
Medialized versus Lateralized Center of Rotation in Reverse Total Shoulder Arthroplasty: A Systematic Review and Meta-Analysis

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Search
2.5. Data Collection Process
2.6. Data Items
2.7. Study Risk of Bias Assessment
2.8. Statistical Analysis
3. Results
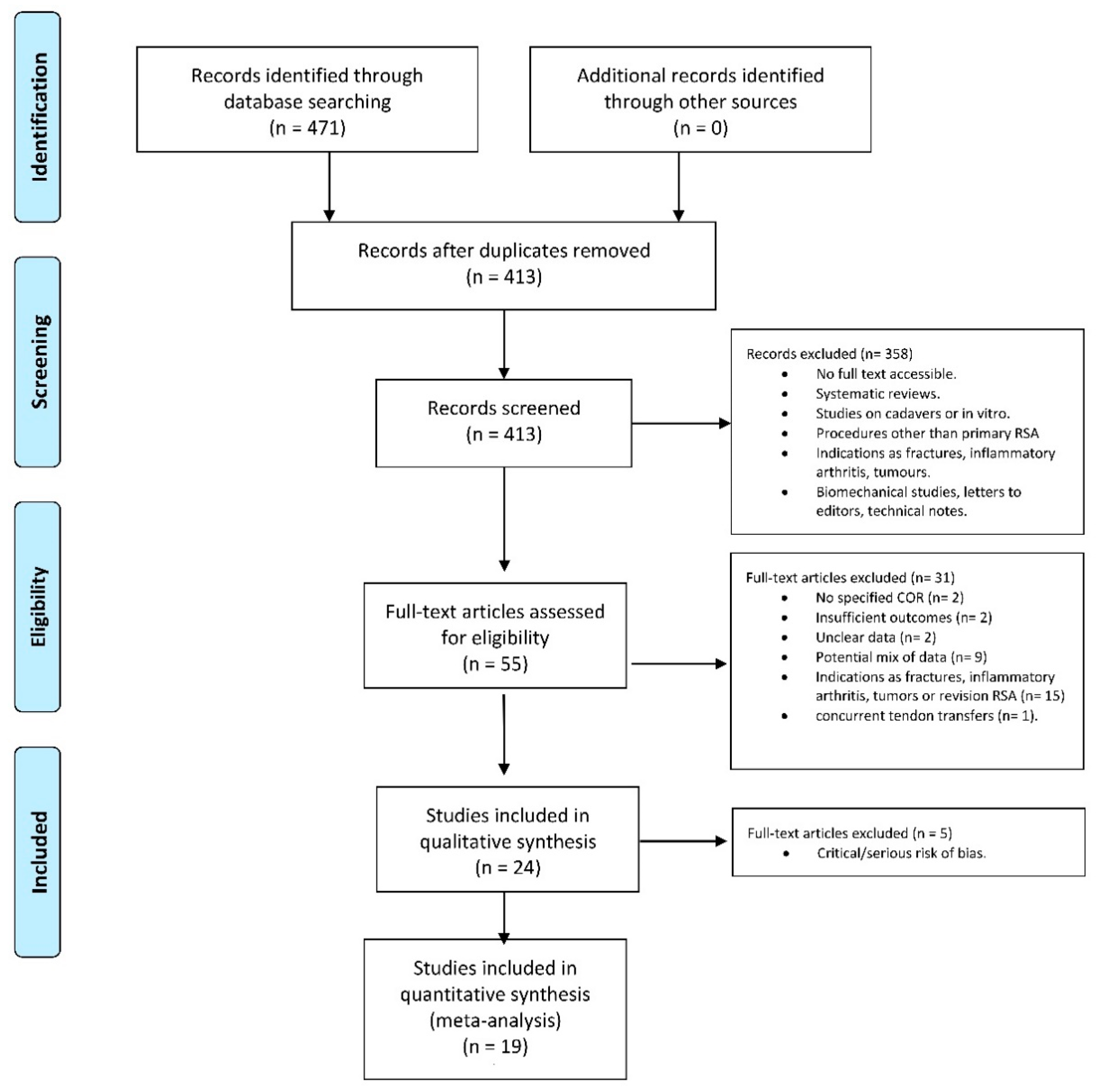
3.1. Study Selection
3.2. Study Characteristics
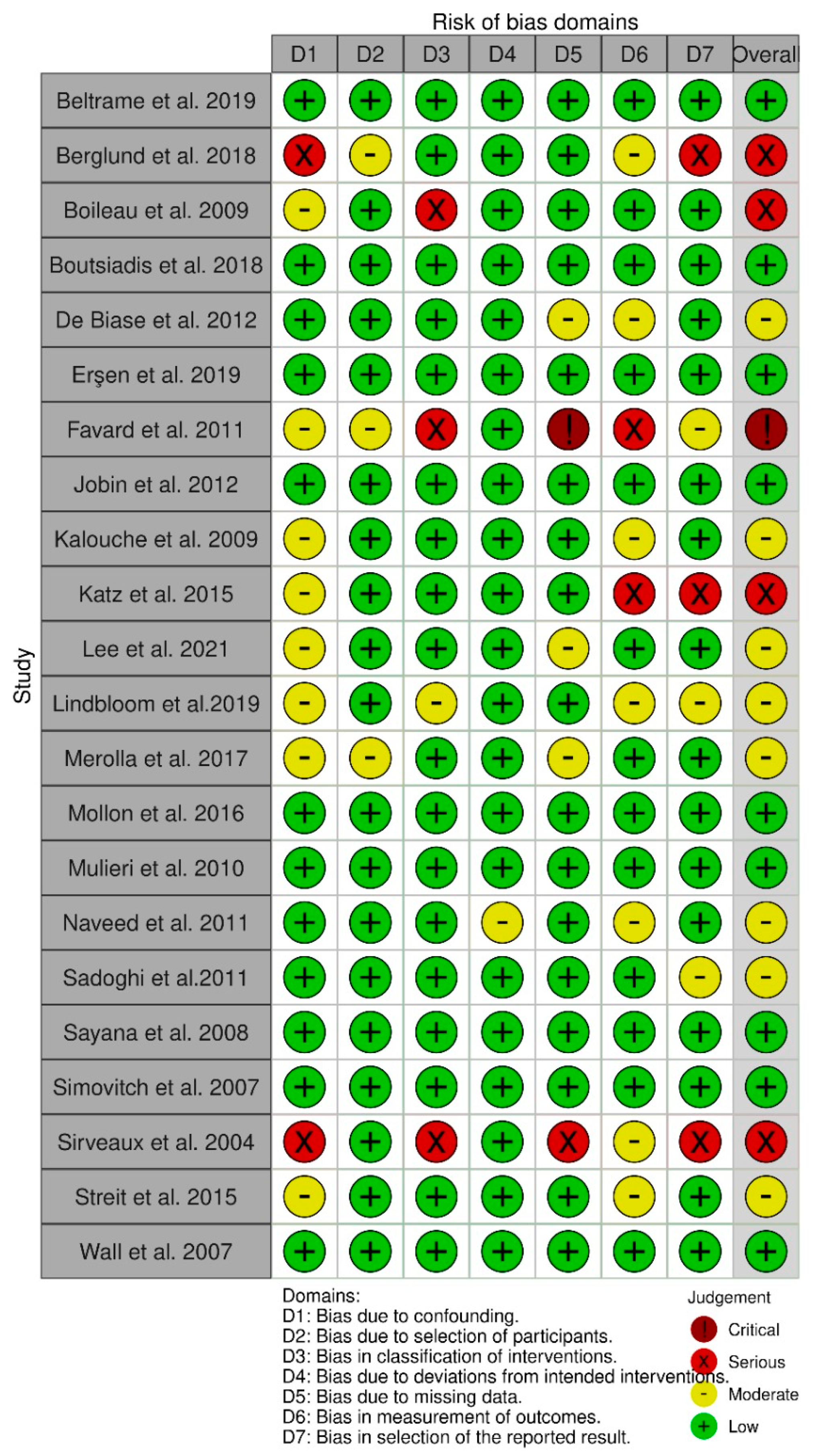
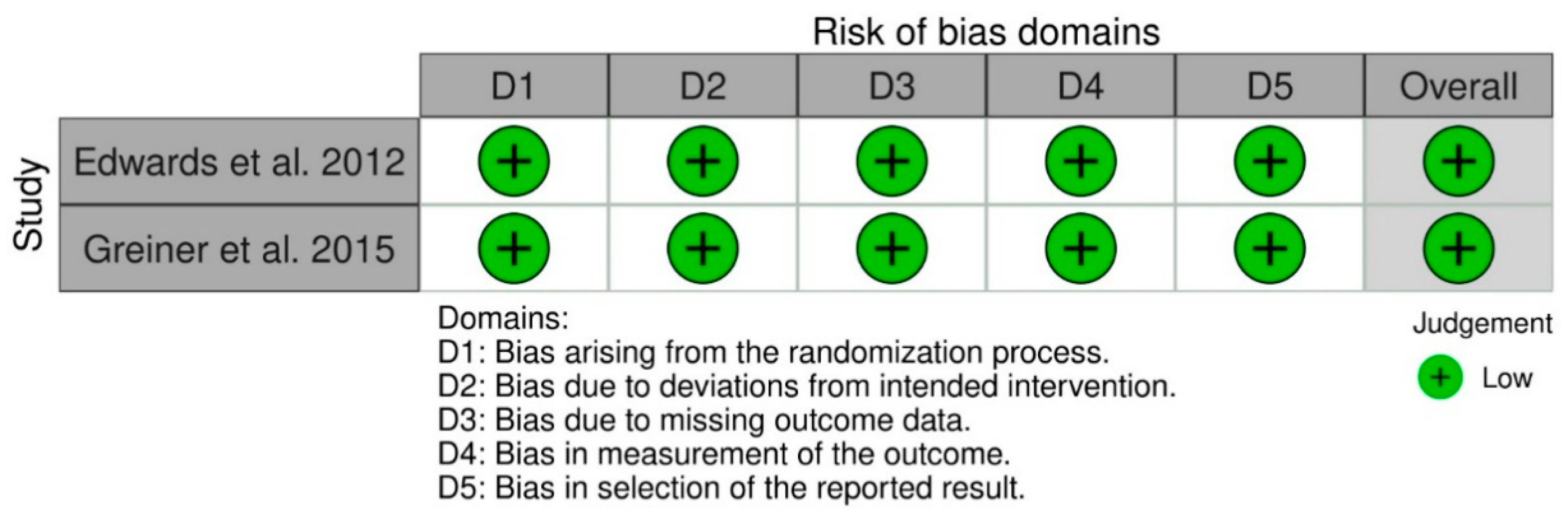
3.3. Quality of Evidence
3.4. Surgical Procedure
3.5. Meta-Analysis Results
3.5.1. Outcome Measures
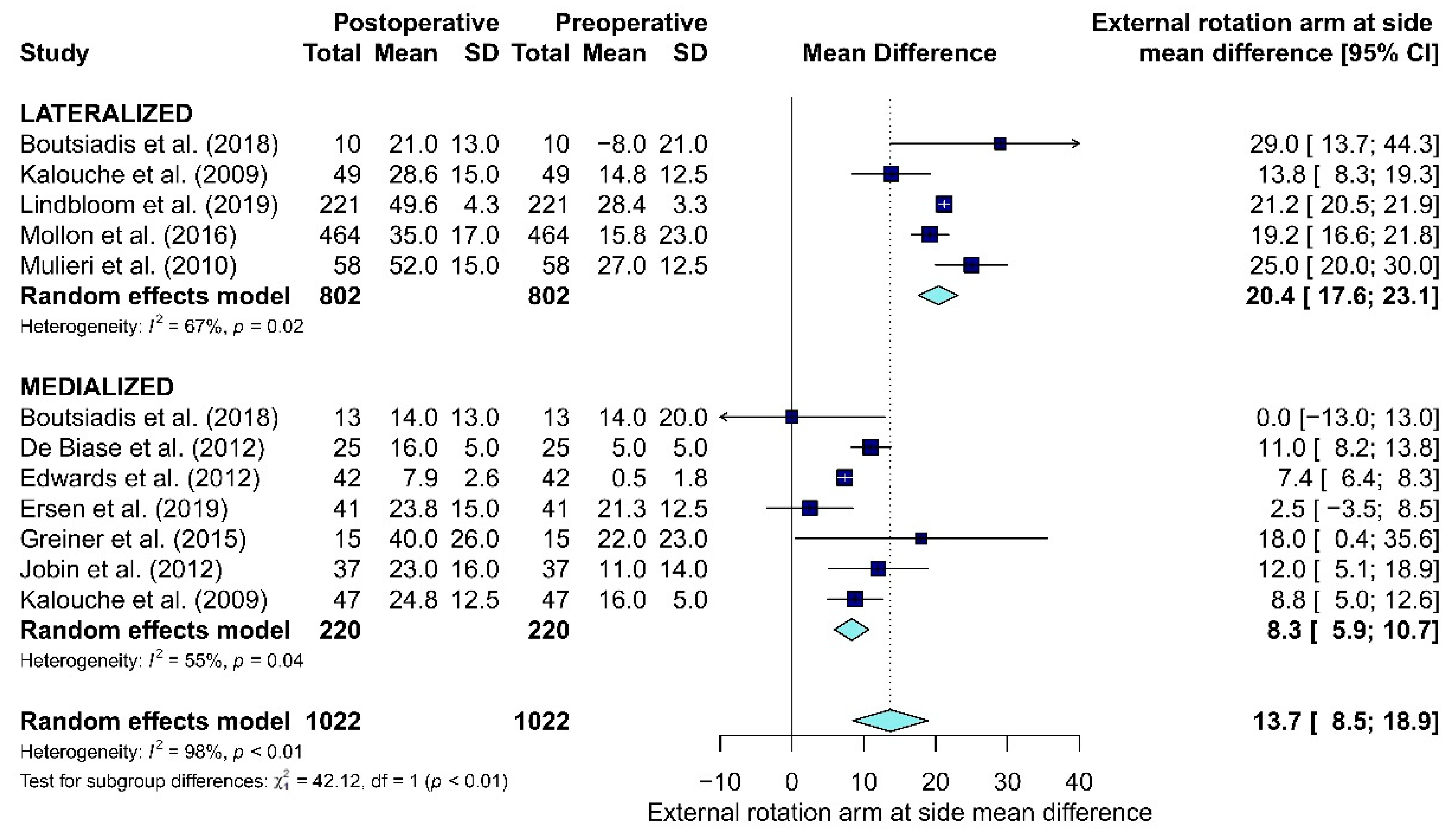
3.5.2. Active ROMs
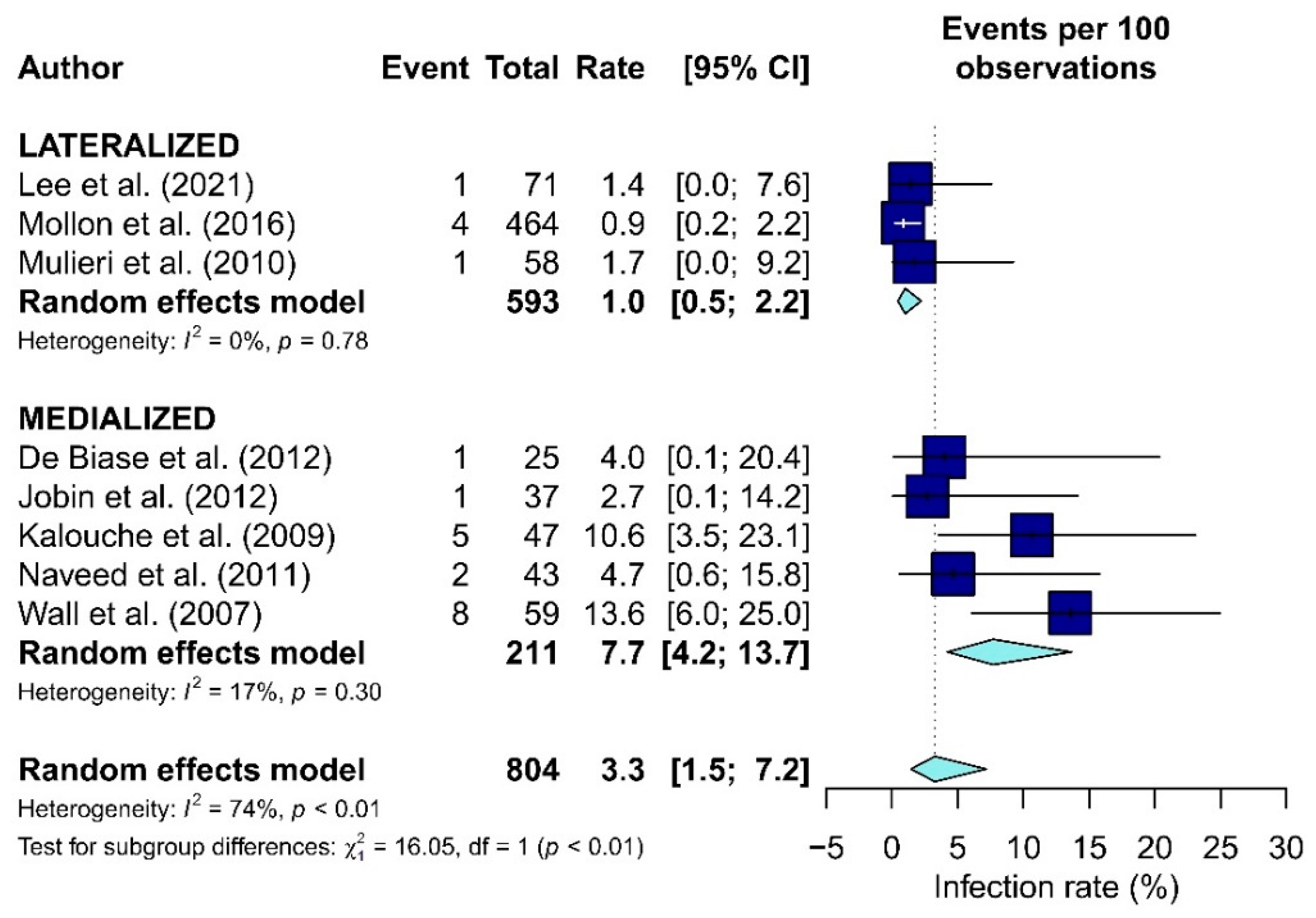
3.5.3. Complications
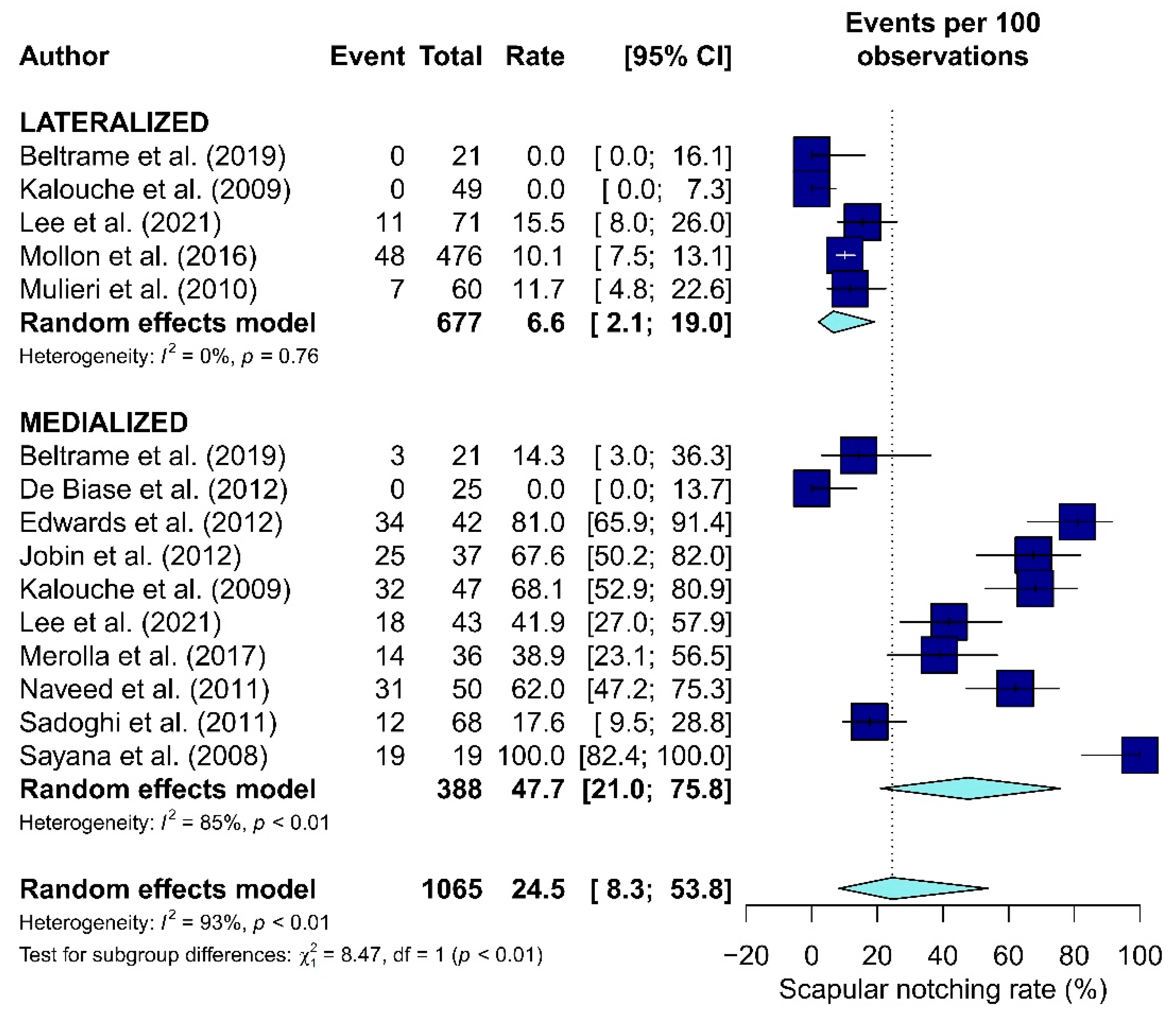
3.5.4. Scapular Notching
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Chakravarty, K.; Webley, M. Shoulder joint movement and its relationship to disability in the elderly. J. Rheumatol. 1993, 20, 1359–1361. [Google Scholar]
- Tashjian, R.Z. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin. Sports Med. 2012, 31, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Berton, A.; Longo, U.G.; De Salvatore, S.; Sciotti, G.; Santamaria, G.; Piergentili, I.; De Marinis, M.G.; Denaro, V. A Historical Analysis of Randomized Controlled Trials in the Management of Pain in Rotator Cuff Tears. J. Clin. Med. 2021, 10, 4072. [Google Scholar] [CrossRef] [PubMed]
- Berliner, J.L.; Regalado-Magdos, A.; Ma, C.B.; Feeley, B.T. Biomechanics of reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2015, 24, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Samitier, G.; Alentorn-Geli, E.; Torrens, C.; Wright, T.W. Reverse shoulder arthroplasty. Part 1: Systematic review of clinical and functional outcomes. Int. J. Shoulder Surg. 2015, 9, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrillo, S.; Longo, U.G.; Papalia, R.; Denaro, V. Reverse shoulder arthroplasty for massive irreparable rotator cuff tears and cuff tear arthropathy: A systematic review. Musculoskelet. Surg. 2017, 101, 105–112. [Google Scholar] [CrossRef]
- Cho, C.H.; Jung, J.W.; Na, S.S.; Bae, K.C.; Lee, K.J.; Kim, D.H. Is Acromial Fracture after Reverse Total Shoulder Arthroplasty a Negligible Complication?: A Systematic Review. Clin. Orthop. Surg. 2019, 11, 427–435. [Google Scholar] [CrossRef]
- Youn, S.M.; Lee, H.S.; Rhee, S.M.; Rhee, Y.G. Medialized vs. lateralized humeral implant in reverse total shoulder arthroplasty: The comparison of outcomes in pseudoparalysis with massive rotator cuff tear. J. Shoulder Elb. Surg. 2021, in press. [Google Scholar] [CrossRef]
- Kirzner, N.; Paul, E.; Moaveni, A. Reverse shoulder arthroplasty vs BIO-RSA: Clinical and radiographic outcomes at short term follow-up. J. Orthop. Surg. Res. 2018, 13, 256. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.S.; Gaal, B.T.; Roche, A.M.; Namdari, S.; Grawe, B.M.; Lawler, M.; Dalton, S.; King, J.J.; Helmkamp, J.; Garrigues, G.E.; et al. The modern reverse shoulder arthroplasty and an updated systematic review for each complication: Part I. JSES Int. 2020, 4, 929–943. [Google Scholar] [CrossRef]
- Boutsiadis, A.; Lenoir, H.; Denard, P.J.; Panisset, J.C.; Brossard, P.; Delsol, P.; Guichard, F.; Barth, J. The lateralization and distalization shoulder angles are important determinants of clinical outcomes in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2018, 27, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Boileau, P.; Moineau, G.; Roussanne, Y.; O’Shea, K. Bony increased-offset reversed shoulder arthroplasty: Minimizing scapular impingement while maximizing glenoid fixation. Clin. Orthop. Relat. Res. 2011, 469, 2558–2567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frankle, M.; Siegal, S.; Pupello, D.; Saleem, A.; Mighell, M.; Vasey, M. The Reverse Shoulder Prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency. A minimum two-year follow-up study of sixty patients. J. Bone Jt. Surg. Am. 2005, 87, 1697–1705. [Google Scholar] [CrossRef]
- Kalouche, I.; Sevivas, N.; Wahegaonker, A.; Sauzieres, P.; Katz, D.; Valenti, P. Reverse shoulder arthroplasty: Does reduced medialisation improve radiological and clinical results? Acta Orthop. Belg. 2009, 75, 158–166. [Google Scholar]
- Valenti, P.; Sauzières, P.; Katz, D.; Kalouche, I.; Kilinc, A.S. Do less medialized reverse shoulder prostheses increase motion and reduce notching? Clin. Orthop. Relat. Res. 2011, 469, 2550–2557. [Google Scholar] [CrossRef] [Green Version]
