
Perinatal Mental Health during COVID-19 Pandemic: An Integrative Review and Implications for Clinical Practice

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Eligibility Criteria
2.3. Data Collection Process
2.4. Data Items
2.5. Quality Assessment
3. Results
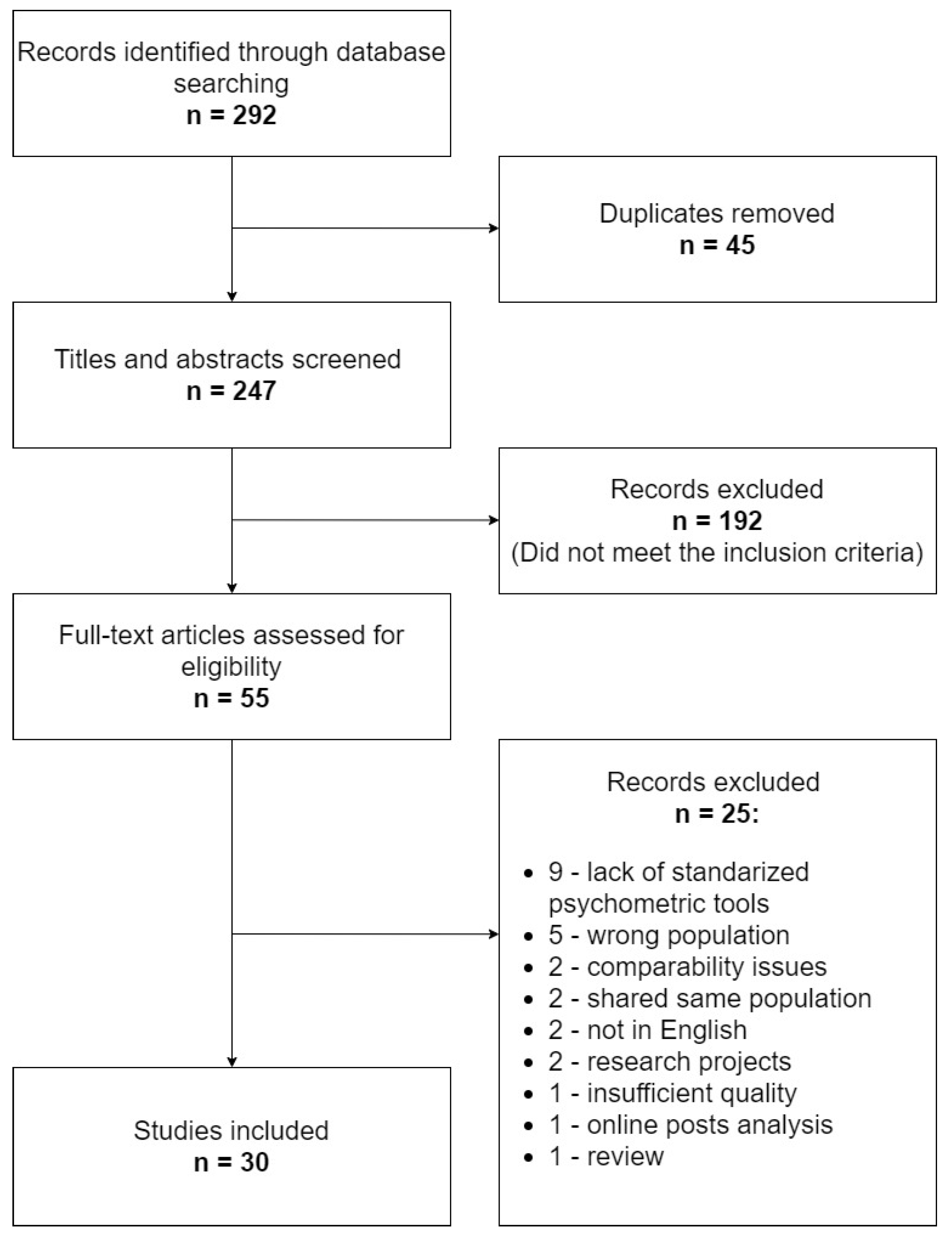
3.1. Search Results
3.2. General Characteristics of the Studies

{kind=link}
| Ref | Country | Time | Participants | Recruitment | Tools |
|---|---|---|---|---|---|
| Assessment of depression and anxiety | |||||
| [24] | Belgium | No information | 5866:2421 pregnant and 3445 breastfeeding women | Online survey | EPDS 1 GAD-7 |
| [25] | Canada | 04.2020 | 1754 pregnant women: 496 before and 1258 during the pandemic | Online survey—social media, advertisements in prenatal clinics | K10 |
| [26,27] | Canada | 04.2020 | 1987 pregnant women | Online survey—social media | EPDS 1 PROMIS PRAQ |
| [28] | China | 02.2020 | 156 pregnant women | Online survey—social media and distributed by doctors | SDS SAS |
| [29] | China | 02–03.2020 | 859:544 pregnant and 315 non-pregnant women | Online survey—social media | PHQ-9 GAD-7 |
| [30] | China | 03–06.2020 (remission phase) | 625:516 pregnant and 109 postpartum women | Written survey—hospital patients | EPDS 1 GAD-7 |
| [31] | Italy | 03–05.2020 | 575:389 pregnant and 186 postpartum women | Online survey—social media | EPDS 1 STAI |
| [32] | Turkey | No information | 260 pregnant women | Online survey—hospital patients | EPDS 2 BDI BAI |
| [33] | Turkey | 04–05.2020 | 63 pregnant women before and during the pandemic | Face-to-face interviews—hospital patients | IDAS II BAI |
| [34] | Turkey | 06–07.2020 | 403 pregnant women | Online survey—social media | HADS |
| [35] | USA | 03–04.2020 | 31 pregnant and postpartum women | Phone interview and online survey—social media | PHQ-2 GAD-7 |
| [36] | USA | 04–05.2020 | 913 pregnant women | Online survey—medical records system | PHQ-2 GAD-7 |
| [37] | Qatar | 06–07.2020 | 288 pregnant and postpartum women | Written survey—hospital patients | PHQ-9 GAD-7 |
| Assessment of depression | |||||
| [38] | China | 01–02.2020 | 4124 pregnant women: 2839 before and 1285 after the epidemic declaration in China | Written survey—hospital patients | EPDS 3 |
| [39] | Hong Kong | 01–04.2020 | 4531 postpartum women (1 day and 1 week after delivery): 3577 before and 954 during the pandemic | Written survey—hospital patients | EPDS 3 |
| [40] | Israel | 03–05.2020 | 369 high-risk pregnant women: 279 before and 90 during the pandemic | Written survey—patients of high-risk pregnancy units | EPDS 3 |
| [41] | Italy | 03–05.2020 | 192 postpartum women: 101 before and 91 during the pandemic | Written survey—hospital patients | EPDS 1 |
