
Systemic Inflammatory Parameters in Patients with Elderly-Onset Rheumatoid Arthritis (EORA) and Young-Onset Rheumatoid Arthritis (YORA)—An Observational Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical and Laboratory Findings
2.3. Statistical Analysis
3. Results
3.1. Demographic and Disease-Related Variables in 113 RA Patients
3.2. Clinical Characteristics of Patients with YORA and EORA
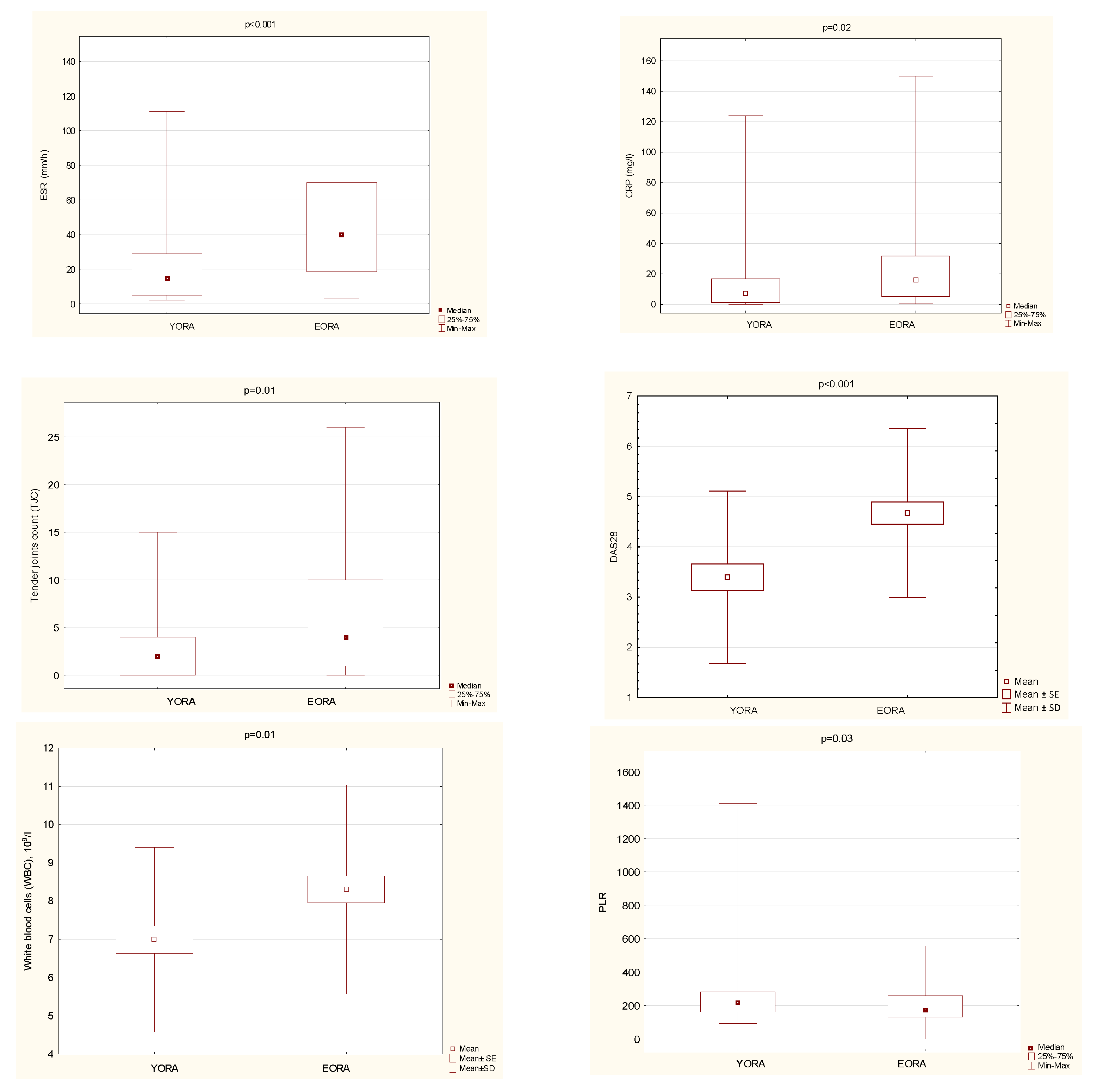
3.3. Disease Activity Parameters in Patients with YORA and EORA
3.4. Relationship between the Disease Activity and Metabolic Parameters with Timewise and Hematological Inflammatory Markers (NLR and PLR) in 113 RA Patients
3.5. Relationship between Hematological Systemic Inflammatory Markers (NLR and PLR) and Disease Activity Parameters in EORA and YORA Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- MacGregor, A.J.; Silman, A.J. Rheumatoid arthritis: Classification and epidemiology. In Rheumatology, 2nd ed.; Klippel, J.H., Dieppe, P.A., Eds.; Mosby: London, UK, 1998; pp. 2.1–2.6. [Google Scholar]
- Targońska-Stępniak, B. Rheumatoid arthritis in elderly people. Wiad. Lek. 2019, 72, 1676–1682. [Google Scholar] [CrossRef]
- Soubrier, M.; Mathieu, S.; Payet, S.; Dubost, J.J.; Ristori, J.M. Elderly-onset rheumatoid arthritis. Joint Bone Spine 2010, 77, 290–296. [Google Scholar] [CrossRef]
- Kobak, S.; Bes, C. An autumn tale: Geriatric rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2018, 10, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Ruban, T.N.; Jacob, B.; Pope, J.E.; Keystone, E.C.; Bombardier, C.; Kuriya, B. The influence of age at disease onset on disease activity and disability: Results from the Ontario Best Practices Research Initiative. Clin. Rheumatol. 2016, 35, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Innala, L.; Berglin, E.; Möller, B.; Ljung, L.; Smedby, T.; Södergren, A.; Magnusson, S.; Rantapää-Dahlqvist, S.; Wållberg-Jonsson, S. Age at onset determines severity and choice of treatment in early rheumatoid arthritis: A prospective study. Arthritis Res. Ther. 2014, 16, R94. [Google Scholar] [CrossRef] [Green Version]
- Ohe, Y.; Fushida, S.; Yamaguchi, T.; Kinoshita, J.; Saito, H.; Okamoto, K.; Nakamura, K.; Tajima, H.; Ninomiya, I.; Ohta, T. Peripheral Blood Platelet-Lymphocyte Ratio Is Good Predictor of Chemosensitivity and Prognosis in Gastric Cancer Patients. Cancer Manag. Res. 2020, 12, 1303–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Shen, J.; Lu, Z.; Chen, M.; Fang, X.; Wang, G. High neutrophil-to-lymphocyte ratio is associated with increased carotid artery intima-media thickness in type 2 diabetes. J. Diabetes Investig. 