Synergistic Anticancer Activity of N-Hydroxy-7-(2-Naphthylthio) Heptanomide, Sorafenib, and Radiation Therapy in Patient-Derived Anaplastic Thyroid Cancer Models

 , ,
, ,
Abstract
:1. Introduction
2. Results
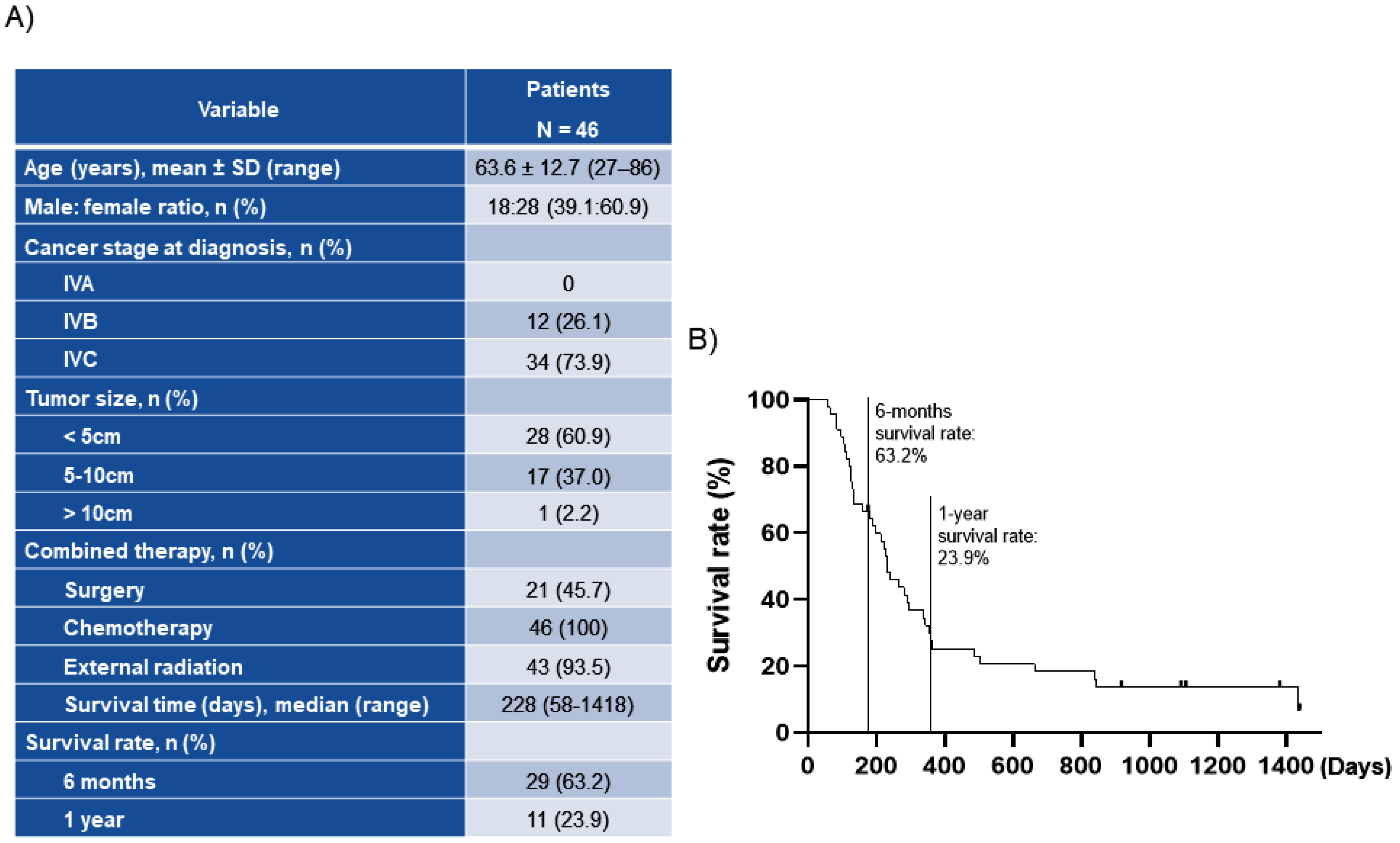
2.1. Patient Disease Characteristics
2.2. Characteristics of Patient-Derived Thyroid Cancer Cell Lines
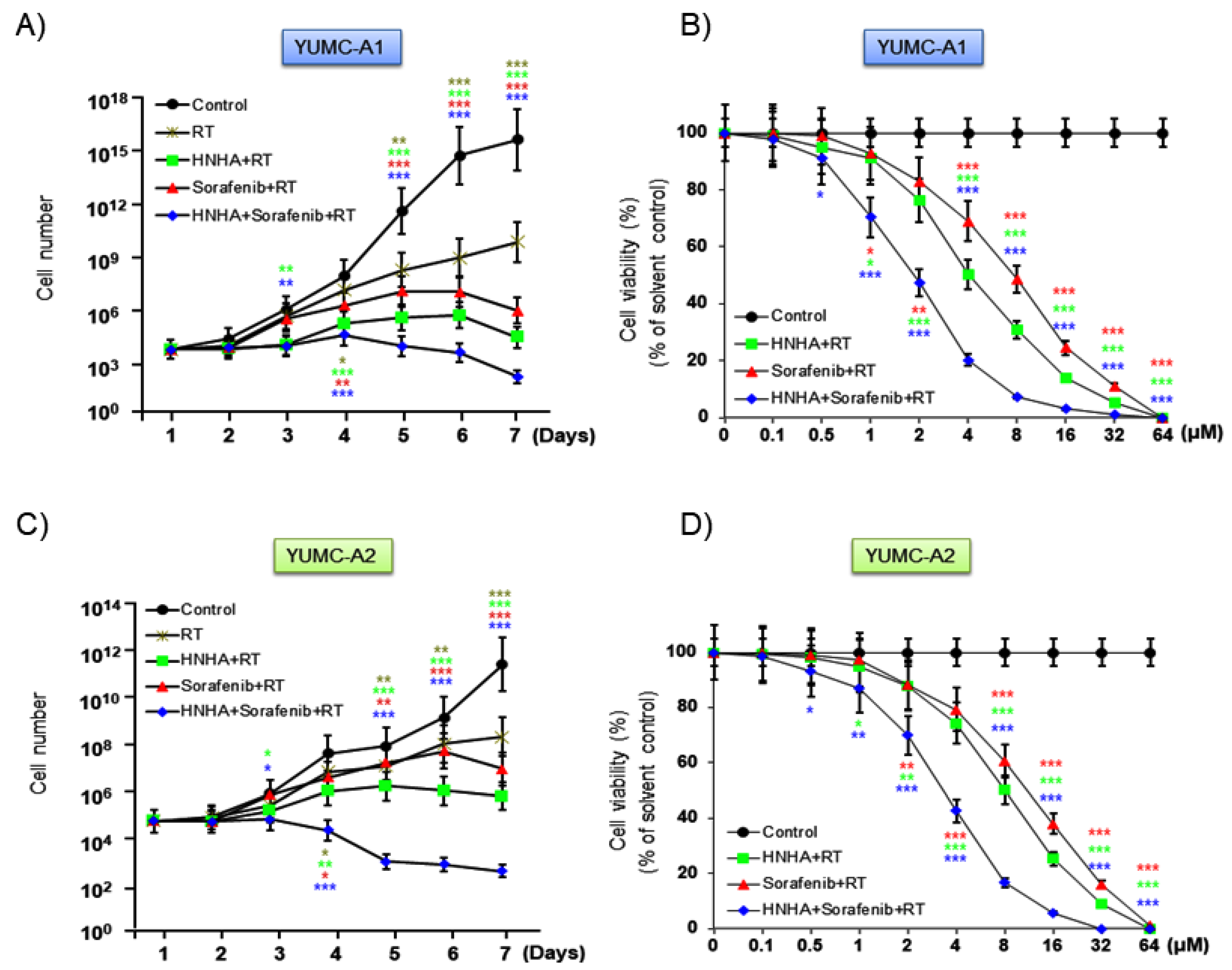
2.3. Combination of HNHA and Sorafenib with Radiation Was More Effective Than Either HNHA or Sorafenib with Radiation
2.4. Combination of HNHA and Sorafenib with Radiation Was More Effective in Inducing Apoptosis and Cell Cycle Arrest in YUMC-A1 and YUMC-A2 Than HNHA or Sorafenib with Radiation
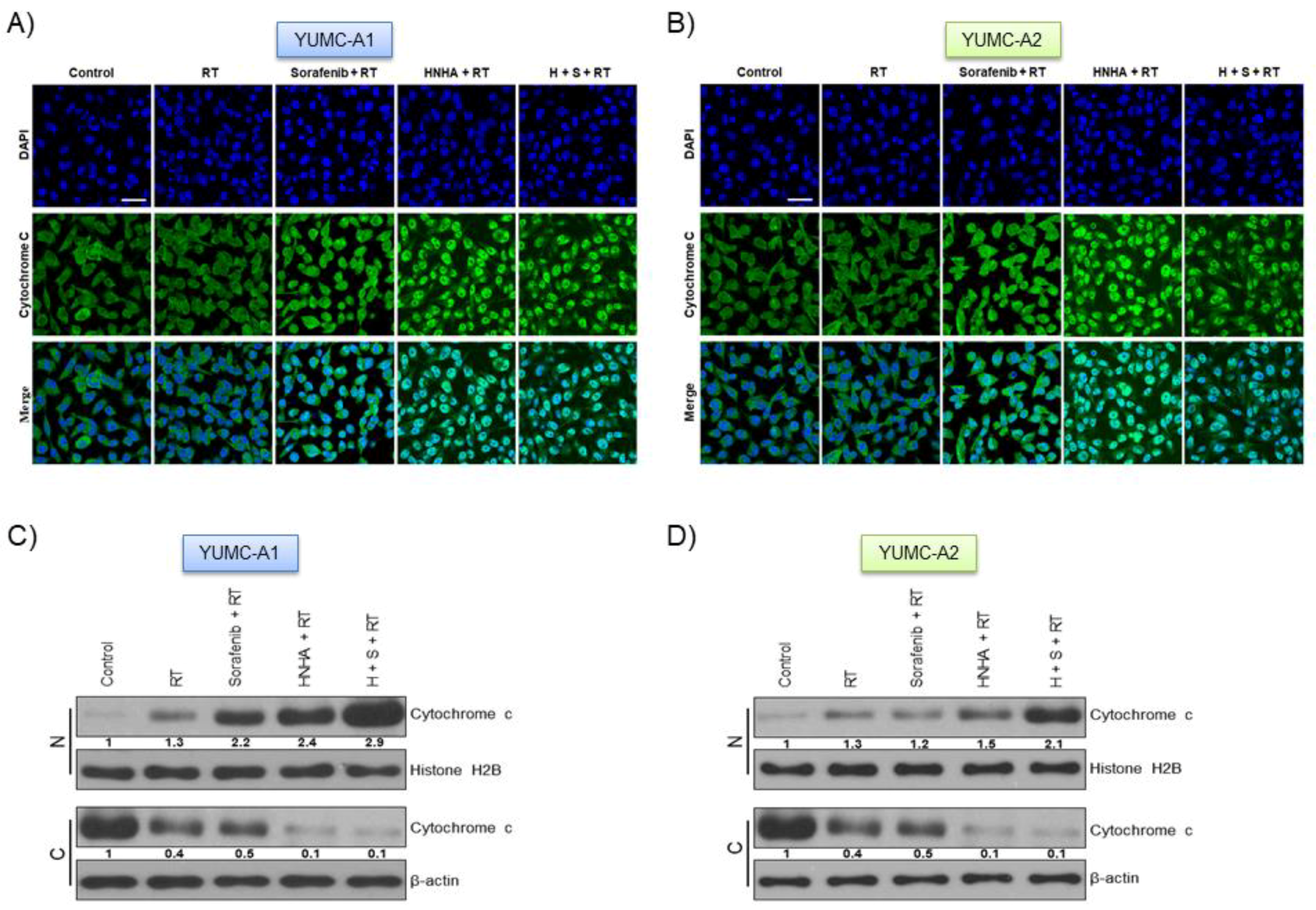
2.5. Combination of HNHA, Sorafenib, and Radiation Induced Cytochrome c Release from Mitochondria and Translocation from the Cytoplasm to the Nucleus in ATC Cells
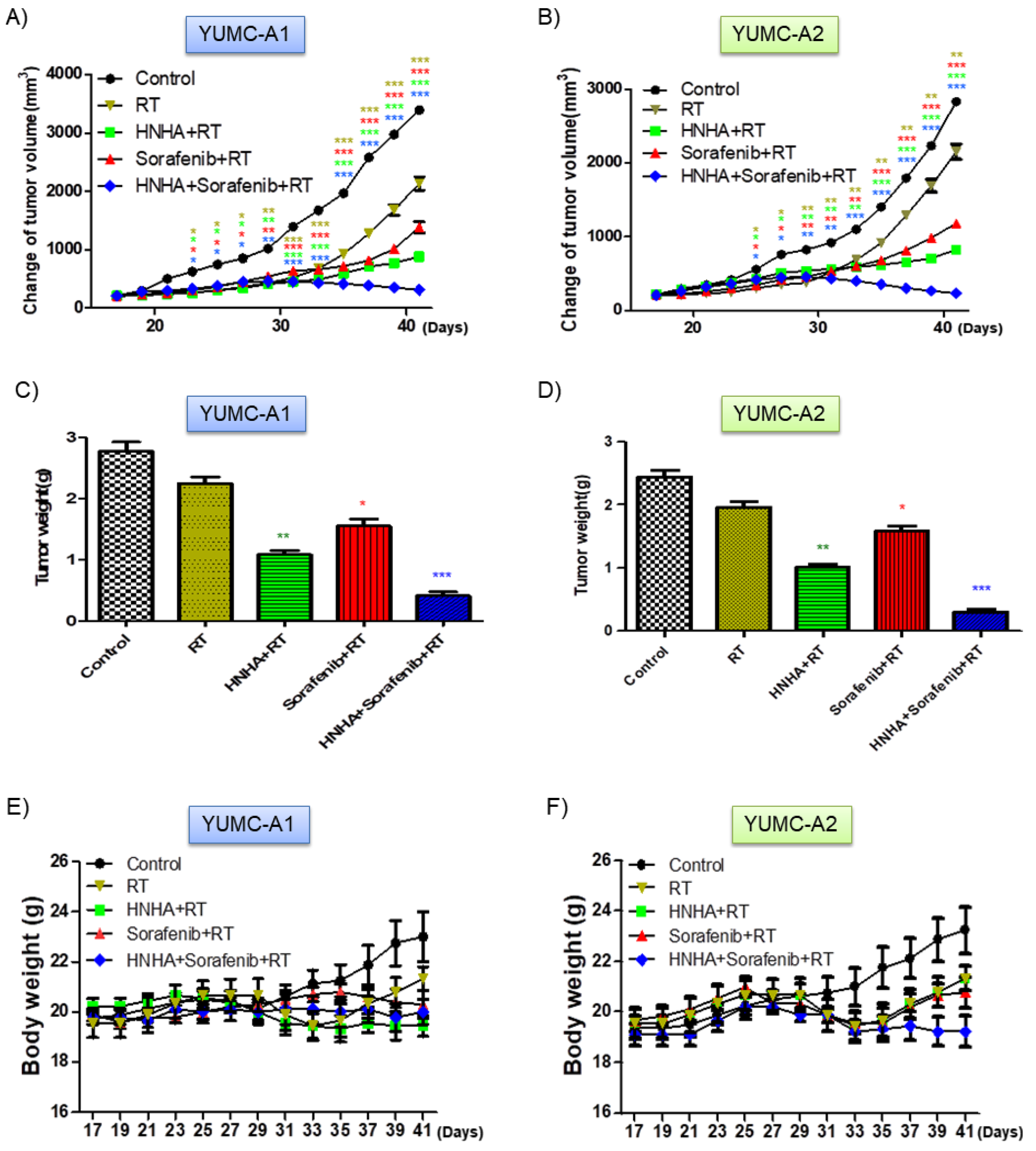
2.6. Combination of HNHA, Sorafenib, and Radiation Significantly Suppressed Tumor Growth in a Mouse Xenograft Model
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patients
4.3. Tissue Specimens
4.4. Ethical Considerations
4.5. Statistical Analysis
4.6. Tumor Cell Isolation and Primary Culture
4.7. Preparation of DNA
4.8. Preparation of Libraries
4.9. Analysis of DNA Sequences
4.10. Cell Culture
4.11. Cell Viability Assay
4.12. Irradiation
4.13. Flow Cytometry Analysis of Cell Cycle
4.14. Immunofluorescence Analysis and Confocal Imaging
4.15. Cellular Fractionation
4.16. Immunoblot Analysis
4.17. Human Thyroid Cancer Cell Xenograft
4.18. Immunohistochemistry
4.19. Statistical Analysis
4.20. Image Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HNHA | N-hydroxy-7-(2-naphthylthio) heptanomide |
| EMT | Epithelial–Mesenchymal Transition |
| FGFR | Fibroblast Growth Factor Receptor |
| IRB | Institutional Review Board |
| RPMI | Roswell Park Memorial Institute |
| FBS | Fetal Bovine Serum |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide |
| PBS | Phosphate-Buffered Saline |
References
- Kohrle, J. Thyroid hormones and derivatives: Endogenous thyroid hormones and their targets. Methods Mol. Biol. 2018, 1801, 85–104. [Google Scholar]
