
Adapting the Pore Size of Individual, 3D-Printed CPC Scaffolds in Maxillofacial Surgery

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Virtual Scaffold Planning
2.2. Scaffold Fabrication
2.3. Scaffold Characterization
2.4. Colonization
2.5. Statistics
3. Results
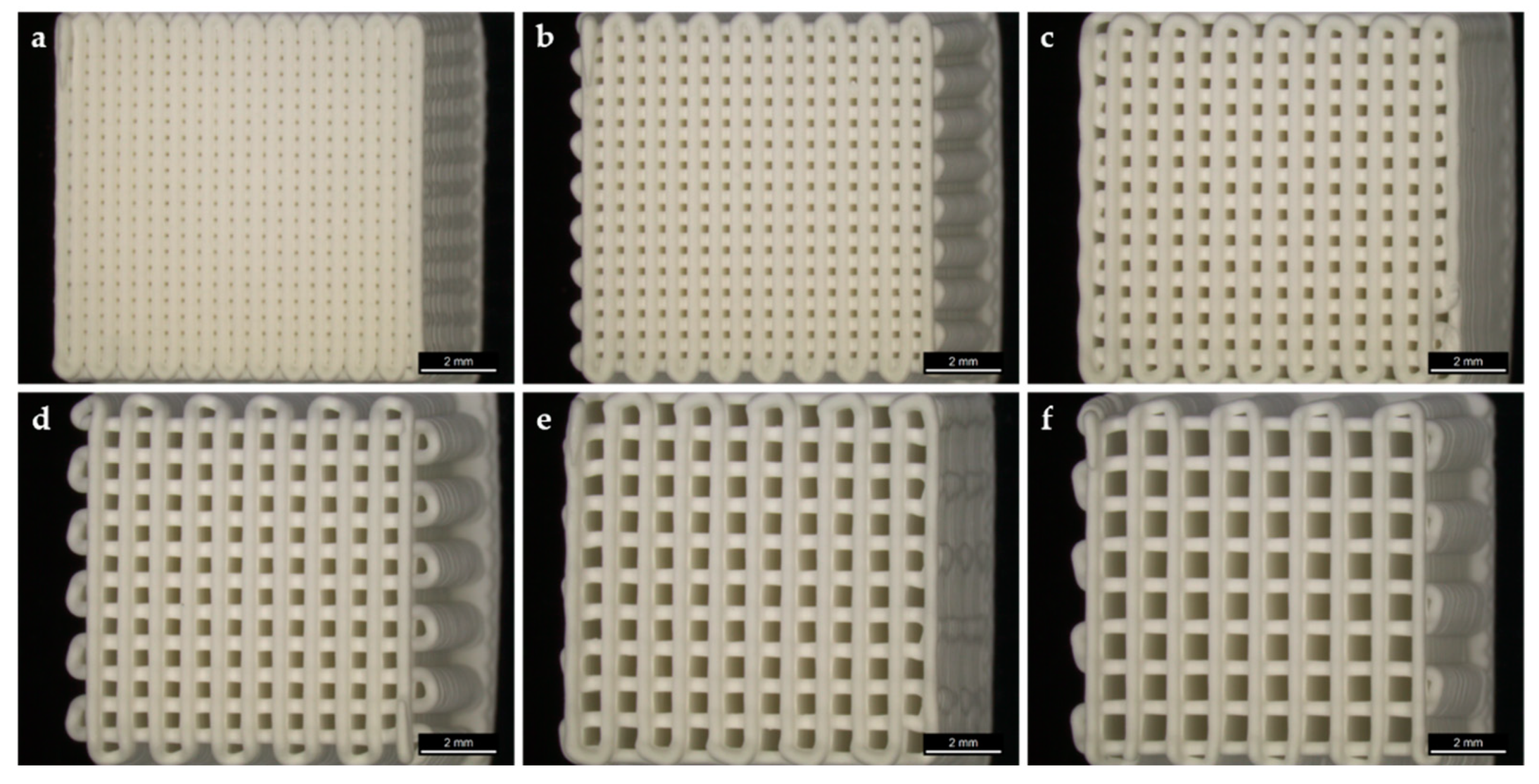
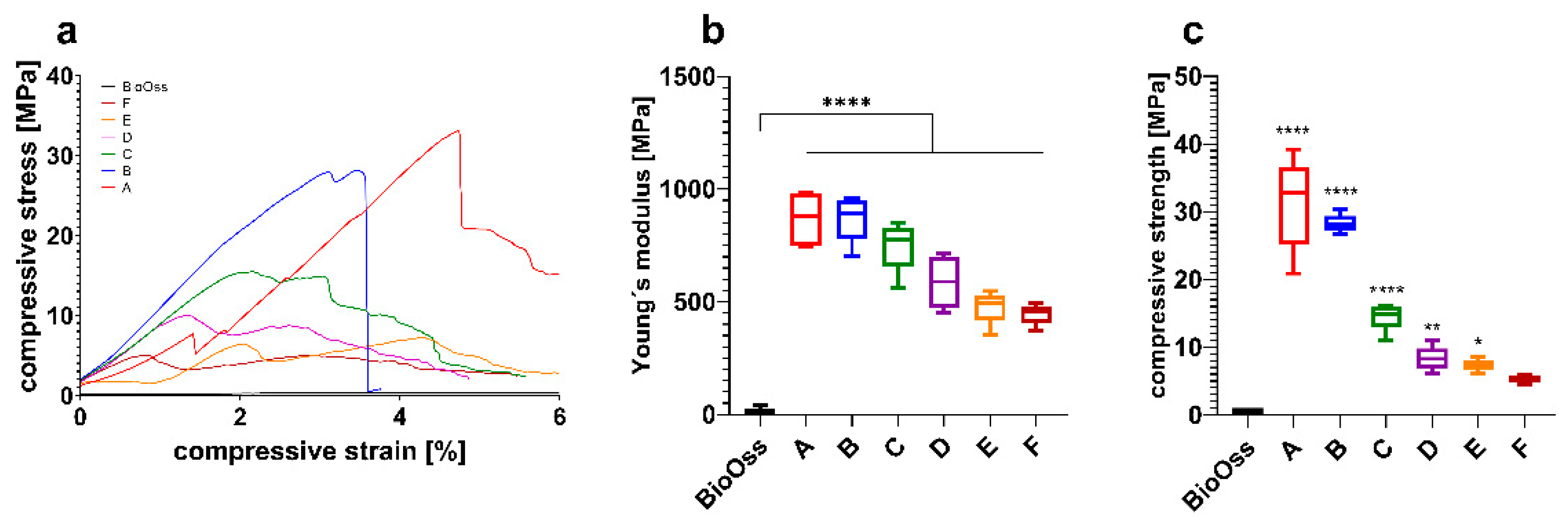
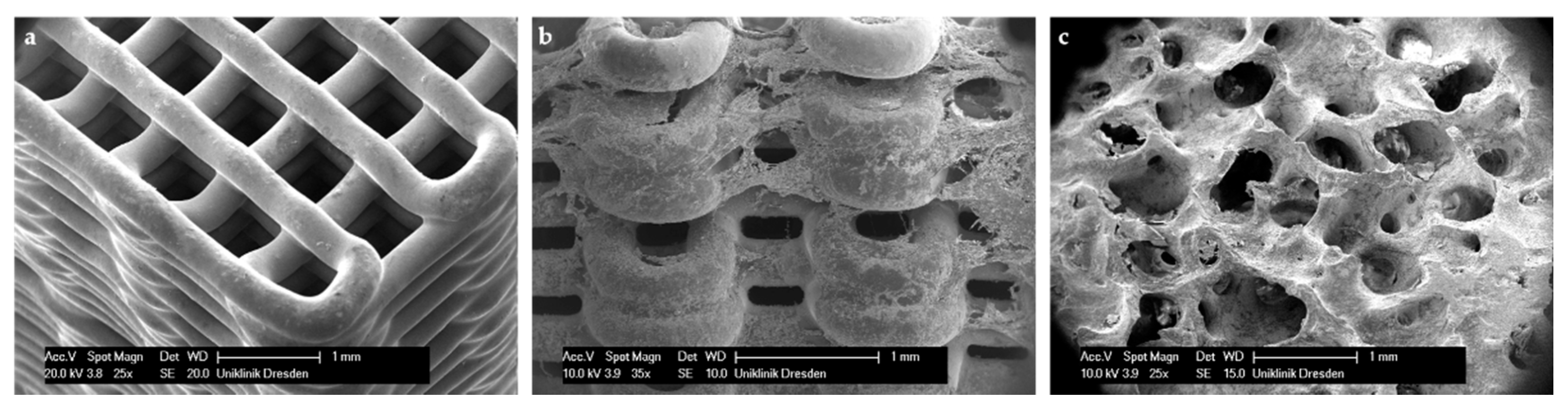
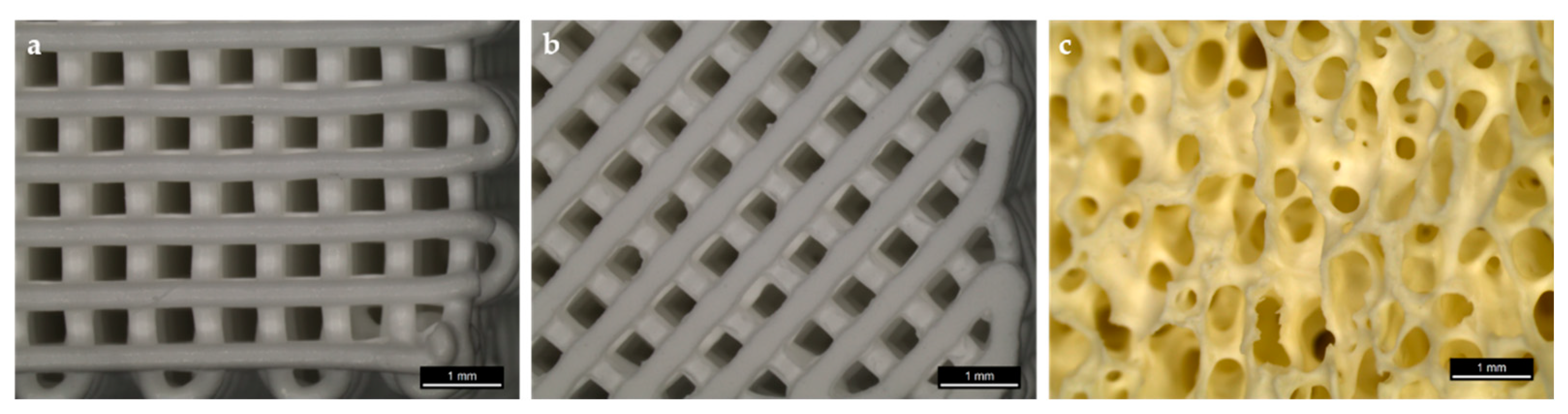
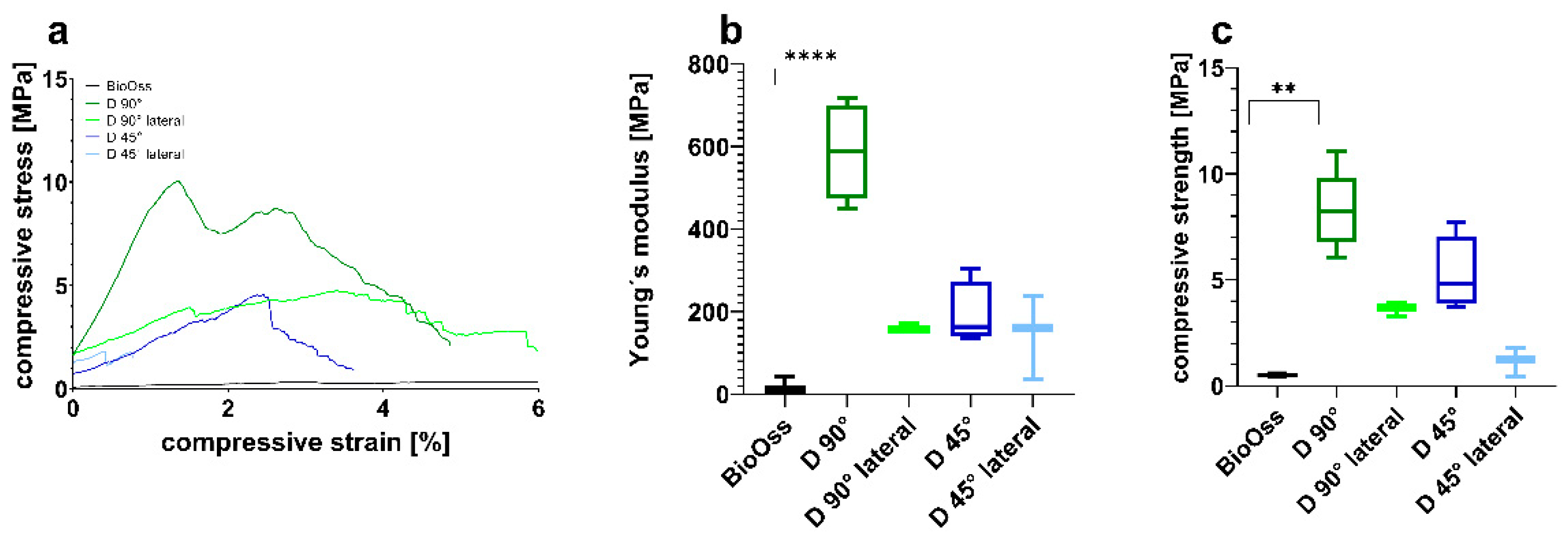
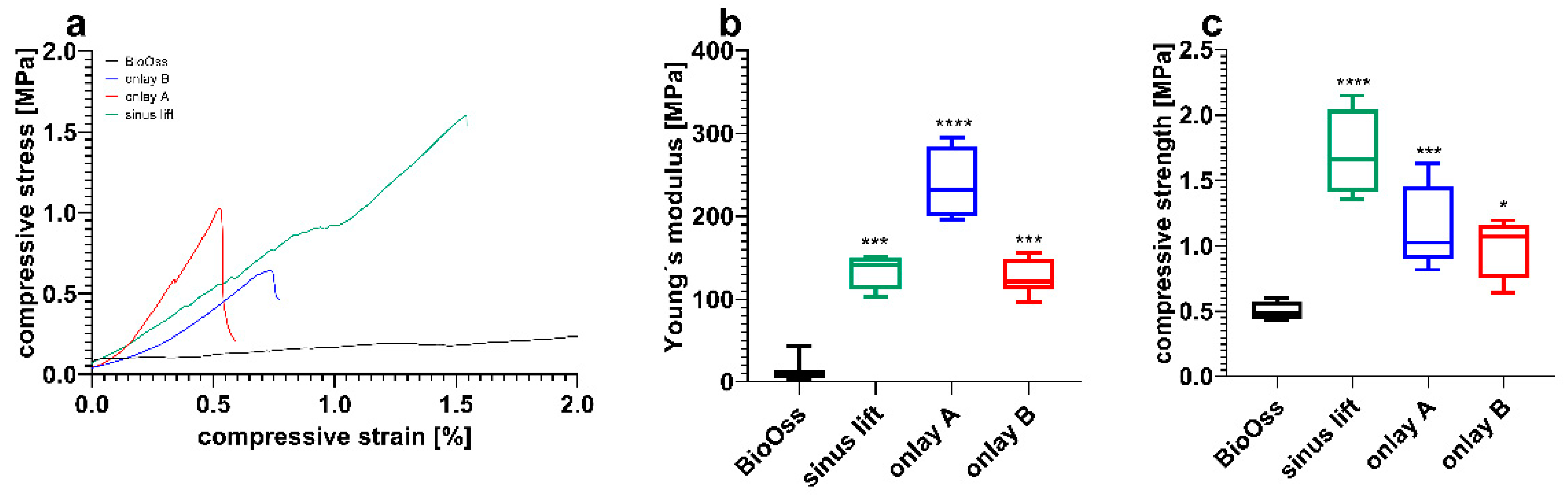
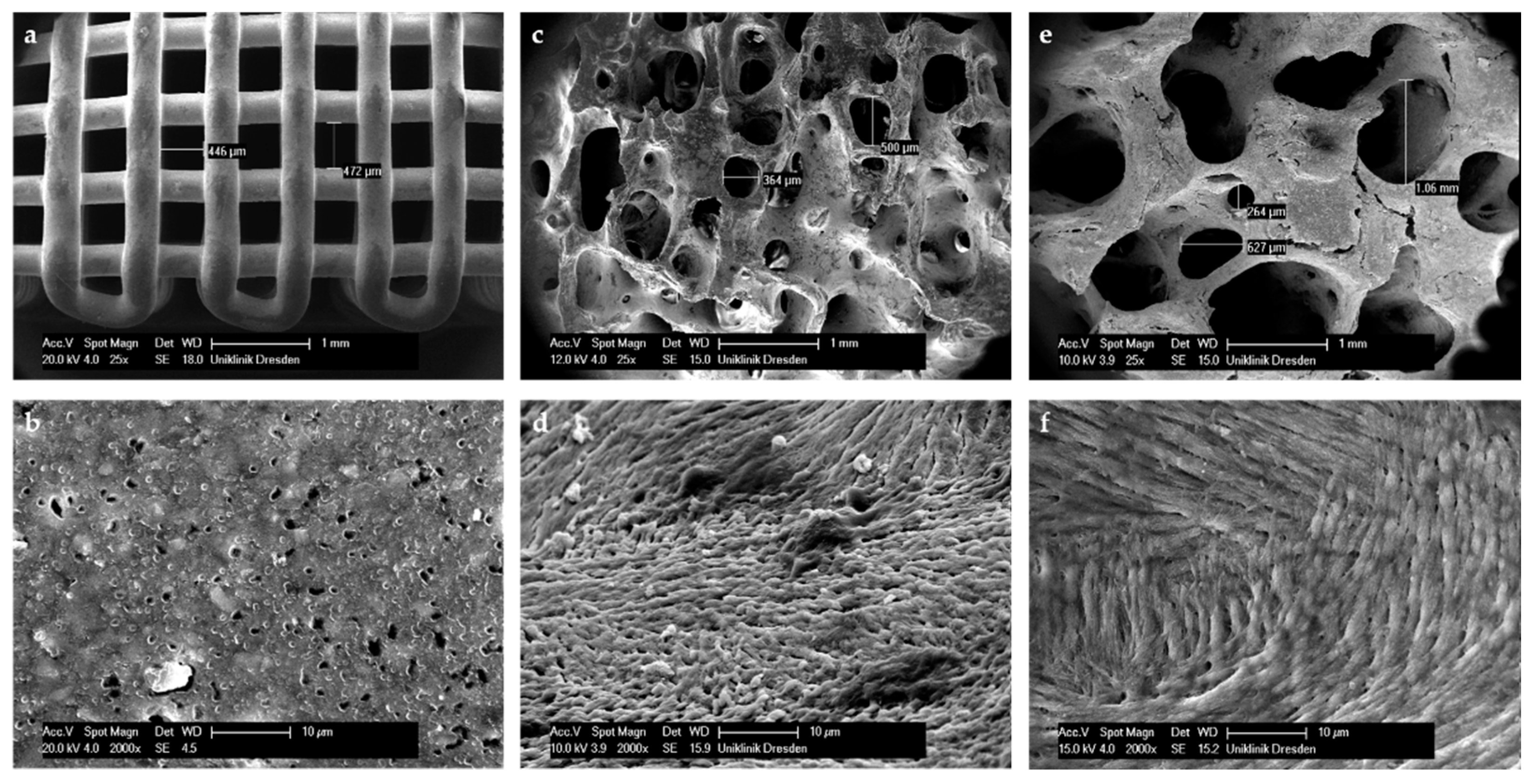
3.1. Scaffold Fabrication and Mechanical Testing
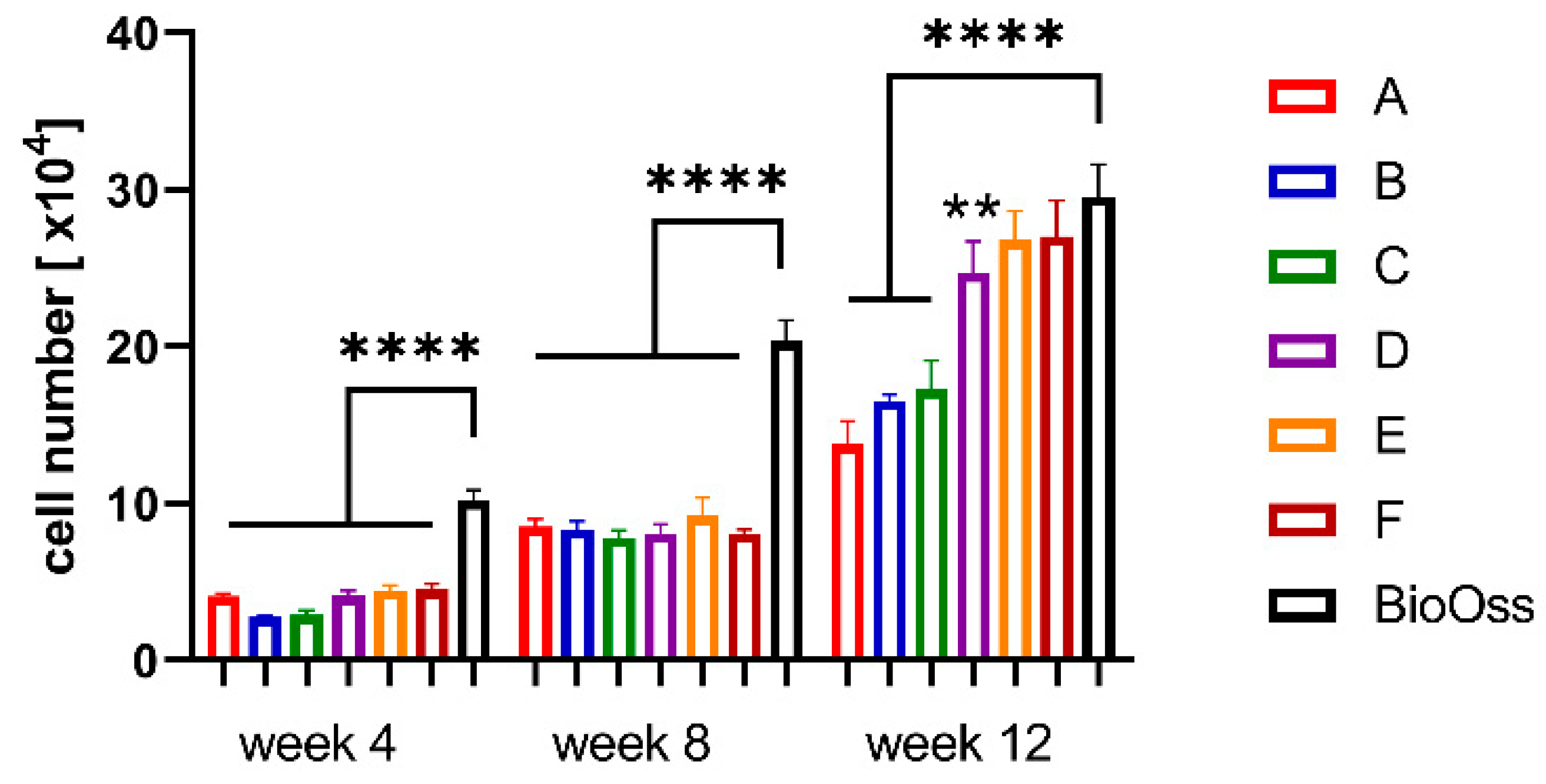
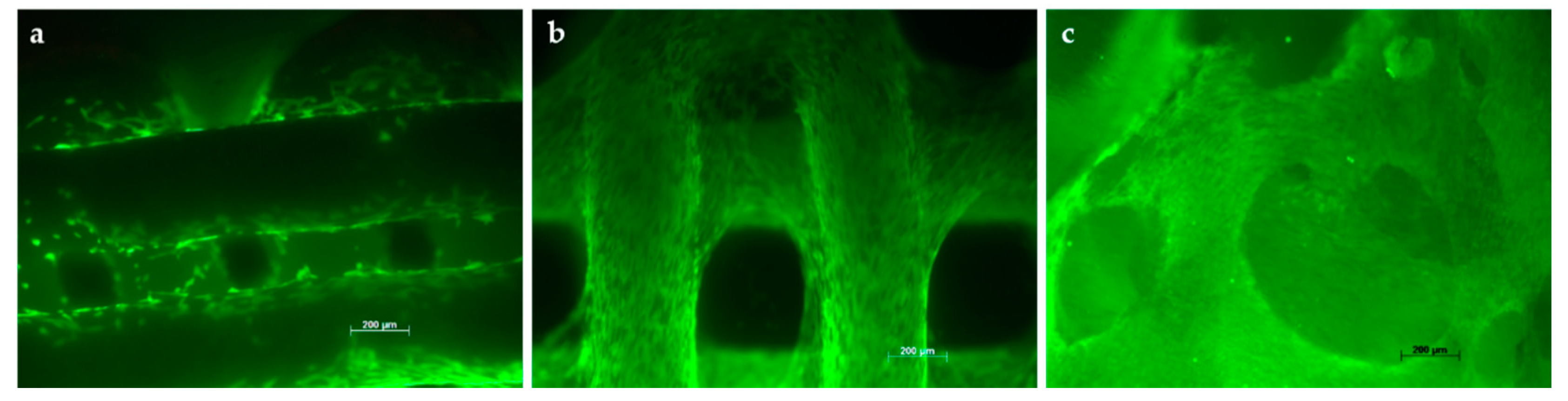
3.2. Colonization of Scaffolds
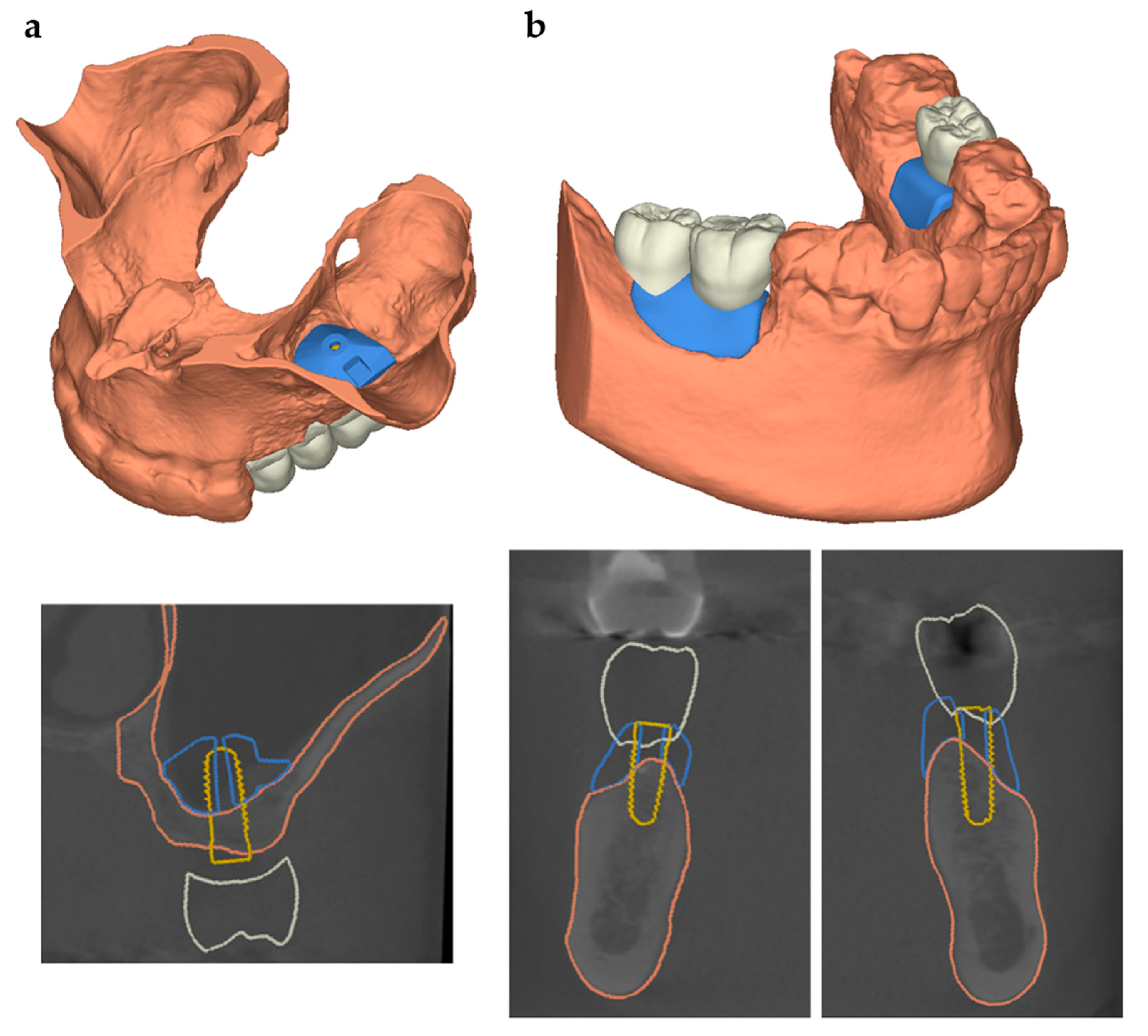
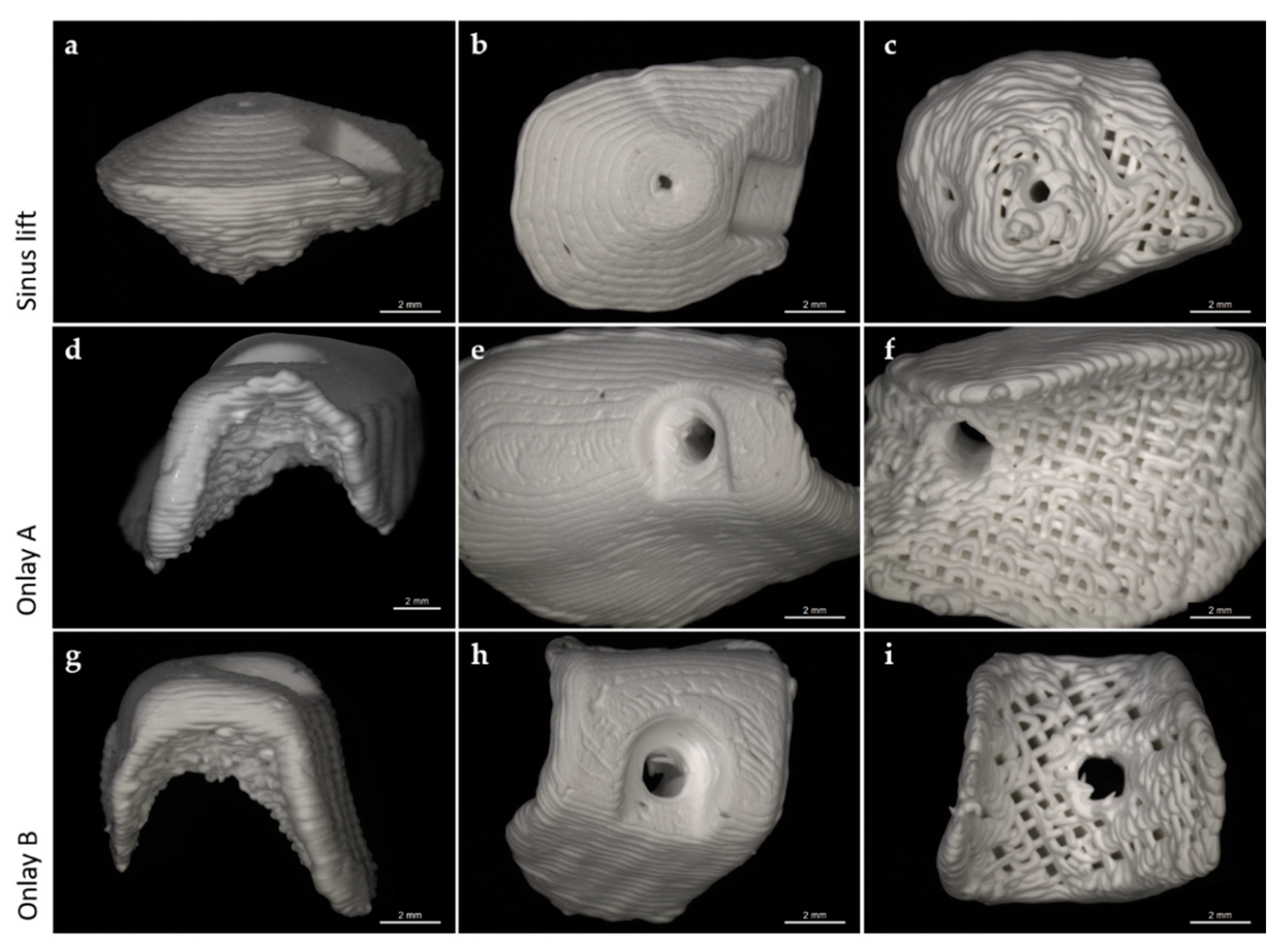
3.3. Scaffold Design for Intraoral Applications
3.4. Preliminary Investigations of Individual Scaffolds for Clinical Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shamsoddin, E.; Houshmand, B.; Golabgiran, M. Biomaterial selection for bone augmentation in implant dentistry: A systematic review. J. Adv. Pharm. Technol. Res. 2019, 10, 46–50. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Deluiz, D.; Deb, S.; Bruun, N.H.; Tinoco, E.M.B. Harvesting of Autogenous Bone Graft from the Ascending Mandibular Ramus Compared with the Chin Region: A Systematic Review and Meta-Analysis Focusing on Complications and Donor Site Morbidity. J. Oral Maxillofac. Res. 2020, 11, e1. [Google Scholar] [CrossRef]
- Scheerlinck, L.M.; Muradin, M.S.; van der Bilt, A.; Meijer, G.J.; Koole, R.; Van Cann, E.M. Donor site complications in bone grafting: Comparison of iliac crest, calvarial, and mandibular ramus bone. Int. J. Oral Maxillofac. Implant. 