
Differential Effects of Comorbid Psychiatric Disorders on Treatment Outcome in Posttraumatic Stress Disorder from Childhood Trauma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Randomization and Masking
2.3. Procedures
2.4. Outcomes
2.5. Treatment
2.6. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Primary Outcome
3.3. Secondary Outcomes
3.4. Sensitivity Analysis
4. Discussion
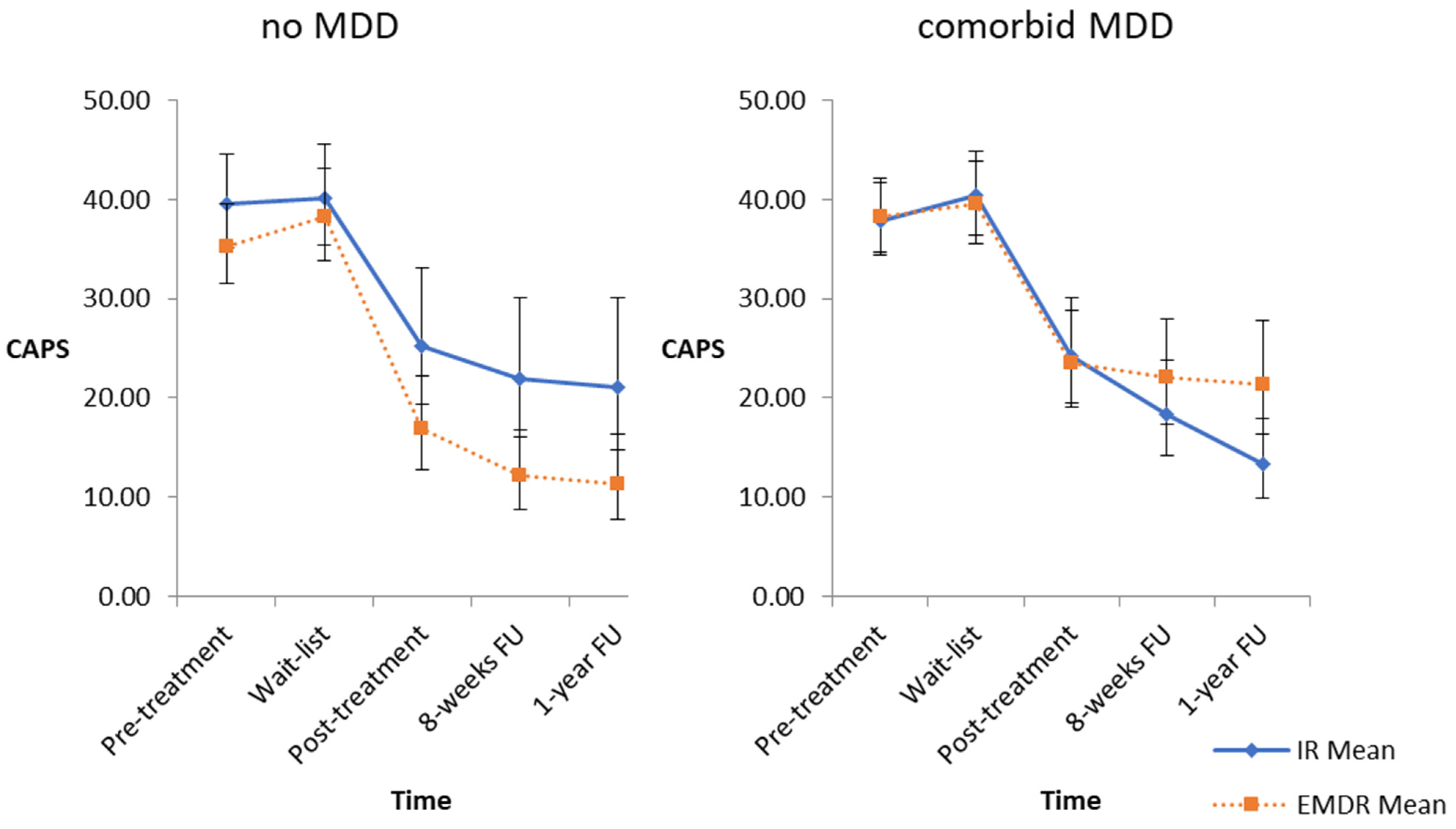
4.1. Effects of Major Depressive Disorder
4.2. Effect of AD
4.3. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bleich, A.; Koslowsky, M.; Dolev, A.; Lerer, B. Post-traumatic stress disorder and depression. An analysis of comorbidity. Br. J. Psychiatry 1997, 170, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Ikin, J.F.; Creamer, M.C.; Sim, M.R.; McKenzie, D.P. Comorbidity of PTSD and depression in Korean War veterans: Prevalence, predictors, and impairment. J. Affect. Disord. 2010, 125, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Adams, Z.W.; Danielson, C.K.; Sumner, J.A.; McCauley, J.L.; Cohen, J.R.; Ruggiero, K.J. Comorbidity of PTSD, Major Depression, and Substance Use Disorder Among Adolescent Victims of the Spring 2011 Tornadoes in Alabama and Joplin, Missouri. Psychiatry 2015, 78, 170–185. [Google Scholar] [PubMed]
- Salcioglu, E.; Basoglu, M.; Livanou, M. Post-traumatic stress disorder and comorbid depression among survivors of the 1999 earthquake in Turkey. Disasters 2007, 31, 115–129. [Google Scholar] [CrossRef]
- Tural, U.; Onder, E.; Aker, T. Effect of depression on recovery from PTSD. Community Ment. Health J. 2012, 48, 161–166. [Google Scholar] [CrossRef]
- Momartin, S.; Silove, D.; Manicavasagar, V.; Steel, Z. Comorbidity of PTSD and depression: Associations with trauma exposure, symptom severity and functional impairment in Bosnian refugees resettled in Australia. J. Affect. Disord. 2004, 80, 231–238. [Google Scholar] [CrossRef]
- Kilpatrick, D.G.; Ruggiero, K.J.; Acierno, R.; Saunders, B.E.; Resnick, H.S.; Best, C.L. Violence and risk of PTSD, major depression, substance abuse/dependence, and comorbidity: Results from the National Survey of Adolescents. J. Consult. Clin. Psychol. 2003, 71, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.L.; Vogt, D.S.; Resick, P.A. Cognitive and affective predictors of treatment outcome in Cognitive Processing Therapy and Prolonged Exposure for posttraumatic stress disorder. Behav. Res. Ther. 2009, 47, 737–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cloitre, M.; Garvert, D.W.; Weiss, B.J. Depression as a moderator of STAIR Narrative Therapy for women with post-traumatic stress disorder related to childhood abuse. Eur. J. Psychotraumatol. 2017, 8, 1377028. [Google Scholar] [CrossRef] [PubMed]
- Spinhoven, P.; Penninx, B.W.; van Hemert, A.M.; de Rooij, M.; Elzinga, B.M. Comorbidity of PTSD in anxiety and depressive disorders: Prevalence and shared risk factors. Child Abuse Negl. 2014, 38, 1320–1330. [Google Scholar] [CrossRef]
