Circulating MicroRNAs as Novel Biomarkers for Osteoporosis and Fragility Fracture Risk: Is There a Use in Assessment Risk?

 , ,
, ,
Abstract
:1. Introduction
2. Aim
3. C-miRs in OP
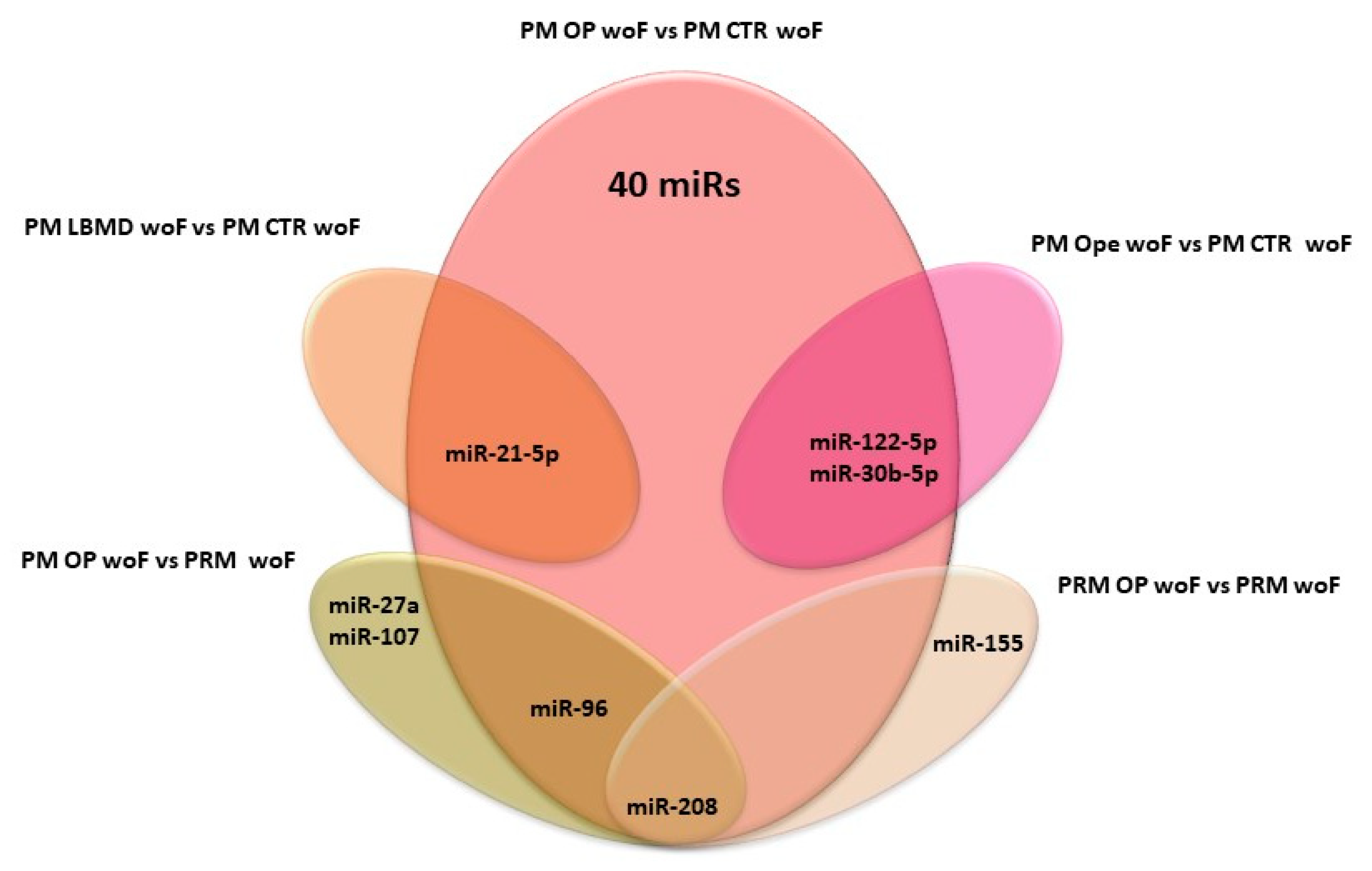
3.1. C-miR Signatures in OP/Ope woF
3.1.1. PM OP/Ope vs. PM CTRs
3.1.2. PM OP vs. PRM CTRs
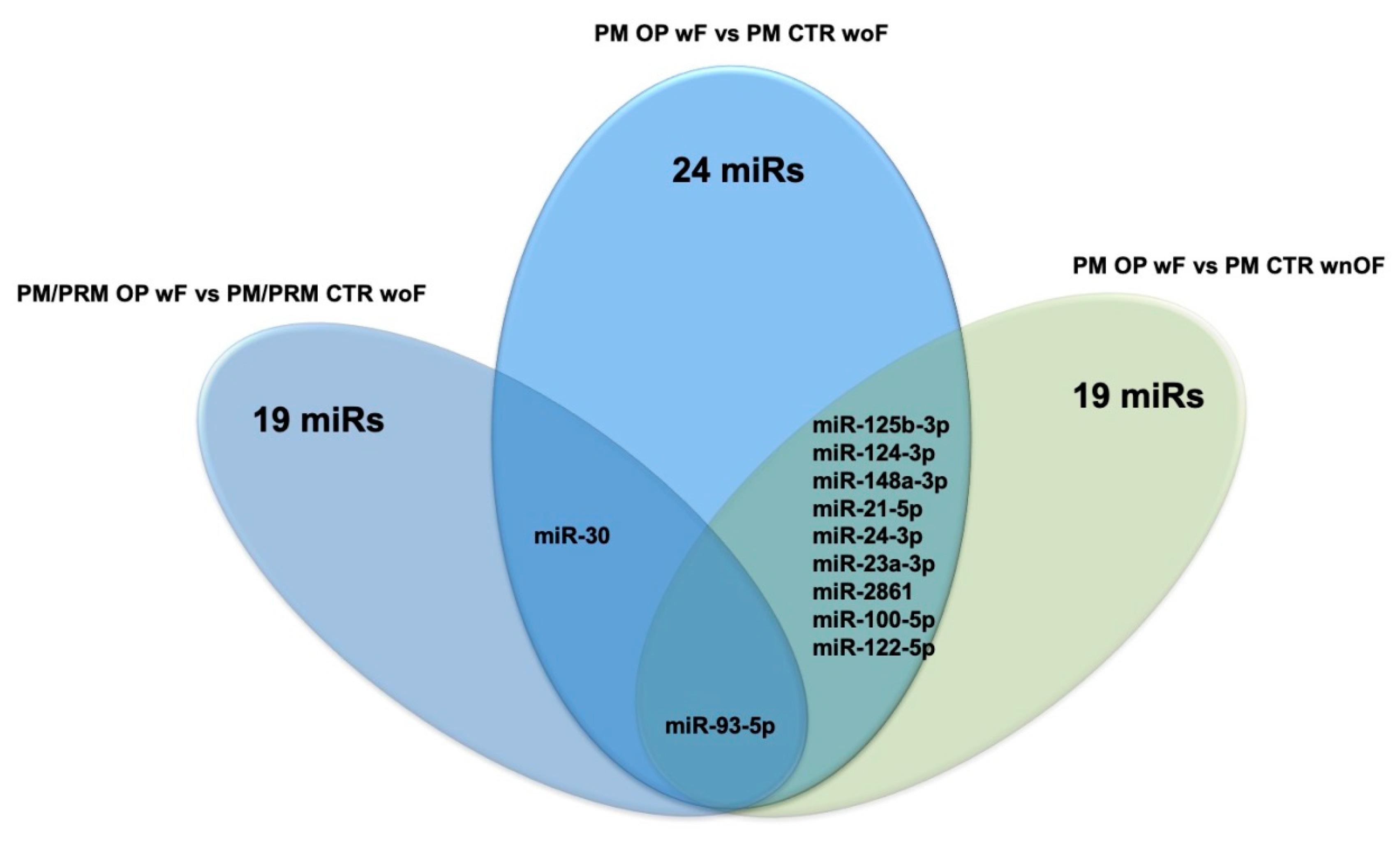
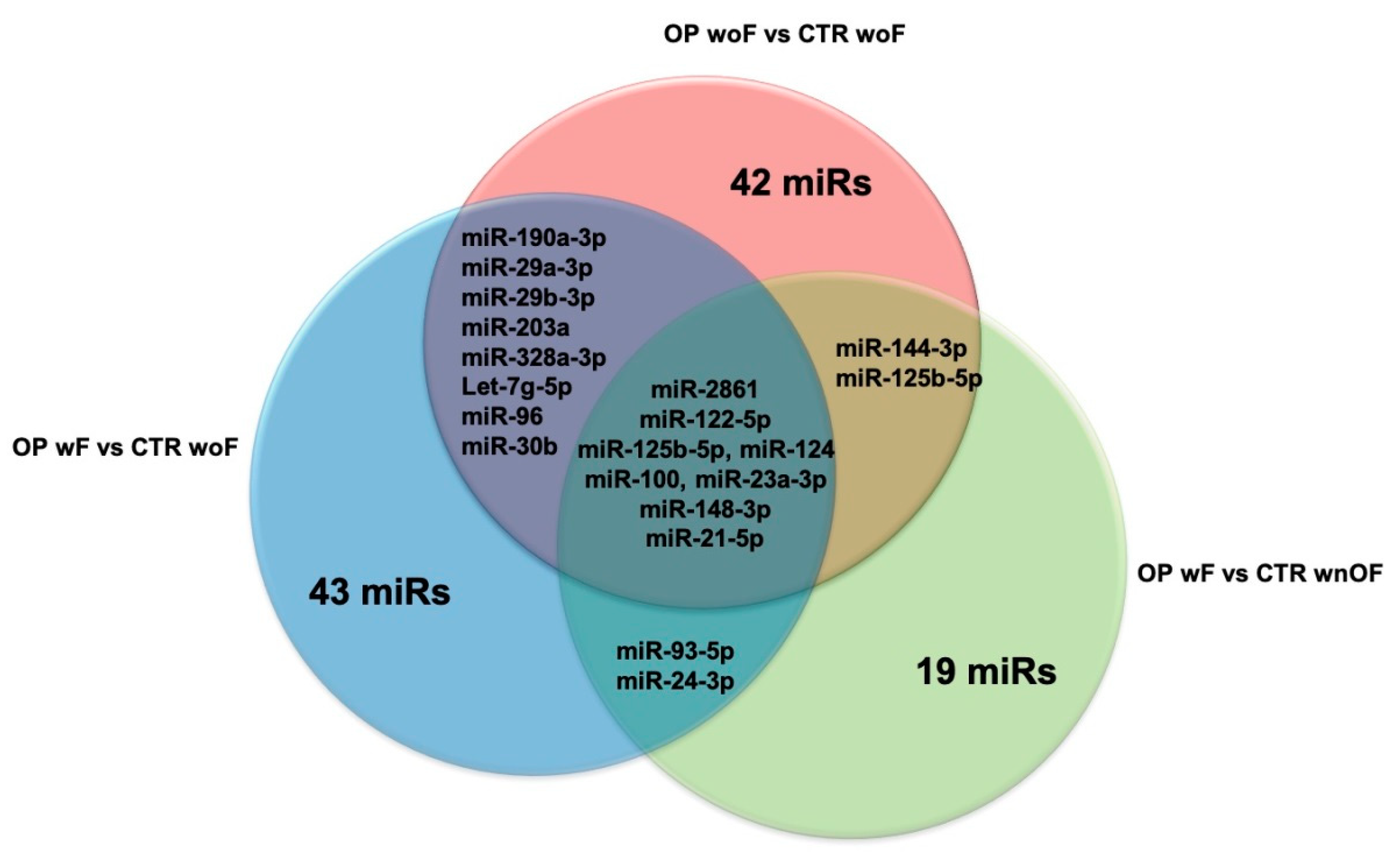
3.2. C-miR Signatures in OP wF
3.2.1. OP wF vs. CTR woF
3.2.2. OP wF vs. CTR wnOF
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BALP | Bone phosphatase alkaline |
| BMD | Bone mineral mass |
| CTRs | Controls |
| CTx | C-terminal type I collagen crosslinks |
| DXA | Dual energy X-ray absorptiometry |
| FRAX-H | 10-year probability of a hip osteoporotic fracture |
| FRAX-M | 10-year probability of a major osteoporotic fracture |
| hBMSCs | Human bone marrow stem cells |
| LD | Linear dichroism |
| OBs | Osteoblast cells |
| OCs | Osteoclast cells |
| OP | Osteoporosis |
| Ope | Osteopenia |
| OVX | Ovariectomy |
| PIPN | Type I pro-collagen pro-peptide |
| PM | Post-menopausal |
| PRM | Pre-menopausal |
| PTH | Parathyroid hormone |
| TRAP5 | Tartrate-resistant acid phosphatase 5b |
| wF | With fractures |
| wnOF | With not osteoporotic fractures |
| woF | Without fractures |
References
- Consensus, A. Consensus development conference: Diagnosis, prophylaxis, and treatment of osteoporosis. Am. J. Med. 1993, 94, 646–650. [Google Scholar] [CrossRef]
- Zhao, W.; Shen, G.; Ren, H.; Liang, D.; Yu, X.; Zhang, Z.; Huang, J.; Qiu, T.; Tang, J.; Shang, Q.; et al. Therapeutic potential of microRNAs in osteoporosis function by regulating the biology of cells related to bone homeostasis. J. Cell. Physiol. 2018, 233, 9191–9208. [Google Scholar] [CrossRef]
- Facts and Statistics. International Osteoporosis Foundation. Available online: https://www.iofbonehealth.org/facts-statistics (accessed on 13 July 2020).