2013, 28, 222–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saha, A.; Shah, S.; Waknis, P.; Bhujbal, P.; Aher, S.; Vaswani, V. Comparison of minimally invasive versus conventional open harvesting technique for iliac bone graft in secondary alveolar bone grafting in cleft palate patients: A systematic review. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 241–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakoi, A.M.; Iorio, J.A.; Cahill, P.J. Autologous bone graft harvesting: A review of grafts and surgical techniques. Musculoskelet. Surg. 2015, 99, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Srivastava, V. Biomaterials and 3D printing techniques used in the medical field. J. Med. Eng. Technol. 2021, 45, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthc. Eng. 2019, 2019, 5340616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parmar, H.; Khan, T.; Tucci, F.; Umer, R.; Carlone, P. Advanced robotics and additive manufacturing of composites: Towards a new era in Industry 4.0. Mater. Manuf. Process. 2021, 1–35. [Google Scholar] [CrossRef]
- Öztürkmen, Y.; Canikliołu, M.; Karamehmetołu, M.; Fiükür, E. Calcium phosphate cement augmentation in the treatment of depressed tibial plateau fractures with open reduction and internal fixation. Acta. Orthop. Et. Traumatol. Turc. 2010, 44, 262–269. [Google Scholar] [CrossRef]
- Ji, C.; Ahn, J.G. Clinical experience of the brushite calcium phosphate cement for the repair and augmentation of surgically induced cranial defects following the pterional craniotomy. J. Korean Neurosurg. Soc. 2010, 47, 180–184. [Google Scholar] [CrossRef]
- Xu, H.H.K.; Wang, P.; Wang, L.; Bao, C.; Chen, Q.; Weir, M.D.; Chow, L.C.; Zhao, L.; Zhou, X.; Reynolds, M.A. Calcium phosphate cements for bone engineering and their biological properties. Bone Res. 2017, 5, 11056. [Google Scholar] [CrossRef] [Green Version]