- Lädermann, A.; Denard, P.J.; Boileau, P.; Farron, A.; Deransart, P.; Terrier, A.; Ston, J.; Walch, G. Effect of humeral stem design on humeral position and range of motion in reverse shoulder arthroplasty. Int. Orthop. 2015, 39, 2205–2213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berton, A.; De Salvatore, S.; Candela, V.; Cortina, G.; Lo Presti, D.; Massaroni, C.; Petrillo, S.; Denaro, V. Delayed Rehabilitation Protocol after Rotator Cuff Repair. Osteology 2021, 1, 29–38. [Google Scholar] [CrossRef]
- Jobin, C.M.; Brown, G.D.; Bahu, M.J.; Gardner, T.R.; Bigliani, L.U.; Levine, W.N.; Ahmad, C.S. Reverse total shoulder arthroplasty for cuff tear arthropathy: The clinical effect of deltoid lengthening and center of rotation medialization. J. Shoulder Elb. Surg. 2012, 21, 1269–1277. [Google Scholar] [CrossRef]
- Roche, C.P.; Diep, P.; Hamilton, M.; Crosby, L.A.; Flurin, P.H.; Wright, T.W.; Zuckerman, J.D.; Routman, H.D. Impact of inferior glenoid tilt, humeral retroversion, bone grafting, and design parameters on muscle length and deltoid wrapping in reverse shoulder arthroplasty. Bull. Hosp. Jt. Dis. 2013, 71, 284–293. [Google Scholar]
- Cho, N.S.; Nam, J.H.; Hong, S.J.; Kim, T.W.; Lee, M.G.; Ahn, J.T.; Rhee, Y.G. Radiologic Comparison of Humeral Position according to the Implant Designs Following Reverse Shoulder Arthroplasty: Analysis between Medial Glenoid/Medial Humerus, Lateral Glenoid/Medial Humerus, and Medial Glenoid/Lateral Humerus Designs. Clin. Shoulder Elb. 2018, 21, 192–199. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M.A.; Roche, C.P.; Diep, P.; Flurin, P.H.; Routman, H.D. Effect of prosthesis design on muscle length and moment arms in reverse total shoulder arthroplasty. Bull. Hosp. Jt. Dis. 2013, 71 (Suppl. S2), S31–S35. [Google Scholar]
- Routman, H.D. The role of subscapularis repair in reverse total shoulder arthroplasty. Bull. Hosp. Jt. Dis. 2013, 71 (Suppl. S2), 108–112. [Google Scholar]
- Helmkamp, J.K.; Bullock, G.S.; Amilo, N.R.; Guerrero, E.M.; Ledbetter, L.S.; Sell, T.C.; Garrigues, G.E. The clinical and radiographic impact of center of rotation lateralization in reverse shoulder arthroplasty: A systematic review. J. Shoulder Elb. Surg. 2018, 27, 2099–2107. [Google Scholar] [CrossRef]
- Costantini, O.; Choi, D.S.; Kontaxis, A.; Gulotta, L.V. The effects of progressive lateralization of the joint center of rotation of reverse total shoulder implants. J. Shoulder Elb. Surg. 2015, 24, 1120–1128. [Google Scholar] [CrossRef]
- Greiner, S.; Schmidt, C.; Herrmann, S.; Pauly, S.; Perka, C. Clinical performance of lateralized versus non-lateralized reverse shoulder arthroplasty: A prospective randomized study. J. Shoulder Elb. Surg. 2015, 24, 1397–1404. [Google Scholar] [CrossRef]
- Gutiérrez, S.; Levy, J.C.; Lee, W.E.; Keller, T.S.; Maitland, M.E. Center of rotation affects abduction range of motion of reverse shoulder arthroplasty. Clin. Orthop. Relat. Res. 2007, 458, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Henninger, H.B.; Barg, A.; Anderson, A.E.; Bachus, K.N.; Burks, R.T.; Tashjian, R.Z. Effect of lateral offset center of rotation in reverse total shoulder arthroplasty: A biomechanical study. J. Shoulder Elb. Surg. 2012, 21, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Lädermann, A.; Walch, G.; Lubbeke, A.; Drake, G.N.; Melis, B.; Bacle, G.; Collin, P.; Edwards, T.B.; Sirveaux, F. Influence of arm lengthening in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2012, 21, 336–341. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Sirveaux, F.; Favard, L.; Oudet, D.; Huquet, D.; Walch, G.; Molé, D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J. Bone Jt. Surg Br. 2004, 86, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Streit, J.J.; Shishani, Y.; Gobezie, R. Medialized Versus Lateralized Center of Rotation in Reverse Shoulder Arthroplasty. Orthopedics 2015, 38, e1098–e1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Merolla, G.; Walch, G.; Ascione, F.; Paladini, P.; Fabbri, E.; Padolino, A.; Porcellini, G. Grammont humeral design versus onlay curved-stem reverse shoulder arthroplasty: Comparison of clinical and radiographic outcomes with minimum 2-year follow-up. J. Shoulder Elb. Surg. 2018, 27, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chun, Y.M.; Kim, D.S.; Lee, D.H.; Shin, S.J. Early restoration of shoulder function in patients with the Grammont prosthesis compared to lateralized humeral design in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2021, 30, 2533–2542. [Google Scholar] [CrossRef]
