
Clonal Expansion of Tumor-Infiltrating T Cells and Analysis of the Tumor Microenvironment within Esophageal Squamous Cell Carcinoma Relapsed after Definitive Chemoradiation Therapy

 ,
, 
Abstract
:1. Introduction
2. Results
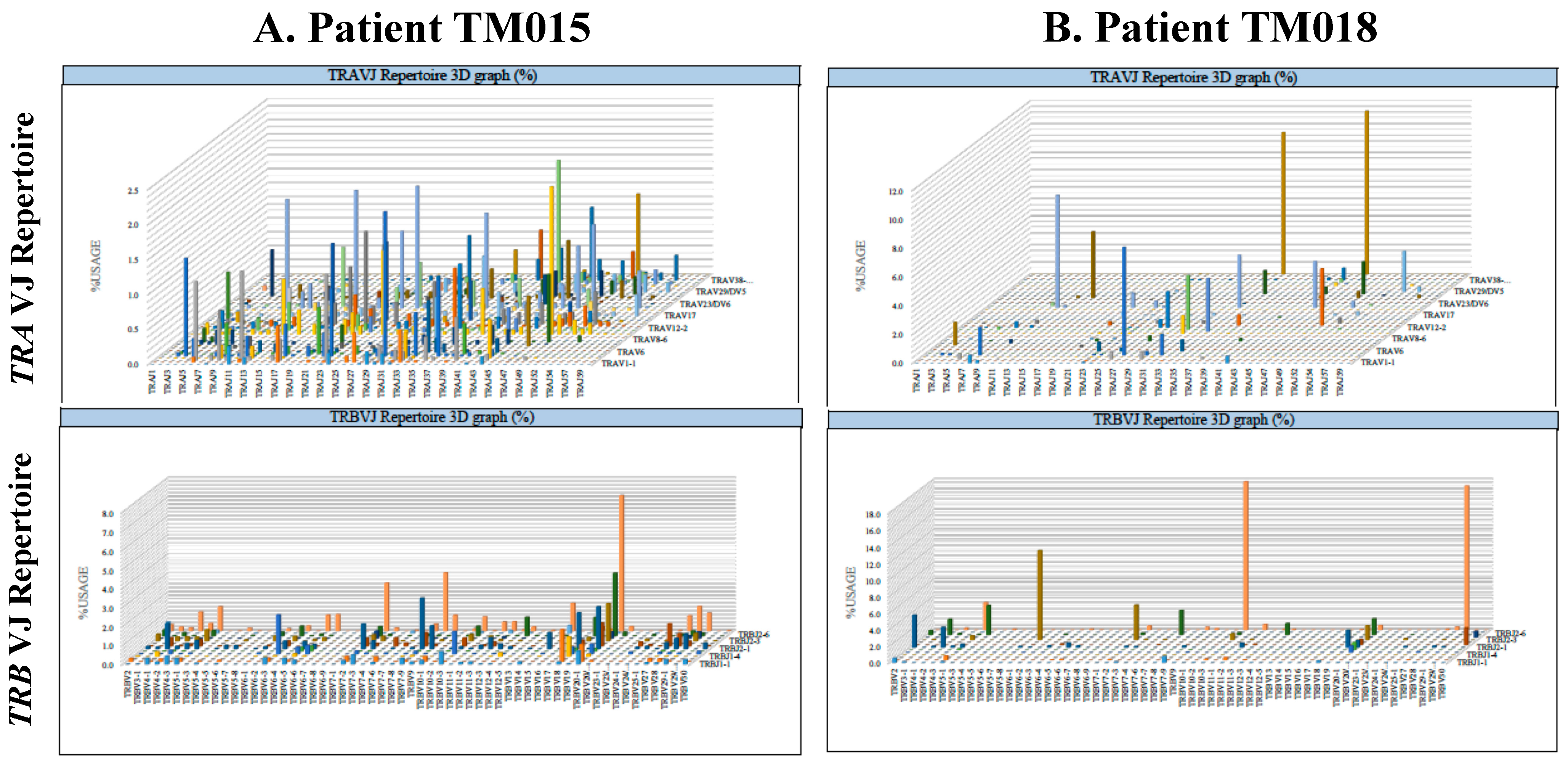
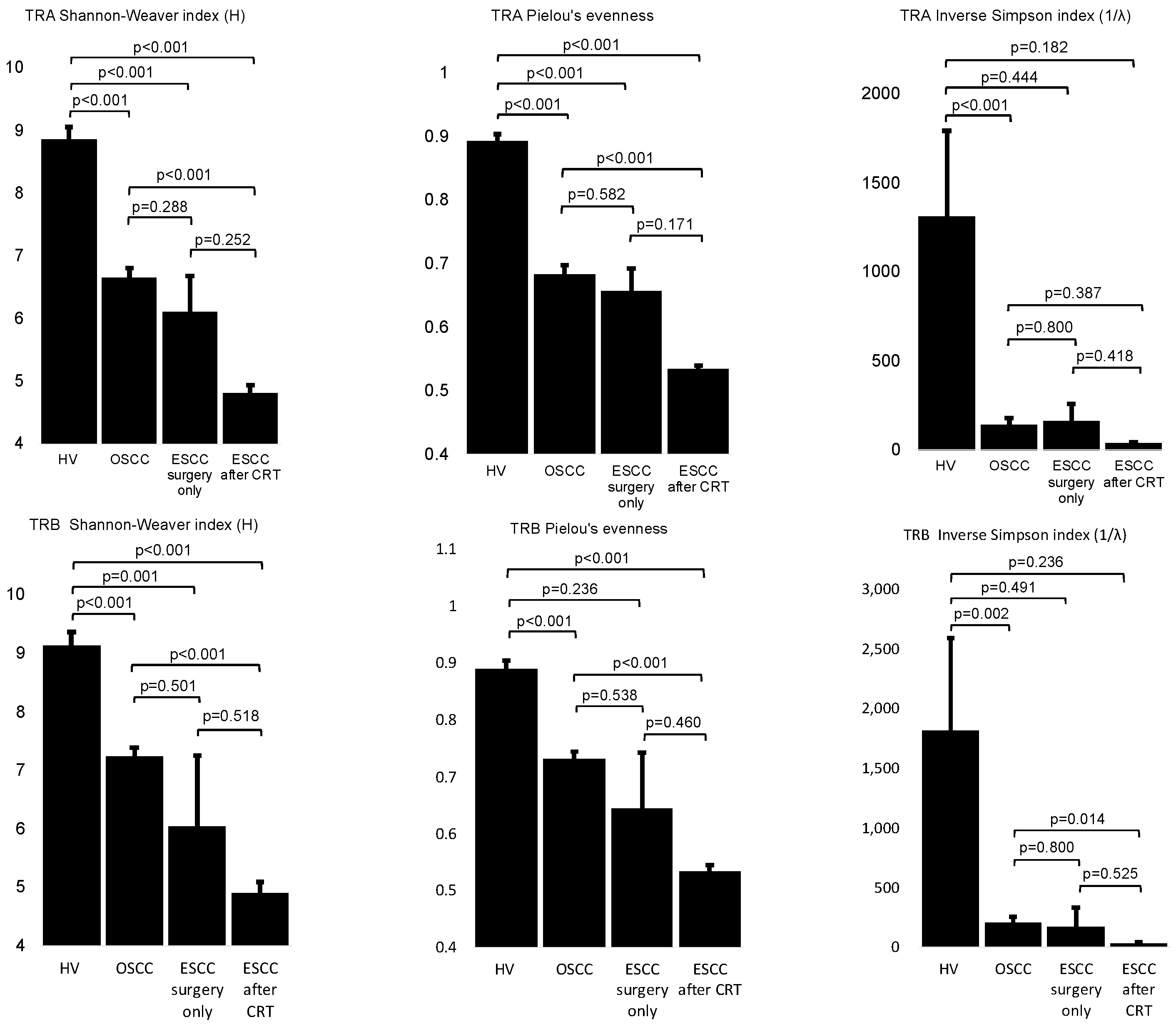
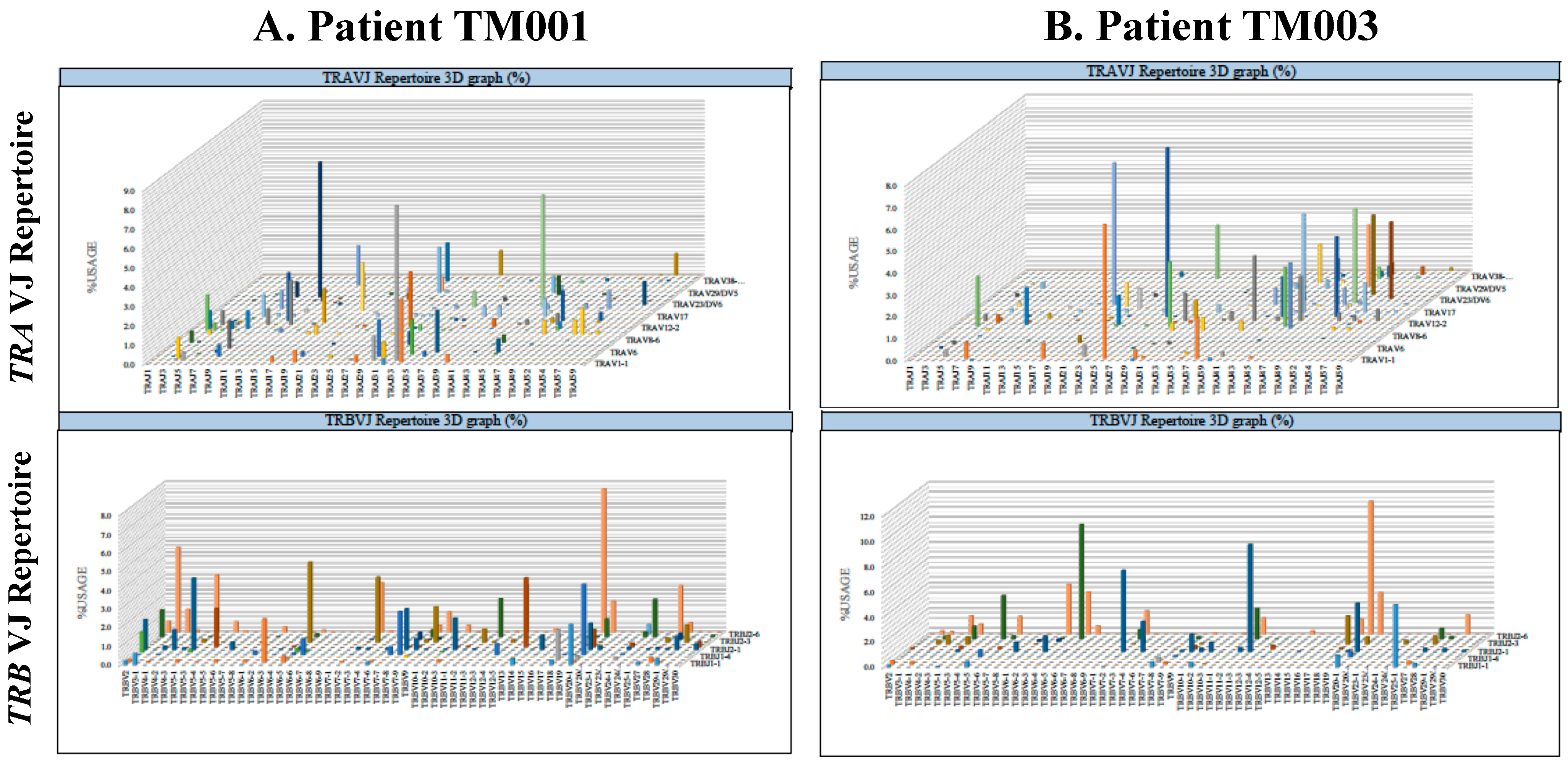