- Jabbar, A.; Pingitore, A.; Pearce, S.H.; Zaman, A.; Iervasi, G.; Razvi, S. Thyroid hormones and cardiovascular disease. Nat. Rev. Cardiol. 2017, 14, 39–55. [Google Scholar] [CrossRef] [PubMed]
- Accorroni, A.; Chiellini, G.; Origlia, N. Effects of thyroid hormones and their metabolites on learning and memory in normal and pathological conditions. Curr. Drug Metab. 2017, 18, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; McFadden, D.G.; Durante, C. Thyroid cancer. Lancet 2016, 388, 2783–2795. [Google Scholar] [CrossRef]
- Sherman, S.I. Thyroid carcinoma. Lancet 2003, 361, 501–511. [Google Scholar] [CrossRef]
- Schlumberger, M.J. Papillary and follicular thyroid carcinoma. N. Engl. J. Med. 1998, 338, 297–306. [Google Scholar] [CrossRef]
- Schlumberger, M.J.; Torlantano, M. Papillary and follicular thyroid carcinoma. Bailliere’s Best Pract. Res. Clin. Endocrinol. Metab. 2000, 14, 601–613. [Google Scholar] [CrossRef] [Green Version]
- Smallridge, R.C. Approach to the patient with anaplastic thyroid carcinoma. J. Clin. Endocrinol. Metab. 2012, 97, 2566–2572. [Google Scholar] [CrossRef] [Green Version]
- Giuffrida, D.; Gharib, H. Anaplastic thyroid carcinoma: Current diagnosis and treatment. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2000, 11, 1083–1089. [Google Scholar] [CrossRef]
- Saini, S.; Tulla, K.; Maker, A.V.; Burman, K.D.; Prabhakar, B.S. Therapeutic advances in anaplastic thyroid cancer: A current perspective. Mol. Cancer 2018, 17, 154. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, V.R.; Hreno, J.; Patil, T.; Bowles, D.W. New therapies for anaplastic thyroid cancer. Drugs Today 2018, 54, 695–704. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.P.; Shaha, A.R. Anaplastic thyroid cancer. Oral Oncol. 2013, 49, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; Ferrarotto, R.; Garden, A.S.; Ahmed, S.; Busaidy, N.L.; Dadu, R.; Williams, M.D.; Skinner, H.; Gunn, G.B.; Grosu, H.; et al. Neoadjuvant braf- and immune-directed therapy for anaplastic thyroid carcinoma. Thyroid Off. J. Am. Thyroid Assoc. 2018, 28, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Pasieka, J.L. Anaplastic thyroid cancer. Curr. Opin. Oncol. 2003, 15, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Bernet, V.; Smallridge, R. New therapeutic options for advanced forms of thyroid cancer. Expert Opin. Emerg. Drugs 2014, 19, 225–241. [Google Scholar] [CrossRef]