- Mulieri, P.; Dunning, P.; Klein, S.; Pupello, D.; Frankle, M. Reverse shoulder arthroplasty for the treatment of irreparable rotator cuff tear without glenohumeral arthritis. J. Bone Jt. Surg. Am. 2010, 92, 2544–2556. [Google Scholar] [CrossRef]
- Wall, B.; Nové-Josserand, L.; O’Connor, D.P.; Edwards, T.B.; Walch, G. Reverse total shoulder arthroplasty: A review of results according to etiology. J. Bone Jt. Surg. Am. 2007, 89, 1476–1485. [Google Scholar] [CrossRef]
- Katz, D.; Valenti, P.; Kany, J.; Elkholti, K.; Werthel, J.D. Does lateralisation of the centre of rotation in reverse shoulder arthroplasty avoid scapular notching? Clinical and radiological review of one hundred and forty cases with forty five months of follow-up. Int. Orthop. 2016, 40, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Boileau, P.; Gonzalez, J.F.; Chuinard, C.; Bicknell, R.; Walch, G. Reverse total shoulder arthroplasty after failed rotator cuff surgery. J. Shoulder Elb. Surg. 2009, 18, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Favard, L.; Levigne, C.; Nerot, C.; Gerber, C.; De Wilde, L.; Mole, D. Reverse prostheses in arthropathies with cuff tear: Are survivorship and function maintained over time? Clin. Orthop. Relat. Res. 2011, 469, 2469–2475. [Google Scholar] [CrossRef] [Green Version]
- Mollon, B.; Mahure, S.A.; Roche, C.P.; Zuckerman, J.D. Impact of scapular notching on clinical outcomes after reverse total shoulder arthroplasty: An analysis of 476 shoulders. J. Shoulder Elb. Surg. 2017, 26, 1253–1261. [Google Scholar] [CrossRef]
- Lindbloom, B.J.; Christmas, K.N.; Downes, K.; Simon, P.; McLendon, P.B.; Hess, A.V.; Mighell, M.A.; Frankle, M.A. Is there a relationship between preoperative diagnosis and clinical outcomes in reverse shoulder arthroplasty? An experience in 699 shoulders. J. Shoulder Elb. Surg. 2019, 28, S110–S117. [Google Scholar] [CrossRef]
- Beltrame, A.; Di Benedetto, P.; Cicuto, C.; Cainero, V.; Chisoni, R.; Causero, A. Onlay versus Inlay humeral steam in Reverse Shoulder Arthroplasty (RSA): Clinical and biomechanical study. Acta Biomed. 2019, 90, 54–63. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Edwards, T.B.; Trappey, G.J.; Riley, C.; O’Connor, D.P.; Elkousy, H.A.; Gartsman, G.M. Inferior tilt of the glenoid component does not decrease scapular notching in reverse shoulder arthroplasty: Results of a prospective randomized study. J. Shoulder Elb. Surg. 2012, 21, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Berglund, D.D.; Rosas, S.; Triplet, J.J.; Kurowicki, J.; Horn, B.; Levy, J.C. Restoration of External Rotation Following Reverse Shoulder Arthroplasty without Latissimus Dorsi Transfer. JB JS Open Access 2018, 3, e0054. [Google Scholar] [CrossRef]
- Sadoghi, P.; Vavken, P.; Leithner, A.; Hochreiter, J.; Weber, G.; Pietschmann, M.F.; Müller, P.E. Impact of previous rotator cuff repair on the outcome of reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2011, 20, 1138–1146. [Google Scholar] [CrossRef]
- Sayana, M.K.; Kakarala, G.; Bandi, S.; Wynn-Jones, C. Medium term results of reverse total shoulder replacement in patients with rotator cuff arthropathy. Ir. J. Med. Sci. 2009, 178, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Naveed, M.A.; Kitson, J.; Bunker, T.D. The Delta III reverse shoulder replacement for cuff tear arthropathy: A single-centre study of 50 consecutive procedures. J. Bone Jt. Surg. Br. 2011, 93, 57–61. [Google Scholar] [CrossRef]
- De Biase, C.F.; Delcogliano, M.; Borroni, M.; Castagna, A. Reverse total shoulder arthroplasty: Radiological and clinical result using an eccentric glenosphere. Musculoskelet. Surg. 2012, 96 (Suppl. S1), S27–S34. [Google Scholar] [CrossRef] [PubMed]
- Simovitch, R.W.; Helmy, N.; Zumstein, M.A.; Gerber, C. Impact of fatty infiltration of the teres minor muscle on the outcome of reverse total shoulder arthroplasty. J. Bone Jt. Surg. Am. 2007, 89, 934–939. [Google Scholar] [CrossRef]
