for European paediatric and congenital cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar]
- Pappone, C.; Santinelli, V. Brugada syndrome: Progress in diagnosis and management. Arrhythmia Electrophysiol. Rev. 2019, 8, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Antzelevitch, C.; Yan, G.-X.; Ackerman, M.J.; Borggrefe, M.; Corrado, D.; Guo, J.; Gussak, I.; Hasdemir, C.; Horie, M.; Huikuri, H.; et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Hear. Rhythm 2016, 13, e295–e324. [Google Scholar] [CrossRef] [Green Version]
- Matusik, P.S.; Bryll, A.; Matusik, P.T.; Pac, A.; Popiela, T.J. Electrocardiography and cardiac magnetic resonance imaging in the detection of left ventricular hypertrophy: The impact of indexing methods. Kardiol. Pol. 2020, 78, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Kucharz, A.; Kułakowski, P. Fragmented QRS and arrhythmic events in patients with implantable cardioverter-defibrillators. Kardiol. Pol. 2020, 78, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Matusik, P.T. Biomarkers and cardiovascular risk stratification. Eur. Heart J. 2019, 40, 1483–1485. [Google Scholar] [CrossRef]
- Matusik, P.T.; Małecka, B.; Lelakowski, J.; Undas, A. Association of NT-proBNP and GDF-15 with markers of a prothrombotic state in patients with atrial fibrillation off anticoagulation. Clin. Res. Cardiol. 2020, 109, 426–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asvestas, D.; Tse, G.; Baranchuk, A.; Bazoukis, G.; Liu, T.; Saplaouras, A.; Korantzopoulos, P.; Goga, C.; Efremidis, M.; Sideris, A.; et al. High risk electrocardiographic markers in Brugada syndrome. Int. J. Cardiol. Heart Vasc. 2018, 18, 58–64. [Google Scholar] [CrossRef]
- Okólska, M.; Łach, J.; Matusik, P.T.; Pająk, J.; Mroczek, T.; Podolec, P.; Tomkiewicz-Pająk, L. Heart Rate variability and its associations with organ complications in adults after fontan operation. J. Clin. Med. 2021, 10, 4492. [Google Scholar] [CrossRef] [PubMed]
- Pruszczyk, P.; Skowrońska, M.; Ciurzyński, M.; Kurnicka, K.; Lankei, M.; Konstantinides, S. Assessment of pulmonary embolism severity and the risk of early death. Pol. Arch. Intern. Med. 2021, 131. [Google Scholar] [CrossRef] [PubMed]
- Letsas, K.P.; Vlachos, K.; Conte, G.; Efremidis, M.; Nakashima, T.; Duchateau, J.; Bazoukis, G.; Frontera, A.; Mililis, P.; Tse, G.; et al. Right ventricular outflow tract electroanatomical abnormalities in asymptomatic and high-risk symptomatic patients with Brugada syndrome: Evidence for a new risk stratification tool? J. Cardiovasc. Electrophysiol. 2021, 32, 2997–3007. [Google Scholar] [CrossRef]
- Lee, S.; Zhou, J.; Li, K.H.C.; Leung, K.S.K.; Lakhani, I.; Liu, T.; Wong, I.C.K.; Mok, N.S.; Mak, C.; Jeevaratnam, K.; et al. Territory-wide cohort study of Brugada syndrome in Hong Kong: Predictors of long-term outcomes using random survival forests and non-negative matrix factorisation. Open Heart 2021, 8, e001505. [Google Scholar] [CrossRef]
- Lee, S.; Wong, W.T.; Wong, I.C.K.; Mak, C.; Mok, N.S.; Liu, T.; Tse, G. Ventricular Tachyarrhythmia Risk in Paediatric/Young vs. Adult Brugada Syndrome Patients: A Territory-Wide Study. Front. Cardiovasc. Med. 2021, 8, 671666. [Google Scholar] [CrossRef]
- Tse, G.; Zhou, J.; Lee, S.; Liu, T.; Bazoukis, G.; Mililis, P.; Wong, I.C.K.; Chen, C.; Xia, Y.; Kamakura, T.; et al. Incorporating latent variables using nonnegative matrix factorization improves risk stratification in Brugada syndrome. J. Am. Heart Assoc. 2020, 9, e012714. [Google Scholar] [CrossRef] [PubMed]