| [42] | Japan | 05–06.2020 | 1777 pregnant women | Online survey—users of applications | EPDS 1 |
| [43] | Turkey | 06.2020 | 223 postpartum women (48 h after delivery) | Written survey—hospital patients | EPDS 1 |
| [44] | USA | 02–06.2020 | 485 pregnant women | Written survey—hospital patients | EPDS 4 |
| [45] | USA | 04.2020 | 2099 pregnant women | Online survey—social media | EPDS 5 |
| Assessment of anxiety | |||||
| [46] | China | 02.2020 | 1947 pregnant women | Online survey—social media and written survey—hospital patients | SAS |
| [47] | China | 02.2020 | 308 pregnant women | Online survey—hospital patients | SAS |
| [48] | Israel | 03–04.2020 | 403 pregnant women | Online survey—social media | PRAS |
| [49] | Italy | 03.2020 | 178 pregnant women | Online survey—hospital patients | STAI |
| [50] | Italy | 03–04.2020 | 100 pregnant women | Written survey—hospital patients | STAI-SF |
| [51] | Turkey | 04.2020 | 203 pregnant and 101 non-pregnant women | Written survey—hospital patients | STAI |
| [52] | USA | 04.2020 | 788 pregnant women | Online survey—social media | GAD-7 PREPS |
| [53] | USA | 04.2020 | 2740 pregnant women | Online survey—social media | PRAS VAS-anxiety |
| [54] | USA | 04–05.2020 | 4451 pregnant women | Online survey—social media | PREPS |
3.3. Depression and Anxiety Symptoms
| Reference | Symptoms of Depression | Symptoms of Anxiety | Comparator |
|---|---|---|---|
| Depression and Anxiety | |||
| [24] | ↑ Pregnancy—25.3%; postpartum 23.6% | ↑ 39.4% mild; 13.6% moderate-to-severe anxiety | Estimates in Belgium prior to the pandemic |
| [25] | ↑ | ↑ | Pre-pandemic cohort |
| [26] | ↑ 37% | ↑ 57% | Similar pre-pandemic pregnancy cohorts |
| [28] | ↑ 50.6% | ↔ 8.3% | Literature data |
| [29] | ↓ 5.3% | ↓ 6.8% | Non-pregnant women during pandemic |
| [30] | 19.2% | 31.2% | None |
| [31] | ↑ 34.2% (pregnant women) ↑ 26.3% (postpartum women) | ↑ 64% (pregnant women) ↑ 57.7% (postpartum women) | Literature data |
| [32] | 35.4% | None | |
| [33] | ↑ | ↑ | Test–retest study |
| [34] | 56.3% | 64.5% | None |
| [35] | 12% | 60% | None |
| [36] | 9.9% | 11.1% | None |
| [37] | ↑ 39.2% | ↑ 34.4% | Literature data |
| Depression | |||
| [38] | ↑ 29.6% | Pre-alert group | |
| [39] | ↑ 14.4% | Pre-alert group | |
| [40] | ↔ 25.0% | Pre-pandemic hospitalized high-risk pregnancy group | |
| [41] | ↑ 28.6% | Pre-pandemic control group | |
| [42] | 17% | None | |
| [43] | 14.7% | None | |
| [44] | ↓ score ≥ 9 in EPDS—15.1% score ≥ 12 8.2% | Pre-restriction group | |
| [45] | 24% | None | |
| Anxiety | |||
| [46] | 17.2% | None | |
| [47] | ↑ 14.3% | General population prior to COVID-19 | |