- Ma, R.; Minsky, N.; Morshed, S.A.; Davies, T.F. Stemness in human thyroid cancers and derived cell lines: The role of asymmetrically dividing cancer stem cells resistant to chemotherapy. J. Clin. Endocrinol. Metab. 2014, 99, E400–E409. [Google Scholar] [CrossRef]
- Chen, C.H.; Chen, M.C.; Wang, J.C.; Tsai, A.C.; Chen, C.S.; Liou, J.P.; Pan, S.L.; Teng, C.M. Synergistic interaction between the hdac inhibitor, mpt0e028, and sorafenib in liver cancer cells in vitro and in vivo. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 1274–1287. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.; Yacoub, A.; Hamed, H.A.; Poklepovic, A.; Tye, G.; Grant, S.; Dent, P. Sorafenib and hdac inhibitors synergize to kill cns tumor cells. Cancer Biol. Ther. 2012, 13, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Suraweera, A.; O’Byrne, K.J.; Richard, D.J. Combination therapy with histone deacetylase inhibitors (hdaci) for the treatment of cancer: Achieving the full therapeutic potential of hdaci. Front. Oncol. 2018, 8, 92. [Google Scholar] [CrossRef] [Green Version]
- West, A.C.; Johnstone, R.W. New and emerging hdac inhibitors for cancer treatment. J. Clin. Investig. 2014, 124, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Bolden, J.E.; Shi, W.; Jankowski, K.; Kan, C.Y.; Cluse, L.; Martin, B.P.; MacKenzie, K.L.; Smyth, G.K.; Johnstone, R.W. Hdac inhibitors induce tumor-cell-selective pro-apoptotic transcriptional responses. Cell Death Dis. 2013, 4, e519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banik, D.; Moufarrij, S.; Villagra, A. Immunoepigenetics combination therapies: An overview of the role of hdacs in cancer immunotherapy. Int. J. Mol. Sci. 2019, 20, 2241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceccacci, E.; Minucci, S. Inhibition of histone deacetylases in cancer therapy: Lessons from leukaemia. Br. J. Cancer 2016, 114, 605–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.C.; Kim, S.M.; Jeon, J.Y.; Kim, B.W.; Kim, H.K.; Chang, H.J.; Lee, Y.S.; Kim, S.Y.; Choi, S.H.; Park, C.S.; et