- Letsas, K.P.; Asvestas, D.; Baranchuk, A.; Liu, T.; Georgopoulos, S.; Efremidis, M.; Korantzopoulos, P.; Bazoukis, G.; Tse, G.; Sideris, A.; et al. Prognosis, risk stratification, and management of asymptomatic individuals with Brugada syndrome: A systematic review. Pacing Clin. Electrophysiol. 2017, 40, 1332–1345. [Google Scholar] [CrossRef] [PubMed]
- Marsman, E.M.J.; Postema, P.G.; Remme, C.A. Brugada syndrome: Update and future perspectives. Heart 2021, 2020, 318258. [Google Scholar] [CrossRef]
- Honarbakhsh, S.; Providência, R.; Lambiase, P.D.; Centre, S.B.H.B.H. Risk stratification in Brugada syndrome: Current status and emerging approaches. Arrhythmia Electrophysiol. Rev. 2018, 7, 79–83. [Google Scholar] [CrossRef]
- Matusik, P.T.; Komar, M.; Podolec, J.; Karkowski, G.; Lelakowski, J.; Podolec, P. Exercise ECG unmasked Brugada sign: Manifestation of the risk of sports-associated sudden cardiac arrest (RCD code: V-1A.1). J. Rare Cardiovasc. Dis. 2017, 3, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Abe, A.; Kobayashi, K.; Yuzawa, H.; Sato, H.; Fukunaga, S.; Fujino, T.; Okano, Y.; Yamazaki, J.; Miwa, Y.; Yoshino, H.; et al. Comparison of late potentials for 24 hours between Brugada syndrome and arrhythmogenic right ventricular cardiomyopathy using a novel signal-averaging system based on holter ECG. Circ. Arrhythmia Electrophysiol. 2012, 5, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Kawada, S.; Morita, H.; Antzelevitch, C.; Morimoto, Y.; Nakagawa, K.; Watanabe, A.; Nishii, N.; Nakamura, K.; Ito, H. Shanghai Score system for diagnosis of brugada syndrome: Validation of the score system and system and reclassification of the patients. JACC Clin. Electrophysiol. 2018, 4, 724–730. [Google Scholar] [CrossRef]
- Wilde, A.A.M. The Shanghai score system in Brugada syndrome: Using it beyond a diagnostic score. JACC Clin. Electrophysiol. 2018, 4, 731–732. [Google Scholar] [CrossRef]
- Wijeyeratne, Y.D.; Tanck, M.W.; Mizusawa, Y.; Batchvarov, V.; Barc, J.; Crotti, L.; Bos, J.M.; Tester, D.J.; Muir, A.; Veltmann, C.; et al. SCN5A Mutation Type and a Genetic Risk Score Associate Variably with Brugada Syndrome Phenotype in SCN5A Families. Circ. Genom. Precis. Med. 2020, 13, e002911. [Google Scholar] [CrossRef]
- Veltmann, C.; Papavassiliu, T.; Konrad, T.; Doesch, C.; Kuschyk, J.; Streitner, F.; Haghi, D.; Michaely, H.; Schoenberg, S.; Borggrefe, M.; et al. Insights into the location of type I ECG in patients with Brugada syndrome: Correlation of ECG and cardiovascular magnetic resonance imaging. Heart Rhythm 2012, 9, 414–421. [Google Scholar] [CrossRef]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: A report of the American college of cardiology/American Heart association task force on clinical practice guidelines and the heart rhythm society. J. Am. Coll. Cardiol. 2018, 72, e91–e220. [Google Scholar] [PubMed]
- Wakamiya, A.; Kamakura, T.; Shinohara, T.; Yodogawa, K.; Murakoshi, N.; Morita, H.; Takahashi, N.; Inden, Y.; Shimizu, W.; Nogami, A.; et al. Improved risk stratification of patients with Brugada syndrome by the new Japanese circulation society guideline―A multicenter validation study. Circ. J. 2020, 84, 2158–2165. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Gasparini, M.; Napolitano, C.; Della Bella, P.; Ottonelli, A.G.; Sassone, B.; Giordano, U.; Pappone, C.; Mascioli, G.; Rossetti, G.; et al. Risk stratification in Brugada syndrome: Results of the PRELUDE (PRogrammed ELectrical stimUlation preDictive valuE) registry. J. Am. Coll. Cardiol. 2012, 59, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigi, M.A.B.; Aslani, A.; Shahrzad, S. aVR sign as a risk factor for life-threatening arrhythmic events in patients with Brugada syndrome. Heart Rhythm 2007, 4, 1009–1012. [Google Scholar] [CrossRef]