| [49] | ↑ 77.0% | Literature data | |
| [50] | 68% | None | |
| [51] | ↑ 62.6% | Literature data | |
| [52] | Mild—35.6%; moderate—21.6%; severe anxiety symptoms—21.7% | None | |
3.4. Risk Factors
| Perinatal care | Uncertainty and concerns about perinatal care [26,35] Alterations to prenatal appointments [53,54,57] Discomfort with hospital and ambulatory visits [34] |
| Social factors | Social isolation [26] Lack of social support [31,35,42] Being single [36,42] Partner’s absence at delivery [31] Tension/conflict at home [26,53] |
| Demographic | Being a woman of color [36,54] Being an Arab woman [48] Education level (high—[49], low—[34,53]) Younger age [36,42] |
| Financial | Low income, financial difficulties [25,42] COVID-19-related financial stress and income loss [45,54] Unemployment [34,42] |
| Factors concerning COVID-19 | Stress of getting infected with COVID-19 [26,35,42,48,52,53] Suffering subjective symptoms of suspected infection [46] Perceived risk of having had COVID-19 [54] Having infected friends/families/colleagues [57] Self or family member being an essential worker [53] Living in a location with a large number of COVID-19 cases [46,53] |
| Health state | High-risk pregnancy [48,52,54] Chronic illness [54] Previous psychiatric diagnosis [25,31] Previous adverse experiences during pregnancy [57] |
| Insufficient information | No information about the effects of COVID-19 [34] Inconsistent messaging from information sources [35] |
3.5. Protective Factors
| Social | Social support [26,47,48] Partner emotional support [35] Low hostility level in close relationships [36] Use of virtual communication platforms [35] |
| COVID-related information | Information from healthcare workers and televised pandemic-related information [37] More knowledge about COVID-19 [46] Rational perception of COVID-related risk [46,47] |
| Activity | Physical activity [26,34] Access to outdoor space [35,54] Engagement in various healthy behaviors [35,54] |
| Personal | More self-reliance [36] Better emotion regulation [36] Positive attitudes towards online medical consultation [46] |
4. Discussion
4.1. Anxiety and Depression Symptoms in Pregnant Women and New Mothers
4.2. Risk and Protective Factors
4.3. Practical Implications
4.3.1. Information for Pregnant Women and New Mothers
- Recommendations concerning social isolation behaviors, breastfeeding and impacts of disasters on mental and physical health [35];
- Infection prevention procedures for labor, delivery and postpartum [52];
- The way medical and midwife care is provided in the time of COVID-19 and methods of conducting visits (in the surgery and online) [35];
- Information on how to get help and/or psychological support [35].
