
The Effect of Discharge Mode on the Distribution of Myocardial Pulsed Electric Field—A Simulation Study for Pulsed Field Ablation of Atrial Fibrillation


Abstract
:1. Introduction
2. Methods
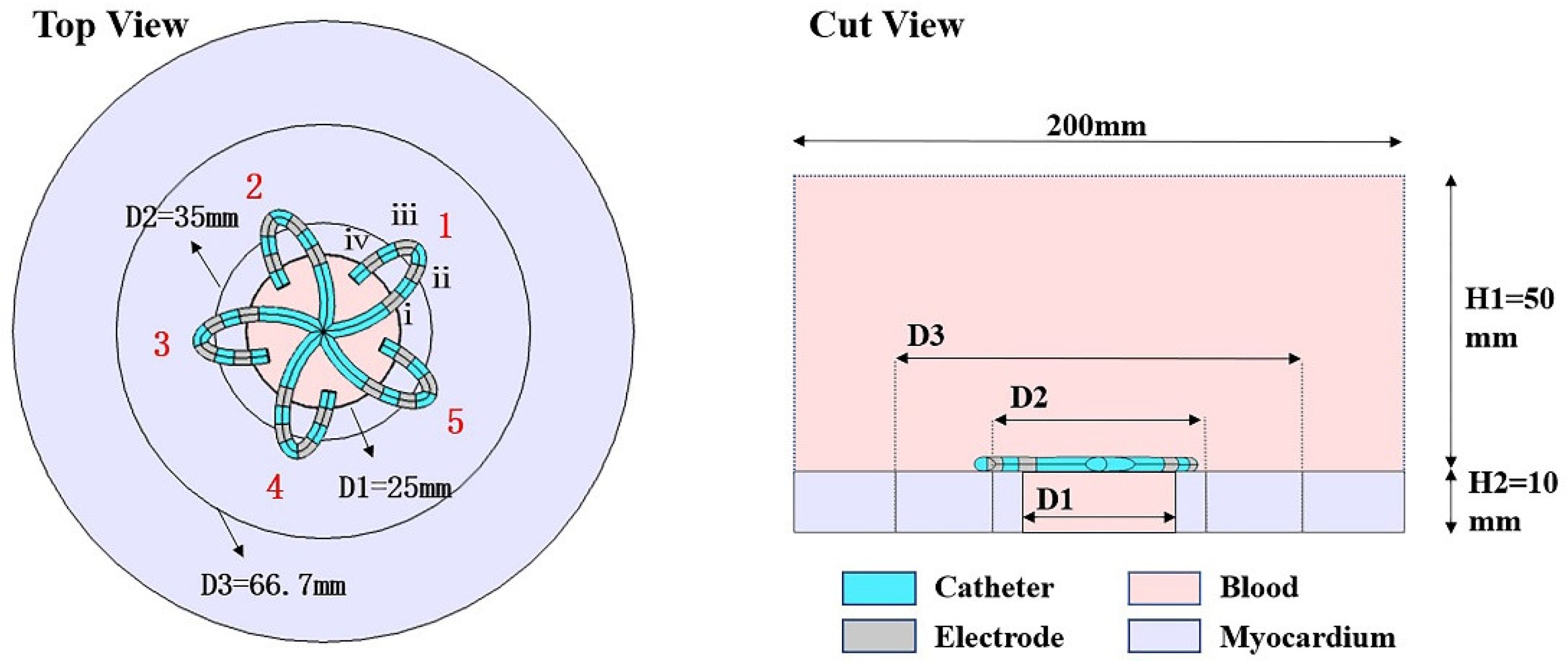
2.1. Construction of the Finite Element Model of Myocardial PFA
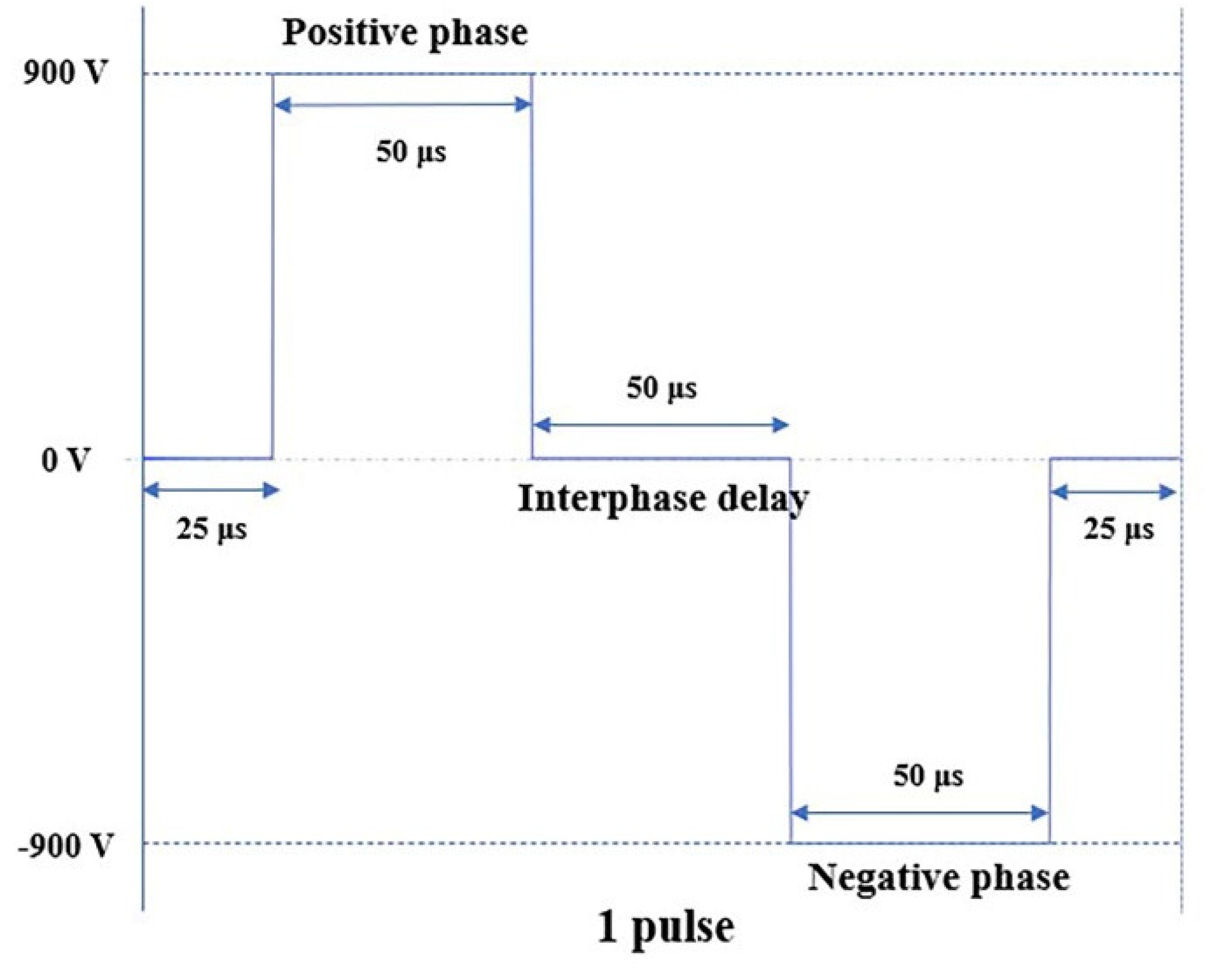
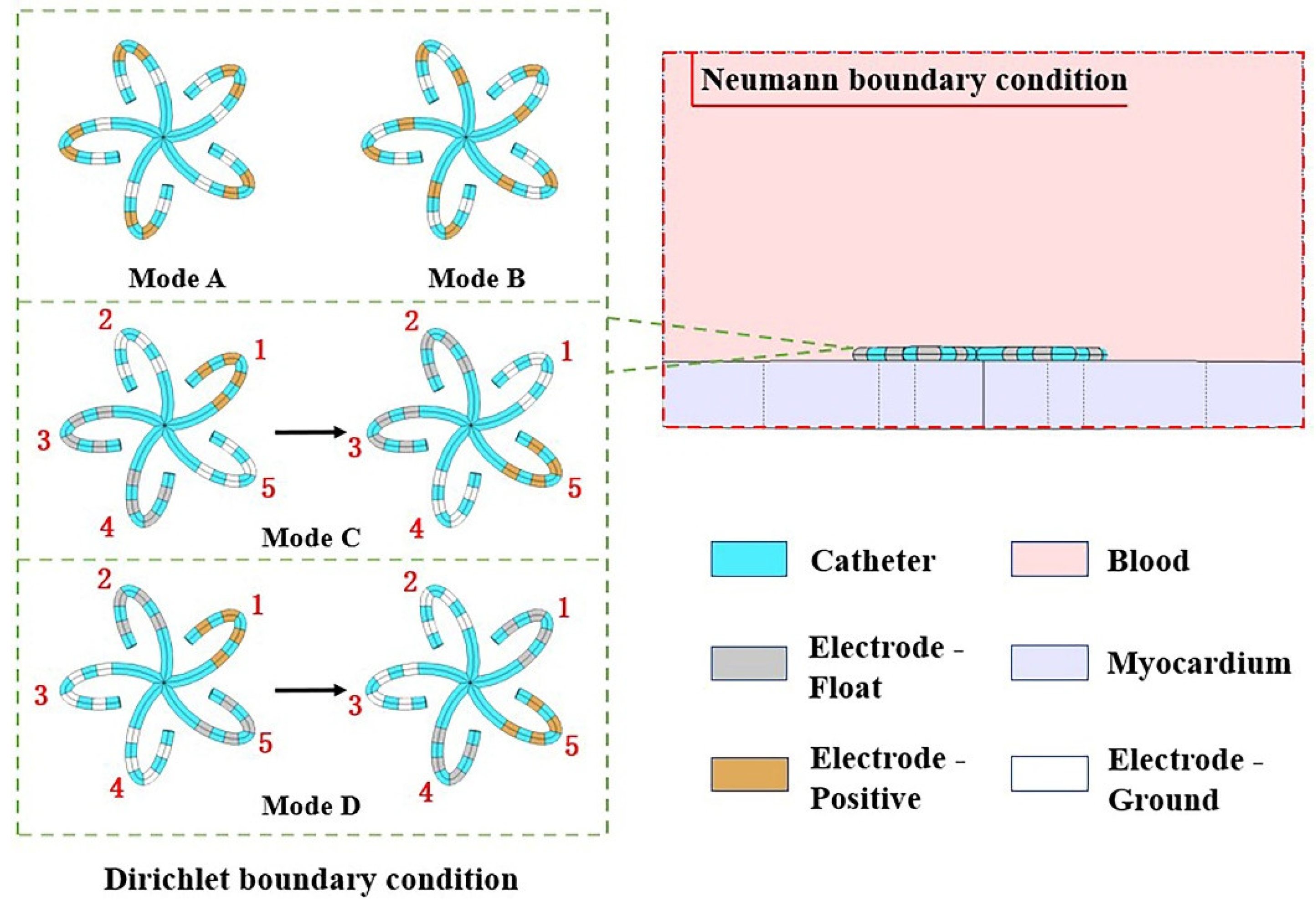
2.2. Simulation
3. Results
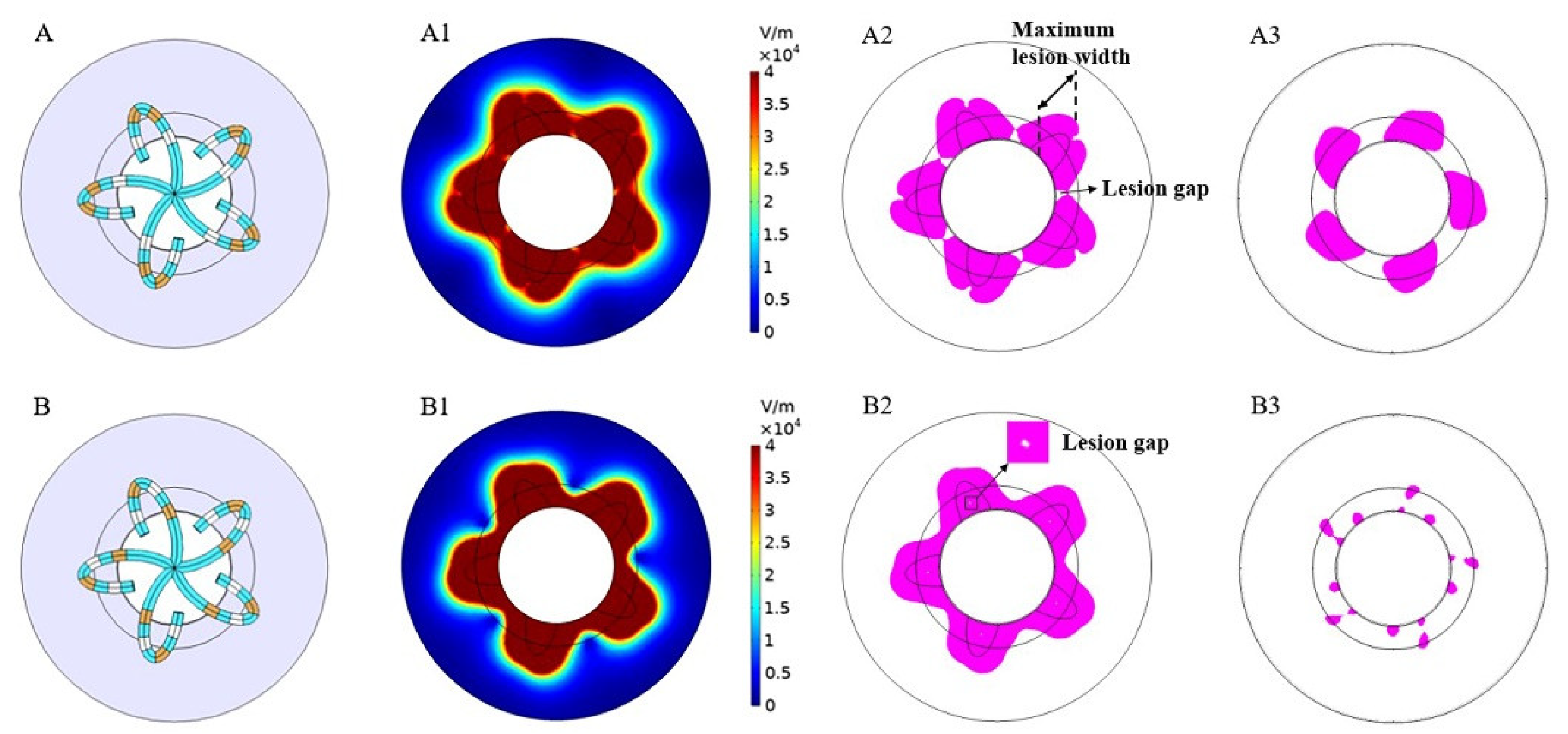
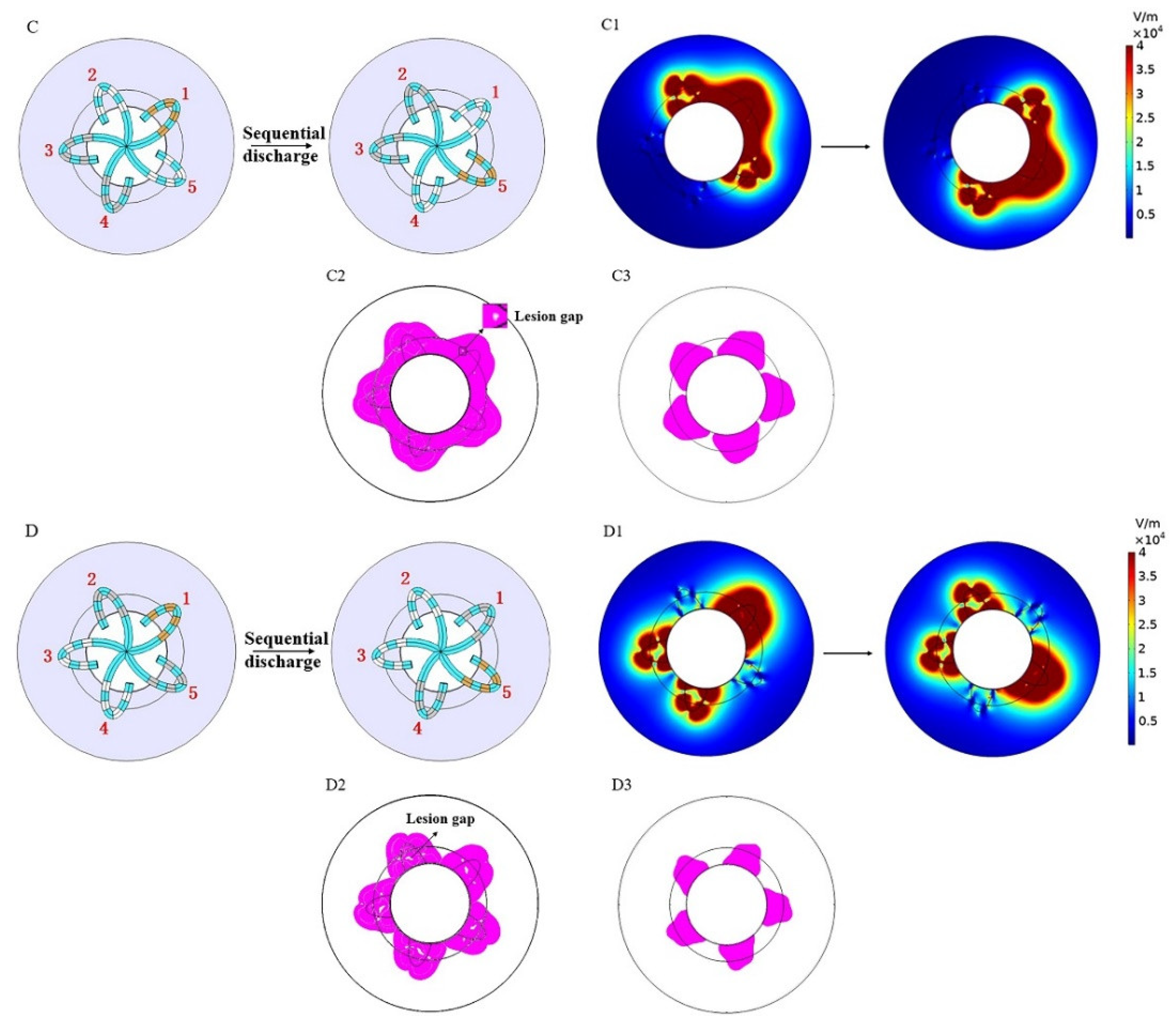
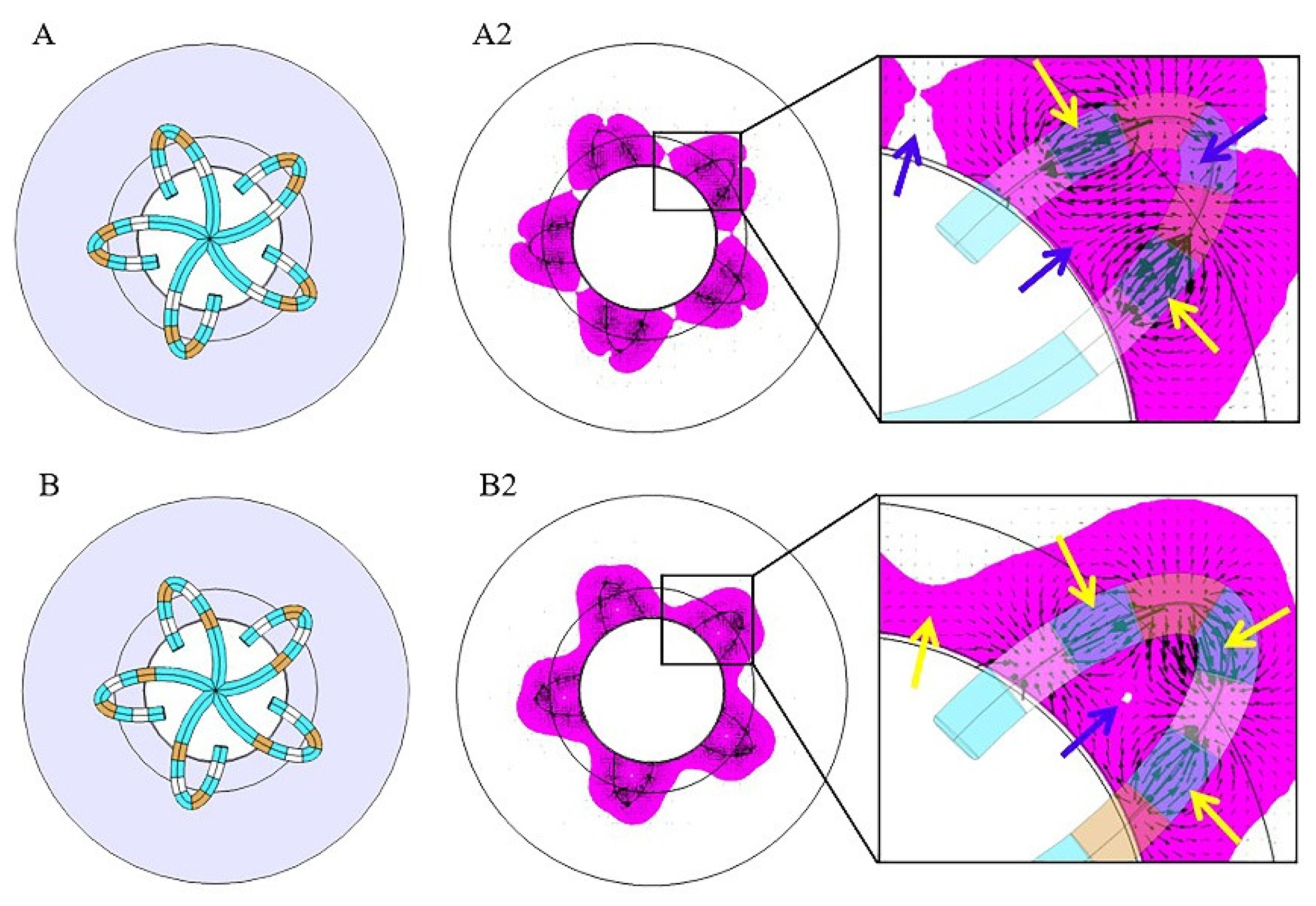
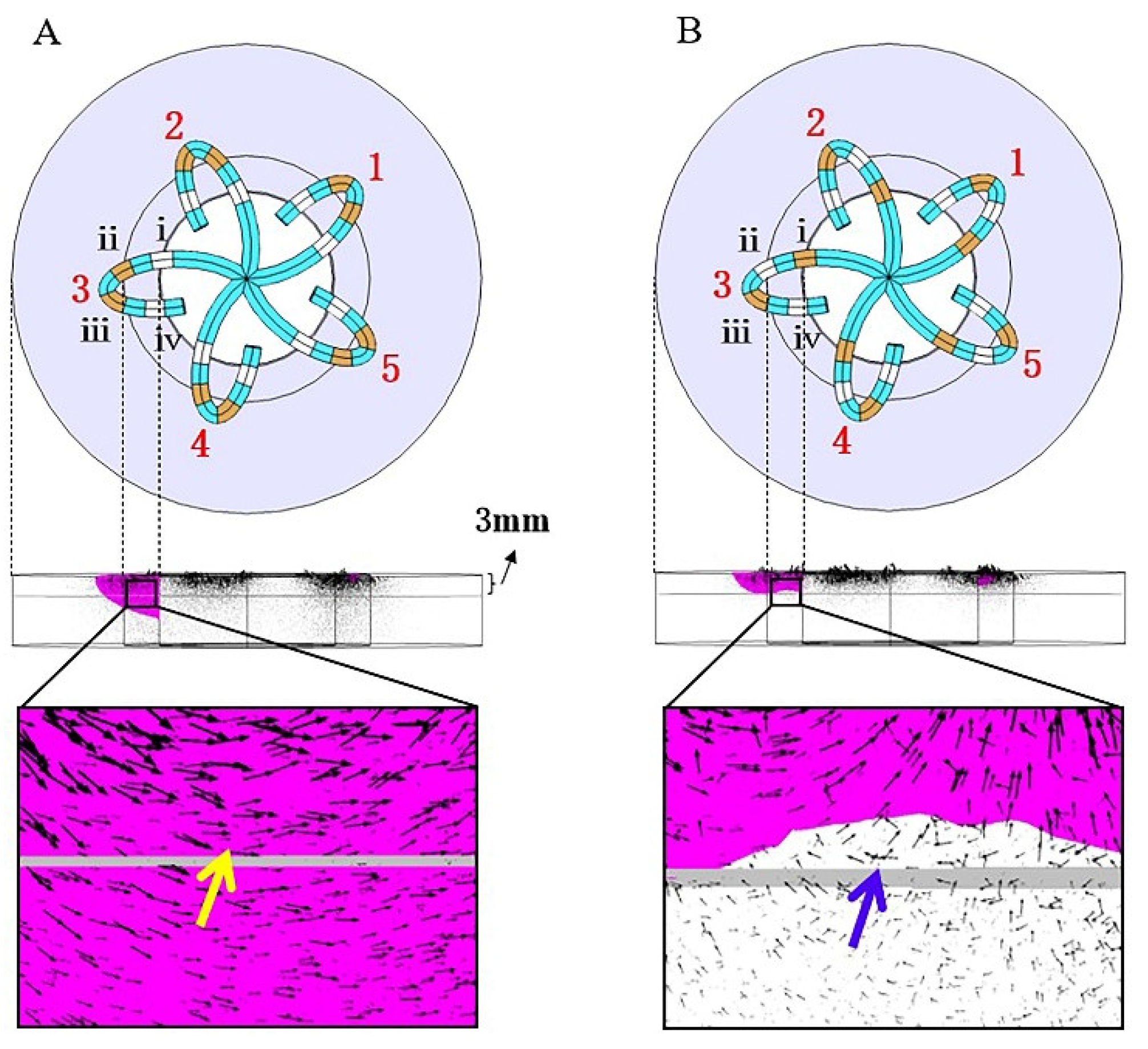
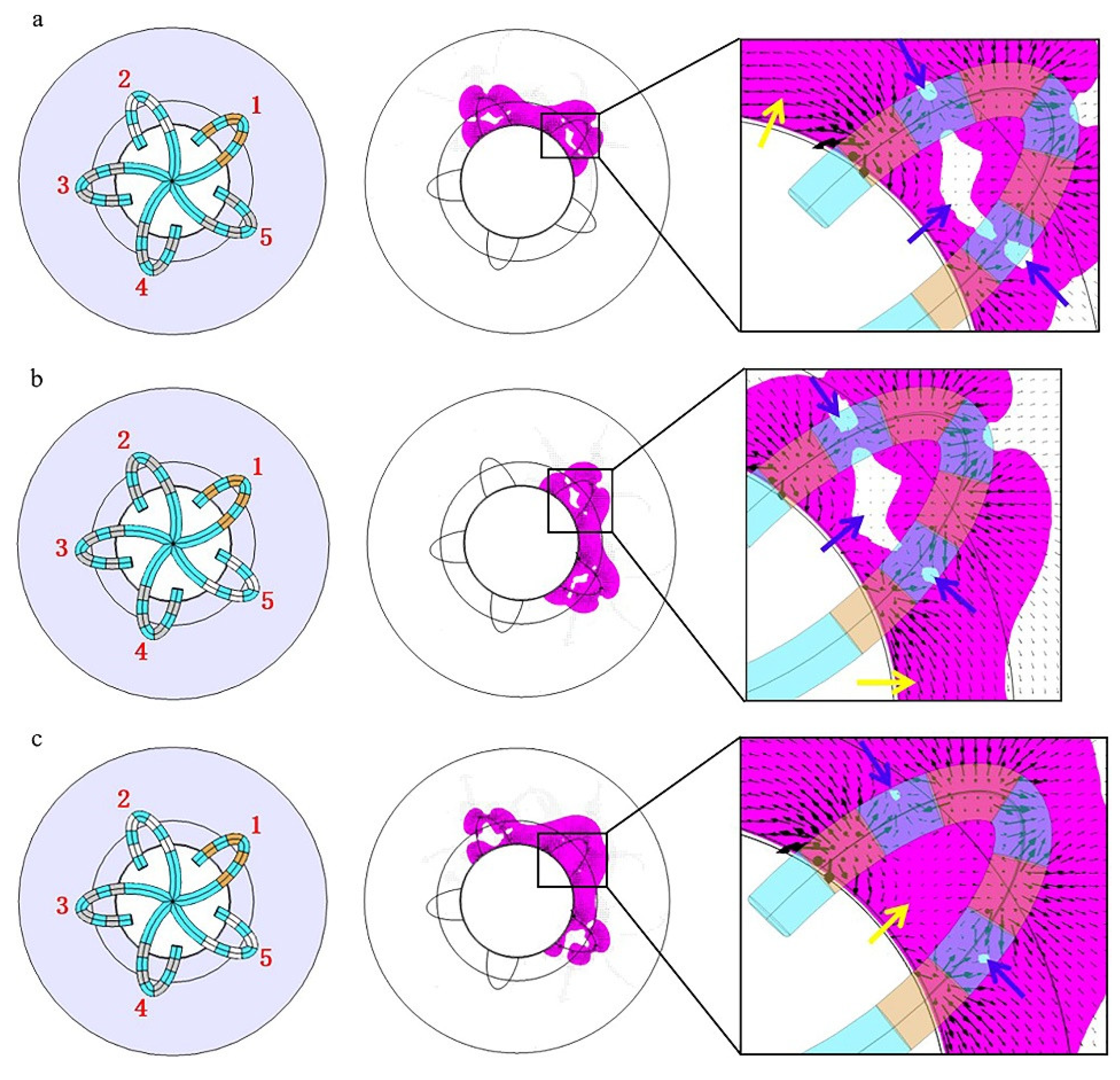
3.1. Electric Field Distribution without Catheter Rotation
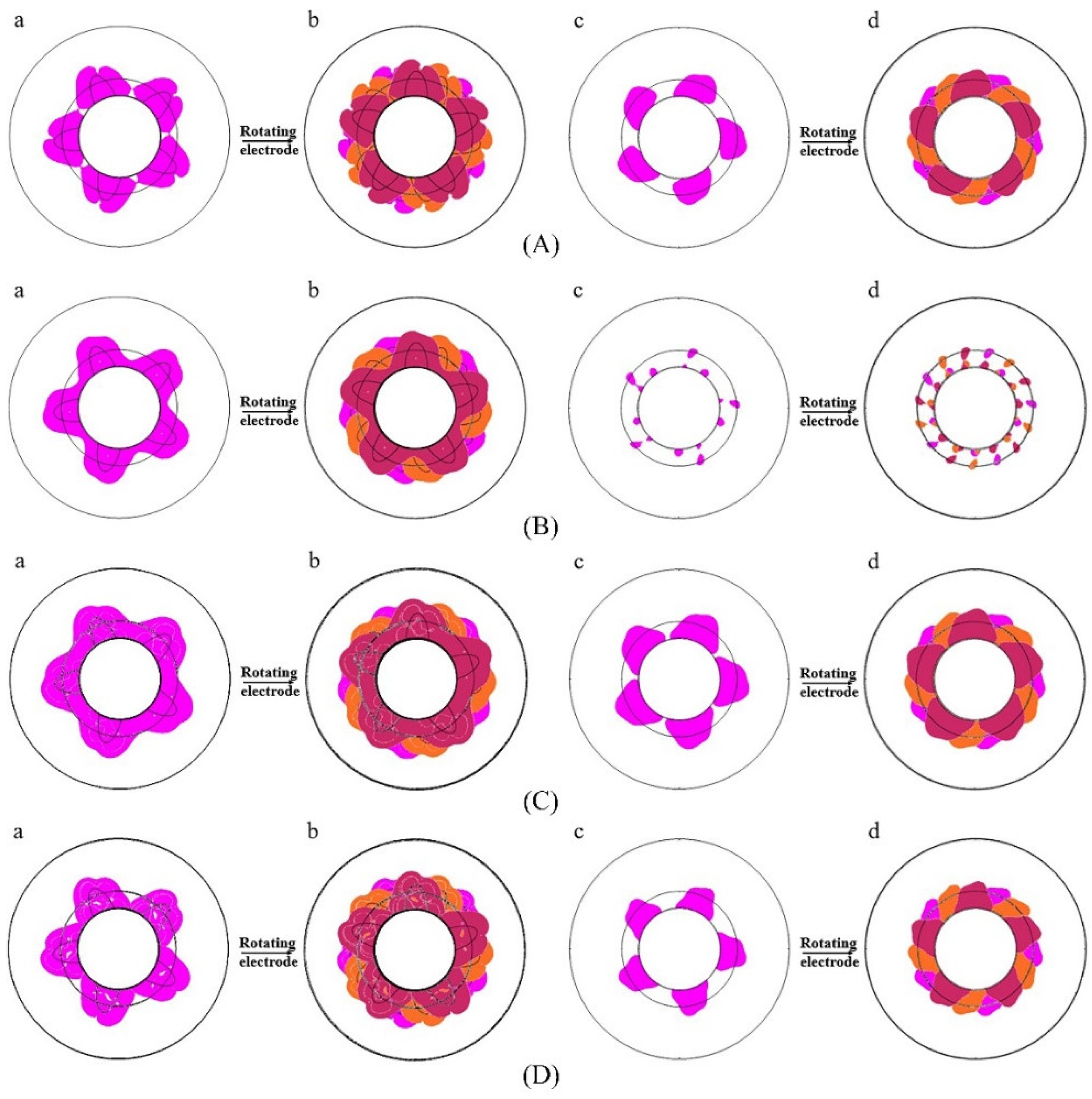
3.2. Electric Field Distribution with Catheter Rotation
4. Discussion
4.1. Influencing Factors of Electric Field Distribution in the Myocardium
4.2. Inspirations for the Clinical Application of PFA
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gleason, K.T.; Dennison Himmelfarb, C.R.; Ford, D.E.; Lehmann, H.; Samuel, L.; Han, H.R.; Jain, S.K.; Naccarelli, G.V.; Aggarwal, V.; Nazarian, S. Association of sex, age and education level with patient reported outcomes in atrial fibrillation. BMC Cardiovasc. Disord. 2019, 19, 85. [Google Scholar] [CrossRef] [Green Version]
