
Immunohistochemical Evaluation of Periodontal Regeneration Using a Porous Collagen Scaffold

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Immunohistochemistry
2.1.1. Negative Controls
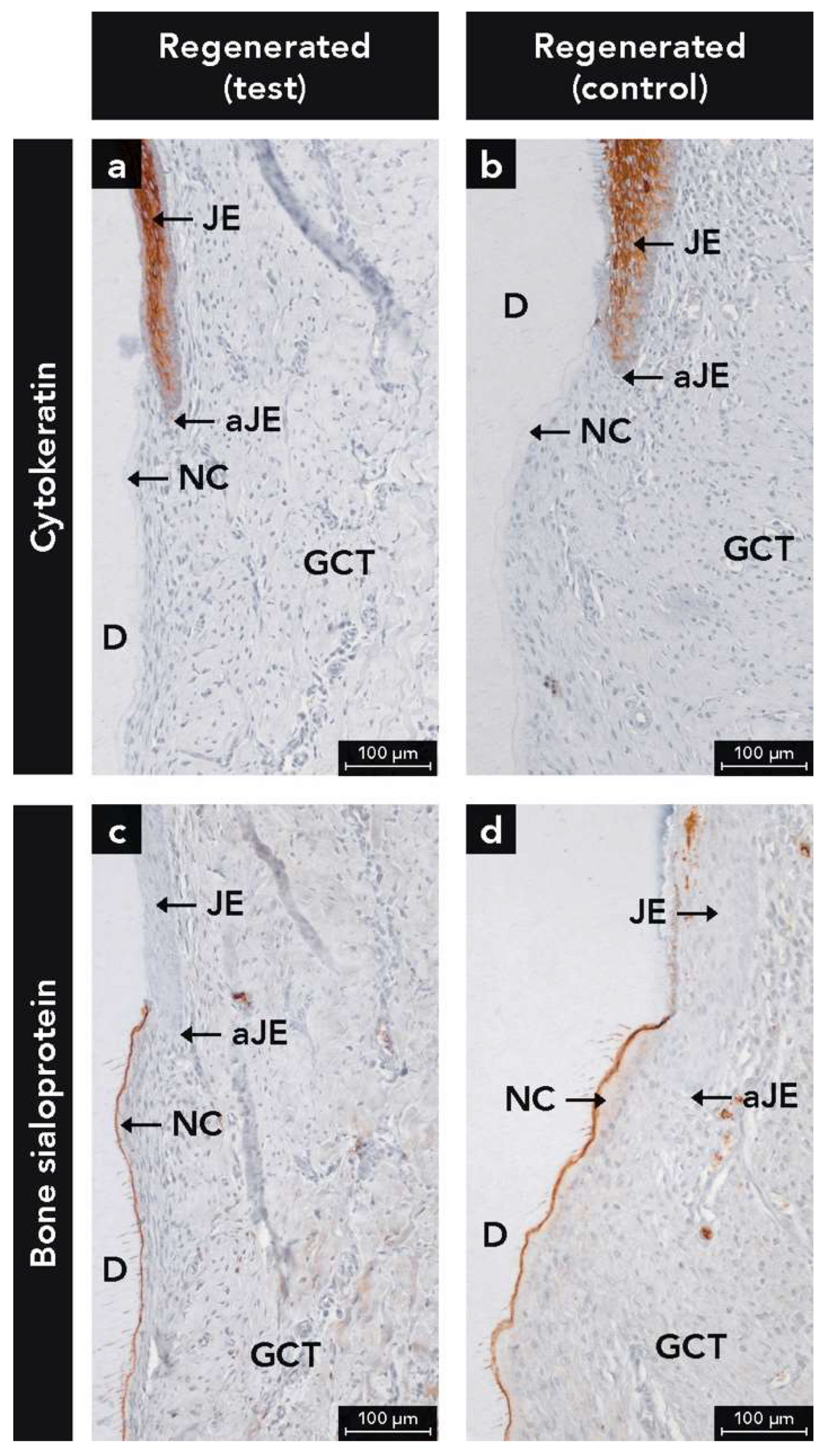
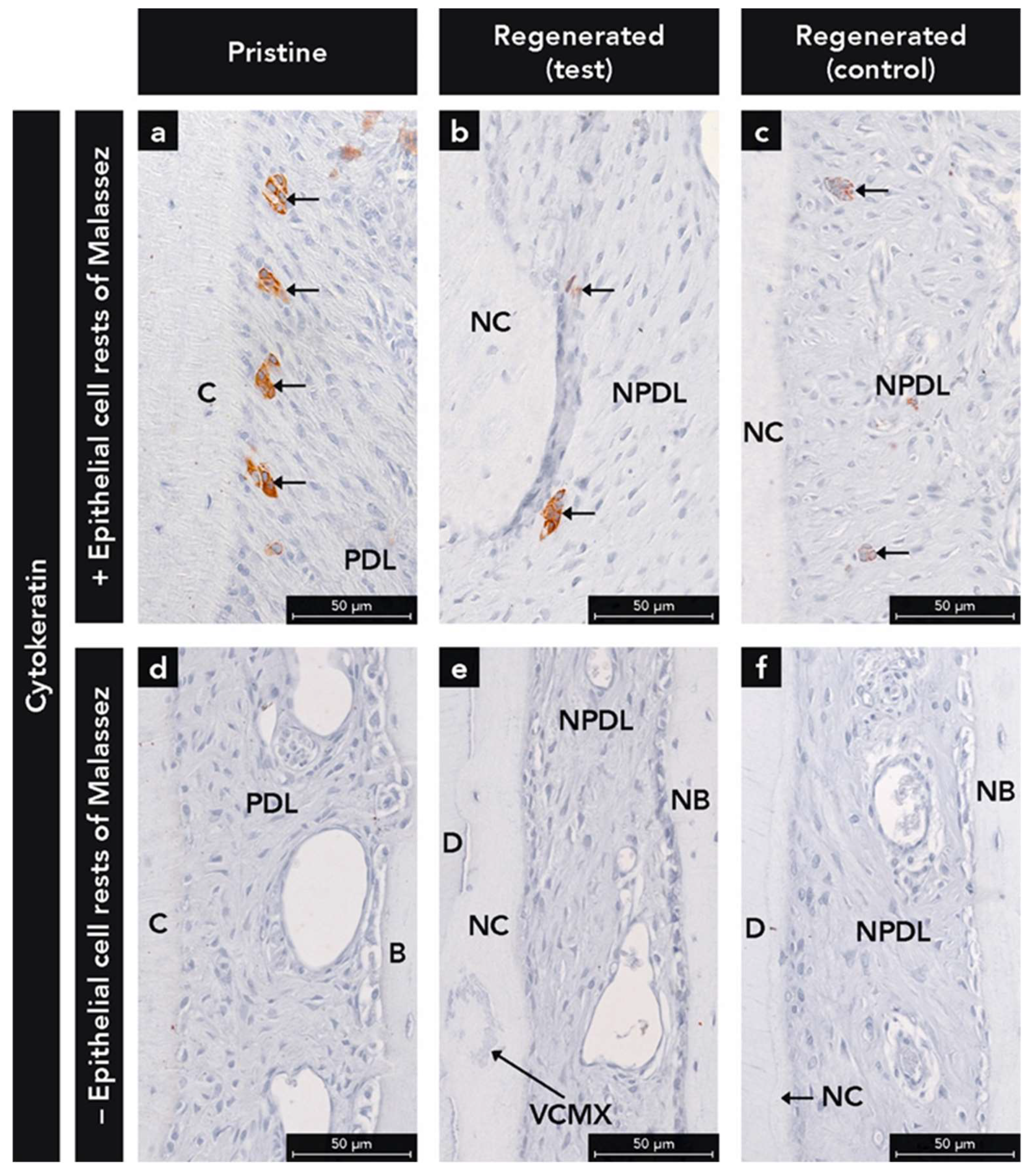
2.1.2. Anti-Cytokeratin Antibody
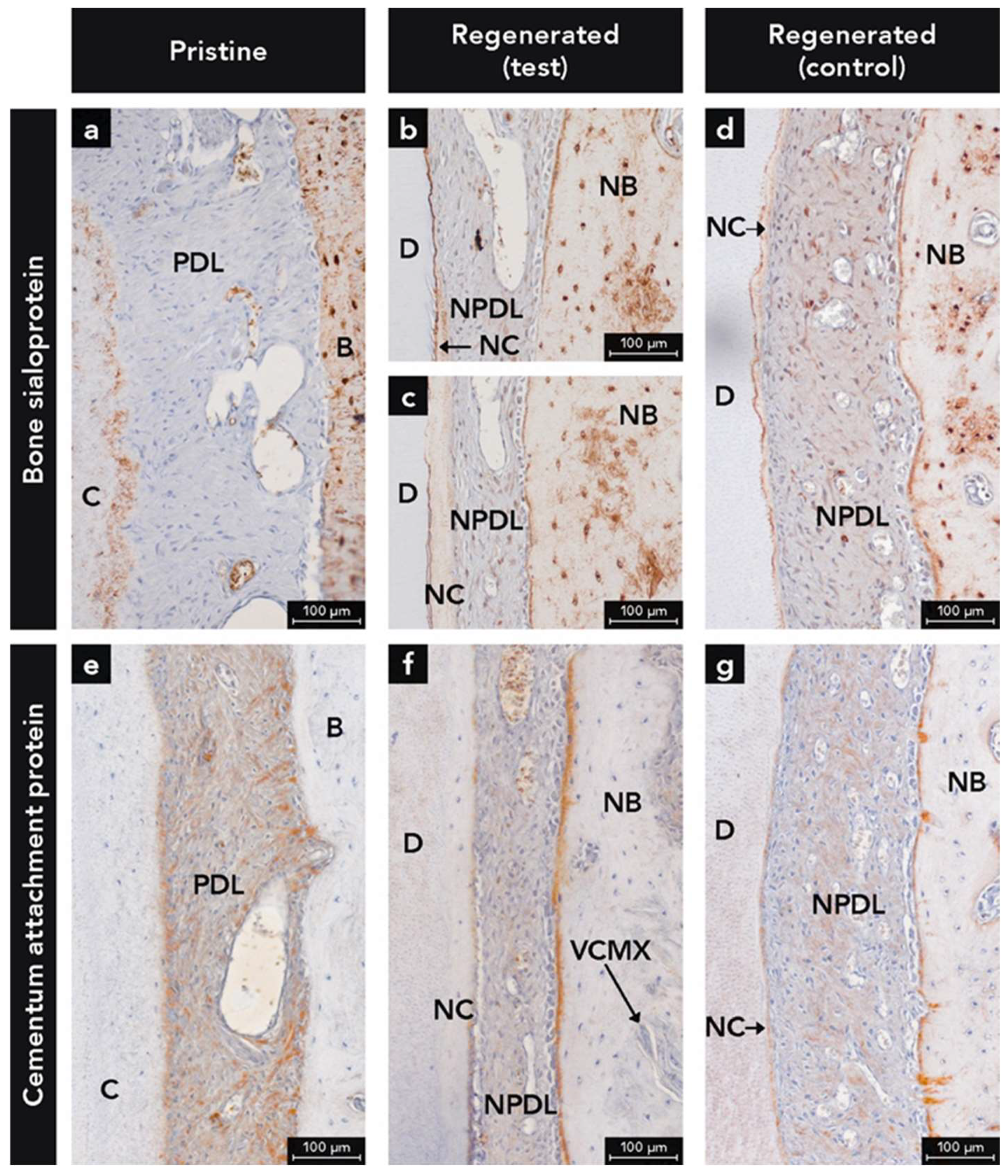
2.1.3. Anti-Bone Sialoprotein Antibody
2.1.4. Anti-Cementum Attachment Protein Antibody
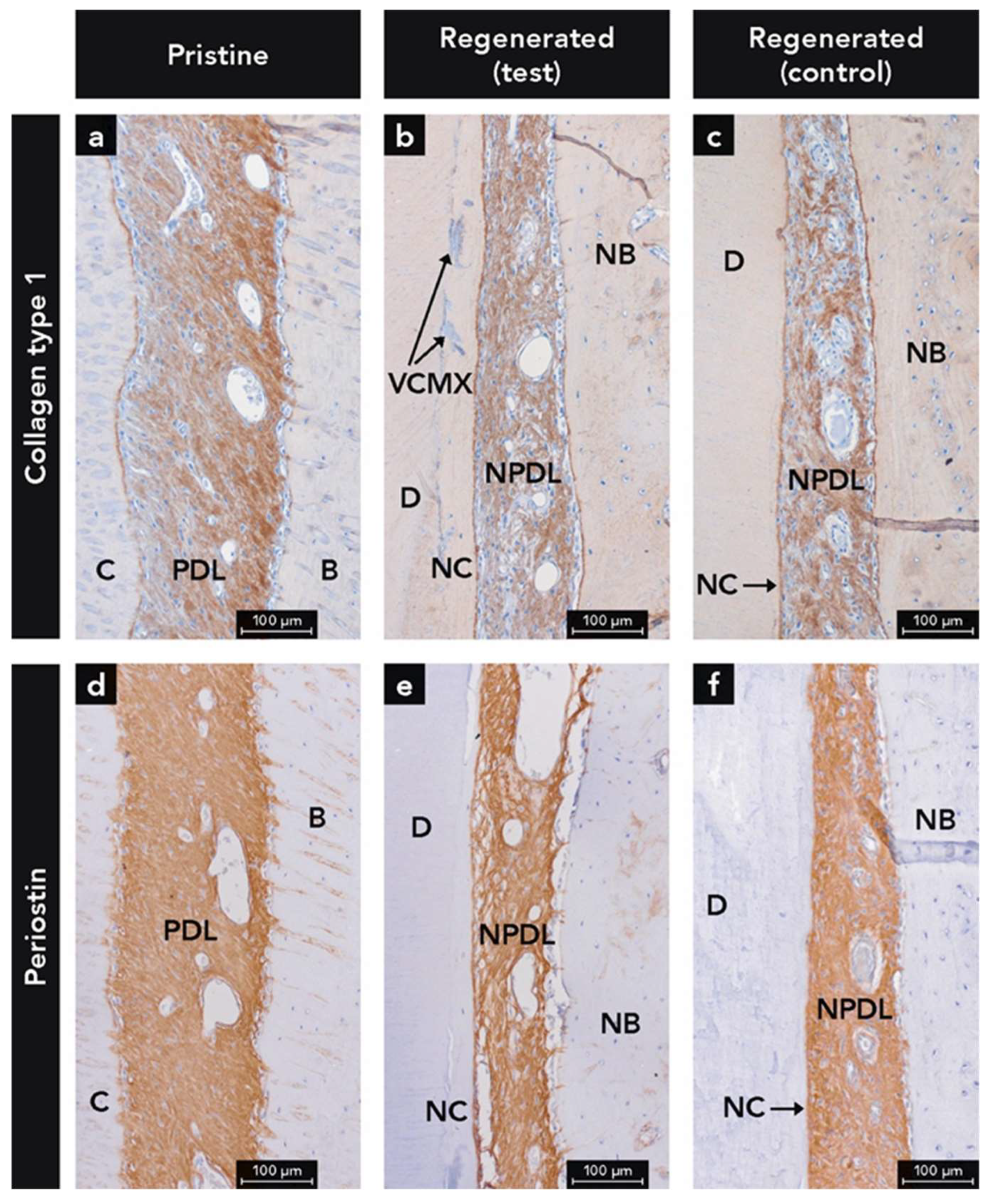
2.1.5. Anti-Collagen Type 1 Antibody
2.1.6. Anti-Periostin Antibody
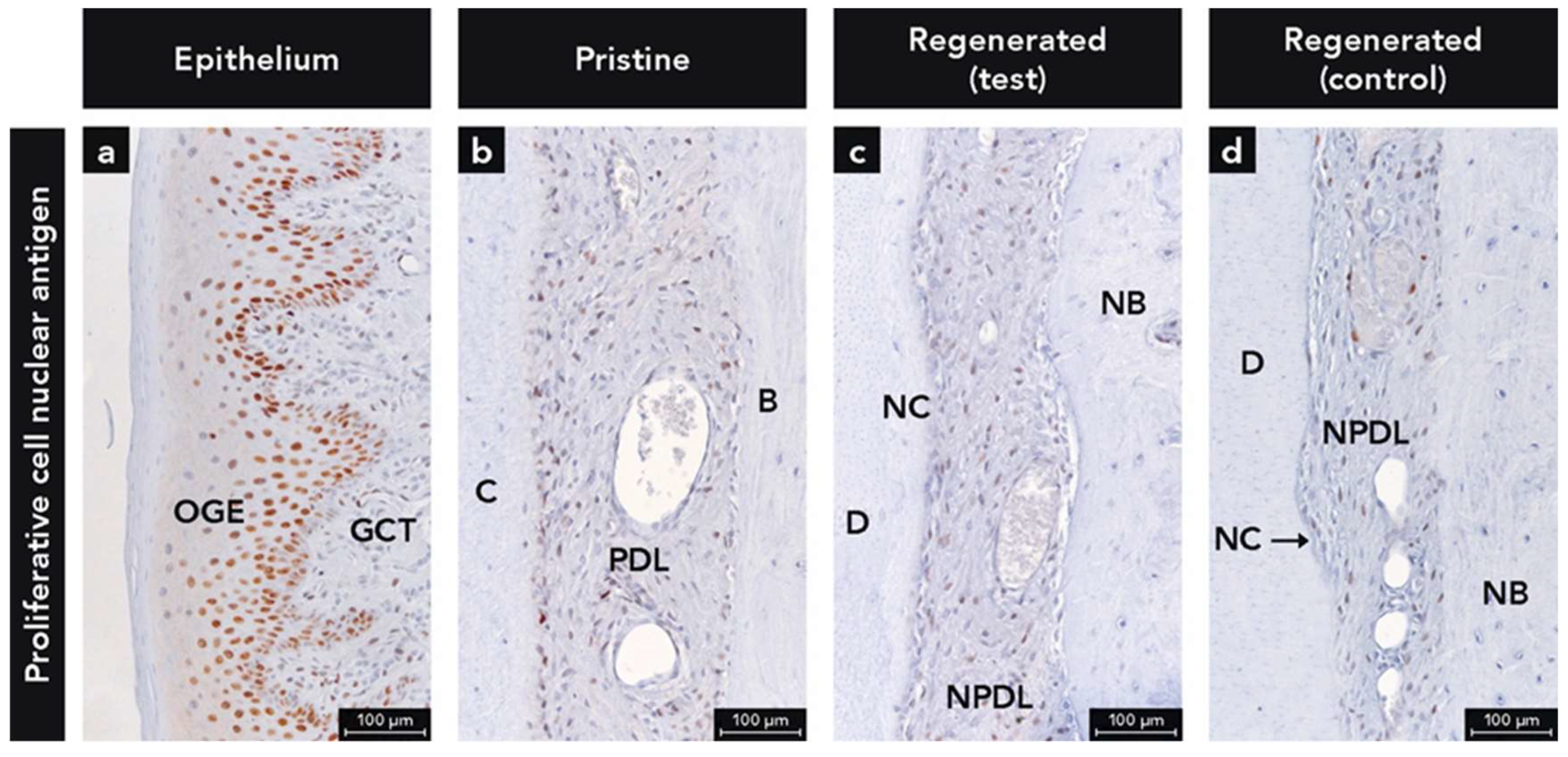
2.1.7. Anti-Proliferative Cell Nuclear Antigen Antibody
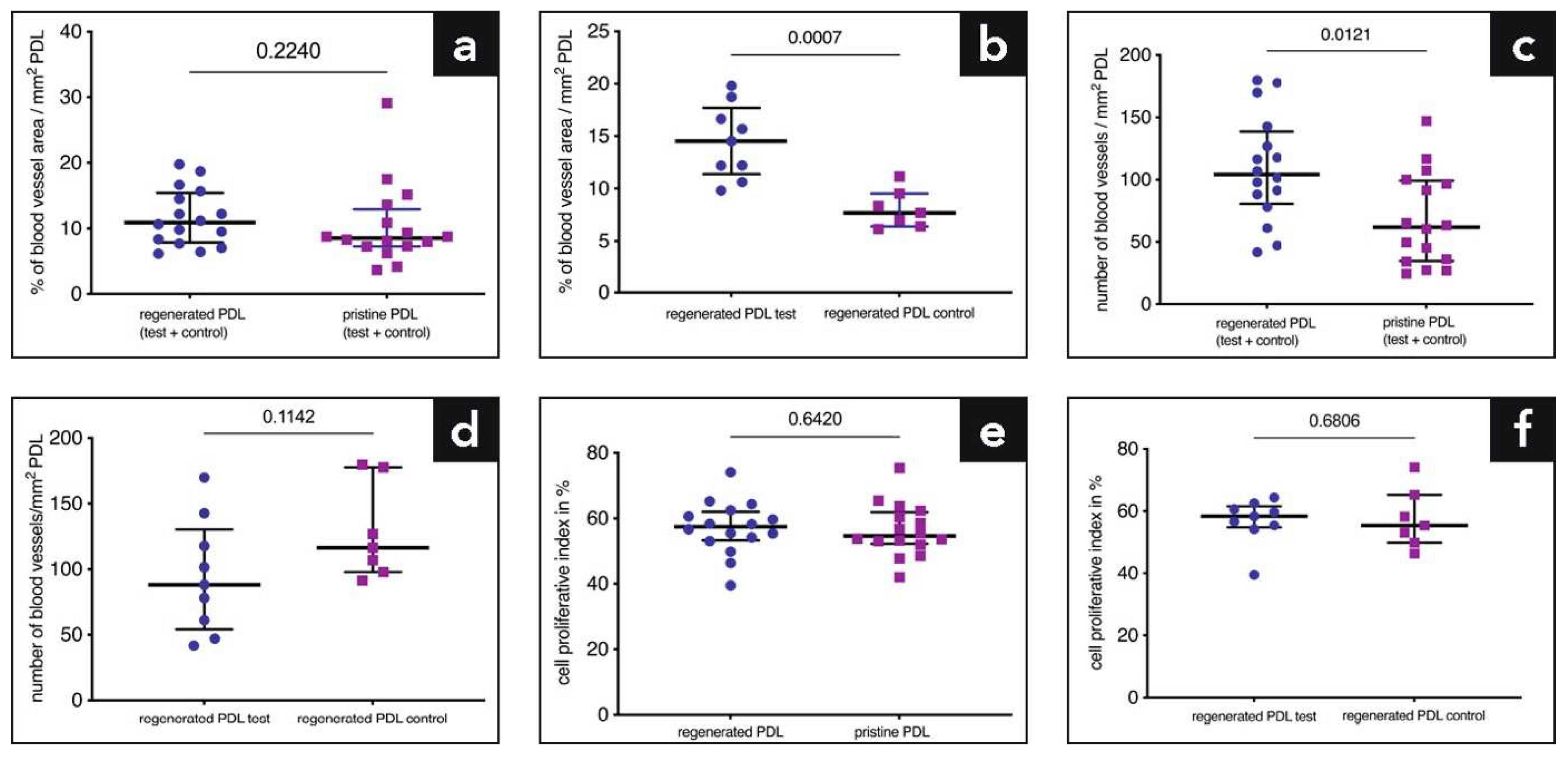
2.2. Quantitative Analysis of Blood Vessels and Proliferating Cells
3. Discussion
4. Materials and Methods
4.1. Animals & Surgical Procedure
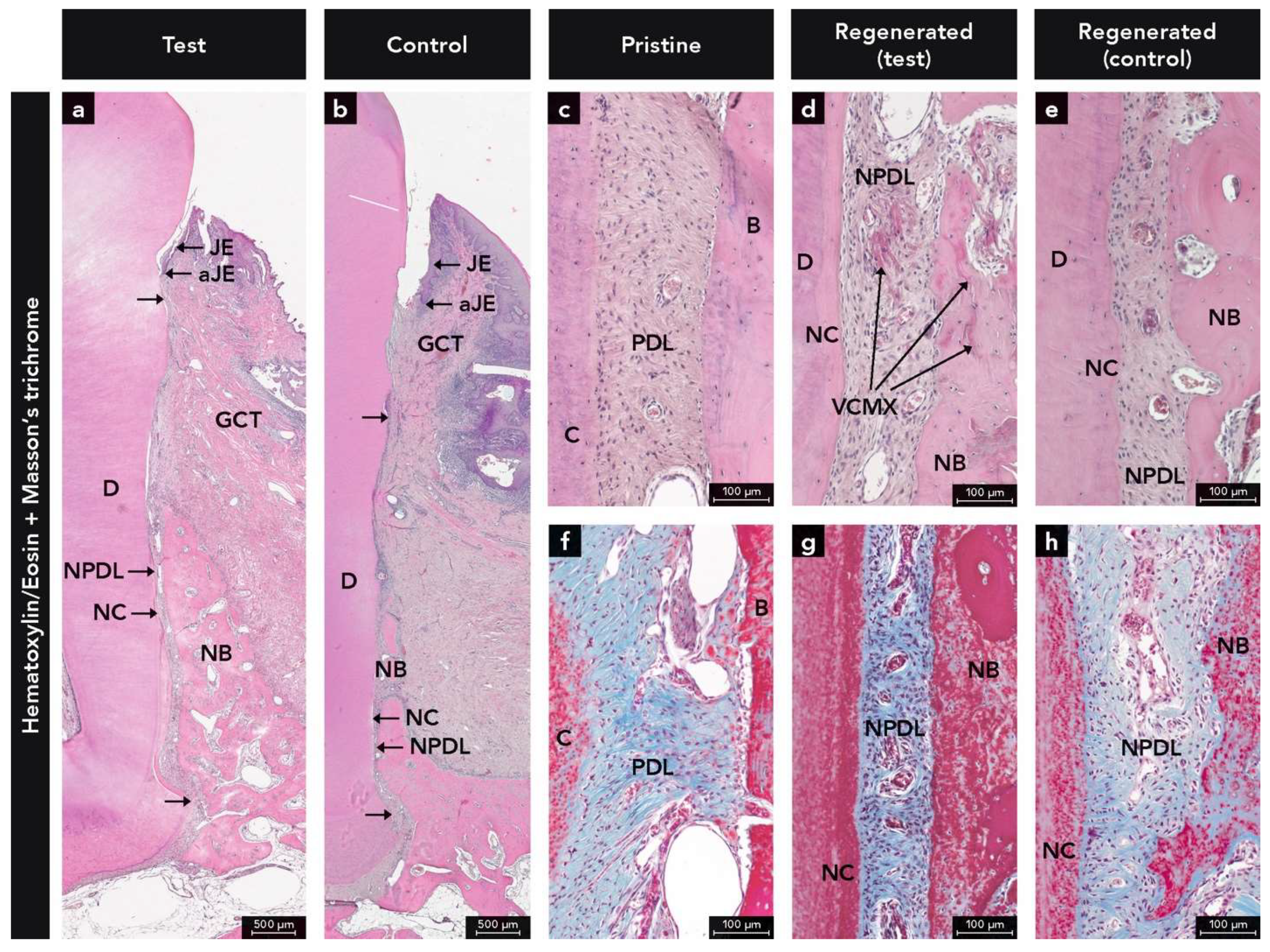
4.2. Histological Processing & Descriptive Analysis
4.3. Immunohistochemistry
4.3.1. Anti-Cytokeratin Antibody
4.3.2. Anti-Bone Sialoprotein Antibody
4.3.3. Anti-Cementum Attachment Protein Antibody
4.3.4. Collagen Type 1 Anti-Collagen Type 1 Antibody
4.3.5. Anti-Periostin Antibody
4.3.6. Anti-Proliferative Cell Nuclear Antigen Antibody
4.4. Quantitative Analysis of Proliferating Cells and Blood Vessels
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Avila-Ortiz, G.; De Buitrago, J.G.; Reddy, M.S. Periodontal regeneration—Furcation defects: A systematic review from the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S108–S130. [Google Scholar] [CrossRef] [Green Version]
- Cortellini, P.; Tonetti, M.S. Clinical concepts for regenerative therapy in intrabony defects. Periodontol. 2000 2015, 68, 282–307. [Google Scholar] [CrossRef]
- Kao, R.T.; Nares, S.; Reynolds, M.A. Periodontal regeneration—Intrabony defects: A systematic review from the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S77–S104. [Google Scholar] [CrossRef]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G.; Nemcovsky, C.; Donos, N.; Lyngstadaas, S.P.; Deschner, J.; Dard, M.; et al. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef]
- Reynolds, M.A.; Kao, R.T.; Camargo, P.M.; Caton, J.G.; Clem, D.S.; Fiorellini, J.P.; Geisinger, M.L.; Mills, M.P.; Nares, S.; Nevins, M.L. Periodontal regeneration—Intrabony defects: A consensus report from the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S105–S107. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; Jepsen, K.; Eickholz, P.; Jepsen, S. Clinical concepts for regenerative therapy in furcations. Periodontol. 2000 2015, 68, 308–332. [Google Scholar] [CrossRef]