2017, 8, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Cho, H.J.; Lee, H.Y.; Ki, Y.J.; Jeon, E.S.; Hwang, K.K.; Chae, S.C.; Baek, S.H.; Kang, S.M.; Choi, D.J.; et al. Neutrophil-Lymphocyte Ratio in Patients with Acute Heart Failure Predicts In-Hospital and Long-Term Mortality. J. Clin. Med. 2020, 9, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.; Zhang, Z.; Lin, F.; Ren, Y.; Liu, D.; Zhong, R.; Liang, Y. Comparisons of neutrophil-, monocyte-, eosinophil-, and basophil- lymphocyte ratios among various systemic autoimmune rheumatic diseases. APMIS 2017, 125, 863–871. [Google Scholar] [CrossRef]
- Targońska-Stępniak, B.; Zwolak, R.; Piotrowski, M.; Grzechnik, K.; Majdan, M. The Relationship between Hematological Markers of Systemic Inflammation (Neutrophil-To-Lymphocyte, Platelet-To-Lymphocyte, Lymphocyte-To-Monocyte Ratios) and Ultrasound Disease Activity Parameters in Patients with Rheumatoid Arthritis. J. Clin. Med. 2020, 9, 2760. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerek, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Prevoo, M.L.; van’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight-joint counts: Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar] [CrossRef] [Green Version]
- van der Heijde, D. How to read radiographs according to the Sharp/van der Heijde method. J. Rheumatol. 2000, 27, 261–263. [Google Scholar] [PubMed]
- Duru, N.; van der Goes, M.C.; Jacobs, J.W.; Andrews, T.; Boers, M.; Buttgereit, F.; Caeyers, N.; Cutolo, M.; Halliday, S.; Da Silva, J.A.; et al. EULAR evidence-based and consensus-based recommendations on the management of medium to high-dose glucocorticoid therapy in rheumatic diseases. Ann. Rheum. Dis. 2013, 72, 1905–1913. [Google Scholar] [CrossRef] [PubMed]
- Wongrakpanich, S.; Wongrakpanich, A.; Melhado, K.; Rangaswami, J. A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in the Elderly. Aging Dis. 2018, 9, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Radovits, B.J.; Kievit, W.; Fransen, J.; van de Laar, M.A.; Jansen, T.L.; van Riel, P.L.; Laan, R.F. Influence of age on the outcome of antitumour necrosis factor alpha therapy in rheumatoid arthritis. Ann. Rheum. Dis. 2009, 68, 1470–1473. [Google Scholar] [CrossRef] [PubMed]
- Montenont, E.; Rondina, M.T.; Campbell, R.A. Altered functions of platelets during aging. Curr. Opin. Hematol. 2019, 26, 336–342. [Google Scholar] [CrossRef]
- Biino, G.; Santimone, I.; Minelli, C.; Sorice, R.; Frongia, B.; Traglia, M.; Ulivi, S.; Di Castelnuovo, A.; Gögele, M.; Nutile, T.; et al. Age- and sex-related variations in platelet count in Italy: A proposal of reference ranges based on 40987 subjects’ data. PLoS ONE 2013, 8, e54289. [Google Scholar]