al. Synergistic activity of n-hydroxy-7-(2-naphthylthio) heptanomide and sorafenib against cancer stem cells, anaplastic thyroid cancer. Neoplasia 2017, 19, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Park, K.C.; Jeon, J.Y.; Kim, B.W.; Kim, H.K.; Chang, H.J.; Choi, S.H.; Park, C.S.; Chang, H.S. Potential anti-cancer effect of n-hydroxy-7-(2-naphthylthio) heptanomide (hnha), a novel histone deacetylase inhibitor, for the treatment of thyroid cancer. BMC Cancer 2015, 15, 1003. [Google Scholar] [CrossRef] [Green Version]
- Park, K.C.; Heo, J.H.; Jeon, J.Y.; Choi, H.J.; Jo, A.R.; Kim, S.W.; Kwon, H.J.; Hong, S.J.; Han, K.S. The novel histone deacetylase inhibitor, n-hydroxy-7-(2-naphthylthio) hepatonomide, exhibits potent antitumor activity due to cytochrome-c-release-mediated apoptosis in renal cell carcinoma cells. BMC Cancer 2015, 15, 19. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Shi, Y.; Xing, P.; Wang, L.; Feng, Y.; Han, X.; He, X. Sorafenib in metastatic radioactive iodine-refractory differentiated thyroid cancer: A pilot study. Mol. Clin. Oncol. 2014, 2, 87–92. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Adnane, L.; Newell, P.; Villanueva, A.; Llovet, J.M.; Lynch, M. Preclinical overview of sorafenib, a multikinase inhibitor that targets both raf and vegf and pdgf receptor tyrosine kinase signaling. Mol. Cancer Ther. 2008, 7, 3129–3140. [Google Scholar] [CrossRef] [Green Version]
- Gounder, M.M.; Mahoney, M.R.; Van Tine, B.A.; Ravi, V.; Attia, S.; Deshpande, H.A.; Gupta, A.A.; Milhem, M.M.; Conry, R.M.; Movva, S.; et al. Sorafenib for advanced and refractory desmoid tumors. N. Engl. J. Med. 2018, 379, 2417–2428. [Google Scholar] [CrossRef]
- Chen, M.; Neul, C.; Schaeffeler, E.; Frisch, F.; Winter, S.; Schwab, M.; Koepsell, H.; Hu, S.; Laufer, S.; Baker, S.D.; et al. Sorafenib activity and disposition in liver cancer does not depend on organic cation transporter 1. Clin. Pharmacol. Ther. 2020, 107, 227–237. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, S.M.; Chang, H.J.; Kim, B.W.; Lee, Y.S.; Park, C.S.; Park, K.C.; Chang, H.S. Solat (sorafenib lenvatinib alternating treatment): A new treatment protocol with alternating sorafenib and lenvatinib for refractory thyroid cancer. BMC Cancer 2018, 18, 956. [Google Scholar] [CrossRef] [Green Version]