- Boterhoven de Haan, K.L.; Lee, C.W.; Fassbinder, E.; van Es, S.M.; Menninga, S.; Meewisse, M.L.; Rijkeboer, M.; Kousemaker, M.; Arntz, A. Imagery rescripting and eye movement desensitisation and reprocessing as treatment for adults with post-traumatic stress disorder from childhood trauma: Randomised clinical trial. Br. J. Psychiatry 2020, 217, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Galatzer-Levy, I.R.; Nickerson, A.; Litz, B.T.; Marmar, C.R. Patterns of lifetime PTSD comorbidity: A latent class analysis. Depress. Anxiety 2013, 30, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.; Mills, K.; Slade, T.; McFarlane, A.C.; Bryant, R.A.; Creamer, M.; Silove, D.; Teesson, M. Remission from post-traumatic stress disorder in the general population. Psychol. Med. 2012, 42, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Pérez Benítez, C.I.; Zlotnick, C.; Dyck, I.; Stout, R.; Angert, E.; Weisberg, R.; Keller, M. Predictors of the long-term course of comorbid PTSD: A naturalistic prospective study. Int. J. Psychiatry Clin. Pract. 2013, 17, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Ajdacic-Gross, V.; Rodgers, S.; Kleim, B.; Seifritz, E.; Vetter, S.; Egger, S.T.; Rössler, W.; Castelao, E.; Preisig, M.; et al. Predictors of remission from PTSD symptoms after sexual and non-sexual trauma in the community: A mediated survival-analytic approach. Psychiatry Res. 2018, 260, 262–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S.; Fedoroff, I.C.; Koch, W.J.; Thordarson, D.S.; Fecteau, G.; Nicki, R.M. Posttraumatic stress disorder arising after road traffic collisions: Patterns of response to cognitive-behavior therapy. J. Consult. Clin. Psychol. 2001, 69, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Haagen, J.F.; Ter Heide, F.J.; Mooren, T.M.; Knipscheer, J.W.; Kleber, R.J. Predicting post-traumatic stress disorder treatment response in refugees: Multilevel analysis. Br. J. Clin. Psychol. 2017, 56, 69–83. [Google Scholar] [CrossRef]
- Markowitz, J.C.; Petkova, E.; Neria, Y.; Van Meter, P.E.; Zhao, Y.; Hembree, E.; Lovell, K.; Biyanova, T.; Marshall, R.D. Is Exposure Necessary? A Randomized Clinical Trial of Interpersonal Psychotherapy for PTSD. Am. J. Psychiatry 2015, 172, 430–440. [Google Scholar] [CrossRef] [Green Version]
- Van Minnen, A.; Arntz, A.; Keijsers, G.P. Prolonged exposure in patients with chronic PTSD: Predictors of treatment outcome and dropout. Behav. Res. Ther. 2002, 40, 439–457. [Google Scholar] [CrossRef]
- Karatzias, A.; Power, K.; McGoldrick, T.; Brown, K.; Buchanan, R.; Sharp, D.; Swanson, V. Predicting treatment outcome on three measures for post-traumatic stress disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2007, 257, 40–46. [Google Scholar] [CrossRef]