- Rundberg Nilsson, A.; Soneji, S.; Adolfsson, S.; Bryder, D.; Pronk, C.J. Human and Murine Hematopoietic Stem Cell Aging Is Associated with Functional Impairments and Intrinsic Megakaryocytic/Erythroid Bias. PLoS ONE 2016, 11, e0158369. [Google Scholar] [CrossRef] [Green Version]
- Liaw, F.-Y.; Huang, C.-F.; Chen, W.L.; Wu, L.W.; Peng, T.C.; Chang, Y.-W.; Kao, T.-W. Higher Platelet-to-Lymphocyte Ratio Increased the Risk of Sarcopenia in the Community-Dwelling Older Adults. Sci. Rep. 2017, 7, 16609. [Google Scholar] [CrossRef] [Green Version]
- Fang, T.; Wang, Y.; Yin, X.; Zhai, Z.; Zhang, Y.; Yang, Y.; You, Q.; Li, Z.; Ma, Y.; Li, C.; et al. Diagnostic Sensitivity of NLR and PLR in Early Diagnosis of Gastric Cancer. J. Immunol. Res. 2020, 2020, 9146042. [Google Scholar] [CrossRef] [PubMed]
- Ye, G.L.; Chen, Q.; Chen, X.; Liu, Y.Y.; Yin, T.T.; Meng, Q.H.; Liu, Y.C.; Wei, H.Q.; Zhou, Q.H. The prognostic role of platelet-to-lymphocyte ratio in patients with acute heart failure: A cohort study. Sci. Rep. 2019, 9, 10639. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Fu, Y.; Gao, Y.; Zhang, Q. Platelet-to-lymphocyte ratio predicts long-term survival in laryngeal cancer. Eur. Arch. Otorhinolaryngol. 2018, 275, 553–559. [Google Scholar] [CrossRef]
- Boulos, D.; Proudman, S.M.; Metcalf, R.G.; McWilliams, L.; Hall, C.; Wicks, I.P. The neutrophil-lymphocyte ratio in early rheumatoid arthritis and its ability to predict subsequent failure of triple therapy. Semin. Arthritis Rheum. 2019, 49, 373–376. [Google Scholar] [CrossRef]
- Sargin, G.; Senturk, T.; Yavasoglu, I.; Kose, R. Relationship between neutrophil-lymphocyte, platelet-lymphocyte ratio and disease activity in rheumatoid arthritis treated with rituximab. Int. J. Rheum. Dis. 2018, 21, 2122–2127. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekara, S.; Mukhtar Ahmad, M.; Renuka, P.; Anupama, K.R.; Renuka, K. Characterization of neutrophil-to-lymphocyte ratio as a measure of inflammation in rheumatoid arthritis. Int. J. Rheum. Dis. 2017, 20, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.D. Red blood cell distribution width: A promising index for estimating activity of autoimmune disease. J. Lab. Precis. Med. 2016, 1, 4. [Google Scholar] [CrossRef]
- Lin, F.; Wang, X.; Liang, Y.; Liu, D.; Zhang, Y.; Zhong, R.; Yang, Z. Red Blood Cell Distribution Width in Rheumatoid Arthritis, Ankylosing Spondylitis and Osteoarthritis: True Inflammatory Index or Effect of Anemia? Ann. Clin. Lab. Sci. 2018, 48, 301–307. [Google Scholar] [PubMed]


{kind=link}
| Data | YORA (n = 50) | EORA (n = 63) | p-Value |
|---|---|---|---|
| Age, years | 41.5 (±13.7) | 73.6 (±6.6) | <0.001 |
| Gender, female/male (n,%) | 46 (92.0)/ 4 (8.0) | 47 (74.6)/ 16 (25.4) | 0.02 |
| Body mass index (BMI), kg/m2 | 23.4 (±4.1) | 26.0 (±5.8) | 0.04 |