4.3.2. Assessment of Risk Factors and Screening for Depression/Anxiety Symptoms
- Mental health issues should be addressed during visits—questions should be asked about perceived stress, symptoms of mental health problems and social support [25];
- It is necessary to pay particular attention to patients from the depression or anxiety risk groups in the times of COVID-19, i.e., single and without social support, younger age, with financial difficulties, unemployed, those with high stress of getting infected, with high-risk pregnancy, with chronic illness, with previous psychiatric diagnosis and with previous adverse experiences during pregnancy;
- It is important to continue to monitor the mood of postpartum patients, especially women with anxiety and depressive disorders in pregnancy [53];
- Remote questionnaires may prove useful in identifying women with mental health problems [49].
4.3.3. Interventions in Women with Perinatal Mental Health Problems
4.4. Limitations
4.5. Long-Term Effects of the COVID-19 Pandemic
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Pneumonia of Unknown Cause—China. Available online: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/ (accessed on 14 February 2021).
- WHO. Novel Coronavirus—China. Available online: http://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 14 February 2021).
- Anand, K.B.; Karade, S.; Sen, S.; Gupta, R.M. SARS-CoV-2: Camazotz’s Curse. Med J. Armed Forces India 2020, 76, 136–141. [Google Scholar] [CrossRef]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- WHO. Announces COVID-19 Outbreak a Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 14 February 2021).
- Worldometers. Available online: https://www.worldometers.info/coronavirus/ (accessed on 1 March 2021).
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Druckenmiller, H.; Huang, L.Y.; Hultgren, A.; Krasovich, E. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature 2020, 584, 262–267. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Buekens, P.; Alger, J.; Bréart, G.; Cafferata, M.L.; Harville, E.; Tomasso, G. A call for action for COVID-19 surveillance and research during pregnancy. Lancet Glob. Health 2020, 8, 877–878. [Google Scholar] [CrossRef]
- Orsolini, L.; Valchera, A.; Vecchiotti, R.; Tomasetti, C.; Iasevoli, F.; Fornaro, M.; De Berardis, D.; Perna, G.; Pompili, M.; Bellantuono, C. Suicide during Perinatal Period: Epidemiology, Risk Factors, and Clinical Correlates. Front. Psychiatry 2016, 7, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, T.; Diego, M.; Hernandez-Reif, M.; Figueiredo, B.; Deeds, O.; Ascencio, A.; Schanberg, S.; Kuhn, C. Comorbid depression and anxiety effects on pregnancy and neonatal outcome. Infant Behav. Dev. 2010, 33, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tirumalaraju, V.; Suchting, R.; Evans, J.; Goetzl, L.; Refuerzo, J.; Neumann, A.; Anand, D.; Ravikumar, R.; Green, C.E.; Cowen, P.J.; et al. Risk of Depression in the Adolescent and Adult Offspring of Mothers With Perinatal Depression: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e208783. [Google Scholar] [CrossRef] [PubMed]
- Borchers, L.R.; Dennis, E.L.; King, L.S.; Humphreys, K.L.; Gotlib, I.H. Prenatal and postnatal depressive symptoms, infant white matter, and toddler behavioral problems. J. Affect. Disord. 2020, 282, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 pandemic and maternal mental health: A systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2020, 1–8. [Google Scholar] [CrossRef]
- Sun, F.; Zhu, J.; Tao, H.; Ma, Y.; Jin, W. A systematic review involving 11,187 participants evaluating the impact of COVID-19 on anxiety and depression in pregnant women. J. Psychosom. Obstet. Gynecol. 2020, 42, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Tomfohr-Madsen, L.M.; Racine, N.; Giesbrecht, G.F.; Lebel, C.; Madigan, S. Depression and anxiety in pregnancy during COVID-19: A rapid review and meta-analysis. Psychiatry Res. 2021, 300, 113912. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.; Guan, J.; Cao, L.; Wang, M.; Zhao, H.; Chen, L.; Yan, L. Psychological effects caused by COVID-19 pandemic on pregnant women: A systematic review with meta-analysis. Asian J. Psychiatry 2021, 56, 102533. [Google Scholar] [CrossRef]