- Reitmaier, S.; Kovtun, A.; Schuelke, J.; Kanter, B.; Lemm, M.; Hoess, A.; Heinemann, S.; Nies, B.; Ignatius, A. Strontium(II) and mechanical loading additively augment bone formation in calcium phosphate scaffolds. J. Orthop. Res. 2018, 36, 106–117. [Google Scholar] [CrossRef] [Green Version]
- Cha, J.K.; Kim, C.; Pae, H.C.; Lee, J.S.; Jung, U.W.; Choi, S.H. Maxillary sinus augmentation using biphasic calcium phosphate: Dimensional stability results after 3-6 years. J. Periodontal. Implant. Sci. 2019, 49, 47–57. [Google Scholar] [CrossRef]
- Wach, T.; Kozakiewicz, M. Fast-versus slow-resorbable calcium phosphate bone substitute materials-texture analysis after 12 months of observation. Materials 2020, 13, 3854. [Google Scholar] [CrossRef] [PubMed]
- Marongiu, G.; Verona, M.; Cardoni, G.; Capone, A. Synthetic bone substitutes and mechanical devices for the augmentation of osteoporotic proximal humeral fractures: A systematic review of clinical studies. J. Funct. Biomater. 2020, 11, 29. [Google Scholar] [CrossRef]
- Rolvien, T.; Barbeck, M.; Wenisch, S.; Amling, M.; Krause, M. Cellular Mechanisms Responsible for Success and Failure of Bone Substitute Materials. Int. J. Mol. Sci. 2018, 19, 2893. [Google Scholar] [CrossRef] [Green Version]
- Pepelassi, E.; Perrea, D.; Dontas, I.; Ulm, C.; Vrotsos, I.; Tangl, S. Porous Titanium Granules in comparison with Autogenous Bone Graft in Femoral Osseous Defects: A Histomorphometric Study of Bone Regeneration and Osseointegration in Rabbits. Biomed. Res. Int. 2019, 2019, 8105351. [Google Scholar] [CrossRef] [Green Version]
- Duda, M.; Pajak, J. The issue of bioresorption of the Bio-Oss xenogeneic bone substitute in bone defects. Ann. Univ. Mariae Curie-Skłodowska. Sect. D Med. 2004, 59, 269–277. [Google Scholar]