- Morillo, C.A.; Banerjee, A.; Perel, P.; Wood, D.; Jouven, X. Atrial fibrillation: The current epidemic. J. Geriatr. Cardiol. 2017, 14, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kim, Y.; Oh, G.; Kim, S.H.; Choi, Y.; Hwang, Y.; Kim, T.-S.; Kim, S.-H.; Kim, J.-H.; Jang, S.-W.; et al. A deep learning model to predict recurrence of atrial fibrillation after pulmonary vein isolation. Int. J. Arrhythmia 2020, 21, 19. [Google Scholar]
- Bhardwaj, R.; Koruth, J.S. Novel ablation approaches for challenging atrial fibrillation cases (mapping, irrigation, and catheters). Cardiol. Clin. 2019, 37, 207–219. [Google Scholar] [CrossRef]
- Howard, B.; Haines, D.E.; Verma, A.; Packer, D.; Kirchhof, N.; Barka, N.; Onal, B.; Fraasch, S.; Miklavčič, D.; Stewart, M.T. Reduction in pulmonary vein stenosis and collateral damage with pulsed field ablation compared with radiofrequency ablation in a canine model. Circ. Arrhythmia Electrophysiol. 2020, 13, e008337. [Google Scholar]
- Koruth, J.S.; Kuroki, K.; Kawamura, I.; Brose, R.; Viswanathan, R.; Buck, E.D.; Donskoy, E.; Neuzil, P.; Dukkipati, S.R.; Reddy, V.Y. Pulsed field ablation versus radiofrequency ablation: Esophageal injury in a novel porcine model. Circ. Arrhythmia Electrophysiol. 2020, 13, e008303. [Google Scholar]