2.1. Clonal Expansion of Tumor-Infiltrating T Lymphocytes Was Significantly Induced within Esophageal and Oral Squamous Cell Carcinoma Tumor Tissues and Mostly Induced within Esophageal Squamous Cell Carcinoma That Relapsed after Definitive CRT
2.2. Divergency of the T-Cell Receptor Repertoire of Tumor-Infiltrating Lymphocytes Was Not Significantly Different between Patients with Good or Poor Prognoses after Salvage Surgery for Esophageal Squamous Cell Carcinoma Locally Relapsed after Definitive Chemoradiation Therapy
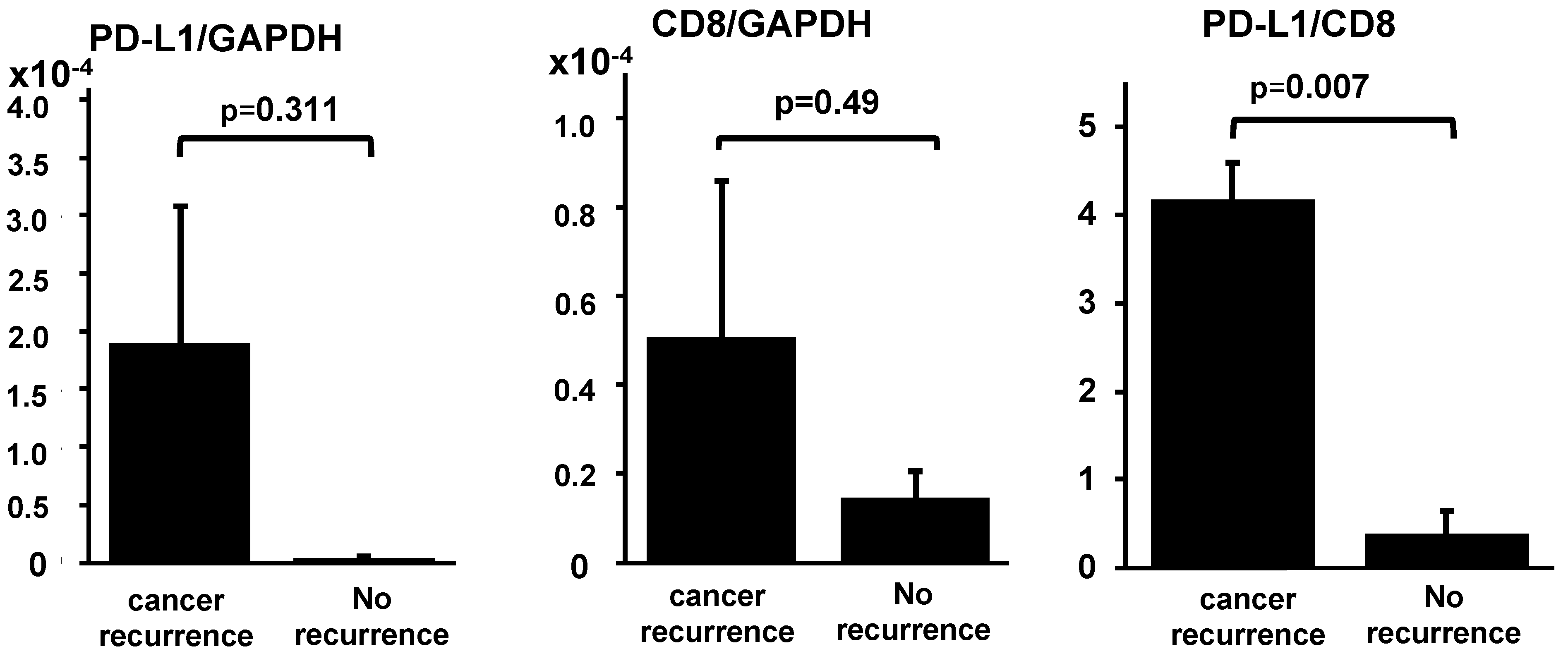
2.3. Ratio of PD-L1 mRNA to CD8B mRNA within Tumor Tissues Significantly Higher in Patients with Poor Prognoses after Salvage Surgery for Locally Relapsed Esophageal Squamous Cell Carcinoma after Definitive Chemoradiation Therapy
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. RNA Extraction from Tumor Tissues
4.3. T-Cell Receptor Repertoire Analysis
4.4. cDNA Synthesis and Quantitative Polymerase Chain Reaction
- CD8B-forward 5′-GGCATCTACTTCTGCATGATCGTC-3′
- CD8B-reverse 5′-TGGGTAACCGGCACACTCTC-3′
- PD-L1-forward 5′-AAATGGAACCTGGCGAAAGC-3′
- PD-L1-reverse 5′-GATGAGCCCCTCAGGCATTT-3′
- GAPDH-forward 5′-GCACCGTCAAGGCTGAGAAC-3′
- GAPDH-reverse 5′-ATGGTGGTGAAGACGCCAGT-3′.