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Leibson, C.L.; Tosteson, A.N.A.; Gabriel, S.E.; Ransom, J.E.; Melton, L.J. Mortality, Disability, and Nursing Home Use for Persons with and without Hip Fracture: A Population-Based Study. J. Am. Geriatr. Soc. 2002, 50, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Siris, E.S.; Adler, R.; Bilezikian, J.; Bolognese, M.; Dawson-Hughes, B.; Favus, M.J.; Harris, S.T.; Jan de Beur, S.M.; Khosla, S.; Lane, N.E.; et al. The clinical diagnosis of osteoporosis: A position statement from the National Bone Health Alliance Working Group. Osteoporos. Int. 2014, 25, 1439–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, G.; Lanteri, P.; Colombini, A.; Banfi, G. Blood biochemical markers of bone turnover: Pre-analytical and technical aspects of sample collection and handling. Clin. Chem. Lab. Med. 2012, 50, 771–789. [Google Scholar] [CrossRef] [PubMed]
- Cranney, A.; Jamal, S.A.; Tsang, J.F.; Josse, R.G.; Leslie, W.D. Low bone mineral density and fracture burden in postmenopausal women. CMAJ 2007, 177, 575–580. [Google Scholar] [CrossRef] [Green Version]
- Silverman, S.L.; Calderon, A.D. The utility and limitations of FRAX: A US perspective. Curr. Osteoporos. Rep. 2010, 8, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Bottani, M.; Banfi, G.; Lombardi, G. Perspectives on miRNAs as Epigenetic Markers in Osteoporosis and Bone Fracture Risk: A Step Forward in Personalized Diagnosis. Front. Genet. 2019, 10, 1044. [Google Scholar] [CrossRef]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.C.; Feinbaum, R.L.; Ambros, V. The C. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell 1993, 75, 843–854. [Google Scholar] [CrossRef]
- Cerutti, H.; Casas-Mollano, J.A. On the origin and functions of RNA-mediated silencing: From protists to man. Curr. Genet. 2006, 50, 81–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Kowdley, K.V. MicroRNAs in common human diseases. Genom. Proteom. Bioinform. 2012, 10, 246–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chim, S.S.C.; Shing, T.K.F.; Hung, E.C.W.; Leung, T.-Y.; Lau, T.-K.; Chiu, R.W.K.; Lo, Y.M.D. Detection and characterization of placental microRNAs in maternal plasma. Clin. Chem. 2008, 54, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Lawrie, C.H.; Gal, S.; Dunlop, H.M.; Pushkaran, B.; Liggins, A.P.; Pulford, K.; Banham, A.H.; Pezzella, F.; Boultwood, J.; Wainscoat, J.S.; et al. Detection of elevated levels of tumour-associated microRNAs in serum of patients with diffuse large B-cell lymphoma. Br. J. Haematol. 