- Loh, P.; van Es, R.; Groen, M.H.A.; Neven, K.; Kassenberg, W.; Wittkampf, F.H.; Doevendans, P.A. Pulmonary vein isolation with single pulse irreversible electroporation: A first in human study in 10 patients with atrial fibrillation. Circ. Arrhythmia Electrophysiol. 2020, 13, e008192. [Google Scholar]
- Zimmermann, U.; Friedrich, U.; Mussauer, H.; Gessner, P.; Hamel, K.; Sukhorukov, V. Electromanipulation of mammalian cells: Fundamentals and application. IEEE Trans. Plasma Sci. 2000, 28, 72–82. [Google Scholar] [CrossRef]
- Zupanic, A.; Kos, B.; Miklavcic, D. Treatment planning of electroporation-based medical interventions: Electrochemotherapy, gene electrotransfer and irreversible electroporation. Phys. Med. Biol. 2012, 57, 5425–5440. [Google Scholar]
- Lindemann, F.; Nedios, S.; Seewöster, T.; Hindricks, G. Pulmonalvenenisolation bei vorhofflimmern mittels „pulsed field ablation“. Herz 2021, 46, 318–322. [Google Scholar]
- Vižintin, A.; Vidmar, J.; Ščančar, J.; Miklavčič, D. Effect of interphase and interpulse delay in high-frequency irreversible electroporation pulses on cell survival, membrane permeabilization and electrode material release. Bioelectrochemistry 2020, 134, 107523. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, I.A.; Latouche, E.L.; DeWitt, M.R.; Swet, J.H.; Kirks, R.C.; Baker, E.H.; Iannitti, D.A.; Vrochides, D.; Davalos, R.V.; McKillop, I.H. Induction of rapid, reproducible hepatic ablations using next-generation, high frequency irreversible electroporation (H-FIRE) in vivo. Hpb 2016, 18, 726–734. [Google Scholar] [PubMed] [Green Version]