- Sculean, A.; Nikolidakis, D.; Nikou, G.; Ivanovic, A.; Chapple, I.L.; Stavropoulos, A. Biomaterials for promoting periodontal regeneration in human intrabony defects: A systematic review. Periodontol. 2000 2015, 68, 182–216. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Wikesjo, U.M. Growth and differentiation factors for periodontal regeneration: A review on factors with clinical testing. J. Periodontal Res. 2012, 47, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Abusleme, L.; Hoare, A.; Hong, B.Y.; Diaz, P.I. Microbial signatures of health, gingivitis, and periodontitis. Periodontol. 2000 2021, 86, 57–78. [Google Scholar] [CrossRef]
- Curtis, M.A.; Diaz, P.I.; Van Dyke, T.E. The role of the microbiota in periodontal disease. Periodontol. 2000 2020, 83, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.; Curtis, M.A. Microbial transitions from health to disease. Periodontol. 2000 2021, 86, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: Intra-bony defects, furcation defects and periodontal plastic surgery. A systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 67–82. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Nikolidakis, D.; Schwarz, F. Regeneration of periodontal tissues: Combinations of barrier membranes and grafting materials—Biological foundation and preclinical evidence: A systematic review. J. Clin. Periodontol. 2008, 35, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Susin, C.; Fiorini, T.; Lee, J.; De Stefano, J.A.; Dickinson, D.P.; Wikesjo, U.M. Wound healing following surgical and regenerative periodontal therapy. Periodontol. 2000 2015, 68, 83–98. [Google Scholar] [CrossRef]
- Caballé-Serrano, J.; Zhang, S.; Ferrantino, L.; Simion, M.; Chappuis, V.; Bosshardt, D.D. Tissue Response to a Porous Collagen Matrix Used for Soft Tissue Augmentation. Materials 2019, 12, 3721. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [Green Version]
- Rico-Llanos, G.A.; Borrego-González, S.; Moncayo-Donoso, M.; Becerra, J.; Visser, R. Collagen Type I Biomaterials as Scaffolds for Bone Tissue Engineering. Polymers 2021, 13, 599. [Google Scholar] [CrossRef]
- Zuhr, O.; Baumer, D.; Hurzeler, M. The addition of soft tissue replacement grafts in plastic periodontal and implant surgery: Critical elements in design and execution. J. Clin. Periodontol. 2014, 41 (Suppl. 15), S123–S142. [Google Scholar] [CrossRef]