2008, 141, 672–675. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Ba, Y.; Ma, L.; Cai, X.; Yin, Y.; Wang, K.; Guo, J.; Zhang, Y.; Chen, J.; Guo, X.; et al. Characterization of microRNAs in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef] [Green Version]
- Weber, J.A.; Baxter, D.H.; Zhang, S.; Huang, D.Y.; Huang, K.H.; Lee, M.J.; Galas, D.J.; Wang, K. The microRNA spectrum in 12 body fluids. Clin. Chem. 2010, 56, 1733–1741. [Google Scholar] [CrossRef]
- Gallo, A.; Tandon, M.; Alevizos, I.; Illei, G.G. The majority of microRNAs detectable in serum and saliva is concentrated in exosomes. PLoS ONE 2012, 7, e30679. [Google Scholar] [CrossRef] [Green Version]
- Turchinovich, A.; Weiz, L.; Burwinkel, B. Extracellular miRNAs: The mystery of their origin and function. Trends Biochem. Sci. 2012, 37, 460–465. [Google Scholar] [CrossRef]
- Morrow, D.A.; de Lemos, J.A. Benchmarks for the assessment of novel cardiovascular biomarkers. Circulation 2007, 115, 949–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mestdagh, P.; Hartmann, N.; Baeriswyl, L.; Andreasen, D.; Bernard, N.; Chen, C.; Cheo, D.; D’Andrade, P.; DeMayo, M.; Dennis, L.; et al. Evaluation of quantitative miRNA expression platforms in the microRNA quality control (miRQC) study. Nat. Methods 2014, 11, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Donati, S.; Ciuffi, S.; Brandi, M.L. Human Circulating miRNAs Real-time qRT-PCR-based Analysis: An Overview of Endogenous Reference Genes Used for Data Normalization. Int. J. Mol. Sci. 2019, 20, 4353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Wang, Z.; Fu, Q.; Zhang, J. Plasma miRNA levels correlate with sensitivity to bone mineral density in postmenopausal osteoporosis patients. Biomarkers 2014, 19, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, K.; Pang, Q.; Yang, C.; Zhang, H.; Wu, F.; Cao, H.; Liu, H.; Wan, Y.; Xia, W.; et al. Identification of suitable reference gene and biomarkers of serum miRNAs for osteoporosis. Sci. Rep. 2016, 6, 36347. [Google Scholar] [CrossRef]