- Erşen, A.; Birişik, F.; Bayram, S.; Şahinkaya, T.; Demirel, M.; Atalar, A.C.; Demirhan, M. Isokinetic Evaluation of Shoulder Strength and Endurance after Reverse Shoulder Arthroplasty: A Comparative Study. Acta Orthop. Traumatol. Turc. 2019, 53, 452–456. [Google Scholar] [CrossRef]
- Baulot, E.; Chabernaud, D.; Grammont, P.M. Results of Grammont’s inverted prosthesis in omarthritis associated with major cuff destruction. Apropos of 16 cases. Acta Orthop. Belg. 1995, 61 (Suppl. S1), 112–119. [Google Scholar]
- Alentorn-Geli, E.; Samitier, G.; Torrens, C.; Wright, T.W. Reverse shoulder arthroplasty. Part 2: Systematic review of reoperations, revisions, problems, and complications. Int. J. Shoulder Surg. 2015, 9, 60–67. [Google Scholar] [CrossRef]
- Boileau, P.; Watkinson, D.; Hatzidakis, A.M.; Hovorka, I. Neer Award 2005: The Grammont reverse shoulder prosthesis: Results in cuff tear arthritis, fracture sequelae, and revision arthroplasty. J. Shoulder Elb. Surg. 2006, 15, 527–540. [Google Scholar] [CrossRef]
- Longo, U.G.; Candela, V.; De Salvatore, S.; Piergentili, I.; Panattoni, N.; Casciani, E.; Faldetta, A.; Marchetti, A.; De Marinis, M.G.; Denaro, V. Arthroscopic Rotator Cuff Repair Improves Sleep Disturbance and Quality of Life: A Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 3797. [Google Scholar] [CrossRef] [PubMed]
- Panattoni, N.; Longo, U.G.; De Salvatore, S.; Castaneda, N.S.C.; Risi Ambrogioni, L.; Piredda, M.; De Marinis, M.G.; Denaro, V. The influence of psychosocial factors on patient-reported outcome measures in rotator cuff tears pre- and post-surgery: A systematic review. Qual. Life Res. 2021, 1–26. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; De Salvatore, S.; Piergentili, I.; Casciani, E.; Faldetta, A.; De Marinis, M.G.; Denaro, V. Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Pittsburgh Sleep Quality Index in Patients Who Underwent Rotator Cuff Tear Repair. Int. J. Environ. Res. Public Health 2021, 18, 8666. [Google Scholar] [CrossRef]
- Werthel, J.D.; Walch, G.; Vegehan, E.; Deransart, P.; Sanchez-Sotelo, J.; Valenti, P. Lateralization in reverse shoulder arthroplasty: A descriptive analysis of different implants in current practice. Int. Orthop. 2019, 43, 2349–2360. [Google Scholar] [CrossRef] [PubMed]
- Nabergoj, M.; Onishi, S.; Lädermann, A.; Kalache, H.; Trebše, R.; Bothorel, H.; Collin, P. Can Lateralization of Reverse Shoulder Arthroplasty Improve Active External Rotation in Patients with Preoperative Fatty Infiltration of the Infraspinatus and Teres Minor? J. Clin Med. 2021, 10, 4130. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Type of Study | LOE | Sample Size TOT. | Sample Size M | Sample Size L | Shoulders | Mean Age ± SD (Range) | Mean Age M | Mean Age L | Gender TOT. | Gender M | Gender L | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | Males | Females | Males | Females | ||||||||||
| Beltrame et al., 2019 | PS | IV | 42 | 21 | 21 | 42 | 73 ± 8.2 (55–88) | 77 ± 3.8 (68–85) | 12 | 30 | 6 | 15 | 6 | 15 | |
| Berglund et al., 2018 | RS; CS | IV | 24 | / | 24 | 24 | / | / | |||||||
| Boileau et al., 2009 | RS; CS | IV | 40 | 40 | / | 42 | 70 (48–82) | 70 (48–82) | / | 7 | 33 | 7 | 33 | / | / |
| Boutsiadis et al., 2018 | PG | II | 46 | 13 (I = 13) | 10 (II = 10) | 23 | 77 ± 7.5 (62–90) | 77 ± 2 (I) | 77 ± 2 (II) | 9 | 37 | ||||
| De Biase et al., 2012 | RS; CS | IV | 25 | 25 | / | 25 | 74.8 (69–87) | 74.8 (69–87) | / | 6 | 19 | 6 | 19 | / | / |
| Edwards et al., 2012 | RCT | I | 42 | 42 (T = 20, Nt = 22) | / | 42 | 69.0 | 71.8 ± 8.0 (T) 66.3 ± 9.8 (Nt) | / | 19 | 23 | 10 (T) 9 (Nt) | 10 (T) 13 (Nt) | ||
| Erșen et al., 2019 | RS; C | III | 41 | 41 | / | 41 | 70.8 (57–84) | 70.8 (57–84) | / | 5 | 36 | 5 | 36 | / | / |
| Favard et al., 2011 | RS; CS | IV | 489 | 464 | / | 509 | 76.1 (50–103) | 76.1 (50–103) | / | ||||||
| Greiner et al., 2015 | RCT | I | 15 | 15 | / | 15 | 75.4 (66–88) | 7 | 8 | 7 | 8 | / | / | ||
| Jobin et al., 2012 | PS; C | II | 37 | 37 | / | 37 | 76 (60–95) | 76 (60–95) | / | 10 | 27 | 10 | 27 | / | / |
| Kalouche et al., 2009 | RS; C | III | 96 | 47 | 49 | 96 | 73.3 (58–88) | 74.9 (52–89) | 22 | 74 | 11 | 36 | 11 | 38 | |
| Katz et al., 2015 | RS; CS | IV | 134 | / | 134 | 140 | 72 (52–90) | / | 72 (52–90) | 34 | 100 | / | / | 34 | 100 |
| Lee et al., 2021 | RS; C | III | 114 | 43 | 71 | 114 | 74.6 ± 4.9 | 73.7 ± 5.4 | 18 | 96 | 7 | 36 | 11 | 60 | |
| Lindbloom et al., 2019 | RS; C | III | 221 | / | 221 | 221 | / | 88 | 133 | / | / | 88 | 133 | ||