- Tavelli, L.; McGuire, M.K.; Zucchelli, G.; Rasperini, G.; Feinberg, S.E.; Wang, H.L.; Giannobile, W.V. Extracellular matrix-based scaffolding technologies for periodontal and peri-implant soft tissue regeneration. J. Periodontol. 2020, 91, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Caballé-Serrano, J.; Zhang, S.; Sculean, A.; Staehli, A.; Bosshardt, D.D. Tissue Integration and Degradation of a Porous Collagen-Based Scaffold Used for Soft Tissue Augmentation. Materials 2020, 13, 2420. [Google Scholar] [CrossRef]
- Thoma, D.S.; Jung, R.E.; Schneider, D.; Cochran, D.L.; Ender, A.; Jones, A.A.; Gorlach, C.; Uebersax, L.; Graf-Hausner, U.; Hammerle, C.H. Soft tissue volume augmentation by the use of collagen-based matrices: A volumetric analysis. J. Clin. Periodontol. 2010, 37, 659–666. [Google Scholar] [CrossRef] [Green Version]
- Thoma, D.S.; Zeltner, M.; Hilbe, M.; Hammerle, C.H.; Husler, J.; Jung, R.E. Randomized controlled clinical study evaluating effectiveness and safety of a volume-stable collagen matrix compared to autogenous connective tissue grafts for soft tissue augmentation at implant sites. J. Clin. Periodontol. 2016, 43, 874–885. [Google Scholar] [CrossRef]
- Zeltner, M.; Jung, R.E.; Hammerle, C.H.; Husler, J.; Thoma, D.S. Randomized controlled clinical study comparing a volume-stable collagen matrix to autogenous connective tissue grafts for soft tissue augmentation at implant sites: Linear volumetric soft tissue changes up to 3 months. J. Clin. Periodontol. 2017, 44, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Mathes, S.H.; Wohlwend, L.; Uebersax, L.; von Mentlen, R.; Thoma, D.S.; Jung, R.E.; Gorlach, C.; Graf-Hausner, U. A bioreactor test system to mimic the biological and mechanical environment of oral soft tissues and to evaluate substitutes for connective tissue grafts. Biotechnol. Bioeng. 2010, 107, 1029–1039. [Google Scholar] [CrossRef]
- Bozic, D.; Grgurevic, L.; Erjavec, I.; Brkljacic, J.; Orlic, I.; Razdorov, G.; Grgurevic, I.; Vukicevic, S.; Plancak, D. The proteome and gene expression profile of cementoblastic cells treated by bone morphogenetic protein-7 in vitro. J. Clin. Periodontol. 2012, 39, 80–90. [Google Scholar] [CrossRef]
- Ao, M.; Chavez, M.B.; Chu, E.Y.; Hemstreet, K.C.; Yin, Y.; Yadav, M.C.; Millán, J.L.; Fisher, L.W.; Goldberg, H.A.; Somerman, M.J.; et al. Overlapping functions of bone sialoprotein and pyrophosphate regulators in directing cementogenesis. Bone 2017, 105, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Foster, B.L.; Soenjaya, Y.; Nociti, F.H., Jr.; Holm, E.; Zerfas, P.M.; Wimer, H.F.; Holdsworth, D.W.; Aubin, J.E.; Hunter, G.K.; Goldberg, H.A.; et