- Bedene, A.; Mencej Bedrač, S.; Ješe, L.; Marc, J.; Vrtačnik, P.; Preželj, J.; Kocjan, T.; Kranjc, T.; Ostanek, B. MiR-148a the epigenetic regulator of bone homeostasis is increased in plasma of osteoporotic postmenopausal women. Wien. Klin. Wochenschr. 2016, 128, 519–526. [Google Scholar] [CrossRef]
- Liu, H.; Liu, Q.; Wu, X.-P.; He, H.-B.; Fu, L. MiR-96 regulates bone metabolism by targeting osterix. Clin. Exp. Pharm. Physiol. 2018, 45, 602–613. [Google Scholar] [CrossRef]
- Chen, R.; Liao, X.; Chen, F.; Wang, B.; Huang, J.; Jian, G.; Huang, Z.; Yin, G.; Liu, H.; Jin, D. Circulating microRNAs, miR-10b-5p, miR-328-3p, miR-100 and let-7, are associated with osteoblast differentiation in osteoporosis. Int. J. Clin. Exp. Pathol. 2018, 11, 1383–1390. [Google Scholar]
- Xia, Z.-L.; Wang, Y.; Sun, Q.-D.; Du, X.-F. MiR-203 is involved in osteoporosis by regulating DKK1 and inhibiting osteogenic differentiation of MSCs. Eur. Rev. Med. Pharm. Sci. 2018, 22, 5098–5105. [Google Scholar] [CrossRef]
- Qiao, L.; Liu, D.; Li, C.-G.; Wang, Y.-J. MiR-203 is essential for the shift from osteogenic differentiation to adipogenic differentiation of mesenchymal stem cells in postmenopausal osteoporosis. Eur. Rev. Med. Pharm. Sci. 2018, 22, 5804–5814. [Google Scholar] [CrossRef]
- Perksanusak, T.; Panyakhamlerd, K.; Hirankarn, N.; Suwan, A.; Vasuratna, A.; Taechakraichana, N. Correlation of plasma microRNA-21 expression and bone turnover markers in postmenopausal women. Climacteric 2018, 21, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Bemben, M.G.; Bemben, D.A. Bone and muscle specific circulating microRNAs in postmenopausal women based on osteoporosis and sarcopenia status. Bone 2019, 120, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Li, X.; Zou, D.; Lian, Y.; Tian, S.; Dou, Z. Expression of microRNA-21 in osteoporotic patients and its involvement in the regulation of osteogenic differentiation. Exp. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Luo, B.; Yang, J.-F.; Wang, Y.-H.; Qu, G.-B.; Hao, P.-D.; Zeng, Z.-J.; Yuan, J.; Yang, R.; Yuan, Y. MicroRNA-579-3p promotes the progression of osteoporosis by inhibiting osteogenic differentiation of mesenchymal stem cells through regulating Sirt1. Eur. Rev. Med. Pharm. Sci. 2019, 23, 6791–6799. [Google Scholar] [CrossRef]
