
Clinical Differences between Community-Acquired Mycoplasma pneumoniae Pneumonia and COVID-19 Pneumonia

Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Analysis Patients
3.2. Clinical Presentation of M. pneumoniae CAP and COVID-19 CAP
3.3. Clinical Presentation of M. pneumoniae CAP and Age- and Gender-Matched COVID-19 CAP
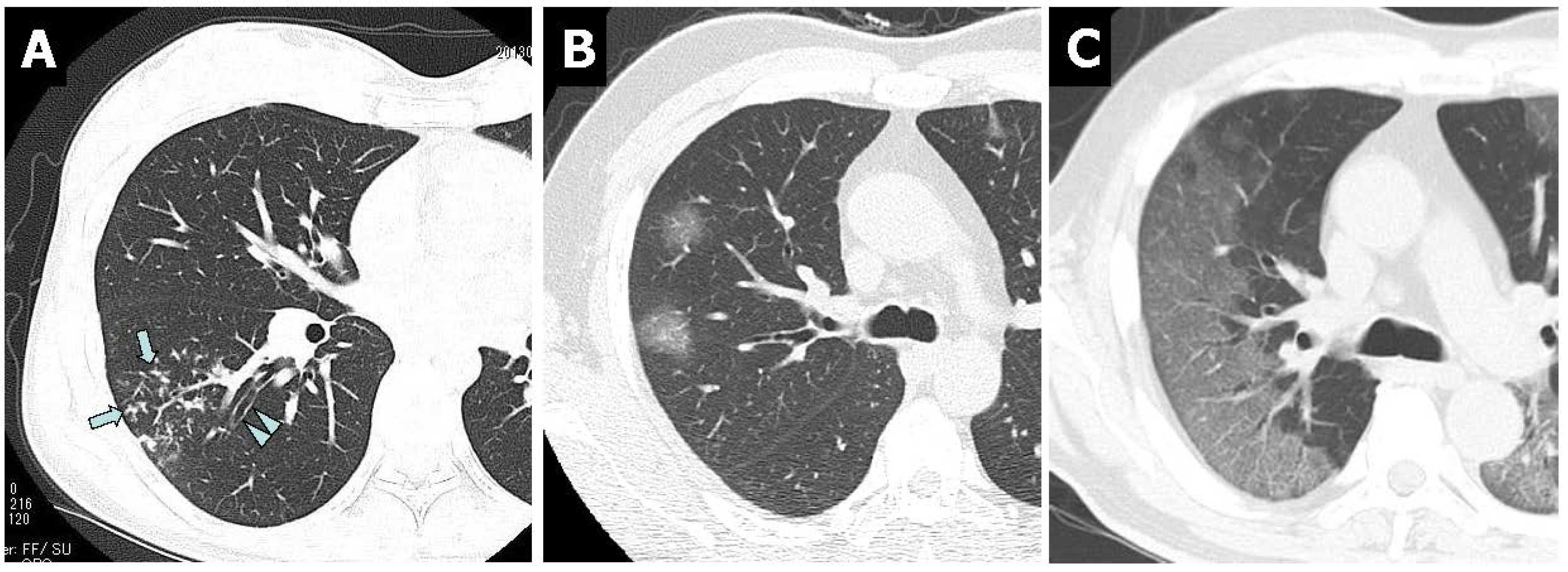
3.4. Chest CT Findings
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Waites, K.B.; Talkington, D.F. Mycoplasma pneumoniae and its role as a human pathogen. Clin. Microbiol. Rev. 2004, 17, 697–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee for The Japanese Respiratory Society guidelines for the management of respiratory infections. Guidelines for the management of community acquired pneumonia in adults, revised edition. Respirology 2006, 11 (Suppl. 3), S79–S133. [Google Scholar]
- Yamasaki, K.; Kawanami, T.; Yatera, K.; Fukuda, K.; Noguchi, S.; Nagata, S.; Nishida, C.; Kido, T.; Ishimoto, H.; Taniguchi, H.; et al. Significance of anaerobes and oral bacteria in community-acquired pneumonia. PLoS ONE 2013, 8, e63103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyashita, N.; Fukano, H.; Mouri, K.; Fukuda, M.; Yoshida, K.; Kobashi, Y.; Niki, Y.; Oka, M. Community-acquired pneumonia in Japan: A prospective ambulatory and hospitalized patient study. J. Med. Microbiol. 2005, 54, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Ishida, T.; Miyashita, N.; Nakahama, C. Clinical differentiation of atypical pneumonia using Japanese guidelines. Respirology 2007, 12, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, N.; Fukano, H.; Yoshida, K.; Niki, Y.; Matsushima, T. Is it possible to distinguish between atypical pneumonia and bacterial pneumonia?: Evaluation of the guidelines for community-acquired pneumonia in Japan. Respir. Med. 2004, 98, 952–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyashita, N.; Higa, F.; Aoki, Y.; Kikuchi, T.; Seki, M.; Tateda, K.; Maki, N.; Uchino, K.; Ogasawara, K.; Kiyota, H.; et al. Clinical presentation of Legionella pneumonia: Evaluation of clinical scoring systems and therapeutic efficacy. J. Infect. Chemother. 2017, 23, 727–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Goto, H.; Kohno, S.; Matsushima, T.; Abe, S.; Aoki, N.; Shimokata, K.; Mikasa, K.; Niki, Y. Nationwide survey on the 2005 guidelines for the management of community-acquired adult pneumonia: Validation of differentiation between bacterial pneumonia and atypical pneumonia. Respir. Investig. 2012, 50, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, Y.D.; Zhao, F.; Ren, L.L.; Song, S.F.; Liu, Y.M.; Zhang, J.Z.; Cao, B. Evaluation of the Japanese Respiratory Society guidelines for the identification of Mycoplasma pneumoniae pneumonia. Respirology 2012, 17, 1131–1136. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Ishida, T.; Togashi, K.; Niimi, A.; Koyama, H.; Ishimori, T.; Kobayashi, H.; Mishima, M. Differentiation of bacterial and non-bacterial community-acquired pneumonia by thin-section computed tomography. Eur. J. Radiol. 