| Merolla et al., 2017 | RS; C | III | 36 | 36 | / | 36 | 75.8 (55–88) | / | 10 | 26 | 10 | 26 | / | / | |
| Mollon et al., 2016 | RS; C | III | 464 | / | 464 | 476 | 72.5 (53–90) | / | 72.5 (53–90) | 164 | 312 | / | / | 164 | 312 |
| Mulieri et al., 2010 | RS; CS | IV | 58 | / | 58 | 60 | 71 (52–88) | / | 71 (52–88) | 16 | 42 | / | / | 16 | 42 |
| Naveed et al., 2011 | RS; CS | IV | 43 | 43 | / | 50 | 81 (59–95) | 81 (59–95) | / | 7 | 36 | 7 | 36 | / | / |
| Sadoghi et al., 2011 | CC | III | 66 | 66 | / | 68 | 66 (53–84) | 66 (53–84) | / | 30 | 36 | 30 | 36 | / | / |
| Sayana et al., 2008 | RS; CS | IV | 18 | 18 | / | 19 | 72.8 (66–80) | 72.8 (66–80) | / | 6 | 12 | 6 | 12 | / | / |
| Simovitch et al., 2007 | PG | II | 42 | 42 | / | 42 | 71.0 (54–85) | 71.0 | / | 11 | 31 | 11 | 31 | / | / |
| Sirveaux et al., 2004 | RS; CS | IV | 77 | 77 | / | 77 | 72.8 (60–86) | 72.8 | / | 14 | 63 | 14 | 73 | / | / |
| Streit et al., 2015 | RS; CC | III | 28 (10 CG) | 9 | 9 | 28 | 70.6 + 74.7 | 70.9 | 70.4 | 5 + 6 | 13 + 4 | 3 | 6 | 2 | 7 |
| Wall et al., 2007 | PG | II | 59 | 59 | / | 59 | / | / | / | ||||||
| Author and Year | Surgical Approach | Prosthesis Design | Surgical Characteristics | Follow Up (Months) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Glenosphere Size (mm) | Glenoid Tilt | Humeral Neck Shaft Angle (°) | Mean | Range Max. | Range Min. | ||||||||||
| M | L | M | L | M | L | M | L | M | L | M | L | M | L | ||
| Beltrame et al., 2019 | Deltopectoral | SMR | Ascend Flex | 155 | 145 | 12 | 12 | ||||||||
| Berglund et al., 2018 | Deltopectoral | / | RSP | / | 32, 32–4, 36, 36–4 | / | / | 135 | / | 43.4 | / | 77 | / | 24 | |
| Boileau et al., 2009 | Deltopectoral (69%) Anterosuperior (31%) | Delta (81%) Aequalis (19%) | / | 36 (95%) 42 (5%) | / | / | / | 50 | / | 119 | / | 24 | / | ||
| Boutsiadis et al., 2018 | Deltopectoral | Aequalis (I) | Ascend Flex (II) | 36 (40), 32 (6) | / | Inferior (10°) | / | 155 (I) | 145 (II) | 39 ± 18 | / | 84 | / | 24 | / |
| De Biase et al., 2012 | Deltopectoral | SMR | / | 36 | / | / | / | 27.5 | / | 46 | / | 24 | / | ||
| Edwards et al., 2012 | Deltopectoral | Aequalis | / | 36 | / | Inferior (10°), None | / | 155 | / | 21 | / | / | 12 | / | |
| Erșen et al., 2019 | Deltopectoral | Delta XTEND | / | / | / | / | 34 | / | 67 | / | 12 | ||||
| Favard et al., 2011 | Anterosuperior (in 301) Deltopectoral (215) Transacromial (in 11) | Delta (in 461) Aequalis (in 66) | / | / | / | / | 90 | / | / | 24 | / | ||||
| Greiner et al., 2015 | Deltopectoral | Aequalis | Aequalis | 36 | 22 ± 8.1 | / | 24 | / | 3 | / | |||||
| Jobin et al., 2012 | Deltopectoral | Zimmer (27) Delta III (7) Aequalis (3) | / | / | Inferior (3° ± 12) | / | / | 16 ± 10 | / | 26 | / | 6 | / | ||
| Kalouche et al., 2009 | Superolateral (M 44, L 41) Deltopectoral (M 3, L 8) | Delta III | Arrow | 36 | 42.8 | 19.1 | 120 | 40 | 12 | 12 | |||||
| Katz et al., 2015 | Superior (82.1%) Deltopectoral (17.8%) | / | Arrow | / | 36 (83%) | / | Slightly Inferior | / | 155 | / | 45 | / | 120 | / | 24 |
| Lee et al., 2021 | Deltopectoral | Aequalis II | Equinoxe | 36 | 36 | 155 | 145 | 24 | 3 | ||||||
| Lindbloom 2019 | Deltopectoral | / | RSP Mononblock AltiVate | / | / | 135 | / | / | / | ||||||
| Merolla et al., 2017 | Deltopectoral | Aequalis II | 36, 42 | / | Centered, Inferior | / | 155 | / | 35.1 | / | 49 | / | 24 | / | |
| Mollon et al., 2016 | / | Equinoxe | 38 × 21 (256) 38 × 25 (10) 42 × 23 (189) 42 × 27 (11) 46 × 25 (10) | / | Not Inferior | / | 145 | / | 38 | / | 93 | / | 22 | ||
| Mulieri et al., 2010 | Deltopectoral | RSP | / | 52 | / | 101 | / | 24 | |||||||
| Naveed et al., 2011 | Deltopectoral Superior | Delta III | / | 42 (men) 36 (women) | / | / | / | 39 | / | 81 | / | 8 | / | ||
| Sadoghi et al., 2011 | Deltopectoral | Delta | / | 36 | / | 150 | / | 42 | / | 96 | / | 24 | / | ||
| Sayana et al., 2008 | Transacromial Deltopectoral | Delta III | / | / | / | / | 30 | / | 66 | / | 18 | / | |||
| Simovitch et al., 2007 | Deltopectoral | Delta III | / | 36 | / | / | / | 43 | 96 | 24 | |||||
| Sirveaux et al., 2004 | Superolateral (72%) Deltopectoral 19% Transacromial (3.7%) Mixed (3.7%) | / | 42 (3.7%) | / | / | / | 44.5 | / | 24 | / | 97 | / | |||
| Streit et al., 2015 | Deltopectoral | Aequalis | Encore | 36 | 32/−4 to 36 | 155 | 135 | 9.6 | 6.6 | ||||||