- Li, L.-Y.; Wang, X.-L.; Wang, G.-S.; Zhao, H.-Y. MiR-373 promotes the osteogenic differentiation of BMSCs from the estrogen deficiency induced osteoporosis. Eur. Rev. Med. Pharm. Sci. 2019, 23, 7247–7255. [Google Scholar] [CrossRef]
- Zhang, H.-L.; Du, X.-Y.; Dong, Q.-R. LncRNA XIXT promotes osteogenic differentiation of bone mesenchymal stem cells and alleviates osteoporosis progression by targeting miRNA-30a-5p. Eur. Rev. Med. Pharm. Sci. 2019, 23, 8721–8729. [Google Scholar] [CrossRef]
- Zhang, H.; Ding, W.; Ji, F.; Wu, D. MicroRNA-410 participates in the pathological process of postmenopausal osteoporosis by downregulating bone morphogenetic protein-2. Exp. Med. 2019. [Google Scholar] [CrossRef]
- Tang, L.; Lu, W.; Huang, J.; Tang, X.; Zhang, H.; Liu, S. miR-144 promotes the proliferation and differentiation of bone mesenchymal stem cells by downregulating the expression of SFRP1. Mol. Med. Rep. 2019, 20, 270–280. [Google Scholar] [CrossRef]
- Lv, R.; Pan, X.; Song, L.; Sun, Q.; Guo, C.; Zou, S.; Zhou, Q. MicroRNA-200a-3p accelerates the progression of osteoporosis by targeting glutaminase to inhibit osteogenic differentiation of bone marrow mesenchymal stem cells. Biomed. Pharmacother. 2019, 116, 108960. [Google Scholar] [CrossRef]
- Lin, C.; Yu, S.; Jin, R.; Xiao, Y.; Pan, M.; Pei, F.; Zhu, X.; Huang, H.; Zhang, Z.; Chen, S.; et al. Circulating miR-338 Cluster activities on osteoblast differentiation: Potential Diagnostic and Therapeutic Targets for Postmenopausal Osteoporosis. Theranostics 2019, 9, 3780–3797. [Google Scholar] [CrossRef]
- Chen, R.; Qiu, H.; Tong, Y.; Liao, F.; Hu, X.; Qiu, Y.; Liao, Y. MiRNA-19a-3p alleviates the progression of osteoporosis by targeting HDAC4 to promote the osteogenic differentiation of hMSCs. Biochem. Biophys. Res. Commun. 