2009, 72, 388–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyashita, N.; Sugiu, T.; Kawai, K.; Oda, K.; Yamaguchi, T.; Ouchi, K.; Kobashi, Y.; Oka, M. Radiographic features of Mycoplasma pneumoniae pneumonia: Differential diagnosis and performance timing. BMC. Med. Imaging 2009, 9, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, H.J.A.; Kwee, T.C.; Yakar, D.; Hope, M.D.; Kwee, R.M. Chest CT imaging signature of coronavirus disease 2019 infection: In pursuit of scientific evidence. Chest 2020, 158, 1885–1895. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Zhang, N.; Xu, X. A systematic review of chest imaging in COVID-19. Quant. Imaging Med. Surg. 2020, 10, 1058–1079. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Document on reporting chest CT findings related to COVID-19: Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA. Radiol. Cardiothoracic. Imaging. 2020, 2, e200152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Xia, W.; Peng, X.; Shao, J. Features discriminating COVID-19 from community-acquired pneumonia in pediatric patients. Front. Pediatr. 2020, 8, 602083. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | M. pneumoniae | COVID-19 | p-Value |
|---|---|---|---|
| No. of patients | 210 | 956 | |
| Median age (IQR), years | 36 (27–52) | 56 (42–70) | <0.001 |
| No. of males/females | 106/104 | 599/357 | 0.001 |
| No. (%) of patients with comorbid illnesses | |||
| Chronic lung disease | 19 (9.0) | 107 (11.2) | 0.393 |
| Diabetes mellitus | 11 (5.2) | 167 (17.5) | <0.001 |
| Chronic heart disease | 6 (2.9) | 45 (4.7) | 0.269 |
| Chronic liver disease | 4 (1.9) | 24 (2.5) | 0.804 |
| Cerebrovascular disease | 3 (1.4) | 26 (2.7) | 0.338 |
| Chronic renal disease | 3 (1.4) | 28 (2.9) | 0.341 |
| Neoplastic disease | 2 (1.0) | 30 (3.1) | 0.100 |
| Autoimmune disease | 2 (1.0) | 23 (2.4) | 0.290 |
| No. (%) of patients with the following clinical signs and symptoms | |||
| Fever (≥37.0 °C) | 207 (98.6) | 822 (85.9) | <0.001 |
| Cough | 206 (98.1) | 604 (63.2) | <0.001 |
| Sputum production | 126 (60.0) | 126 (13.2) | <0.001 |
| Sore throat | 74 (35.2) | 228 (23.8) | 0.001 |
| Headache | 62 (29.5) | 121 (12.7) | <0.001 |
| Shortness of breath | 32 (15.2) | 293 (30.6) | <0.001 |
| Chest pain | 32 (15.2) | 27 (2.8) | <0.001 |
| Nausea or vomiting | 17 (8.1) | 22 (2.3) | 0.0001 |
| Runny nose | 15 (7.1) | 69 (7.2) | >0.999 |
| Joint pain | 14 (6.7) | 58 (6.1) | 0.752 |
| Muscle ache | 9 (4.3) | 30 (3.1) | 0.398 |
| Diarrhea | 5 (2.4) | 82 (8.6) | 0.001 |
| Abdominal pain | 2 (1.0) | 22 (2.3) | 0.288 |
| Loss of taste | 0 | 184 (19.2) | <0.001 |
| Anosmia | 0 | 167 (17.5) | <0.001 |
| Laboratory findings, median (IQR) | |||
| White blood cell count,/µL | 6150 (5070–8460) | 5200 (4200–6700) | 0.122 |
| C-reactive protein, mg/dL | 6.4 (3.3–11.5) | 4.4 (1.6–9.3) | 0.241 |
| Aspartate aminotransferase, U/L | 29 (21–40) | 34 (23–52) | 0.126 |
| Alanine aminotransferase, U/L | 26 (20–39) | 26 (18–43) | >0.999 |
| No. (%) of patients with each pneumonia severity score | |||
| Mild to moderate | 192 (91.4) | 865 (90.5) | 0.793 |
| Severe | 16 (7.6) | 76 (7.9) | >0.999 |
| Extremely severe | 2 (1.0) | 15 (1.6) | 0.752 |
| No. (%) of patients admitted to intensive care unit | 5 (2.4) | 290 (30.3) | <0.001 |