- Schlegel, A.K.; Donath, K. BIO-OSS®-A resorbable bone substitute? J. Long-Term Eff. Med. Implant. 1998, 8, 201–209. [Google Scholar]
- Ledogar, J.A.; Dechow, P.C.; Wang, Q.; Gharpure, P.H.; Gordon, A.D.; Baab, K.L.; Smith, A.L.; Weber, G.W.; Grosse, I.R.; Ross, C.F.; et al. Human feeding biomechanics: Performance, variation, and functional constraints. PeerJ 2016, 26, e2242. [Google Scholar] [CrossRef] [Green Version]
- Righetti, M.A.; Taube, O.L.S.; Palinkas, M.; Gonçalves, L.M.N.; Esposto, D.S.; de Mello, E.C.; Regalo, I.H.; Regalo, S.C.H.; Siéssere, S. Osteoarthrosis: Analyze of the Molar Bite Force, Thickness and Masticatory Efficiency. Prague Med. Rep. 2020, 121, 87–95. [Google Scholar] [CrossRef]
- La Monaca, G.; Iezzi, G.; Cristalli, M.P.; Pranno, N.; Sfasciotti, G.L.; Vozza, I. Comparative Histological and Histomorphometric Results of Six Biomaterials Used in Two-Stage Maxillary Sinus Augmentation Model after 6-Month Healing. Biomed. Res. Int. 2018, 2018, 9430989. [Google Scholar] [CrossRef] [Green Version]
- Yamada, M.; Egusa, H. Current bone substitutes for implant dentistry. J. Prosthodont Res. 2018, 62, 152–161. [Google Scholar] [CrossRef]
- Korn, P.; Ahlfeld, T.; Lahmeyer, F.; Kilian, D.; Sembdner, P.; Stelzer, R.; Pradel, W.; Franke, A.; Rauner, M.; Range, U.; et al. 3D Printing of Bone Grafts for Cleft Alveolar Osteoplasty-In vivo Evaluation in a Preclinical Model. Front. Bioeng. Biotechnol. 2020, 25, 217. [Google Scholar] [CrossRef]
- Sakkas, A.; Wilde, F.; Heufelder, M.; Winter, K.; Schramm, A. Autogenous bone grafts in oral implantology—is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int. J. Implant. Dent. 2017, 3, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Serrabona, J.; Sánchez-Garcés, M.