- Hogenes, A.M.; Slump, C.H.; Te Riet, O.G.; Scholten, G.A.; Meijerink, M.R.; Fütterer, J.J.; van Laarhoven, C.J.H.M.; Overduin, C.G.; Stommel, M.W.J. Effect of irreversible electroporation parameters and the presence of a metal stent on the electric field line pattern. Sci. Rep. 2020, 10, 13517. [Google Scholar] [PubMed]
- Zhao, D.Y.; Li, C.X.; Yan, M.; Chen-guo, Y. The optimal design of electrod array using electroporation based on the finite element. In Proceedings of the 2008 International Conference on High Voltage Engineering and Application, Chongqing, China, 9–12 November 2008; pp. 773–776. [Google Scholar]
- Stewart, M.T.; Haines, D.E.; Verma, A.; Kirchhof, N.; Barka, N.; Grassl, E.; Howard, B. Intracardiac pulsed field ablation: Proof of feasibility in a chronic porcine model. Heart Rhythm 2019, 16, 754–764. [Google Scholar] [CrossRef] [Green Version]
- Yavin, H.; Brem, E.; Zilberman, I.; Shapira-Daniels, A.; Datta, K.; Govari, A.; Altmann, A.; Anic, A.; Wazni, O.; Anter, E. Circular multielectrode pulsed field ablation catheter lasso pulsed field ablation: Lesion characteristics, durability, and effect on neighboring structures. Circ. Arrhythmia Electrophysiol. 2021, 14, e009229. [Google Scholar]