4.5. Diversity Metric Calculation
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, W.; Zheng, R.; Zuo, T.; Zeng, H.; Zhang, S.; He, J. National cancer incidence and mortality in China, 2012. Chin. J. Cancer Res. 2016, 28, 1–11. [Google Scholar] [PubMed]
- Global Burden of Disease Cancer, C.; Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [CrossRef] [PubMed]
- Tachimori, Y.; Ozawa, S.; Numasaki, H.; Ishihara, R.; Matsubara, H.; Muro, K.; Oyama, T.; Toh, Y.; Udagawa, H.; Uno, T.; et al. Comprehensive registry of esophageal cancer in Japan, 2011. Esophagus 2018, 15, 127–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bollschweiler, E.; Holscher, A.H.; Schmidt, M.; Warnecke-Eberz, U. Neoadjuvant treatment for advanced esophageal cancer: Response assessment before surgery and how to predict response to chemoradiation before starting treatment. Chin. J. Cancer Res. 2015, 27, 221–230. [Google Scholar] [PubMed]
- Haisley, K.R.; Hart, K.D.; Nabavizadeh, N.; Bensch, K.G.; Vaccaro, G.M.; Thomas, C.R., Jr.; Schipper, P.H.; Hunter, J.G.; Dolan, J.P. Neoadjuvant chemoradiotherapy with concurrent cisplatin/5-fluorouracil is associated with increased pathologic complete response and improved survival compared to carboplatin/paclitaxel in patients with locally advanced esophageal cancer. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus ISDE 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Shao, M.S.; Wong, A.T.; Schwartz, D.; Weiner, J.P.; Schreiber, D. Definitive or preoperative chemoradiation therapy for esophageal cancer: Patterns of care and survival outcomes. Ann. Thorac. Surg. 2016, 101, 2148–2154. [Google Scholar] [CrossRef]
- Swisher, S.G.; Moughan, J.; Komaki, R.U.; Ajani, J.A.; Wu, T.T.; Hofstetter, W.L.; Konski, A.A.; Willett, C.G. Final results of NRG oncology RTOG 0246: An organ-preserving selective resection strategy in esophageal cancer patients treated with definitive chemoradiation. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2017, 12, 368–374. [Google Scholar] [CrossRef] [Green Version]
- Rawat, S.; Kumar, G.; Kakria, A.; Sharma, M.K.; Chauhan, D. Chemoradiotherapy in the management of locally advanced squamous cell carcinoma esophagus: Is surgical resection required? J. Gastrointest. Cancer 2013, 44, 277–284. [Google Scholar] [CrossRef]
- Teoh, A.Y.; Chiu, P.W.; Yeung, W.K.; Liu, S.Y.; Wong, S.K.; Ng, E.K. Long-term survival outcomes after definitive chemoradiation versus surgery in patients with resectable squamous carcinoma of the esophagus: Results from a randomized controlled trial. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. ESMO 2013, 24, 165–171. [Google Scholar] [CrossRef]
- Yoo, C.; Park, J.H.; Yoon, D.H.; Park, S.I.; Kim, H.R.; Kim, J.H.; Jung, H.Y.; Lee, G.H.; Choi, K.D.; Song, H.J.; et al. Salvage esophagectomy for locoregional failure after chemoradiotherapy in patients with advanced esophageal cancer. Ann. Thorac. Surg. 2012, 94, 1862–1868. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Gu, J.; Wu, T.T.; Swisher, S.G.; Liao, Z.; Correa, A.M.; Liu, J.; Etzel, C.J.; Amos, C.I.; Huang, M.; et al. Genetic variations in radiation and chemotherapy drug action pathways predict clinical outcomes in esophageal cancer. J. Clin. Oncol. 2006, 24, 3789–3798. [Google Scholar] [CrossRef] [PubMed]