Á.; Sánchez-Torres, A.; Gay-Escoda, C. Alveolar distraction osteogenesis for dental implant treatments of the vertical bone atrophy: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e70. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.H.; Eo, M.Y.; Kuk, T.S.; Myoung, H.; Kim, S.M. Rehabilitation of atrophic jaw using iliac onlay bone graft combined with dental implants. Int. J. Implant. Dent. 2019, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Salmen, F.S.; Oliveira, M.R.; Gabrielli, M.A.C.; Piveta, A.C.G.; Pereira Filho, V.A.; Ganrielli, M.F.R. Bone grafting for alveolar ridge reconstruction. Review of 166 cases. Rev. Do Colégio Bras. De Cir. 2017, 44, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepanovska, J.; Matejka, R.; Rosina, J.; Bacakova, L.; Kolarova, H. Treatments for enhancing the biocompatibility of titanium implants. Biomed. Pap. 2020, 164, 23–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samavedi, S.; Whittington, A.R.; Goldstein, A.S. Calcium phosphate ceramics in bone tissue engineering: A review of properties and their influence on cell behavior. Acta Biomater. 2013, 9, 8037–8045. [Google Scholar] [CrossRef]
- Hu, X.; Mei, S.; Wang, F.; Qian, J.; Xie, D.; Zhao, J.; Yang, L.; Wu, Z.; Wei, J. Implantable PEKK/tantalum microparticles composite with improved surface performances for regulating cell behaviors, promoting bone formation and osseointegration. Bioact. Mater. 2021, 6, 928–940. [Google Scholar] [CrossRef] [PubMed]
- Deligianni, D.D.; Katsala, N.D.; Koutsoukos, P.G.; Missirlis, Y.F. Effect of surface roughness of hydroxyapatite on human bone marrow cell adhesion, proliferation, differentiation and detachment strength. Biomaterials 2000, 22, 87–96. [Google Scholar] [CrossRef]