2019, 516, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Suarjana, I.N.; Isbagio, H.; Soewondo, P.; Rachman, I.A.; Sadikin, M.; Prihartono, J.; Malik, S.G.; Soeroso, J. The Role of Serum Expression Levels of Microrna-21 on Bone Mineral Density in Hypostrogenic Postmenopausal Women with Osteoporosis: Study on Level of RANKL, OPG, TGFβ-1, Sclerostin, RANKL/OPG Ratio, and Physical Activity. Acta Med. Indones. 2019, 51, 245–252. [Google Scholar] [PubMed]
- Ding, W.; Ding, S.; Li, J.; Peng, Z.; Hu, P.; Zhang, T.; Pan, L. Aberrant Expression of miR-100 in Plasma of Patients with Osteoporosis and its Potential Diagnostic Value. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef] [PubMed]
- Lei, N.-B.; Liang, X.; Wang, P.; Liu, Q.; Wang, W.-G. Teriparatide alleviates osteoporosis by promoting osteogenic differentiation of hMSCs via miR-375/RUNX2 axis. Eur. Rev. Med. Pharm. Sci. 2019, 23, 11043–11050. [Google Scholar] [CrossRef]
- Lan, C.; Long, L.; Xie, K.; Liu, J.; Zhou, L.; Pan, S.; Liang, J.; Tu, Z.; Gao, Z.; Tang, Y. miRNA-429 suppresses osteogenic differentiation of human adipose-derived mesenchymal stem cells under oxidative stress via targeting SCD-1. Exp. Med. 2019. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.-G.; Hua, Y.; Liu, S.-W.; Hu, W.-Q.; Qian, R.; Xiong, L. MicroRNA-1286 inhibits osteogenic differentiation of mesenchymal stem cells to promote the progression of osteoporosis via regulating FZD4 expression. Eur. Rev. Med. Pharm. Sci. 2020, 24, 1–10. [Google Scholar] [CrossRef]
- Gao, G.-C.; Yang, D.-W.; Liu, W. LncRNA TERC alleviates the progression of osteoporosis by absorbing miRNA-217 to upregulate RUNX2. Eur. Rev. Med. Pharm. Sci. 2020, 24, 526–534. [Google Scholar] [CrossRef]
- Ismail, S.M.; El Boghdady, N.A.; Hamoud, H.S.; Shabayek, M.I. Evaluation of circulating miRNA-208a-3p, miRNA-155–5p and miRNA-637 as potential non-invasive biomarkers and the possible mechanistic insights into pre- and postmenopausal osteoporotic females. Arch. Biochem. Biophys. 2020, 684, 108331. [Google Scholar] [CrossRef]
- Yavropoulou, M.P.; Anastasilakis, A.D.; Makras, P.; Tsalikakis, D.G.; Grammatiki, M.; Yovos, J.G. Expression of microRNAs that regulate bone turnover in the serum of postmenopausal women with low bone mass and vertebral fractures. Eur. J. Endocrinol. 2017, 176, 169–176. [Google Scholar] [CrossRef]