- Yan, H.; Ding, Y.; Guo, W. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Front. Psychol. 2020, 11, 3324. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; Higgins, J.P.; Sterne, J.; Tugwell, P.; Reeves, B.C. Checklists of methodological issues for review authors to consider when including non-randomized studies in systematic reviews. Res. Synth. Methods 2013, 4, 63–77. [Google Scholar] [CrossRef]
- Ceulemans, M.; Hompes, T.; Foulon, V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: A call for action. Int. J. Gynaecol. Obstet. 2020, 151, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Et Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Corrigendum to elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic journal of affective disorders 277 (2020) 5–13. J. Affect. Disord. 2020, 279, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Hu, R.; Lu, C.; Huang, D.; Cui, D.; Huang, G.; Zhang, M. Investigation on the mental health status of pregnant women in China during the Pandemic of COVID-19. Arch. Gynecol. Obstet. 2020, 303, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Shi, H.; Liu, Z.; Peng, S.; Wang, R.; Qi, L.; Li, Z.; Yang, J.; Ren, Y.; Song, X.; et al. The prevalence of psychiatric symptoms of pregnant and non-pregnant women during the COVID-19 epidemic. Transl. Psychiatry 2020, 10, 1–7. [Google Scholar] [CrossRef]
- Zeng, L.N.; Chen, L.G.; Yang, C.M.; Zeng, L.P.; Zhang, L.Y.; Peng, T.M. Mental health care for pregnant women in the COVID-19 outbreak is urgently needed. Women Birth 2020, 34, 210–211. [Google Scholar] [CrossRef]
- Molgora, S.; Accordini, M. Motherhood in the Time of Coronavirus: The Impact of the Pandemic Emergency on Expectant and Postpartum Women’s Psychological Well-Being. Front. Psychol. 2020, 11, 567155. [Google Scholar] [CrossRef]
- Durankuş, F.; Aksu, E. Effects of the COVID-19 pandemic on anxiety and depressive symptoms in pregnant women: A preliminary study. J. Matern. Fetal Neonatal Med. 2020, 1–7. [Google Scholar] [CrossRef]
- Ayaz, R.; Hocaoğlu, M.; Günay, T.; Yardımcı, O.D.; Turgut, A.; Karateke, A. Anxiety and depression symptoms in the same pregnant women before and during the COVID-19 pandemic. J. Perinat. Med. 2020, 48, 965–970. [Google Scholar] [CrossRef]
- Kahyaoglu Sut, H.; Kucukkaya, B. Anxiety, depression, and related factors in pregnant women during the COVID-19 pandemic in Turkey: A web-based cross-sectional study. Perspect. Psychiatr. Care 2020. [Google Scholar] [CrossRef]
- Farewell, C.V.; Jewell, J.; Walls, J.; Leiferman, J.A. A Mixed-Methods Pilot Study of Perinatal Risk and Resilience During COVID-19. J. Prim. Care Community Health 2020, 11. [Google Scholar] [CrossRef]
- Gur, R.E.; White, L.K.; Waller, R.; Barzilay, R.; Moore, T.M.; Kornfield, S.; Njoroge, W.F.M.; Duncan, A.F.; Chaiyachati, B.H.; Parish-Morris, J.; et al. The Disproportionate Burden of the COVID-19 Pandemic Among Pregnant Black Women. Psychiatry Res. 2020, 293, 113475. [Google Scholar] [CrossRef]
- Farrell, T.; Reagu, S.; Mohan, S.; Elmidany, R.; Qaddoura, F.; Ahmed, E.; Corbett, G.; Lindow, S.; Abuyaqoub, S.; Alabdulla, M. The Impact of the COVID-19 Pandemic on the Perinatal Mental Health of Women. J. Perinat. Med. 2020, 48, 971–976. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, C.; Liu, H.; Duan, C.; Li, C.; Fan, J.; Li, H.; Chen, L.; Xu, H.; Li, X.; et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am. J. Obstet. Gynecol. 2020, 223, 240.e1–240.e9. [Google Scholar] [CrossRef] [PubMed]
- Hui, P.W.; Ma, G.; Seto, M.T.Y.; Cheung, K.W. Effect of COVID-19 on delivery plans and postnatal depression scores of pregnant women. Hong Kong Med. J. 2020, 26, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Sade, S.; Sheiner, E.; Wainstock, T.; Hermon, N.; Yaniv Salem, S.; Kosef, T.; Lanxner Battat, T.; Oron, S.; Pariente, G. Risk for Depressive Symptoms among Hospitalized Women in High-Risk Pregnancy Units during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 2449. [Google Scholar] [CrossRef]