- Adenis, A.; Tresch, E.; Dewas, S.; Romano, O.; Messager, M.; Amela, E.; Clisant, S.; Kramar, A.; Mariette, C.; Mirabel, X. Clinical complete responders to definite chemoradiation or radiation therapy for oesophageal cancer: Predictors of outcome. BMC Cancer 2013, 13, 413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, P.M.; Metzger, R.; Schaefer, H.; Baumgarten, F.; Vallbohmer, D.; Brabender, J.; Wolfgarten, E.; Bollschweiler, E.; Baldus, S.E.; Dienes, H.P.; et al. Response evaluation by endoscopy, rebiopsy, and endoscopic ultrasound does not accurately predict histopathologic regression after neoadjuvant chemoradiation for esophageal cancer. Ann. Surg. 2008, 248, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Jang, M.; Tarhan, Y.E.; Katagiri, T.; Sasa, M.; Miyoshi, Y.; Kalari, K.R.; Suman, V.J.; Weinshilboum, R.; Wang, L.; et al. Clonal expansion of antitumor T cells in breast cancer correlates with response to neoadjuvant chemotherapy. Int. J. Oncol. 2016, 49, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Dovedi, S.J.; Cheadle, E.J.; Popple, A.L.; Poon, E.; Morrow, M.; Stewart, R.; Yusko, E.C.; Sanders, C.M.; Vignali, M.; Emerson, R.O.; et al. Fractionated radiation therapy stimulates antitumor immunity mediated by both resident and infiltrating polyclonal T-cell Populations when combined with PD-1 blockade. Clin. Cancer Res. 2017, 23, 5514–5526. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Palashati, H.; Tan, Q.; Ku, W.; Miao, Y.; Xiong, H.; Lu, Z. Immediate and substantial evolution of T-cell repertoire in peripheral blood and tumor microenvironment of patients with esophageal squamous cell carcinoma treated with preoperative chemotherapy. Carcinogenesis 2018, 39, 1389–1398. [Google Scholar] [CrossRef]
- Chow, J.; Hoffend, N.C.; Abrams, S.I.; Schwaab, T.; Singh, A.K.; Muhitch, J.B. Radiation induces dynamic changes to the T cell repertoire in renal cell carcinoma patients. Proc. Natl. Acad. Sci. USA 2020, 117, 23721–23729. [Google Scholar] [CrossRef]
- Lim, Y.J.; Koh, J.; Kim, K.; Chie, E.K.; Kim, B.; Lee, K.B.; Jang, J.Y.; Kim, S.W.; Oh, D.Y.; Bang, Y.J.; et al. High ratio of programmed cell death protein 1 (PD-1)(+)/CD8(+) tumor-infiltrating lymphocytes identifies a poor prognostic subset of extrahepatic bile duct cancer undergoing surgery plus adjuvant chemoradiotherapy. Radiother. Oncol. 2015, 117, 165–170. [Google Scholar] [CrossRef]
- Jiang, Y.; Lo, A.W.I.; Wong, A.; Chen, W.; Wang, Y.; Lin, L.; Xu, J. Prognostic significance of tumor-infiltrating immune cells and PD-L1 expression in esophageal squamous cell carcinoma. Oncotarget 2017, 8, 30175–30189. [Google Scholar] [CrossRef]
- Fumet, J.D.; Richard, C.; Ledys, F.; Klopfenstein, Q.; Joubert, P.; Routy, B.; Truntzer, C.; Gagne, A.; Hamel, M.A.; Guimaraes, C.F.; et al. Prognostic and predictive role of CD8 and PD-L1 determination in lung tumor tissue of patients under anti-PD-1 therapy. Br. J. Cancer 2018, 119, 950–960. [Google Scholar] [CrossRef]
- Yoneda, K.; Kuwata, T.; Kanayama, M.; Mori, M.; Kawanami, T.; Yatera, K.; Ohguri, T.; Hisaoka, M.; Nakayama, T.; Tanaka, F. Alteration in tumoural PD-L1 expression and stromal CD8-positive tumour-infiltrating lymphocytes after concurrent chemo-radiotherapy for non-small cell lung cancer. Br. J. Cancer 2019, 121, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Gennen, K.; Kasmann, L.; Taugner, J.; Eze, C.; Karin, M.; Roengvoraphoj, O.; Neumann, J.; Tufman, A.; Orth, M.; Reu, S.; et al. Prognostic value of PD-L1 expression on tumor cells combined with CD8+ TIL density in patients with locally advanced non-small cell lung cancer treated with concurrent chemoradiotherapy. Radiat. Oncol. 2020, 15, 5. [Google Scholar] [CrossRef]
- Qian, D.; Wang, Y.; Zhao, G.; Cao, F.; Er, P.; Chen, X.; Cheng, J.; Zhang, W.; Li, X.; Zhang, B.; et al. Tumor Remission and Tumor-Infiltrating Lymphocytes During Chemoradiation Therapy: Predictive and Prognostic Markers in Locally Advanced Esophageal Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 319–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, N.; Kato, H.; Igaki, H.; Shinoda, M.; Ozawa, S.; Shimizu, H.; Nakamura, T.; Yabusaki, H.; Aoyama, N.; Kurita, A.; et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907). Ann. Surg. Oncol. 2012, 19, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Stahl, M.; Walz, M.K.; Stuschke, M.; Lehmann, N.; Meyer, H.J.; Riera-Knorrenschild, J.; Langer, P.; Engenhart-Cabillic, R.; Bitzer, M.; Konigsrainer, A.; et al. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J. Clin. Oncol. 2009, 27, 851–856. [Google Scholar] [CrossRef] [Green Version]