- Tsai, C.-F.; Chuang, Y.-T.; Huang, J.-Y.; Ueng, K.-C. Long-term prognosis of febrile individuals with right precordial coved-type ST-segment elevation Brugada pattern: A 10-year prospective follow-up study. J. Clin. Med. 2021, 10, 4997. [Google Scholar] [CrossRef]
- Iacopino, S.; Chierchia, G.-B.; Sorrenti, P.; Pesce, F.; Colella, J.; Fabiano, G.; Campagna, G.; Petretta, A.; Placentino, F.; Filannino, P.; et al. dST-Tiso Interval, a novel electrocardiographic marker of ventricular arrhythmia inducibility in individuals with ajmaline-induced Brugada type I pattern. Am. J. Cardiol. 2021, 159, 94–99. [Google Scholar] [CrossRef]
- Ishikawa, T.; Kimoto, H.; Mishima, H.; Yamagata, K.; Ogata, S.; Aizawa, Y.; Hayashi, K.; Morita, H.; Nakajima, T.; Nakano, Y.; et al. Functionally validated SCN5A variants allow interpretation of pathogenicity and prediction of lethal events in Brugada syndrome. Eur. Heart J. 2021, 42, 2854–2863. [Google Scholar] [CrossRef]
- Letsas, K.P.; Vlachos, K.; Efremidis, M.; Dragasis, S.; Korantzopoulos, P.; Tse, G.; Liu, T.; Bazoukis, G.; Niarchou, P.; Prappa, E.; et al. Right ventricular outflow tract endocardial unipolar substrate mapping: Implications in risk stratification of Brugada syndrome. Rev. Cardiovasc. Med. 2022, 23, 044. [Google Scholar] [CrossRef]
- Chung, C.T.; Bazoukis, G.; Radford, D.; Coakley-Youngs, E.; Rajan, R.; Matusik, P.T.; Liu, T.; Letsas, K.P.; Lee, S.; Tse, G. Predictive risk models for forecasting arrhythmic outcomes in Brugada syndrome: A focused review. J. Electrocardiol. 2022, 72, 28–34. [Google Scholar] [CrossRef]
- Probst, V.; Goronflot, T.; Anys, S.; Tixier, R.; Briand, J.; Berthome, P.; Geoffroy, O.; Clementy, N.; Mansourati, J.; Jesel, L.; et al. Robustness and relevance of predictive score in sudden cardiac death for patients with Brugada syndrome. Eur. Heart J. 2021, 42, 1687–1695. [Google Scholar] [CrossRef]
- Honarbakhsh, S.; Providencia, R.; Garcia-Hernandez, J.; Martin, C.A.; Hunter, R.J.; Lim, W.Y.; Kirkby, C.; Graham, A.J.; Sharifzadehgan, A.; Waldmann, V.; et al. A primary prevention clinical risk score model for patients with Brugada syndrome (BRUGADA-RISK). JACC: Clin. Electrophysiol. 2021, 7, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Letsas, K.P.; Georgopoulos, S.; Vlachos, K. Brugada syndrome:risk stratification and management corresponding author. J. Atr. Fibrillation 2016, 7, 79–83. [Google Scholar]
- Dereci, A.; Yap, S.C.; Schinkel, A.F.L. Meta-Analysis of clinical outcome after implantable cardioverter-defibrillator implantation in patients with Brugada syndrome. JACC Clin. Electrophysiol. 2019, 5, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, G.C.; Fernandes, A.; Cardoso, R.; Nasi, G.; Rivera, M.; Mitrani, R.D.; Goldberger, J.J. Ablation strategies for the management of symptomatic Brugada syndrome: A systematic review. Heart Rhythm 2018, 15, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Nademanee, K.; Veerakul, G.; Chandanamattha, P.; Chaothawee, L.; Ariyachaipanich, A.; Jirasirirojanakorn, K.; Likittanasombat, K.; Bhuripanyo, K.; Ngarmukos, T. Arrhythmia/electrophysiology prevention of ventricular fibrillation episodes in Brugada syndrome by catheter ablation over the anterior right ventricular outflow tract epicardium. Circulation 2011, 123, 1270–1279. [Google Scholar] [CrossRef]
- Asada, S.; Morita, H.; Watanabe, A.; Nakagawa, K.; Nagase, S.; Miyamoto, M.; Morimoto, Y.; Kawada, S.; Nishii, N.; Ito, H. Indication and prognostic significance of programmed ventricular stimulation in asymptomatic patients with Brugada syndrome. Europace 2020, 22, 972–979. [Google Scholar] [CrossRef]