- Zanardo, V.; Manghina, V.; Giliberti, L.; Vettore, M.; Severino, L.; Straface, G. Psychological impact of COVID-19 quarantine measures in northeastern Italy on mothers in the immediate postpartum period. Int. J. Gynaecol. Obstet. 2020, 150, 184–188. [Google Scholar] [CrossRef]
- Matsushima, M.; Horiguchi, H. The COVID-19 Pandemic and Mental Well-Being of Pregnant Women in Japan: Need for Economic and Social Policy Interventions. Disaster Med. Public Health Prep. 2020, 1–6. [Google Scholar] [CrossRef]
- Oskovi-Kaplan, Z.A.; Buyuk, G.N.; Ozgu-Erdinc, A.S.; Keskin, H.L.; Ozbas, A.; Moraloglu Tekin, O. The Effect of COVID-19 Pandemic and Social Restrictions on Depression Rates and Maternal Attachment in Immediate Postpartum Women: A Preliminary Study. Psychiatr. Q. 2020, 92, 675–682. [Google Scholar] [CrossRef]
- Silverman, M.E.; Medeiros, C.; Burgos, L. Early pregnancy mood before and during COVID-19 community restrictions among women of low socioeconomic status in New York City: A preliminary study. Arch. Women’s Ment. Health 2020, 23, 779–782. [Google Scholar] [CrossRef] [PubMed]
- Thayer, Z.M.; Gildner, T.E. COVID-19-related financial stress associated with higher likelihood of depression among pregnant women living in the United States. Am. J. Hum. Biol. 2020, 33, e23508. [Google Scholar] [CrossRef]
- Liu, X.; Chen, M.; Wang, Y.; Sun, L.; Zhang, J.; Shi, Y.; Wang, J.; Zhang, H.; Sun, G.; Baker, P.N.; et al. Prenatal anxiety and obstetric decisions among pregnant women in Wuhan and Chongqing during the COVID-19 outbreak: A cross-sectional study. Bjog Int. J. Obstet. Gynaecol. 2020, 127, 1229–1240. [Google Scholar] [CrossRef]
- Yue, C.; Liu, C.; Wang, J.; Zhang, M.; Wu, H.; Li, C.; Yang, X. Association between social support and anxiety among pregnant women in the third trimester during the coronavirus disease 2019 (COVID-19) epidemic in Qingdao, China: The mediating effect of risk perception. Int. J. Soc. Psychiatry 2020. [Google Scholar] [CrossRef]
- Taubman-Ben-Ari, O.; Chasson, M.; Abu-Sharkia, S. Childbirth anxieties in the shadow of COVID-19: Self-compassion and social support among Jewish and Arab pregnant women in Israel. Health Soc. Care Community 2020. [Google Scholar] [CrossRef]
- Mappa, I.; Distefano, F.A.; Rizzo, G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: A prospectic observational study. J. Perinat. Med. 2020, 48, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Saccone, G.; Florio, A.; Aiello, F.; Venturella, R.; De Angelis, M.C.; Locci, M.; Bifulco, G.; Zullo, F.; Di Spiezio Sardo, A. Psychological impact of coronavirus disease 2019 in pregnant women. Am. J. Obstet. Gynecol. 2020, 223, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Yassa, M.; Yassa, A.; Yirmibeş, C.; Birol, P.; Ünlü, U.G.; Tekin, A.B.; Sandal, K.; Mutlu, M.A.; Çavuşoğlu, G.; Tug, N. Anxiety levels and obsessive compulsion symptoms of pregnant women during the COVID-19 pandemic. Turk. J. Obstet. Gynecol. 2020, 17, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Pandemic-related pregnancy stress and anxiety among women pregnant during the coronavirus disease 2019 pandemic. Am. J. Obstet. Gynecol. MFM 2020, 2, 100155. [Google Scholar] [CrossRef]
- Moyer, C.A.; Compton, S.D.; Kaselitz, E.; Muzik, M. Pregnancy-related anxiety during COVID-19: A nationwide survey of 2740 pregnant women. Arch. Women’s Ment. Health 2020, 23, 757–765. [Google Scholar] [CrossRef]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Vulnerability and resilience to pandemic-related stress among U.S. women pregnant at the start of the COVID-19 pandemic. Soc. Sci. Med. 2020, 266, 113348. [Google Scholar] [CrossRef]
- Suchowiak, S.; Wszołek, K.; Suwalska, J.; Łojko, D.; Suwalska, A. Screening for perinatal depression: A review of tools and barriers. Neuropsychiatr. I Neuropsychol. 2020, 15, 60–69. [Google Scholar] [CrossRef]
- Preis, H.; Mahaffey, B.; Lobel, M. Psychometric properties of the Pandemic-Related Pregnancy Stress Scale (PREPS). J. Psychosom. Obstet. Gynaecol. 2020, 41, 191–197. [Google Scholar] [CrossRef]