| Concomitant diseases (n,%) | 40 (80.0) | 61 (96.8) | 0.004 |
| Rheumatoid Arthritis (RA)-Related Variables: | |||
| Disease duration, years | 18.3 (±12.3) | 8.6 (±5.4) | <0.001 |
| Age at RA diagnosis, years | 24 (20–27) | 64 (62–67) | <0.001 |
| Joint involvement at RA onset (n,%) | |||
| small hand joints | 43 (86) | 54 (85.7) | |
| wrist | 36 (72) | 44 (69.8) | |
| elbow | 18 (36) | 16 (25.4) | NS |
| shoulder | 19 (38) | 29 (46) | |
| small joints of feet | 21 (42) | 18 (28.6) | |
| ankle | 14 (28) | 13 (20.6) | |
| knee | 31 (62) | 40 (63.5) | |
| hip | 2 (4) | 8 (12.7) | |
| Positive RF-IgM (n,%) | 42 (84.0) | 57 (90.5) | NS |
| Positive anti-CCP (n,%) | 43 (86.0) | 57 (90.5) | NS |
| Positive both (RF-IgM, anti-CCP) (n,%) | 39 (78.0) | 54 (90.0) | NS |
| Seronegative (n,%) | 4 (8.0) | 1 (1.6) | NS |
| Extra-articular manifestations (n,%) | 18 (36.0) | 15 (23.8) | NS |
| Erosions (hands/feet) (n,%) | 48 (96.0) | 57 (90.5) | NS |
| First drug used (n,%) | |||
| NSAID | 20 (40.0) | 38 (60.3) | 0.03 |
| GC | 11 (22.0) | 6 (9.5) | NS |
| DMARD | 19 (38) | 19 (30.2) | NS |
| First DMARD used (n,%) | |||
| MTX | 26 (52) | 54 (85.7) | <0.001 |
| Anti-malarial drug | 6 (12) | 6 (9.5) | NS |
| Sulphalazin | 11 (22.0) | 3 (4.8) | 0.01 |
| Other | 7 (14.0) | 0 | 0.002 |
| Current biological treatment (n,%) | 34 (68.0) | 6 (9.5) | <0.001 |
| Anti-TNF | 23 (46.0) | 5 (7.9) | <0.001 |
| Other | 11 (22.0) | 1 (1.6) | <0.001 |
| Current low dose glucocorticoid use (n,%) | 47 (94.0) | 49 (77.8) | 0.02 |
| Data | All RA patients (n = 113) | YORA (n = 50) | EORA (n = 63) | p-Value (YORA vs. EORA) |
|---|---|---|---|---|
| Laboratory Results: | ||||
| Hemoglobin, g/dL | 12.5 (±1.3) | 12.5 (±1.3) | 12.4 (±1.3) | NS |
| PLT,109/L | 306.0 (±98.8) | 310.3 (±86.5) | 302.7 (±107.8) | NS |
| WBC, 109/L | 7.7 (±2.7) | 7.0 (±2.4) | 8.3 (±2.7) | 0.01 |
| ANC, 109/L | 5.7 (±3.3) | 4.8 (±2.1) | 6.3 (±3.8) | 0.02 |
| ALC, 109/L | 1.6 (±0.8) | 1.5 (±0.6) | 1.7 (±0.9) | NS |
| NLR | 3.06 (2.4–5.2) | 3.0 (2.1–4.8) | 3.1 (2.3–5.6) | NS |
| PLR | 187.9 (138.7–265.2) | 216.8 (161.6–282.0) | 169.1 (129.6–258.4) | 0.03 |
| CRP, mg/L | 10.8 (2.8–29.7) | 7.2 (1.3–16.8) | 16.0 (5.3–32.0) | 0.02 |
| ESR, mm/h | 26 (12–58) | 15 (5–29) | 39.5 (18.5–70) | <0.001 |
| Creatinine, mg/dL | 0.8 (0.6–0.9) | 0.7 (0.6–0.8) | 0.9 (0.7–1.0) | <0.001 |
| Uric acid, mg/dL | 5.3 (±1.6) | 4.4 (±1.6) | 5.7 (±1.5) | 0.001 |
| Clinical Parameters of RA Activity: | ||||
| TJC | 3 (1–7) | 2 (0–4) | 4 (1–10) | 0.01 |
| SJC | 1 (0–4) | 1 (0–4) | 2 (0–5) | NS |
| PGA (VAS), mm | 34.9 (±25.6) | 29.4 (±27.3) | 39.1 (±23.6) | NS |
| Morning stiffness, minutes | 75.0 (±57.6) | 51.5 (±58.8) | 83.5 (±55.8) | NS |
| DAS28 | 3.9 (±1.7) | 3.2 (±1.6) | 4.4 (±1.5) | <0.001 |