al. Deficiency in acellular cementum and periodontal attachment in bsp null mice. J. Dent. Res. 2013, 92, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, M.; Iwase, M.; Maslan, S.; Nozaki, N.; Yamauchi, M.; Handa, K.; Takahashi, O.; Sato, S.; Kawase, T.; Teranaka, T.; et al. Expression of cementum-derived attachment protein in bovine tooth germ during cementogenesis. Bone 2001, 29, 242–248. [Google Scholar] [CrossRef]
- Arzate, H.; Olson, S.W.; Page, R.C.; Gown, A.M.; Narayanan, A.S. Production of a monoclonal antibody to an attachment protein derived from human cementum. FASEB J. 1992, 6, 2990–2995. [Google Scholar] [CrossRef] [PubMed]
- BarKana, I.; Narayanan, A.S.; Grosskop, A.; Savion, N.; Pitaru, S. Cementum attachment protein enriches putative cementoblastic populations on root surfaces in vitro. J. Dent. Res. 2000, 79, 1482–1488. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Ikezawa, K.; Parker, T.; Saito, M.; Narayanan, A.S. Characterization of a collagenous cementum-derived attachment protein. J. Bone Min. Res. 1996, 11, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, K.; Amizuka, N.; Takeshita, S.; Takamatsu, H.; Katsuura, M.; Ozawa, H.; Toyama, Y.; Bonewald, L.F.; Kudo, A. Identification and characterization of a novel protein, periostin, with restricted expression to periosteum and periodontal ligament and increased expression by transforming growth factor beta. J. Bone Min. Res. 1999, 14, 1239–1249. [Google Scholar] [CrossRef] [PubMed]
- Kruzynska-Frejtag, A.; Wang, J.; Maeda, M.; Rogers, R.; Krug, E.; Hoffman, S.; Markwald, R.R.; Conway, S.J. Periostin is expressed within the developing teeth at the sites of epithelial-mesenchymal interaction. Dev. Dyn 2004, 229, 857–868. [Google Scholar] [CrossRef]
- Wilde, J.; Yokozeki, M.; Terai, K.; Kudo, A.; Moriyama, K. The divergent expression of periostin mRNA in the periodontal ligament during experimental tooth movement. Cell Tissue Res. 2003, 312, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Schweizer, J.; Bowden, P.E.; Coulombe, P.A.; Langbein, L.; Lane, E.B.; Magin, T.M.; Maltais, L.; Omary, M.B.; Parry, D.A.D.; Rogers, M.A.; et al. New consensus nomenclature for mammalian keratins. J. Cell Biol. 2006, 174, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Moll, R.; Divo, M.; Langbein, L. The human keratins: Biology and pathology. Histochem Cell Biol. 2008, 129, 705–733. [Google Scholar] [CrossRef] [Green Version]