- Zeng, X.; Li, W.; Sun, H.; Luo, X.; Garg, S.; Liu, T.; Zhang, J.; Zhang, Y. Mental Health Outcomes in Perinatal Women During the Remission Phase of COVID-19 in China. Front. Psychiatry 2020, 11, 571876. [Google Scholar] [CrossRef]
- Hotopf, M.; Bullmore, E.; O’Connor, R.C.; Holmes, E.A. The scope of mental health research during the COVID-19 pandemic and its aftermath. Br. J. Psychiatry 2020, 217, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Caparros-Gonzalez, R.A.; Ganho-Ávila, A.; Torre-Luque, A. The COVID-19 Pandemic Can Impact Perinatal Mental Health and the Health of the Offspring. Behav. Sci. 2020, 10, 162. [Google Scholar] [CrossRef]
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernàndez-Flix, S.; de Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Camps, J.; et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. medRxiv 2020. [Google Scholar] [CrossRef]
- Salzberger, B.; Buder, F.; Lampl, B.; Ehrenstein, B.; Hitzenbichler, F.; Holzmann, T.; Schmidt, B.; Hanses, F. Epidemiology of SARS-CoV-2. Infection 2020, 49, 233–239. [Google Scholar] [CrossRef]
- Parra-Saavedra, M.; Villa-Villa, I.; Pérez-Olivo, J.; Guzman-Polania, L.; Galvis-Centurion, P.; Cumplido-Romero, Á.; Santacruz-Vargas, D.; Rivera-Moreno, E.; Molina-Giraldo, S.; Guillen-Burgos, H.; et al. Attitudes and collateral psychological effects of COVID-19 in pregnant women in Colombia. Int. J. Gynaecol. Obstet 2020, 151, 203–208. [Google Scholar] [CrossRef]
- RCOG. Coronavirus Infection and Pregnancy; Royal College of Obstetrics and Gynaecologists: London, UK, 2020. [Google Scholar]
- Wu, C.Y.; Chang, C.K.; Hayes, R.D.; Broadbent, M.; Hotopf, M.; Stewart, R. Clinical risk assessment rating and all-cause mortality in secondary mental healthcare: The South London and Maudsley NHS Foundation Trust Biomedical Research Centre (SLAM BRC) Case Register. Psychol. Med. 2012, 42, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, P.; Borreani, E.; Ghosh, P.; Methuen, C.; Patel, M.; Joseph, M. Screening for suicidal thoughts in primary care: The views of patients and general practitioners. Ment. Health Fam. Med. 2008, 5, 229–235. [Google Scholar]
- Dazzi, T.; Gribble, R.; Wessely, S.; Fear, N. Does asking about suicide and related behaviours induce suicide ideation? What is the evidence? Psychol. Med. 2014, 44, 3361–3363. [Google Scholar] [CrossRef] [Green Version]
- Peahl, A.F.; Smith, R.D.; Moniz, M.H. Prenatal care redesign: Creating flexible maternity care models through virtual care. Am. J. Obstet. Gynecol. 2020, 223, 389.e1–389.e10. [Google Scholar] [CrossRef]
- Madden, N.; Emeruwa, U.N.; Friedman, A.M.; Aubey, J.J.; Aziz, A.; Baptiste, C.D.; Coletta, J.M.; D’Alton, M.E.; Fuchs, K.M.; Goffman, D.; et al. Telehealth Uptake into Prenatal Care and Provider Attitudes during the COVID-19 Pandemic in New York City: A Quantitative and Qualitative Analysis. Am. J. Perinatol. 2020, 37, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, D.; Faucher, M.A.; Bouzid, J.; Quint-Bouzid, M.; Nelson, D.B.; Duryea, E. Patient Perspectives on Audio-Only Virtual Prenatal Visits Amidst the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Pandemic. Obstet. Gynecol. 2020, 136, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Hermann, A.; Deligiannidis, K.M.; Bergink, V.; Monk, C.; Fitelson, E.M.; Robakis, T.K.; Birndorf, C. Response to SARS-Covid-19-related visitor restrictions on labor and delivery wards in New York City. Arch. Women’s Ment. Health 2020, 23, 793–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet. Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- WHO. Resolutions And Decisions. In Proceedings of the World Health Organization Fifty-Eighth World Health Assembly, Geneva, Switzerland, 16–25 May 2005. [Google Scholar]
- CDC. Centers for Disease Control and Prevention (CDC). Interim Considerations for Infection Prevention and Control of Coronavirus Disease 2019 (COVID-19) in Inpatient Obstetric Healthcare Settings; Updated 20 May 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/inpatient-obstetric-healthcare-guidance.html (accessed on 23 February 2021).