- Pitoia, F.; Jerkovich, F. Selective use of sorafenib in the treatment of thyroid cancer. Drug Des. Dev. Ther. 2016, 10, 1119–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norbury, C.J.; Zhivotovsky, B. DNA damage-induced apoptosis. Oncogene 2004, 23, 2797–2808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kweon, S.S.; Shin, M.H.; Chung, I.J.; Kim, Y.J.; Choi, J.S. Thyroid cancer is the most common cancer in women, based on the data from population-based cancer registries, south korea. Jpn. J. Clin. Oncol. 2013, 43, 1039–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: Globocan 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Oh, C.M.; Lee, D.H.; Lee, J.S. Cancer statistics in korea: Incidence, mortality, survival, and prevalence in 2011. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2014, 46, 109–123. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.W.; No, J.H.; Chung, J.H.; Min, Y.K.; Lee, M.S.; Lee, M.K.; Yang, J.H.; Kim, K.W. Prevalence, clinical and ultrasonographic characteristics of thyroid incidentalomas. Thyroid Off. J. Am. Thyroid Assoc. 2004, 14, 29–33. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the united states. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Han, M.A.; Choi, K.S.; Lee, H.Y.; Kim, Y.; Jun, J.K.; Park, E.C. Current status of thyroid cancer screening in korea: Results from a nationwide interview survey. Asian Pac. J. Cancer Prev. 2011, 12, 1657–1663. [Google Scholar]
- Keutgen, X.M.; Sadowski, S.M.; Kebebew, E. Management of anaplastic thyroid cancer. Gland Surg. 2015, 4, 44–51. [Google Scholar]
- Soares, P.; Lima, J.; Preto, A.; Castro, P.; Vinagre, J.; Celestino, R.; Couto, J.P.; Prazeres, H.; Eloy, C.; Maximo, V.; et al. Genetic alterations in poorly differentiated and undifferentiated thyroid carcinomas. Curr. Genom. 