- Reddy, V.Y.; Neuzil, P.; Koruth, J.S.; Petru, J.; Funosako, M.; Cochet, H.; Sediva, L.; Chovanec, M.; Dukkipati, S.R.; Jais, P. Pulsed field ablation for pulmonary vein isolation in atrial fibrillation. J. Am. Coll. Cardiol. 2019, 74, 315–326. [Google Scholar] [CrossRef]
- Guo, F.; Deng, H.; Qian, K.; Li, X. Characterization of dispersion and anisotropic-conductivity in tissue model during electroporation pulses. Bioelectrochemistry 2022, 144, 108029. [Google Scholar]
- Merola, G.; Fusco, R.; Di Bernardo, E.; D’Alessio, V.; Izzo, F.; Granata, V.; Contartese, D.; Cadossi, M.; Audenino, A.; Gallo, G.P. Design and characterization of a minimally invasive bipolar electrode for electroporation. Biology 2020, 9, 303. [Google Scholar]
- Mercadal, B.; Arena, C.B.; Davalos, R.V.; Ivorra, A. Avoiding nerve stimulation in irreversible electroporation: A numerical modeling study. Phys. Med. Biol. 2017, 62, 8060–8079. [Google Scholar] [CrossRef] [Green Version]
- Reddy, V.Y.; Anic, A.; Koruth, J.; Petru, J.; Funasako, M.; Minami, K.; Breskovic, T.; Sikiric, I.; Dukkipati, S.R.; Kawamura, I. Pulsed field ablation in patients with persistent atrial fibrillation. J. Am. Coll. Cardiol. 2020, 76, 1068–1080. [Google Scholar] [CrossRef]