- Thapa, S.B.; Mainali, A.; Schwank, S.E.; Acharya, G. Maternal mental health in the time of the COVID-19 pandemic. Acta Obstet. Et Gynecol. Scand. 2020, 99, 817–818. [Google Scholar] [CrossRef]
- Jenkins, E.K.; McAuliffe, C.; Hirani, S.; Richardson, C.; Thomson, K.C.; McGuinness, L.; Morris, J.; Kousoulis, A.; Gadermann, A. A portrait of the early and differential mental health impacts of the COVID-19 pandemic in Canada: Findings from the first wave of a nationally representative cross-sectional survey. Prev. Med. 2021, 145, 106333. [Google Scholar] [CrossRef]
- O’Connor, K.; Wrigley, M.; Jennings, R.; Hill, M.; Niazi, A. Mental health impacts of COVID-19 in Ireland and the need for a secondary care mental health service response. Ir. J. Psychol. Med. 2020, 1–9. [Google Scholar] [CrossRef]
- O’Connor, E.; Senger, C.A.; Henninger, M.L.; Coppola, E.; Gaynes, B.N. Interventions to Prevent Perinatal Depression: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2019, 321, 588–601. [Google Scholar] [CrossRef] [Green Version]
- Accortt, E.E.; Wong, M.S. It Is Time for Routine Screening for Perinatal Mood and Anxiety Disorders in Obstetrics and Gynecology Settings. Obstet. Gynecol. Surv. 2017, 72, 553–568. [Google Scholar] [CrossRef] [PubMed]
- Cox, E.Q.; Sowa, N.A.; Meltzer-Brody, S.E.; Gaynes, B.N. The Perinatal Depression Treatment Cascade: Baby Steps Toward Improving Outcomes. J. Clin. Psychiatry 2016, 77, 1189–1200. [Google Scholar] [CrossRef] [PubMed]
- Osborne, L.M.; Kimmel, M.C.; Surkan, P.J. The Crisis of Perinatal Mental Health in the Age of Covid-19. Matern. Child Health J. 2021, 25, 349–352. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwalska, J.; Napierała, M.; Bogdański, P.; Łojko, D.; Wszołek, K.; Suchowiak, S.; Suwalska, A. Perinatal Mental Health during COVID-19 Pandemic: An Integrative Review and Implications for Clinical Practice. J. Clin. Med. 2021, 10, 2406. https://doi.org/10.3390/jcm10112406
Suwalska J, Napierała M, Bogdański P, Łojko D, Wszołek K, Suchowiak S, Suwalska A. Perinatal Mental Health during COVID-19 Pandemic: An Integrative Review and Implications for Clinical Practice. Journal of Clinical Medicine. 2021; 10(11):2406. https://doi.org/10.3390/jcm10112406
Chicago/Turabian StyleSuwalska, Julia, Maria Napierała, Paweł Bogdański, Dorota Łojko, Katarzyna Wszołek, Sara Suchowiak, and Aleksandra Suwalska. 2021. "Perinatal Mental Health during COVID-19 Pandemic: An Integrative Review and Implications for Clinical Practice" Journal of Clinical Medicine 10, no. 11: 2406. https://doi.org/10.3390/jcm10112406