- Barak, V.; Goike, H.; Panaretakis, K.W.; Einarsson, R. Clinical utility of cytokeratins as tumor markers. Clin. Biochem. 2004, 37, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Rao, R.S.; Patil, S.; Ganavi, B.S. Oral cytokeratins in health and disease. J. Contemp Dent. Pract. 2014, 15, 127–136. [Google Scholar] [CrossRef]
- Sculean, A.; Berakdar, M.; Pahl, S.; Windisch, P.; Brecx, M.; Reich, E.; Donos, N. Patterns of cytokeratin expression in monkey and human periodontium following regenerative and conventional periodontal surgery. J. Periodontal Res. 2001, 36, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Stadlinger, B.; Terheyden, H. Cell-to-cell communication--periodontal regeneration. Clin. Oral Implant. Res. 2015, 26, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Gronthos, S.; Bartold, P.M. Role of the epithelial cell rests of Malassez in the development, maintenance and regeneration of periodontal ligament tissues. Periodontol. 2000 2013, 63, 217–233. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, N.; Kawaguchi, H.; Ogawa, T.; Uchida, T.; Kurihara, H. Immunohistochemical characteristics of epithelial cell rests of Malassez during cementum repair. J. Periodontal Res. 2003, 38, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.; Berglundh, T.; Lindhe, J. The periodontal tissues in healed degree III furcation defects. An experimental study in dogs. J. Clin. Periodontol. 1996, 23, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Lioubavina, N.; Theilade, J.; Karring, T. Absence of Malassez epithelial rests in the regenerated periodontal ligament. A pilot study in the monkey. J. Periodontal Res. 1998, 33, 310–314. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Zalzal, S.; McKee, M.D.; Nanci, A. Developmental appearance and distribution of bone sialoprotein and osteopontin in human and rat cementum. Anat. Rec. 1998, 250, 13–33. [Google Scholar] [CrossRef]
- Foster, B.L. Methods for studying tooth root cementum by light microscopy. Int. J. Oral Sci. 2012, 4, 119–128. [Google Scholar] [CrossRef] [Green Version]
- Matsuura, M.; Herr, Y.; Han, K.Y.; Lin, W.L.; Genco, R.J.; Cho, M.I. Immunohistochemical expression of extracellular matrix components of normal and healing periodontal tissues in the beagle dog. J. Periodontol. 1995, 66, 579–593. [Google Scholar] [CrossRef]
- Nanci, A. Content and distribution of noncollagenous matrix proteins in bone and cementum: Relationship to speed of formation and collagen packing density. J. Struct Biol. 1999, 126, 256–269. [Google Scholar] [CrossRef]