- Boffetta, P.; Hashibe, M. Alcohol and cancer. Lancet Oncol. 2006, 7, 149–156. [Google Scholar] [CrossRef]
- Pelucchi, C.; Gallus, S.; Garavello, W.; Bosetti, C.; La Vecchia, C. Alcohol and tobacco use, and cancer risk for upper aerodigestive tract and liver. Eur. J. Cancer Prev. 2008, 17, 340–344. [Google Scholar] [CrossRef]
- Khammanivong, A.; Anandharaj, A.; Qian, X.; Song, J.M.; Upadhyaya, P.; Balbo, S.; Bandyopadhyay, D.; Dickerson, E.B.; Hecht, S.S.; Kassie, F. Transcriptome profiling in oral cavity and esophagus tissues from (S)-N’-nitrosonornicotine-treated rats reveals candidate genes involved in human oral cavity and esophageal carcinogenesis. Mol. Carcinog. 2016, 55, 2168–2182. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zhang, B.; Sun, Z. Spectrum of EGFR aberrations and potential clinical implications: Insights from integrative pan-cancer analysis. Cancer Commun. 2020, 40, 43–59. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.S.; Mellman, I. Oncology meets immunology: The cancer-immunity cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Bernal-Estevez, D.; Sanchez, R.; Tejada, R.E.; Parra-Lopez, C. Chemotherapy and radiation therapy elicits tumor specific T cell responses in a breast cancer patient. BMC Cancer 2016, 16, 591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz-Pamplona, R.; Melas, M.; Maoz, A.; Schmit, S.L.; Rennert, H.; Lejbkowicz, F.; Greenson, J.K.; Sanjuan, X.; Lopez-Zambrano, M.; Alonso, M.H.; et al. Lymphocytic infiltration in stage II microsatellite stable colorectal tumors: A retrospective prognosis biomarker analysis. PLoS Med. 2020, 17, e1003292. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, E.; Yamashita, K.; Tanaka, T.; Sawada, R.; Sugita, Y.; Arimoto, A.; Fujita, M.; Takiguchi, G.; Matsuda, T.; Oshikiri, T.; et al. Neoadjuvant Chemotherapy Increases PD-L1 Expression and CD8(+) Tumor-infiltrating Lymphocytes in Esophageal Squamous Cell Carcinoma. Anticancer Res. 2019, 39, 4539–4548. [Google Scholar] [CrossRef] [PubMed]
- Keane, C.; Gould, C.; Jones, K.; Hamm, D.; Talaulikar, D.; Ellis, J.; Vari, F.; Birch, S.; Han, E.; Wood, P.; et al. The T-cell receptor repertoire influences the tumor microenvironment and is associated with survival in aggressive B-cell lymphoma. Clin. Cancer Res. 2017, 23, 1820–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schumacher, K.; Haensch, W.; Roefzaad, C.; Schlag, P.M. Prognostic significance of activated CD8(+) T cell infiltrations within esophageal carcinomas. Cancer Res. 2001, 61, 3932–3936. [Google Scholar]
- Tokito, T.; Azuma, K.; Kawahara, A.; Ishii, H.; Yamada, K.; Matsuo, N.; Kinoshita, T.; Mizukami, N.; Ono, H.; Kage, M.; et al. Predictive relevance of PD-L1 expression combined with CD8+ TIL density in stage III non-small cell lung cancer patients receiving concurrent chemoradiotherapy. Eur. J. Cancer 2016, 55, 7–14. [Google Scholar] [CrossRef]
- Troiano, G.; Rubini, C.; Togni, L.; Caponio, V.C.A.; Zhurakivska, K.; Santarelli, A.; Cirillo, N.; Lo Muzio, L.; Mascitti, M. The immune phenotype of tongue squamous cell carcinoma predicts early relapse and poor prognosis. Cancer Med. 2020, 9, 8333–8344. [Google Scholar] [CrossRef]