| Wall et al., 2007 | Deltopectoral (98.7%) | Delta III, Aequalis | / | 40 | 86 | 24 (81.6%) | |||||||||
| Author and Year | Constant-Murley Score | Absolute Ases Score | Simple Shoulder Test | Oxford Shoulder Score | Visual Analog Scale For Pain | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| L | M | L | M | L | M | L | M | L | M | ||||||||||||
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | ||
| Beltrame et al., 2019 | 39 | 71 | 41 | 70 | |||||||||||||||||
| Berglund et al., 2018 | |||||||||||||||||||||
| Boileau et al., 2009 | / | / | 25.4 (7–59) | 55.8 (0–11) | / | / | / | / | / | / | / | / | 3.3 (0–11) | 11.1 (3–15) | |||||||
| Boutsiadis et al., 2018 | II = 21 ± 2.5 (8–30) | 67 ± 4 (41–86) | I = 23 ± 3 (12–46) | 62 ± 3 (45–71) | 79 ± 5 (53–100) | 75 ± 4 (53–98) | 7 ± 1 (82–12) | 7 ± 0.5 (4–11) | |||||||||||||
| De Biase et al., 2012 | / | / | 30 (24–40) | 64 (56–74) | / | / | / | / | / | / | / | / | |||||||||
| Edwards et al., 2012 | T | 13.1 ± 9.2 | 63.6 ± 12.3 | / | / | 56.3 ± 10.6 | 78.9 ± 10.8 | / | / | / | / | / | / | ||||||||
| Nt | / | / | 15.7 ± 10.8 | 71.4 ± 14.9 | / | / | 59.6 ± 5.5 | 86.5 ± 11.6 | / | / | / | / | / | / | |||||||
| Erșen et al., 2019 | 38 ± 14 | 65 ± 11 | |||||||||||||||||||
| Favard et al., 2011 | / | / | 23.9 ± 9.9 | 61.5 ± 16.9 | / | / | / | / | / | / | / | / | 3.3 ± 3.3 | 12.2 ± 3.7 | |||||||
| Greiner et al., 2015 | / | / | 26.1 ± 15.1 | 61.5 ± 16.0 | |||||||||||||||||
| Jobin et al., 2012 | / | / | / | / | 24 ± 14 | 69 ± 24 | / | / | 2.0 ± 1.9 | 7.5 ± 2.9 | / | / | / | / | |||||||
| Kalouche et al., 2009 | 24.6 (11–40) | 62.2 (49–75) | 28.6 (14–45) | 66.0 (50–86) | |||||||||||||||||
| Katz et al., 2015 | 26 (11–53) | 64 (26–85) | / | / | / | / | 8.66 | / | / | / | / | 3 (0–12) | 13,7 (5–15) | / | / | ||||||
| Lee et al., 2021 | 69 ± 10.7 | / | 68.5 ± 10.2 | 79.0 ± 9.7 | 78.1 ± 10.2 | / | 1.6 ± 1.3 | 1.7 ± 1.5 | |||||||||||||
| Lindbloom 2019 | M. | 36 (33–40) | 68 (64–72) | / | / | 2 (1–2) | 5 (5–6) | / | / | ||||||||||||
| F | 43 (38–47) | 76 (71–81) | / | / | 3 (2–3) | 7 (6–7) | / | / | |||||||||||||
| Merolla et al., 2017 | / | / | 17.9 | 69.6 | / | / | 8.4 | 0.9 | |||||||||||||
| Mollon et al., 2016 | Nn | 35.0 ± 13.8 | 71.0 ± 14.2 | / | / | 38.2 ± 15.7 | 84.1 ± 17.1 | / | / | 3.5 ± 2.2 | 10.1 ± 2.6 | / | / | / | / | / | / | ||||
| Y | 32.7 ± 12.8 | 66.0 ± 13.9 | / | / | 34.3 ± 15.0 | 78.1 ± 21.8 | / | / | 3 ± 2.2 | 9.4 ± 3.0 | / | / | / | / | / | / | |||||
| Mulieri et al., 2010 | / | / | 33 | 75 | / | / | 1.6 | 6.5 | / | / | / | / | 6.3 | 1.9 | / | / | |||||
| Naveed et al., 2011 | / | / | 17 | 59 | / | / | 19 (14–23) | 65 (48–82) | / | / | / | / | 44 (40–51) | 23 (18–28) | / | / | |||||
| Sadoghi et al., 2011 | / | / | 31.3 (14–63) | 60 (19–88) | / | / | / | / | / | / | 21.5 (12–41) | 40.8 (32–50) | / | / | |||||||
| Sayana et al., 2008 | / | / | 14.8 | 60.9 | |||||||||||||||||
| Simovitch et al., 2007 | / | / | 38 | 78 | / | / | / | / | / | / | / | / | |||||||||
| Sirveaux et al., 2004 | / | / | 22.60 (4–50) | 65.5 (34–85) | / | / | / | / | / | / | / | / | 2.7 (0–10) | 13.4 (5–15) | |||||||
| Streit et al., 2015 | 71.0 | 75.1 | 0.7 | 0.3 | |||||||||||||||||
| Wall et al., 2007 | / | / | 22.8 | 59.7 | / | / | / | / | / | / | / | / | 3.5 | 12.3 | |||||||
| Author and Year | Self-Assessed Satisfaction | Complications | Revisions | ||||
|---|---|---|---|---|---|---|---|
| L | M | L | M | L | M | ||
| Beltrame et al., 2019 | None | None | |||||
| Berglund et al., 2018 | |||||||
| Boileau et al., 2009 | 37 benefited from the operation 34 very satisfied/satisfied 5 disappointed/dissatisfied | Bony spur (23) | / | 1 | |||
| Boutsiadis et al., 2018 | |||||||
| De Biase et al., 2012 | / | / | Dislocation Infection | / | |||
| Edwards et al., 2012 | T | / | / | Dislocation (1) | / | 1 | |
| Nt | / | / | / | ||||
| Erșen et al., 2019 | |||||||
| Favard et al., 2011 | / | Infection (27) Loosening (27) Dislocation (19) Haematoma (14) Neurologic (6) | / | 13 +… | |||
| Greiner et al., 2015 | / | Acromial fracture (2) | |||||
| Jobin et al., 2012 | / | / | Infection (1) Baseplate-glenoid fixation failure (1) | / | 2 (4%) | ||
| Kalouche et al., 2009 | Disassembly (3) Dislocation (1) | Infection (5) Fracture (2) | 7 | 4 | |||
| Katz et al., 2015 | 91% better or much better 4% same 5% worse | / | Fracture (5), Nerve palsy (4), Humeral bearing failure (8), Infection (3), glenoid loosening (4) | / | 12 | / | |