- Dickinson, D.P.; Coleman, B.G.; Batrice, N.; Lee, J.; Koli, K.; Pennington, C.; Susin, C.; Wikesjö, U.M. Events of wound healing/regeneration in the canine supraalveolar periodontal defect model. J. Clin. Periodontol. 2013, 40, 527–541. [Google Scholar] [CrossRef]
- MacNeil, R.L.; D’Errico, J.A.; Ouyang, H.; Berry, J.; Strayhorn, C.; Somerman, M.J. Isolation of murine cementoblasts: Unique cells or uniquely-positioned osteoblasts? Eur. J. Oral Sci 1998, 106 (Suppl. 1), 350–356. [Google Scholar] [CrossRef] [Green Version]
- MacNeil, R.L.; Berry, J.; D’Errico, J.; Strayhorn, C.; Piotrowski, B.; Somerman, M.J. Role of two mineral-associated adhesion molecules, osteopontin and bone sialoprotein, during cementogenesis. Connect. Tissue Res. 1995, 33, 1–7. [Google Scholar] [CrossRef]
- Lao, M.; Marino, V.; Bartold, P.M. Immunohistochemical study of bone sialoprotein and osteopontin in healthy and diseased root surfaces. J. Periodontol. 2006, 77, 1665–1673. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Degen, T.; Lang, N.P. Sequence of protein expression of bone sialoprotein and osteopontin at the developing interface between repair cementum and dentin in human deciduous teeth. Cell Tissue Res. 2005, 320, 399–407. [Google Scholar] [CrossRef] [Green Version]
- Ivanovski, S.; Li, H.; Daley, T.; Bartold, P.M. An immunohistochemical study of matrix molecules associated with barrier membrane-mediated periodontal wound healing. J. Periodontal Res. 2000, 35, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Sodek, J.; Ganss, B.; McKee, M.D. Osteopontin. Crit. Rev. Oral Biol. Med. Off. Publ. Am. Assoc. Oral Biol. 2000, 11, 279–303. [Google Scholar] [CrossRef] [PubMed]
- Denhardt, D.T.; Noda, M. Osteopontin expression and function: Role in bone remodeling. J. Cell Biochem. 1998, 72 (Suppl. 30–31), 92–102. [Google Scholar] [CrossRef]
- Rittling, S.R.; Denhardt, D.T. Osteopontin function in pathology: Lessons from osteopontin-deficient mice. Exp. Nephrol. 1999, 7, 103–113. [Google Scholar] [CrossRef]
- Si, J.; Wang, C.; Zhang, D.; Wang, B.; Zhou, Y. Osteopontin in Bone Metabolism and Bone Diseases. Med. Sci. Monit 2020, 26, e919159. [Google Scholar] [CrossRef] [PubMed]
- Iwata, T.; Mizuno, N.; Nagahara, T.; Kaneda-Ikeda, E.; Kajiya, M.; Kitagawa, M.; Takeda, K.; Yoshioka, M.; Yagi, R.; Takata, T.; et al. Identification of regulatory mRNA and microRNA for differentiation into cementoblasts and periodontal ligament cells. J. Periodontal Res. 2021, 56, 69–82. [Google Scholar] [CrossRef]
- ADA and AAP introduce dentists to new time saving periodontal evaluation system. Va. Dent. J. 1992, 69, 16–17.