- Chen, Y.; Lu, Y.; Wang, Y.; Yang, H.; Xia, Y.; Chen, M.; Song, H.; Li, T.; Li, D.; Wang, J.; et al. Comparison of salvage chemoradiation versus salvage surgery for recurrent esophageal squamous cell carcinoma after definitive radiochemotherapy or radiotherapy alone. Dis. Esophagus Off. J. Int. Soc. Dis. Esophagus ISDE 2014, 27, 134–140. [Google Scholar] [CrossRef]
- Kitaura, K.; Shini, T.; Matsutani, T.; Suzuki, R. A new high-throughput sequencing method for determining diversity and similarity of T cell receptor (TCR) alpha and beta repertoires and identifying potential new invariant TCR alpha chains. BMC Immunol. 2016, 17, 38. [Google Scholar] [CrossRef] [Green Version]
- Hassan, S.S.; Akram, M.; King, E.C.; Dockrell, H.M.; Cliff, J.M. PD-1, PD-L1 and PD-L2 gene expression on T-cells and natural killer cells declines in conjunction with a reduction in PD-1 protein during the intensive phase of tuberculosis treatment. PLoS ONE 2015, 10, e0137646. [Google Scholar] [CrossRef]
- Carey, A.J.; Hope, J.L.; Mueller, Y.M.; Fike, A.J.; Kumova, O.K.; van Zessen, D.B.H.; Steegers, E.A.P.; van der Burg, M.; Katsikis, P.D. Public clonotypes and convergent recombination characterize the naive CD8(+) T-cell receptor repertoire of extremely preterm neonates. Front. Immunol. 2017, 8, 1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | First-Line Therapy | Radiation Dose (gy) | Concurrent Chemotherapy | fTNM | Prognosis After Salvage Esophagectomy | ||
|---|---|---|---|---|---|---|---|
| Cancer Recurrence | Prognosis | Recurrence-Free Survival (Months) | |||||
| ESCC | CRT | 60 | CDDP+5-FU | T2N1M0 | yes | cancer death | 18.4 |
| ESCC | CRT | 60 | CDDP+5-FU | T2N1M0 | no | survive | 22.9 |
| ESCC | CRT | 60 | CDDP+5-FU | T3N0M0 | no | survive | 74.1 |
| ESCC | CRT | 60 | CDDP+5-FU | T4N1M0 | yes | cancer death | 6.6 |
| ESCC | surgery alone | 0 | no | T2N1M0 | no | survive | 117.7 |
| ESCC | surgery alone | 0 | no | T3N0M0 | no | died from other disease | 67.2 |
| ESCC | CRT | 60 | CDDP+5-FU | T3N0M0 | yes | cancer death | 9.5 |
| OSCC | surgery alone | 0 | no | T2N0M0 | |||
| OSCC | surgery alone | 0 | no | T1N1M0 | |||
| OSCC | surgery alone | 0 | no | T2N2bM0 | |||
| OSCC | surgery alone | 0 | no | T2N1M0 | |||
| OSCC | surgery alone | 0 | no | T4aN0M0 | |||
| OSCC | surgery alone | 0 | no | T4aN3bM1 | |||
| OSCC | surgery alone | 0 | no | T1N1M0 | |||
| OSCC | surgery alone | 0 | no | T4N1M0 | |||
| OSCC | surgery alone | 0 | no | T1N1M0 | |||
| OSCC | surgery alone | 0 | no | T3N0M0 | |||
| OSCC | surgery alone | 0 | no | T1N1M0 | |||
| OSCC | surgery alone | 0 | no | T2N2bM0 | |||
| OSCC | surgery alone | 0 | no | T3N0M0 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, T.; Kumagai, K.; Nasu, K.; Yoshizawa, T.; Kuwano, K.; Hamada, Y.; Kanazawa, H.; Suzuki, R. Clonal Expansion of Tumor-Infiltrating T Cells and Analysis of the Tumor Microenvironment within Esophageal Squamous Cell Carcinoma Relapsed after Definitive Chemoradiation Therapy. Int. J. Mol. Sci. 2021, 22, 1098. https://doi.org/10.3390/ijms22031098
Mori T, Kumagai K, Nasu K, Yoshizawa T, Kuwano K, Hamada Y, Kanazawa H, Suzuki R. Clonal Expansion of Tumor-Infiltrating T Cells and Analysis of the Tumor Microenvironment within Esophageal Squamous Cell Carcinoma Relapsed after Definitive Chemoradiation Therapy. International Journal of Molecular Sciences. 2021; 22(3):1098. https://doi.org/10.3390/ijms22031098
Chicago/Turabian StyleMori, Takahiro, Kenichi Kumagai, Keisuke Nasu, Takamasa Yoshizawa, Koji Kuwano, Yoshiki Hamada, Hideki Kanazawa, and Ryuji Suzuki. 2021. "Clonal Expansion of Tumor-Infiltrating T Cells and Analysis of the Tumor Microenvironment within Esophageal Squamous Cell Carcinoma Relapsed after Definitive Chemoradiation Therapy" International Journal of Molecular Sciences 22, no. 3: 1098. https://doi.org/10.3390/ijms22031098