| No. (%) of patients with in-hospital mortality | 0 | 18 (1.9) | 0.057 |
| Variables | M. pneumoniae | COVID-19 | p-Value |
|---|---|---|---|
| No. of patients | 210 | 210 | |
| Median age (IQR), years | 36 (27–52) | 36 (27–52) | >0.999 |
| No. of males/females | 106/104 | 106/104 | >0.999 |
| No. (%) of patients with comorbid illnesses | |||
| Chronic lung disease | 19 (9.0) | 15 (7.1) | 0.592 |
| Diabetes mellitus | 11 (5.2) | 21 (10.0) | 0.097 |
| Chronic heart disease | 6 (2.9) | 4 (1.9) | 0.751 |
| Chronic liver disease | 4 (1.9) | 3 (1.4) | >0.999 |
| Cerebrovascular disease | 3 (1.4) | 3 (1.4) | >0.999 |
| Chronic renal disease | 3 (1.4) | 2 (1.0) | >0.999 |
| Neoplastic disease | 2 (1.0) | 2 (1.0) | >0.999 |
| Autoimmune disease | 2 (1.0) | 2 (1.0) | >0.999 |
| No. (%) of patients with the following clinical signs and symptoms | |||
| Fever (≥37.0 °C) | 207 (98.6) | 178 (84.8) | <0.001 |
| Cough | 206 (98.1) | 141 (67.1) | <0.001 |
| Sputum production | 126 (60.0) | 29 (13.8) | <0.001 |
| Sore throat | 74 (35.2) | 73 (34.8) | >0.999 |
| Headache | 62 (29.5) | 46 (21.9) | 0.094 |
| Shortness of breath | 32 (15.2) | 42 (20.0) | 0.249 |
| Chest pain | 32 (15.2) | 9 (4.3) | 0.0002 |
| Nausea or vomiting | 17 (8.1) | 7 (3.3) | 0.057 |
| Runny nose | 15 (7.1) | 17 (8.1) | 0.854 |
| Joint pain | 14 (6.7) | 26 (12.4) | 0.066 |
| Muscle ache | 9 (4.3) | 12 (5.7) | 0.655 |
| Diarrhea | 5 (2.4) | 14 (6.7) | 0.058 |
| Abdominal pain | 2 (1.0) | 7 (3.3) | 0.175 |
| Loss of taste | 0 | 68 (32.4) | <0.001 |
| Anosmia | 0 | 70 (33.3) | <0.001 |
| Laboratory findings, median (IQR) | |||
| White blood cell count,/µL | 6150 (5070–8460) | 5500 (4400–6200) | 0.208 |
| C-reactive protein, mg/dL | 6.4 (3.3–11.5) | 4.3 (1.8–9.0) | 0.299 |
| Aspartate aminotransferase, U/L | 29 (21–40) | 29 (22–46) | >0.999 |
| Alanine aminotransferase, U/L | 26 (20–39) | 25 (19–41) | 0.891 |
| No. (%) of patients with each pneumonia severity score | |||
| Mild to moderate | 192 (91.4) | 204 (97.1) | 0.594 |
| Severe | 16 (7.6) | 6 (2.9) | 0.046 |
| Extremely severe | 2 (1.0) | 0 | 0.499 |
| No. (%) of patients admitted to intensive care unit | 5 (2.4) | 18 (8.6) | 0.009 |
| No. (%) of patients with in-hospital mortality | 0 | 0 | >0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyashita, N.; Nakamori, Y.; Ogata, M.; Fukuda, N.; Yamura, A.; Ishiura, Y.; Nomura, S. Clinical Differences between Community-Acquired Mycoplasma pneumoniae Pneumonia and COVID-19 Pneumonia. J. Clin. Med. 2022, 11, 964. https://doi.org/10.3390/jcm11040964
Miyashita N, Nakamori Y, Ogata M, Fukuda N, Yamura A, Ishiura Y, Nomura S. Clinical Differences between Community-Acquired Mycoplasma pneumoniae Pneumonia and COVID-19 Pneumonia. Journal of Clinical Medicine. 2022; 11(4):964. https://doi.org/10.3390/jcm11040964
Chicago/Turabian StyleMiyashita, Naoyuki, Yasushi Nakamori, Makoto Ogata, Naoki Fukuda, Akihisa Yamura, Yoshihisa Ishiura, and Shosaku Nomura. 2022. "Clinical Differences between Community-Acquired Mycoplasma pneumoniae Pneumonia and COVID-19 Pneumonia" Journal of Clinical Medicine 11, no. 4: 964. https://doi.org/10.3390/jcm11040964