- Rios, H.F.; Ma, D.; Xie, Y.; Giannobile, W.V.; Bonewald, L.F.; Conway, S.J.; Feng, J.Q. Periostin is essential for the integrity and function of the periodontal ligament during occlusal loading in mice. J. Periodontol. 2008, 79, 1480–1490. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Rios, H.F.; Jin, Q.; Sugai, J.V.; Padial-Molina, M.; Taut, A.D.; Flanagan, C.L.; Hollister, S.J.; Giannobile, W.V. Tissue engineering bone-ligament complexes using fiber-guiding scaffolds. Biomaterials 2012, 33, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Norris, R.A.; Damon, B.; Mironov, V.; Kasyanov, V.; Ramamurthi, A.; Moreno-Rodriguez, R.; Trusk, T.; Potts, J.D.; Goodwin, R.L.; Davis, J.; et al. Periostin regulates collagen fibrillogenesis and the biomechanical properties of connective tissues. J. Cell Biochem. 2007, 101, 695–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanci, A.; Bosshardt, D.D. Structure of periodontal tissues in health and disease. Periodontol. 2000 2006, 40, 11–28. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Bergomi, M.; Vaglio, G.; Wiskott, A. Regional structural characteristics of bovine periodontal ligament samples and their suitability for biomechanical tests. J. Anat. 2008, 212, 319–329. [Google Scholar] [CrossRef]
- Follin, M.E.; Nilsson, L.P. Blood supply in bone and periodontal ligament tissue surrounding mandibular fourth premolars in dogs—A morphological study. Eur. J. Orthod 1986, 8, 167–171. [Google Scholar] [CrossRef]
- Foong, K.; Sims, M.R. Blood volume in human bicuspid periodontal ligament determined by electron microscopy. Arch. Oral Biol. 1999, 44, 465–474. [Google Scholar] [CrossRef]
- Mehdizadeh, H.; Sumo, S.; Bayrak, E.S.; Brey, E.M.; Cinar, A. Three-dimensional modeling of angiogenesis in porous biomaterial scaffolds. Biomaterials 2013, 34, 2875–2887. [Google Scholar] [CrossRef]
- Embery, G. An update on the biochemistry of the periodontal ligament. Eur. J. Orthod 1990, 12, 77–80. [Google Scholar] [CrossRef]
- Gould, T.R.; Brunette, D.M.; Dorey, J. Cell turnover in the periodontal ligament determined by continuous infusion of H3-thymidine using osmotic minipumps. J. Periodontal Res. 1982, 17, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Lekic, P.; McCulloch, C.A. Periodontal ligament cell population: The central role of fibroblasts in creating a unique tissue. Anat. Rec. 1996, 245, 327–341. [Google Scholar] [CrossRef]
- Beertsen, W.; McCulloch, C.A.; Sodek, J. The periodontal ligament: A unique, multifunctional connective tissue. Periodontol. 2000 1997, 13, 20–40. [Google Scholar] [CrossRef]
- Liu, J.; Ruan, J.; Weir, M.D.; Ren, K.; Schneider, A.; Wang, P.; Oates, T.W.; Chang, X.; Xu, H.H.K. Periodontal Bone-Ligament-Cementum Regeneration via Scaffolds and Stem Cells. Cells 2019, 8, 537. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; He, X.T.; Yin, Y.; Wu, R.X.; Tian, B.M.; Chen, F.M. Administration of signalling molecules dictates stem cell homing for in situ regeneration. J. Cell. Mol. Med. 2017, 21, 3162–3177. [Google Scholar] [CrossRef]
- Karring, T.; Isidor, F.; Nyman, S.; Lindhe, J. New attachment formation on teeth with a reduced but healthy periodontal ligament. J. Clin. Periodontol. 1985, 12, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Karring, T.; Nyman, S.; Lindhe, J. Healing following implantation of periodontitis affected roots into bone tissue. J. Clin. Periodontol. 1980, 7, 96–105. [Google Scholar] [CrossRef]
- Polimeni, G.; Xiropaidis, A.V.; Wikesjö, U.M. Biology and principles of periodontal wound healing/regeneration. Periodontol. 2000 2006, 41, 30–47. [Google Scholar] [CrossRef]
- Ramseier, C.A.; Rasperini, G.; Batia, S.; Giannobile, W.V. Advanced reconstructive technologies for periodontal tissue repair. Periodontol. 2000 2012, 59, 185–202. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.Y.; Li, X.; Wang, J.; He, X.T.; Sun, H.H.; Chen, F.M. Concise Review: Periodontal Tissue Regeneration Using Stem Cells: Strategies and Translational Considerations. Stem Cells Transl. Med. 2019, 8, 392–403. [Google Scholar] [CrossRef] [Green Version]
- Carmagnola, D.; Tarce, M.; Dellavia, C.; Rimondini, L.; Varoni, E.M. Engineered scaffolds and cell-based therapy for periodontal regeneration. J. Appl. Biomater. Funct Mater. 2017, 15, e303–e312. [Google Scholar] [CrossRef] [Green Version]
- d’vanzo, N.; Bruno, M.C.; Giudice, A.; Mancuso, A.; Gaetano, F.; Cristiano, M.C.; Paolino, D.; Fresta, M. Influence of Materials Properties on Bio-Physical Features and Effectiveness of 3D-Scaffolds for Periodontal Regeneration. Molecules 2021, 26, 1643. [Google Scholar] [CrossRef]
- Ashworth, J.C.; Mehr, M.; Buxton, P.G.; Best, S.M.; Cameron, R.E. Optimising collagen scaffold architecture for enhanced periodontal ligament fibroblast migration. J. Mater. Sci. Mater. Med. 2018, 29, 166. [Google Scholar] [CrossRef] [Green Version]
- Owen, S.C.; Shoichet, M.S. Design of three-dimensional biomimetic scaffolds. J. Biomed. Mater. Res. A 2010, 94, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- Tayalia, P.; Mazur, E.; Mooney, D.J. Controlled architectural and chemotactic studies of 3D cell migration. Biomaterials 2011, 32, 2634–2641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donos, N.; Park, J.C.; Vajgel, A.; de Carvalho Farias, B.; Dereka, X. Description of the periodontal pocket in preclinical models: Limitations and considerations. Periodontol. 2000 2018, 76, 16–34. [Google Scholar] [CrossRef]