2011, 12, 609–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, B.; Ma, H.; Ma, M.; Zhang, Z.; Sun, Z.; Hsieh, I.Y.; Okenwa, O.; Guan, H.; Li, J.; Lv, W. The incidence and survival analysis for anaplastic thyroid cancer: A seer database analysis. Am. J. Transl. Res. 2019, 11, 5888–5896. [Google Scholar] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 american thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid Off. J. Am. Thyroid Assoc. 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, C.; Hu, W.; He, Y.; Zhang, Y.; Zhang, G.; Xu, Y.; Tang, J. Cytokine-mediated therapeutic resistance in breast cancer. Cytokine 2018, 108, 151–159. [Google Scholar] [CrossRef]
- Aiello, N.M.; Kang, Y. Context-dependent emt programs in cancer metastasis. J. Exp. Med. 2019, 216, 1016–1026. [Google Scholar] [CrossRef] [Green Version]
- Wade, C.A.; Kyprianou, N. Profiling prostate cancer therapeutic resistance. Int. J. Mol. Sci. 2018, 19, 904. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.C. Cancer stem cells: Role in tumor growth, recurrence, metastasis, and treatment resistance. Medicine 2016, 95, S20–S25. [Google Scholar] [CrossRef]
- Lee, Y.S.; Kim, S.M.; Kim, B.W.; Chang, H.J.; Kim, S.Y.; Park, C.S.; Park, K.C.; Chang, H.S. Anti-cancer effects of hnha and lenvatinib by the suppression of emt-mediated drug resistance in cancer stem cells. Neoplasia 2018, 20, 197–206. [Google Scholar] [CrossRef]
- Ramakrishnan, V.; Timm, M.; Haug, J.L.; Kimlinger, T.K.; Wellik, L.E.; Witzig, T.E.; Rajkumar, S.V.; Adjei, A.A.; Kumar, S. Sorafenib, a dual raf kinase/vascular endothelial growth factor receptor inhibitor has significant anti-myeloma activity and synergizes with common anti-myeloma drugs. Oncogene 2010, 29, 1190–1202. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Cao, Y.; Chen, C.; Zhang, X.; McNabola, A.; Wilkie, D.; Wilhelm, S.; Lynch, M.; Carter, C. Sorafenib blocks the raf/mek/erk pathway, inhibits tumor angiogenesis, and induces tumor cell apoptosis in hepatocellular carcinoma model plc/prf/5. Cancer Res. 2006, 66, 11851–11858. [Google Scholar] [CrossRef] [Green Version]
- Miyanaga, N.; Akaza, H. Sorafenib(nexavar). Gan Kagaku Ryoho. Cancer Chemother. 2009, 36, 1029–1033. [Google Scholar]
- Wilhelm, S.; Carter, C.; Lynch, M.; Lowinger, T.; Dumas, J.; Smith, R.A.; Schwartz, B.; Simantov, R.; Kelley, S. Discovery and development of sorafenib: A multikinase inhibitor for treating cancer. Nat. Rev. Drug Discov. 2006, 5, 835–844. [Google Scholar] [CrossRef] [PubMed]