- Mandourah, A.Y.; Ranganath, L.; Barraclough, R.; Vinjamuri, S.; Hof, R.V.; Hamill, S.; Czanner, G.; Dera, A.A.; Wang, D.; Barraclough, D.L. Circulating microRNAs as potential diagnostic biomarkers for osteoporosis. Sci. Rep. 2018, 8, 8421. [Google Scholar] [CrossRef]
- Ramírez-Salazar, E.G.; Carrillo-Patiño, S.; Hidalgo-Bravo, A.; Rivera-Paredez, B.; Quiterio, M.; Ramírez-Palacios, P.; Patiño, N.; Valdés-Flores, M.; Salmerón, J.; Velázquez-Cruz, R. Serum miRNAs miR-140-3p and miR-23b-3p as potential biomarkers for osteoporosis and osteoporotic fracture in postmenopausal Mexican-Mestizo women. Gene 2018, 679, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Hu, L.; Wang, S.; Huang, T.; Zhang, M.; Yang, M.; Zhen, W.; Yang, D.; Lu, W.; Guan, M.; et al. Circulating MicroRNA-19b Identified from Osteoporotic Vertebral Compression Fracture Patients Increases Bone Formation. J. Bone Min. Res. 2020, 35, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Feurer, E.; Kan, C.; Croset, M.; Sornay-Rendu, E.; Chapurlat, R. Lack of Association between Select Circulating miRNAs and Bone Mass, Turnover, and Fractures: Data from the OFELY Cohort. J. Bone Min. Res. 2019, 34, 1074–1085. [Google Scholar] [CrossRef] [PubMed]
- You, L.; Pan, L.; Chen, L.; Gu, W.; Chen, J. MiR-27a is Essential for the Shift from Osteogenic Differentiation to Adipogenic Differentiation of Mesenchymal Stem Cells in Postmenopausal Osteoporosis. Cell. Physiol. Biochem. 2016, 39, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Lin, X.; Chen, C.; Li, S.; Zhang, S.; Chen, Z.; Li, D.; Zhao, F.; Yang, C.; Yin, C.; et al. Circulating miR-181c-5p and miR-497-5p Are Potential Biomarkers for Prognosis and Diagnosis of Osteoporosis. J. Clin. Endocrinol. Metab. 2020, 105, 1445–1460. [Google Scholar] [CrossRef] [PubMed]
- Pala, E.; Denkçeken, T. Differentially expressed circulating miRNAs in postmenopausal osteoporosis: A meta-analysis. Biosci. Rep. 2019, 39, BSR20190667. [Google Scholar] [CrossRef] [Green Version]