- Selvig, K.A. Discussion: Animal models in reconstructive therapy. J. Periodontol 1994, 65, 1169–1172. [Google Scholar] [CrossRef]
- Lee, J.S.; Wikesjö, U.M.; Jung, U.W.; Choi, S.H.; Pippig, S.; Siedler, M.; Kim, C.K. Periodontal wound healing/regeneration following implantation of recombinant human growth/differentiation factor-5 in a beta-tricalcium phosphate carrier into one-wall intrabony defects in dogs. J. Clin. Periodontol. 2010, 37, 382–389. [Google Scholar] [CrossRef]
- Park, J.C.; Wikesjö, U.M.; Koo, K.T.; Lee, J.S.; Kim, Y.T.; Pippig, S.D.; Bastone, P.; Kim, C.S.; Kim, C.K. Maturation of alveolar bone following implantation of an rhGDF-5/PLGA composite into 1-wall intra-bony defects in dogs: 24-week histometric observations. J. Clin. Periodontol. 2012, 39, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Animal models for periodontal regeneration and peri-implant responses. Periodontol. 2000 2015, 68, 66–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oz, H.S.; Puleo, D.A. Animal models for periodontal disease. J. Biomed. Biotechnol. 2011, 2011, 754857. [Google Scholar] [CrossRef] [Green Version]
- Kilkenny, C.; Browne, W.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Animal research: Reporting in vivo experiments--the ARRIVE guidelines. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2011, 31, 991–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imber, J.C.; Bosshardt, D.D.; Stähli, A.; Saulacic, N.; Deschner, J.; Sculean, A. Preclinical evaluation of the effect of a volume-stable collagen matrix on periodontal regeneration in two-wall intrabony defects. J. Clin. Periodontol. 2021, 48, 560–569. [Google Scholar] [CrossRef]
- Varley, C.L.; Armitage, S.; Dickson, A.J. Activation of stress-activated protein kinases by hepatocyte isolation induces gene 33 expression. Biochem. Biophys. Res. Commun. 1999, 254, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Ebensberger, U.; Pohl, Y.; Filippi, A. PCNA-expression of cementoblasts and fibroblasts on the root surface after extraoral rinsing for decontamination. Dent. Traumatol 2002, 18, 262–266. [Google Scholar] [CrossRef]
- Celenligil-Nazliel, H.; Ayhan, A.; Uzun, H.; Ruacan, S. The effect of age on proliferating cell nuclear antigen expression in oral gingival epithelium of healthy and inflamed human gingiva. J. Periodontol 2000, 71, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Franquemont, D.W.; Frierson, H.F., Jr. Proliferating cell nuclear antigen immunoreactivity and prognosis of gastrointestinal stromal tumors. Mod. Pathol. 1995, 8, 473–477. [Google Scholar]
- Liu, J.; Li, Q.; Liu, S.; Gao, J.; Qin, W.; Song, Y.; Jin, Z. Periodontal Ligament Stem Cells in the Periodontitis Microenvironment Are Sensitive to Static Mechanical Strain. Stem Cells Int. 2017, 2017, 1380851. [Google Scholar] [CrossRef]
- Yu, C.C.; Woods, A.L.; Levison, D.A. The assessment of cellular proliferation by immunohistochemistry: A review of currently available methods and their applications. Histochem. J. 1992, 24, 121–131. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| % of Blood Vessel Area/mm2 | Number of Blood Vessels/mm2 | Proliferative Index PI | ||||
|---|---|---|---|---|---|---|
| Mean, SD | Median | Mean, SD | Median | Mean, SD | Median | |
| Groups | ||||||
| Regenerated test 1 | 14.48 ± 3.52 | 10.91 | 94.26 ± 43.40 | 88.14 | 56.81 ± 7.26 | 58.36 |
| Regenerated control 2 | 8.05 ± 1.85 | 7.70 | 128.17 ± 36.45 | 116.50 | 57.45 ± 9.50 | 55.38 |
| Regenerated total t+c 3 | 11.66 ± 4.33 | 10.91 | 109.09 ± 42.87 | 104.30 | 57.09 ± 8.02 | 57.44 |
| Pristine test 4 | 11.56 ± 7.37 | 8.29 | 63.01 ± 35.22 | 49.56 | 55.25 ± 6.93 | 53.79 |
| Pristine control 5 | 8.86 ± 4.34 | 8.73 | 78.21 ± 39.49 | 78.39 | 57.85 ± 9.50 | 56.80 |
| Pristine total t+c 6 | 10.38 ± 6.20 | 8.51 | 68.28 ± 37.30 | 61.89 | 56.39 ± 7.97 | 56.39 |
| p value 1 vs. 2 | 0.007 | 0.114 | 0.680 | |||
| p value 3 vs. 6 | 0.224 | 0.012 | 0.642 | |||
| p value 4 vs. 5 | 0.680 | 0.524 | 0.757 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imber, J.-C.; Roccuzzo, A.; Stähli, A.; Saulacic, N.; Deschner, J.; Sculean, A.; Bosshardt, D.D. Immunohistochemical Evaluation of Periodontal Regeneration Using a Porous Collagen Scaffold. Int. J. Mol. Sci. 2021, 22, 10915. https://doi.org/10.3390/ijms222010915
Imber J-C, Roccuzzo A, Stähli A, Saulacic N, Deschner J, Sculean A, Bosshardt DD. Immunohistochemical Evaluation of Periodontal Regeneration Using a Porous Collagen Scaffold. International Journal of Molecular Sciences. 2021; 22(20):10915. https://doi.org/10.3390/ijms222010915
Chicago/Turabian StyleImber, Jean-Claude, Andrea Roccuzzo, Alexandra Stähli, Nikola Saulacic, James Deschner, Anton Sculean, and Dieter Daniel Bosshardt. 2021. "Immunohistochemical Evaluation of Periodontal Regeneration Using a Porous Collagen Scaffold" International Journal of Molecular Sciences 22, no. 20: 10915. https://doi.org/10.3390/ijms222010915