- Ramirez, F.D.; Reddy, V.Y.; Viswanathan, R.; Hocini, M.; Jaïs, P. Emerging technologies for pulmonary vein isolation. Circ. Res. 2020, 127, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Platonov, P.G.; Ivanov, V.; Yen, H.S.; Mitrofanova, L. Left atrial posterior wall thickness in patients with and without atrial fibrillation: Data from 298 consecutive autopsies. J. Cardiovasc. Electrophysiol. 2008, 19, 689–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varela, M.; Morgan, R.; Theron, A.; Dillon-Murphy, D.; Chubb, H.; Whitaker, J.; Henning, M.; Aljabar, P.; Schaeffter, T.; Kolbitsch, C.; et al. Novel MRI technique enables non-invasive measurement of atrial wall thickness. IEEE Trans. Med. Imaging 2017, 36, 1607–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güler, E.; Güler, G.B.; Demir, G.G.; Kizilirmak, F.; Güneş, H.M.; Barutçu, I.; Kiliçaslan, F. Effect of pulmonary vein anatomy and pulmonary vein diameters on outcome of cryoballoon catheter ablation for atrial fibrillation. Pacing Clin. Electrophysiol. 2015, 38, 989–996. [Google Scholar] [CrossRef]
- Tada, H.; Kurosaki, K.; Ito, S.; Naito, S.; Yamada, M.; Miyaji, K.; Hashimoto, T.; Yoshimura, Y.; Nogami, A.; Oshima, S.; et al. Left atrial and pulmonary vein ostial ablation as a new treatment for curing persistent atrial fibrillation. Circ. J. 2005, 69, 1057–1063. [Google Scholar] [CrossRef] [Green Version]