- Kamioka, H. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Jpn. Pharmacol. Ther. 2019, 47, 1177–1185. [Google Scholar]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Kewcharoen, J.; Rattanawong, P.; Kanitsoraphan, C.; Mekritthikrai, R.; Prasitlumkum, N.; Putthapiban, P.; Mekraksakit, P.; Pattison, R.J.; Vutthikraivit, W. Atrial fibrillation and risk of major arrhythmic events in Brugada syndrome: A meta-analysis. Ann. Noninvasive Electrocardiol. 2019, 24, e12676. [Google Scholar] [CrossRef] [Green Version]
- de Luna, A.B.; Brugada, J.; Baranchuk, A.; Borggrefe, M.; Breithardt, G.; Goldwasser, D.; Lambiase, P.; Riera, A.P.; Garcia-Niebla, J.; Pastore, C.; et al. Current electrocardiographic criteria for diagnosis of Brugada pattern: A consensus report. J. Electrocardiol. 2012, 45, 433–442. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Radua, J. Ten simple rules for conducting umbrella reviews. Evid. -Based Ment. Health 2018, 21, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijkers, M. Introducing GRADE: A systematic approach to rating evidence in systematic reviews and to guideline development. KT Update 2013, 1, 1–9. [Google Scholar]
- Briggs, J. Checklist for Systematic Reviews and Research Syntheses; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Sheppard, M.N. Sudden Death in congenital heart disease: The role of the autopsy in determining the actual cause. J. Cardiovasc. Dev. Dis. 2020, 7, 58. [Google Scholar] [CrossRef]
- Podolec, P.; Matusik, P.T. New clinical classification of rare cardiovascular diseases and disorders: Relevance for cardiovascular research. Cardiovasc. Res. 2019, 115, e77–e79. [Google Scholar] [CrossRef]
- Podolec, P.; Baranchuk, A.; Brugada, J.; Kukla, P.; Lelakowski, J.; Kopeć, G.; Rubiś, P.; Stępniewski, J.; Podolec, J.; Komar, M.; et al. Clinical classification of rare cardiac arrhythmogenic and conduction disorders, and rare arrhythmias. Pol. Arch. Intern. Med. 2019, 129, 154–159. [Google Scholar] [CrossRef] [Green Version]
- Stevens, T.L.; Wallace, M.J.; el Refaey, M.; Roberts, J.D.; Koenig, S.N.; Mohler, P.J. Arrhythmogenic cardiomyopathy: Molecular insights for improved therapeutic design. J. Cardiovasc. Dev. Dis. 2020, 7, 21. [Google Scholar] [CrossRef]
- Fauchier, L.; Isorni, M.A.; Clementy, N.; Pierre, B.; Simeon, E.; Babuty, D. Prognostic value of programmed ventricular stimulation in Brugada syndrome according to clinical presentation: An updated meta-analysis of worldwide published data. Int. J. Cardiol. 2013, 168, 3027–3029. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aziz, H.M.; Zarzecki, M.P.; Garcia-Zamora, S.; Kim, M.S.; Bijak, P.; Tse, G.; Won, H.-H.; Matusik, P.T. Pathogenesis and Management of Brugada Syndrome: Recent Advances and Protocol for Umbrella Reviews of Meta-Analyses in Major Arrhythmic Events Risk Stratification. J. Clin. Med. 2022, 11, 1912. https://doi.org/10.3390/jcm11071912
Aziz HM, Zarzecki MP, Garcia-Zamora S, Kim MS, Bijak P, Tse G, Won H-H, Matusik PT. Pathogenesis and Management of Brugada Syndrome: Recent Advances and Protocol for Umbrella Reviews of Meta-Analyses in Major Arrhythmic Events Risk Stratification. Journal of Clinical Medicine. 2022; 11(7):1912. https://doi.org/10.3390/jcm11071912
Chicago/Turabian StyleAziz, Hasina Masha, Michał P. Zarzecki, Sebastian Garcia-Zamora, Min Seo Kim, Piotr Bijak, Gary Tse, Hong-Hee Won, and Paweł T. Matusik. 2022. "Pathogenesis and Management of Brugada Syndrome: Recent Advances and Protocol for Umbrella Reviews of Meta-Analyses in Major Arrhythmic Events Risk Stratification" Journal of Clinical Medicine 11, no. 7: 1912. https://doi.org/10.3390/jcm11071912