- Dewar, M.; Paradis, A.; Fortin, C.A. Identifying trajectories and predictors of response to psychotherapy for post-traumatic stress disorder in adults: A systematic review of literature. Can. J. Psychiatry 2020, 65, 71–86. [Google Scholar] [CrossRef]
- Barawi, K.S.; Lewis, C.; Simon, N.; Bisson, J.I. A systematic review of factors associated with outcome of psychological treatments for post-traumatic stress disorder. Eur. J. Psychotraumatol. 2020, 11, 1774240. [Google Scholar] [CrossRef]
- Cloitre, M.; Petkova, E.; Su, Z.; Weiss, B. Patient characteristics as a moderator of post-traumatic stress disorder treatment outcome: Combining symptom burden and strengths. BJPsych Open 2016, 2, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Schnyder, U.; Ehlers, A.; Elbert, T.; Foa, E.B.; Gersons, B.P.; Resick, P.A.; Shapiro, F.; Cloitre, M. Psychotherapies for PTSD: What do they have in common? Eur. J. Psychotraumatol. 2015, 6, 28186. [Google Scholar] [CrossRef] [PubMed]
- Arntz, A.; Weertman, A. Treatment of childhood memories: Theory and practice. Behav. Res. Ther 1999, 37, 715–740. [Google Scholar] [CrossRef]
- Boterhoven de Haan, K.L.; Lee, C.W.; Fassbinder, E.; Voncken, M.J.; Meewisse, M.; Van Es, S.M.; Menninga, S.; Kousemaker, M.; Arntz, A. Imagery rescripting and eye movement desensitisation and reprocessing for treatment of adults with childhood trauma-related post-traumatic stress disorder: IREM study design. BMC Psychiatry 2017, 17, 165. [Google Scholar] [CrossRef]
- Shapiro, F.; Forrest, M. EMDR: Eye Movement Desensitization and Reprocessing; Guilford: New York, NY, USA, 2001. [Google Scholar]
- Arntz, A. Imagery Rescripting as a Therapeutic Technique: Review of Clinical Trials, Basic Studies, and Research Agenda. J. Exp. Psychopathol. 2012, 3, 189–208. [Google Scholar] [CrossRef]
- Lee, C.W.; Cuijpers, P. A meta-analysis of the contribution of eye movements in processing emotional memories. J. Behav. Ther. Exp. Psychiatry 2013, 44, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Leer, A.; Engelhard, I.M.; van den Hout, M.A. How eye movements in EMDR work: Changes in memory vividness and emotionality. J. Behav. Ther. Exp. Psychiatry 2014, 45, 396–401. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B. Structured Clinical Interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition; SCID-I/P: New York, NY, USA, 2002. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33. [Google Scholar]
- First, M.B.; Williams, J.B.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5—Research Version (SCID-5 for DSM-5, Research Version, SCID-5-RV); American Psychiatric Association: Arlington, VA, USA, 2015; pp. 1–94. [Google Scholar]
- Weathers, F.; Blake, D.; Schnurr, P.; Kaloupek, D.; Marx, B.; Keane, T. The Life Events Checklist for DSM-5 (LEC-5). Instrument Available from the National Center for PTSD. 2013. Available online: www.ptsd.va.gov (accessed on 10 December 2013).