- Davalos, R.V.; Mir, L.M.; Rubinsky, B. Tissue ablation with irreversible electroporation. Ann. Biomed. Eng. 2005, 33, 223–231. [Google Scholar] [CrossRef]
- Bhonsle, S.P.; Arena, C.B.; Sweeney, D.C.; Davalos, R.V. Mitigation of impedance changes due to electroporation therapy using bursts of high-frequency bipolar pulses. Biomed. Eng. Online 2015, 14 (Suppl. S3), 1–14. [Google Scholar] [CrossRef] [Green Version]
- Reddy, V.Y.; Dukkipati, S.R.; Neuzil, P.; Anic, A.; Petru, J.; Funasako, M.; Cochet, H.; Minami, K.; Breskovic, T.; Sikiric, I.; et al. Pulsed field ablation of paroxysmal atrial fibrillation: 1-year outcomes of IMPULSE, PEFCAT, and PEFCAT II. JACC. Clin. Electrophysiol. 2021, 7, 614–627. [Google Scholar]
- Viswanathan, R.; Long, G.; Pageard, J.L. Systems, Devices, and Methods for Delivery of Pulsed Electric Field Ablative Energy to Endocardial Tissue. U.S. Patent 10433908B2, 10 August 2019. [Google Scholar]
- Hasgall, P.A.; Di Gennaro, F.; Baumgartner, C.; Neufeld, E.; Lloyd, B.; Gosselin, M.C.; Payne, D.; Klingenböck, A.; Kuster, N. IT’IS Database for Thermal and Electromagnetic Parameters of Biological Tissues; Version 4.0; IT’IS Foundation: Zurich, Switzerland, 15 May 2018. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Myocardium | Blood | Electrode Pt | Catheter |
|---|---|---|---|---|
| Conductivity σ (s/m) | 0.137 | 0.70 | ||
| Relative permittivity | 5250 | 1 | 1 |