- White, P.T.; Cohen, M.S. The discovery and development of sorafenib for the treatment of thyroid cancer. Expert Opin. Drug Discov. 2015, 10, 427–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gui, C.Y.; Ngo, L.; Xu, W.S.; Richon, V.M.; Marks, P.A. Histone deacetylase (hdac) inhibitor activation of p21waf1 involves changes in promoter-associated proteins, including hdac1. Proc. Natl. Acad. Sci. USA 2004, 101, 1241–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almenara, J.; Rosato, R.; Grant, S. Synergistic induction of mitochondrial damage and apoptosis in human leukemia cells by flavopiridol and the histone deacetylase inhibitor suberoylanilide hydroxamic acid (saha). Leukemia 2002, 16, 1331–1343. [Google Scholar] [CrossRef]
- Inoue, H.; Hwang, S.H.; Wecksler, A.T.; Hammock, B.D.; Weiss, R.H. Sorafenib attenuates p21 in kidney cancer cells and augments cell death in combination with DNA-damaging chemotherapy. Cancer Biol. Ther. 2011, 12, 827–836. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Fujita, N.; Tsuruo, T. Caspase-mediated cleavage of p21waf1/cip1 converts cancer cells from growth arrest to undergoing apoptosis. Oncogene 1999, 18, 1131–1138. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.; Armour, E.; Kazanzides, P.; Iordachita, I.; Tryggestad, E.; Deng, H.; Matinfar, M.; Kennedy, C.; Liu, Z.; Chan, T.; et al. High-resolution, small animal radiation research platform with x-ray tomographic guidance capabilities. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1591–1599. [Google Scholar] [CrossRef] [Green Version]
- Cibulskis, K.; Lawrence, M.S.; Carter, S.L.; Sivachenko, A.; Jaffe, D.; Sougnez, C.; Gabriel, S.; Meyerson, M.; Lander, E.S.; Getz, G. Sensitive detection of somatic point mutations in impure and heterogeneous cancer samples. Nat. Biotechnol. 2013, 31, 213–219. [Google Scholar] [CrossRef]
- Narzisi, G.; Corvelo, A.; Arora, K.; Bergmann, E.A.; Shah, M.; Musunuri, R.; Emde, A.K.; Robine, N.; Vacic, V.; Zody, M.C. Genome-wide somatic variant calling using localized colored de bruijn graphs. Commun. Biol. 2018, 1, 20. [Google Scholar] [CrossRef] [Green Version]