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Weiss, D.; Marmar, C. The Impact of Event Scale—Revised; Wilson, J., Keane, T., Eds.; Assessing Psychological Trauma and PTSD: A Handbook for Practitioners; Guildford Press: New York, NY, USA, 1997. [Google Scholar]
- Brewin, C.R.; Wheatley, J.; Patel, T.; Fearon, P.; Hackmann, A.; Wells, A.; Fisher, P.; Myers, S. Imagery rescripting as a brief stand-alone treatment for depressed patients with intrusive memories. Behav. Res. Ther. 2009, 47, 569–576. [Google Scholar] [CrossRef]
- Dominguez, S.; Drummond, P.; Gouldthorp, B.; Janson, D.; Lee, C.W. A randomized controlled trial examining the impact of individual trauma-focused therapy for individuals receiving group treatment for depression. Psychol. Psychother. 2021, 94, 81–100. [Google Scholar] [CrossRef] [PubMed]
- Ostacoli, L.; Carletto, S.; Cavallo, M.; Baldomir-Gago, P.; Di Lorenzo, G.; Fernandez, I.; Hase, M.; Justo-Alonso, A.; Lehnung, M.; Migliaretti, G.; et al. Comparison of Eye Movement Desensitization Reprocessing and Cognitive Behavioral Therapy as Adjunctive Treatments for Recurrent Depression: The European Depression EMDR Network (EDEN) Randomized Controlled Trial. Front. Psychol. 2018, 9, 74. [Google Scholar] [CrossRef]
- McCullough, J.P., Jr. Treatment for chronic depression using Cognitive Behavioral Analysis System of Psychotherapy (CBASP). J. Clin. Psychol. 2003, 59, 833–846. [Google Scholar] [CrossRef] [PubMed]
- Sondermann, S.; Stahl, J.; Grave, U.; Outzen, J.; Moritz, S.; Klein, J.P. Preoperational Thinking as a Measure of Social Cognition Is Associated With Long-Term Course of Depressive Symptoms. A Longitudinal Study Involving Patients with Depression and Healthy Controls. Front. Psychiatry 2020, 11, 652. [Google Scholar] [CrossRef] [PubMed]
- Hase, M.; Plagge, J.; Hase, A.; Braas, R.; Ostacoli, L.; Hofmann, A.; Huchzermeier, C. Eye Movement Desensitization and Reprocessing Versus Treatment as Usual in the Treatment of Depression: A Randomized-Controlled Trial. Front. Psychol. 2018, 9, 1384. [Google Scholar] [CrossRef] [Green Version]
- Kunze, A.E.; Lancee, J.; Morina, N.; Kindt, M.; Arntz, A. Mediators of change in imagery rescripting and imaginal exposure for nightmares: Evidence from a randomized wait-list controlled trial. Behav. Ther. 2019, 50, 978–993. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Press: Washington, DC, USA, 2013. [Google Scholar]
- Carletto, S.; Malandrone, F.; Berchialla, P.; Oliva, F.; Colombi, N.; Hase, M.; Hofmann, A.; Ostacoli, L. Eye movement desensitization and reprocessing for depression: A systematic review and meta-analysis. Eur. J. Psychotraumatol. 2021, 12, 1894736. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Treatment Condition, No. (%) of Patients | |||
|---|---|---|---|