| Remission or Low Disease Activity (DAS28 < 3.2) (n, %) | 40 (35.4) | 25 (50.0) | 15 (23.8) | 0.004 |
| Data/R Spearman | Age | Age at RA Onset | Disease Duration | NLR | PLR |
|---|---|---|---|---|---|
| CRP | 0.31 *** | 0.23 ** | NS | 0.58 *** | 0.44 *** |
| ESR | 0.4 *** | 0.37 *** | NS | 0.39 *** | 0.36 *** |
| DAS28 | 0.39 *** | 0.33 *** | NS | 0.53 *** | 0.3 *** |
| PGA (VAS) | 0.32 *** | 0.23 ** | NS | 0.46 *** | 0.24 ** |
| TJC | NS | NS | NS | 0.39 *** | 0.25 ** |
| SJC | NS | NS | NS | 0.4 *** | 0.35 *** |
| PLR | NS | −0.2 * | NS | 0.67 *** | - |
| NLR | NS | NS | NS | - | 0.67 *** |
| WBC | NS | NS | 0.25 ** | 0.45 *** | NS |
| ANC | NS | 0.19 * | 0.23 ** | 0.72 *** | 0.22 ** |
| ALC | NS | NS | Ns | −0.52 *** | −0.69 *** |
| PLT | NS | NS | NS | 0.34 *** | 0.54 *** |
| Hb | NS | NS | NS | NS | −0.24 ** |
| Creatinine | 0.37 *** | 0.36 *** | NS | NS | NS |
| Uric acid | 0.37 *** | 0.35 *** | NS | NS | NS |
| BMI | 0.25 ** | 0.27 ** | NS | NS | NS |
| Data R Spearman | PLR | NLR | ||
|---|---|---|---|---|
| YORA | EORA | YORA | EORA | |
| CRP | 0.35 * | 0.61 *** | 0.5 *** | 0.63 *** |
| ESR | 0.41 *** | 0.35 *** | 0.35 ** | 0.44 *** |
| Hb | −0.3 * | NS | NS | NS |
| PLT | 0.5 *** | 0.52 *** | 0.46 *** | 0.31 ** |
| WBC | NS | NS | 0.42 *** | 0.48 *** |
| ANC | 0.21 ** | 0.25 *** | 0.67 *** | 0.76 *** |
| ALC | −0.81 *** | −0.61 *** | −0.52 *** | −0.57 *** |
| TJC | 0.33 * | 0.27 * | 0.47 *** | 0.34 *** |
| SJC | NS | 0.45 *** | NS | 0.49 *** |
| PGA (VAS) | 0.24 *** | 0.36 ** | 0.43 *** | 0.43 *** |
| DAS28 | 0.42 *** | 0.35 *** | 0.57 *** | 0.54 *** |
| Morning stiffness | NS | 0.5 *** | NS | 0.56 *** |
| NLR | 0.7 *** | 0.7 *** | - | - |
| PLR | - | - | 0.7 *** | 0.7 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Targońska-Stępniak, B.; Grzechnik, K.; Kolarz, K.; Gągoł, D.; Majdan, M. Systemic Inflammatory Parameters in Patients with Elderly-Onset Rheumatoid Arthritis (EORA) and Young-Onset Rheumatoid Arthritis (YORA)—An Observational Study. J. Clin. Med. 2021, 10, 1204. https://doi.org/10.3390/jcm10061204
Targońska-Stępniak B, Grzechnik K, Kolarz K, Gągoł D, Majdan M. Systemic Inflammatory Parameters in Patients with Elderly-Onset Rheumatoid Arthritis (EORA) and Young-Onset Rheumatoid Arthritis (YORA)—An Observational Study. Journal of Clinical Medicine. 2021; 10(6):1204. https://doi.org/10.3390/jcm10061204
Chicago/Turabian StyleTargońska-Stępniak, Bożena, Krzysztof Grzechnik, Katarzyna Kolarz, Danuta Gągoł, and Maria Majdan. 2021. "Systemic Inflammatory Parameters in Patients with Elderly-Onset Rheumatoid Arthritis (EORA) and Young-Onset Rheumatoid Arthritis (YORA)—An Observational Study" Journal of Clinical Medicine 10, no. 6: 1204. https://doi.org/10.3390/jcm10061204