| Lee et al., 2021 | Infection (1) | Acromial fracture (2), Dislocation (1) | 0 | 0 | |||
| Lindbloom 2019 | Dissociation at Morse taper, Recurrent instability | 2 | |||||
| Merolla et al., 2017 | Dislocation (2) | ||||||
| Mollon et al., 2016 | Nn | / | Fracture (8), Infection (4), Glenoid loosening (2) | / | / | ||
| Y | / | Glenoid loosening (1), Fracture (3) | / | / | |||
| Mulieri et al., 2010 | 65% excellent 20% good 10% satisfactory 5% unsatisfactory | / | Fracture (4) Infection (1) Dislocation (1) | 3 | / | ||
| Naveed et al., 2011 | / | 16 patients no pain 15 mild pain 5 moderate pain 0 severe pain | Acromial erosion Fracture (2) Infection (2) | / | 4 | ||
| Sadoghi et al., 2011 | / | / | Nerve lesion (1) Loosening of humeral stem (3) Luxation of glenoid (4) | / | 7 | ||
| Sayana et al., 2008 | / | Glenoid loosening (1) | / | 1 | |||
| Simovitch et al., 2007 | Subjective Shoulder value increased by 39% on average | ||||||
| Sirveaux et al., 2004 | / | / | Glenoid loosening (2) Infection (1) | / | 3 | ||
| Streit et al., 2015 | |||||||
| Wall et al., 2007 | / | 59.7% very satisfied; 33.3% satisfied; 5.9% uncertain; 1.1% disappointed | / | Dislcation (15) Infection (8) Glenoid fractures, humeral fractures, musculocutaneous nerve palsy, radial nerve palsy, glenoid sphere loosening and glenoid base loosening (<5) | |||
| Author and Year | Medialized COR | Lateralized COR | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scapular Notching | Grades of Notching (% or N) | Scapular Notching | Grades of Notching (% or N) | |||||||||
| N | % | Grade I | Grade II | Grade III | Grade IV | N | % | Grade I | Grade II | Grade III | Grade IV | |
| Beltrame et al., 2019 | 3 | 24 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Berglund et al., 2018 | / | / | / | / | / | / | ||||||
| Boileau 2009 | 31 | 74 | 8 | 13 | 5 | 5 | / | / | / | / | / | / |
| Boutsiadis et al., 2018 | ||||||||||||
| De Biase et al., 2012 | 0 | 0 | 0 | 0 | 0 | 0 | / | / | / | / | / | / |
| Edwards et al., 2012 | 15 | 86 | 25% | 40% | 10% | / | / | / | / | / | / | |
| Edwards et al., 2012 | 19 | 75 | 36%% | 45%% | 5%% | / | / | / | / | / | / | |
| Erșen et al., 2019 | / | / | / | / | / | / | ||||||
| Favard et al., 2011 | 50% | / | / | / | / | / | / | |||||
| Greiner et al., 2015 | 0 | 0 | ||||||||||
| Jobin et al., 2012 | 25 | 68 | / | / | / | / | / | / | ||||
| Kalouche et al., 2009 | 32 | 68 | 11 | 11 | 9 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| Katz et al., 2015 | / | / | / | / | / | / | 41 | 29 | 20 | 18 | 3 | 0 |
| Lee et al., 2021 | 18 | 41.8 | 13 | 5 | 0 | 11 | 15.5 | 11 | 0 | 0 | ||
| Lindbloom et al., 2019 | / | / | / | / | / | / | ||||||
| Merolla et al., 2017 | 14 | 39.0 | 11 | 1 | 0 | 0 | / | / | / | / | / | / |
| Mollon et al., 2016 | / | / | / | / | / | / | 48 | 10.1 | 2.1 | |||
| Mulieri et al., 2010 | / | / | / | / | / | / | 7 | 12 | 11.50% | 1.90% | 0 | 0 |
| Naveed et al., 2011 | 31 | 62 | 5 | 7 | 11 | 8 | / | / | / | / | / | / |
| Sadoghi et al., 2011 | 12 | 32 | 23% | 3% | 6% | 0 | / | / | / | / | / | / |
| Sayana et al., 2009 | 19 | 100 | 5 | 8 | 2 | 4 | / | / | / | / | / | / |
| Simovitch et al., 2007 | / | / | / | / | / | / | ||||||
| Sirveaux et al., 2004 | 49 | 64 | 26 | 10 | 7 | 6 | / | / | / | / | / | / |
| Streit et al., 2015 | ||||||||||||
| Wall et al., 2007 | / | / | / | / | / | / | ||||||
| Author and Year | ROM | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Forward Flexion (°) | Abduction (°) | External Rotation Arm-at-Side (°) | External Rotation in Abduction (°) | Internal Rotation | |||||||||||||||||
| L | M | L | M | L | M | L | M | L | M | ||||||||||||
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post | ||
| Beltrame et al., 2019 | 153 (120–180) | 158 (120–180) | 142 (100–170) | 144 (100–180) | 42 (30–60) | 37 (20–40) | 4.6 | 4.8 | |||||||||||||
| Berglund et al., 2018 | −21 | 28 | |||||||||||||||||||
| Boileau et al., 2009 | / | / | 82 (20–180) | 123 (40–170) | / | / | / | / | 5 (−40–+70) | 7 (−30–+60) | / | / | / | / | |||||||
| Boutsiadis et al., 2018 | II = 53 ± 22 (30–90) | 149 ± 8 (90–175) | 63 ± 21 (10–100) | 148 ± 7 (100–170) | 134 ± 9 (80–175) | 134 ± 8.5 (90–170) | –8 ± 21 (−30–20) | 31 ± 13 (15–60) | 14 ± 20 (–30–50) | 14 ± 13 (−10–35) | BUT (Lat. Thigh-Sacroiliac) | L3 (BUT-T12) | SI (BUT-T12) | L3 (BUT-T12) | |||||||