| Total | IR | EMDR | |
| Comorbid disorders | n = 155 (%) | n = 74 (%) | n = 81 (%) |
| Mood disorder | 112 (72.3) | 55 (74.3) | 57 (70.4) |
| MDD | 97 (62.6) | 46 (62.2) | 51 (63.0) |
| Dysthymia | 17 (11) | 7 (9.5) | 10 (12.3) |
| Bipolar disorder type 2 1 | 6 (3.9) | 4 (5.4) | 2 (2.5) |
| Anxiety disorder | 87 (56.1) | 38 (51.4) | 49 (60.5) |
| Panic disorder | 19 (12.3) | 9 (12.2) | 10 (12.3) |
| Panic with agoraphobia | 26 (16.8) | 11 (14.9) | 15 (18.5) |
| Agoraphobia | 5 (3.2) | 1 (1.4) | 4 (4.9) |
| Social phobia | 37 (23.9) | 17 (23.0) | 20 (24.7) |
| OCD | 20 (12.9) | 9 (12.2) | 11 (13.6) |
| GAD | 28 (18.1) | 12 (16.2) | 16 (19.8) |
| Specific phobia | 12 (7.7) 2 | 5 (6.8) | 7 (8.6) |
| Eating disorder | 21 (13.5) | 8 (10.8) | 13 (16.0) |
| Substance abuse | 17 (11.0) | 7 (9.5) | 10 (12.3) |
| Other diagnosis | 39 (25.2) | 16 (21.6) | 23 (28.4) |
| Timepoint | MDD No | MDD Yes | Time by MDD | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Estimated Means (95% CI) | d a | N | Estimated Means (95% CI) | d a | t b | df b | p b | |||||||
| Wait-list | 32 | 39.18 (35.49–43.24) | 0.12 | 56 | 39.98 (36.55–43.73) | 0.13 | 0.08 | 106 | 0.94 | ||||||
| Pre-treatment | 55 | 37.40 (34.11–41.00) | 92 | 38.04 (35.06–41.28) | |||||||||||
| Post-treatment | 49 | 20.65 (16.98–25.12) | 1.55 | 82 | 23.84 (20.45–27.78) | 1.22 | 1.22 | 106 | 0.23 | ||||||
| Eight-week follow-up | 47 | 16.31 (12.99–20.49) | 2.16 | 79 | 20.13 (16.85–24.04) | 1.66 | 1.54 | 106 | 0.13 | ||||||
| One-year follow-up | 38 | 15.41 (11.90–19.97) | 2.31 | 67 | 16.87 (13.82–20.61) | 2.12 | 0.49 | 106 | 0.63 | ||||||
| IR | EMDR | IR | EMDR | Time by Treatment by MDD | |||||||||||
| Estimated Means | Estimated Means | Estimated Means | Estimated Means | t b | df b | p b | |||||||||
| N | (95% CI) | d a | N | (95% CI) | d a | N | (95% CI) | d a | N | (95% CI) | d a | ||||
| Wait-list | 15 | 40.13 (35.35–45.56) | 0.04 | 17 | 38.24 (33.85–43.19) | 0.21 | 24 | 40.41 (36.39–44.89) | 0.17 | 32 | 39.55 (35.61–43.92) | 0.09 | −1.14 | 109 | 0.26 |
| Pre-treatment | 26 | 39.59 (35.15–44.60) | 29 | 35.32 (31.53–39.58) | 44 | 37.88 (34.39–41.72) | 48 | 38.20 (34.69–42.07) | |||||||
| Post-treatment | 26 | 25.26 (19.31–33.05) | 1.17 | 23 | 16.88 (12.80–22.27) | 1.93 | 38 | 24.19 (19.46–30.06) | 1.17 | 44 | 23.49 (19.11–28.88) | 1.27 | 1.22 | 109 | 0.22 |
| Eight-week follow-up | 23 | 21.93 (16.41–27.81) | 1.54 | 24 | 12.14 (8.79–16.75) | 2.79 | 36 | 18.38 (14.23–23.74) | 1.89 | 43 | 22.04 (17.37–27.94) | 1.43 | 2.62 | 109 | 0.01 |
| One-year follow-up | 19 | 21.09 (14.75–30.16) | 1.64 | 19 | 11.26 (7.79–16.27) | 2.98 | 30 | 13.33 (9.94-17.88) | 2.72 | 37 | 21.36 (16.41–27.81) | 1.51 | 3.26 | 109 | 0.001 |