| Discharge Modes | Maximum Lesion Width on the Myocardial Surface (mm) | Maximum Continuous Circumferential Lesion Depth (mm) | Maximum Lesion Depth (mm) |
|---|---|---|---|
| A | 10.8 | 0 | 6.1 |
| B | 10.6 | 1.6 | 3.2 |
| C | 11.8 | 2.7 | 5.1 |
| D | 11.5 | 0.7 | 4.3 |
| Discharge Mode | Maximum Continuous Circumferential Lesion Depth (mm) |
|---|---|
| A | 5.2 |
| B | 2.7 |
| C | 4.7 |
| D | 4.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, X.; Zhang, H.; Zang, L.; Yan, S.; Wu, X. The Effect of Discharge Mode on the Distribution of Myocardial Pulsed Electric Field—A Simulation Study for Pulsed Field Ablation of Atrial Fibrillation. J. Cardiovasc. Dev. Dis. 2022, 9, 95. https://doi.org/10.3390/jcdd9040095
Ji X, Zhang H, Zang L, Yan S, Wu X. The Effect of Discharge Mode on the Distribution of Myocardial Pulsed Electric Field—A Simulation Study for Pulsed Field Ablation of Atrial Fibrillation. Journal of Cardiovascular Development and Disease. 2022; 9(4):95. https://doi.org/10.3390/jcdd9040095
Chicago/Turabian StyleJi, Xingkai, Hao Zhang, Lianru Zang, Shengjie Yan, and Xiaomei Wu. 2022. "The Effect of Discharge Mode on the Distribution of Myocardial Pulsed Electric Field—A Simulation Study for Pulsed Field Ablation of Atrial Fibrillation" Journal of Cardiovascular Development and Disease 9, no. 4: 95. https://doi.org/10.3390/jcdd9040095