- Zhou, K.; Li, Y.; Zhang, L.; Jin, L.; Yuan, F.; Tan, J.; Yuan, G.; Pei, J. Nano-micrometer surface roughness gradients reveal topographical influences on differentiating responses of vascular cells on biodegradable magnesium. Bioact. Mater. 2021, 6, 262–272. [Google Scholar] [CrossRef]
- Richter, R.F.; Ahlfeld, T.; Gelinsky, M.; Lode, A. Development and characterization of composites consisting of calcium phosphate cements and mesoporous bioactive glass for extrusion-based fabrication. Materials 2019, 12, 2022. [Google Scholar] [CrossRef] [Green Version]
- Boughton, O.R.; Ma, S.; Zhao, S.; Arnold, M.; Lewis, A.; Hansen, U.; Cobb, J.P.; Giuliani, F.; Abel, R.L. Measuring bone stiffness using spherical indentation. PLoS ONE 2018, 13, e0200475. [Google Scholar] [CrossRef] [PubMed]
- Oftadeh, R.; Perez-Viloria, M.; Villa-Camacho, J.C.; Vaziri, A.; Nazarian, A. Biomechanics and Mechanobiology of Trabecular Bone: A Review. J. Biomech. Eng. 2015, 137, 0108021–01080215. [Google Scholar] [CrossRef] [Green Version]
- Maska, B.; Lin, G.-H.; Othman, A.; Behdin, S.; Travan, S.; Benavides, E.; Kapila, Y. Dental implants and grafting success remain high despite large variations in maxillary sinus mucosal thickening. Int. J. Implant. Dent. 2017, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Starch-Jensen, T.; Jensen, J.D. Maxillary Sinus Floor Augmentation: A Review of Selected Treatment Modalities. J. Oral Maxillofac. Res. 2017, 8, e3. [Google Scholar] [CrossRef]
- Thoma, D.S.; Cha, J.K.; Jung, U.W. Treatment concepts for the posterior maxilla and mandible: Short implants versus long implants in augmented bone. J. Periodontal Implant. Sci. 2017, 47, 2–12. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.H.; You, C.; Kim, K.H. Combined effect of a microporous layer and type I collagen coating on a biphasic calcium phosphate scaffold for bone tissue engineering. Materials 2015, 8, 1150–1161. [Google Scholar] [CrossRef] [Green Version]