| Timepoint | AD No | AD Yes | Time by AD | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Estimated Means (95% CI) | d a | N | Estimated Means (95% CI) | d a | t b | df b | pb | |||||||
| Wait-list | 32 | 39.89 (35.87–44.36) | 0.20 | 56 | 39.74 (35.74–44.18) | 0.03 | −1.51 | 144 | 0.14 | ||||||
| Pre-treatment | 63 | 36.73 (33.28–40.53) | 84 | 39.27 (35.60–43.32) | |||||||||||
| Post-treatment | 58 | 21.84 (18.13–26.30) | 1.36 | 73 | 23.28 (19.61–27.63) | 1.36 | −0.03 | 144 | 0.98 | ||||||
| Eight-week follow-up | 55 | 19.52 (15.82–24.09) | 1.65 | 71 | 18.37 (15.13–22.30) | 1.98 | −1.06 | 144 | 0.29 | ||||||
| One-year follow-up | 50 | 17.55 (13.84–22.26) | 1.93 | 55 | 17.00 (13.56–21.31) | 2.18 | −0.67 | 144 | 0.51 | ||||||
| IR | EMDR | IR | EMDR | Time by Treatment by AD | |||||||||||
| Estimated Means | Estimated Means | Estimated Means | Estimated Means | t b | df b | p b | |||||||||
| N | (95% CI) | d a | N | (95% CI) | d a | N | (95% CI) | d a | N | (95% CI) | d a | ||||
| Wait-list | 15 | 38.93 (34.20–44.32) | 0.13 | 17 | 40.88 (35.98–46.43) | 0.31 | 24 | 41.27 (36.59–46.55) | 0.07 | 32 | 38.26 (34.00–43.06) | 0.01 | −1.23 | 108 | 0.22 |
| Pre-treatment | 33 | 37.13 (33.09–41.67) | 30 | 36.33 (32.25–40.93) | 37 | 40.17 (35.83–45.04) | 47 | 38.39 (34.44–42.79) | |||||||
| Post-treatment | 34 | 24.50 (19.29–31.12) | 1.08 | 24 | 19.46 (14.84–25.52) | 1.63 | 30 | 24.51 (19.13–31.39) | 1.29 | 43 | 22.11 (17.83–27.43) | 1.44 | 0.75 | 108 | 0.46 |
| Eight-week follow-up | 29 | 20.95 (15.85–27.68) | 1.49 | 26 | 18.19 (13.44–24.62) | 1.80 | 30 | 18.28 (13.78–24.25) | 2.05 | 41 | 18.46 (14.44–23.60) | 1.91 | 0.75 | 108 | 0.46 |
| One-year follow-up | 28 | 15.83 (11.55–21.70) | 2.22 | 22 | 19.46 (13.80–27.44) | 1.63 | 21 | 17.12 (12.19–24.04) | 2.22 | 34 | 16.88 (12.73–22.38) | 2.14 | −0.68 | 108 | 0.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assmann, N.; Fassbinder, E.; Schaich, A.; Lee, C.W.; Boterhoven de Haan, K.; Rijkeboer, M.; Arntz, A. Differential Effects of Comorbid Psychiatric Disorders on Treatment Outcome in Posttraumatic Stress Disorder from Childhood Trauma. J. Clin. Med. 2021, 10, 3708. https://doi.org/10.3390/jcm10163708
Assmann N, Fassbinder E, Schaich A, Lee CW, Boterhoven de Haan K, Rijkeboer M, Arntz A. Differential Effects of Comorbid Psychiatric Disorders on Treatment Outcome in Posttraumatic Stress Disorder from Childhood Trauma. Journal of Clinical Medicine. 2021; 10(16):3708. https://doi.org/10.3390/jcm10163708
Chicago/Turabian StyleAssmann, Nele, Eva Fassbinder, Anja Schaich, Christopher W. Lee, Katrina Boterhoven de Haan, Marleen Rijkeboer, and Arnoud Arntz. 2021. "Differential Effects of Comorbid Psychiatric Disorders on Treatment Outcome in Posttraumatic Stress Disorder from Childhood Trauma" Journal of Clinical Medicine 10, no. 16: 3708. https://doi.org/10.3390/jcm10163708