- Callari, M.; Sammut, S.J.; De Mattos-Arruda, L.; Bruna, A.; Rueda, O.M.; Chin, S.F.; Caldas, C. Intersect-then-combine approach: Improving the performance of somatic variant calling in whole exome sequencing data using multiple aligners and callers. Genome Med. 2017, 9, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.H.; Choi, K.H.; Kim, S.Y.; Park, C.S.; Kim, S.M.; Park, K.C. Patient-derived, drug-resistant colon cancer cells evade chemotherapeutic drug effects via the induction of epithelial-mesenchymal transition-mediated angiogenesis. Int. J. Mol. Sci. 2020, 21, 7469. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Line | Hisopathology | Animal | Cell Proliferation IC50 (μM) | ||||
|---|---|---|---|---|---|---|---|
| HNHA | Sorafenib | HNHA + RT | Sorafenib + RT | HNHA + Sorafenib + RT | |||
| YUMC-A1 | Thryoid, anaplastic | Human | 16.19 (±0.6) | 10.17 (±0.6) | 6.71 (±0.1) | 7.12 (±0.9) | 2.74 (±0.6) * |
| YUMC-A2 | Thyroid, anaplastic | Human | 18.16 (±0.4) | 12.14 (±0.5) | 8.14 (±1.3) | 10.33 (±0.7) | 4.08 (±0.2) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, H.J.; Kim, H.J.; Kim, J.; Kim, S.Y.; Chang, H.-S.; Park, C.S.; Chang, H.-J.; Park, K.C. Synergistic Anticancer Activity of N-Hydroxy-7-(2-Naphthylthio) Heptanomide, Sorafenib, and Radiation Therapy in Patient-Derived Anaplastic Thyroid Cancer Models. Int. J. Mol. Sci. 2021, 22, 536. https://doi.org/10.3390/ijms22020536
Yun HJ, Kim HJ, Kim J, Kim SY, Chang H-S, Park CS, Chang H-J, Park KC. Synergistic Anticancer Activity of N-Hydroxy-7-(2-Naphthylthio) Heptanomide, Sorafenib, and Radiation Therapy in Patient-Derived Anaplastic Thyroid Cancer Models. International Journal of Molecular Sciences. 2021; 22(2):536. https://doi.org/10.3390/ijms22020536
Chicago/Turabian StyleYun, Hyeok Jun, Hee Jun Kim, Jungmin Kim, Sang Yong Kim, Hang-Seok Chang, Cheong Soo Park, Ho-Jin Chang, and Ki Cheong Park. 2021. "Synergistic Anticancer Activity of N-Hydroxy-7-(2-Naphthylthio) Heptanomide, Sorafenib, and Radiation Therapy in Patient-Derived Anaplastic Thyroid Cancer Models" International Journal of Molecular Sciences 22, no. 2: 536. https://doi.org/10.3390/ijms22020536