- Ahlfeld, T.; Köhler, T.; Czichy, C.; Lode, A.; Gelinsky, M. A Methylcellulose Hydrogel as Support for 3D Plotting of Complex Shaped Calcium Phosphate Scaffolds. Gels 2018, 4, 68. [Google Scholar] [CrossRef] [Green Version]
- Ahlfeld, T.; Akkineni, A.R.; Förster, Y.; Köhler, T.; Knaack, S.; Gelinsky, M.; Lode, A. Design and Fabrication of Complex Scaffolds for Bone Defect Healing: Combined 3D Plotting of a Calcium Phosphate Cement and a Growth Factor-Loaded Hydrogel. Ann. Biomed. Eng. 2017, 45, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Lyu, C.; Shao, Z.; Zou, D.; Lu, J. Ridge Alterations following Socket Preservation Using a Collagen Membrane in Dogs. BioMed Res. Int. 2020, 2020, 1487681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarnieri, R.; Stefanelli, L.; De Angelis, F.; Mencio, F.; Pompa, G.; Di Carlo, S. Extraction Socket Preservation Using Porcine-Derived Collagen Membrane Alone or Associated with Porcine-Derived Bone. Clinical Results of Randomized Controlled Study. J. Oral Maxillofac. Res. 2017, 8, e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolerman, R.; Qahaz, N.; Barnea, E.; Mijiritsky, E.; Chaushu, L.; Tal, H.; Nissan, J. Allograft and collagen membrane augmentation procedures preserve the bone level around implants after immediate placement and restoration. Int. J. Environ. Res. Public Health 2020, 17, 1133. [Google Scholar] [CrossRef] [Green Version]
- Garcia, J.; Dodge, A.; Luepke, P.; Wang, H.L.; Kapila, Y.; Lin, G.H. Effect of membrane exposure on guided bone regeneration: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 328–338. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scaffold | Strand-to-Strand- Distance (µm) | Pore Size (µm) | Young’s Modulus # (MPa) | Compressive Strength # (MPa) |