| Sacroiliac (BUT-T12) | L3 (BUT-T12) | ||||||||||||||||||||
| De Biase et al., 2012 | / | / | 66 ± 9 | 148 ± 8 | / | / | 60 ± 9 | 115 ± 14 | / | / | 5 ± 5 | 16 ± 5 | / | / | / | / | |||||
| Edwards et al., 2012 | T | / | / | 36.0 ± 45.6 | 148.0 ± 19.4 | / | / | 32.3. ± 37.4 | 141.8 ± 27.3 | / | / | 0.3 ± 1.3 | 7.4 ± 1.8 | / | / | / | / | ||||
| Nt | / | / | 51.6 ± 49.1 | 156.6 ± 21.2 | / | / | 49.8 ± 49.0 | 155.9 ± 21.0 | / | / | 0.7 ± 1.8 | 8.3 ± 2.6 | / | / | / | / | 40.9 | 77.3 | |||
| Erșen et al., 2019 | 77.5 (50–130) | 111.6 (80–170) | / | / | 84.5 (30–160) | 108.8 (90–170) | / | / | 21.3 (0–50) | 23.8 (0–60) | |||||||||||
| Favard et al., 2011 | / | / | 69.3 ± 34 | 128.6 ± 32.6 | / | / | / | / | 4.9 ± 17.6 | 10.6 ± 18.8 | / | / | 23.5 ± 23.3 | 42.1 ± 30.2 | / | / | |||||
| Greiner et al., 2015 | / | / | 2.3 ± 2.5 | 6.8 ± 2.2 | / | / | 2.1 ± 2.1 | 6.7 ± 2.1 | / | / | 22 ± 23 | Δ 18 ± 26 | / | / | 26 ± 31 | Δ 33 ± 42 | / | / | 3.3 ± 2.8 | 5.3 ± 2.6 | |
| Jobin et al., 2012 | / | / | 38 ± 26 | 144 ± 19 | / | / | / | / | 11 ± 14 | 23 ± 16 | / | / | 18 ± 22 | 44 ± 30 | / | / | L4 ± 3 | L3 ± 3 | |||
| Kalouche et al., 2009 | 61.5 (10.120) | 134.7 (95–180) | 70.3 (20–140) | 140.8 (95–180) | / | 14.8 (−20–70) | 28.6 (0–60) | 16.0 (−20–40) | 24.8 (−10–60) | 18.7 (−20–60) | 51.5 (10–95) | 25.6 (0–60) | 48–0 (0–90) | 4.5 (0–10) | 6.4 (2–10) | 5.2 (0–10) | 6.0 (2–10) | ||||
| Katz et al., 2015 | 73 (10–160) | 132 (40–180) | / | / | 61 (20–150) | 108 (40–170) | / | / | / | / | 30 (0–90) | 54 (0–100) | / | / | / | / | |||||
| Lee et al., 2021 | 132 ± 16 | 130 ± 16 | 125 ± 16 | 127 ± 14 | 48 ± 12 | 48 ± 14 | L2 ± 2 | L2 ± 4 | |||||||||||||
| Lindbloom 2019 | M. | 81 (72–90) | 151 (142–159) | 75 (68–82) | 136 (126–146) | 32 (24–39) | 55 (46–64) | 3 (3–4) | 4 (4–5) | ||||||||||||
| F | 70 (63–78) | 136 (128–144) | 66 (59–73) | 121 (113–130) | 26 (19–33) | 46 (38–54) | 3 (2–3) | 5 (4–5) | |||||||||||||
| Merolla et al., 2017 | / | / | 65 | 142 | / | / | 15 | 30 | / | / | 2.4 | 4.7 | |||||||||
| Mollon et al., 2016 | Nn | 89 ± 40 | 139 ± 26 | / | / | 72 ± 36 | 113 ± 27 | / | / | 16 ± 23 | 35 ± 17 | / | / | / | / | 3.3 ± 1.8 | 4.8 ± 1.6 | / | / | ||
| Y | 89 ± 41 | 130 ± 30 | / | / | 70 ± 36 | 103 ± 23 | / | / | 14 ± 21 | 35 ± 16 | / | / | 3.3 ± 1.8 | 5.3 ± 1.5 | / | / | |||||
| Mulieri et al., 2010 | 53 (0–148) | 134 (10–180) | / | / | 49 (0–140) | 125 (25–180) | / | / | 27 (−20–70) | 51 (−30–90) | / | / | / | / | S1 | L2 | / | / | |||
| Naveed et al., 2011 | / | / | 55 | 105 | / | / | 85 | / | / | / | / | / | / | Buttock (35%) T12 (25%) Sacroiliac joint (20%) Waist (10%) Limited (10%). | |||||||
| Sadoghi et al., 2011 | / | / | 34 | 125 | / | / | 36 | 117 | / | / | 14.1 | 13.9 | / | / | / | / | |||||
| Sayana et al., 2008 | / | / | / | / | / | / | / | / | / | / | |||||||||||
| Simovitch et al., 2007 | / | / | 65 | 115 | / | / | 63 | 111 | / | / | 16 | 20.5 | / | / | / | / | |||||
| Sirveaux et al., 2004 | / | / | 73 | 138 | / | / | / | / | 3.50 | 11.20 | / | / | 17 | 40 | / | / | 4 | 4.8 | |||
| Streit et al., 2015 | 115.6 | 143.9 | 35.0 | 28.3 | −2.2 | −1.8 | |||||||||||||||
| Wall et al., 2007 | / | / | 76 | 142 | / | / | / | / | 5 | 7 | / | / | 29 | 43 | / | / | L5 | L3 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berton, A.; Gulotta, L.V.; Longo, U.G.; De Salvatore, S.; Piergentili, I.; Bandini, B.; Lalli, A.; Mathew, J.; Warren, R.F.; Denaro, V. Medialized versus Lateralized Center of Rotation in Reverse Total Shoulder Arthroplasty: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 5868. https://doi.org/10.3390/jcm10245868
Berton A, Gulotta LV, Longo UG, De Salvatore S, Piergentili I, Bandini B, Lalli A, Mathew J, Warren RF, Denaro V. Medialized versus Lateralized Center of Rotation in Reverse Total Shoulder Arthroplasty: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(24):5868. https://doi.org/10.3390/jcm10245868
Chicago/Turabian StyleBerton, Alessandra, Lawrence V. Gulotta, Umile Giuseppe Longo, Sergio De Salvatore, Ilaria Piergentili, Benedetta Bandini, Alberto Lalli, Joshua Mathew, Russell F. Warren, and Vincenzo Denaro. 2021. "Medialized versus Lateralized Center of Rotation in Reverse Total Shoulder Arthroplasty: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 24: 5868. https://doi.org/10.3390/jcm10245868