|---|---|---|---|---|
| A | 430 | 100 | 870 ± 117 | 31.3 ± 6.8 |
| B | 560 | 230 | 870 ± 101 | 28.3 ± 1.3 |
| C | 690 | 360 | 749 ± 110 | 14.5 ± 2.0 |
| D | 820 | 490 | 586 ± 118 | 8.3 ± 1.8 |
| E | 950 | 620 | 477 ± 73 | 7.4 ± 0.9 |
| F | 1080 | 750 | 444 ± 44 | 5.2 ± 0.6 |
| Control | 7 ± 4 | 0.5 ± 0.007 |
| Scaffold | Young’s Modulus # (MPa) | Compressive Strength Resistance # (MPa) |
|---|---|---|
| 90° | 586 ± 118 | 8.3 ± 1.8 |
| 90° lateral | 159 ± 11 | 3.6 ± 0.3 |
| 45° | 191 ± 77 | 5.3 ± 1.7 |
| 45° lateral | 145 ± 101 | 1.2 ± 0.7 |
| Control | 7 ± 4 | 0.5 ± 0.007 |
| Scaffold | Young’s Modulus # (MPa) | Compressive Strength Resistance # (MPa) |
|---|---|---|
| Sinus lift | 135 ± 21 | 1.7 ± 0.3 |
| Onlay A | 239 ± 45 | 1.2 ± 0.3 |
| Onlay B | 127 ± 22 | 1.0 ± 0.2 |
| Control | 7 ± 4 | 0.5 ± 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muallah, D.; Sembdner, P.; Holtzhausen, S.; Meissner, H.; Hutsky, A.; Ellmann, D.; Assmann, A.; Schulz, M.C.; Lauer, G.; Kroschwald, L.M. Adapting the Pore Size of Individual, 3D-Printed CPC Scaffolds in Maxillofacial Surgery. J. Clin. Med. 2021, 10, 2654. https://doi.org/10.3390/jcm10122654
Muallah D, Sembdner P, Holtzhausen S, Meissner H, Hutsky A, Ellmann D, Assmann A, Schulz MC, Lauer G, Kroschwald LM. Adapting the Pore Size of Individual, 3D-Printed CPC Scaffolds in Maxillofacial Surgery. Journal of Clinical Medicine. 2021; 10(12):2654. https://doi.org/10.3390/jcm10122654
Chicago/Turabian StyleMuallah, David, Philipp Sembdner, Stefan Holtzhausen, Heike Meissner, André Hutsky, Daniel Ellmann, Antje Assmann, Matthias C. Schulz, Günter Lauer, and Lysann M. Kroschwald. 2021. "Adapting the Pore Size of Individual, 3D-Printed CPC Scaffolds in Maxillofacial Surgery" Journal of Clinical Medicine 10, no. 12: 2654. https://doi.org/10.3390/jcm10122654