- Weilner, S.; Skalicky, S.; Salzer, B.; Keider, V.; Wagner, M.; Hildner, F.; Gabriel, C.; Dovjak, P.; Pietschmann, P.; Grillari-Voglauer, R.; et al. Differentially circulating miRNAs after recent osteoporotic fractures can influence osteogenic differentiation. Bone 2015, 79, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Panach, L.; Mifsut, D.; Tarín, J.J.; Cano, A.; García-Pérez, M.Á. Serum Circulating MicroRNAs as Biomarkers of Osteoporotic Fracture. Calcif. Tissue Int. 2015, 97, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Heilmeier, U.; Hackl, M.; Skalicky, S.; Weilner, S.; Schroeder, F.; Vierlinger, K.; Patsch, J.M.; Baum, T.; Oberbauer, E.; Lobach, I.; et al. Serum miRNA Signatures Are Indicative of Skeletal Fractures in Postmenopausal Women with and without Type 2 Diabetes and Influence Osteogenic and Adipogenic Differentiation of Adipose Tissue-Derived Mesenchymal Stem Cells in Vitro: miRNA signatures as tools for fracture risk assessment in type 2 diabetes. J. Bone Min. Res. 2016, 31, 2173–2192. [Google Scholar] [CrossRef] [Green Version]
- Kocijan, R.; Muschitz, C.; Geiger, E.; Skalicky, S.; Baierl, A.; Dormann, R.; Plachel, F.; Feichtinger, X.; Heimel, P.; Fahrleitner-Pammer, A.; et al. Circulating microRNA Signatures in Patients with Idiopathic and Postmenopausal Osteoporosis and Fragility Fractures. J. Clin. Endocrinol. Metab. 2016, 101, 4125–4134. [Google Scholar] [CrossRef]
- Feichtinger, X.; Muschitz, C.; Heimel, P.; Baierl, A.; Fahrleitner-Pammer, A.; Redl, H.; Resch, H.; Geiger, E.; Skalicky, S.; Dormann, R.; et al. Bone-related Circulating MicroRNAs miR-29b-3p, miR-550a-3p, and miR-324-3p and their Association to Bone Microstructure and Histomorphometry. Sci. Rep. 2018, 8, 4867. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Jiang, H.; Can, D.; Xu, H.; Zhang, K.; Guo, S. Evaluation of MicroRNA 125b as a potential biomarker for postmenopausal osteoporosis. Trop. J. Pharm. Res. 2017, 16, 641. [Google Scholar] [CrossRef] [Green Version]
- Seeliger, C.; Karpinski, K.; Haug, A.T.; Vester, H.; Schmitt, A.; Bauer, J.S.; van Griensven, M. Five freely circulating miRNAs and bone tissue miRNAs are associated with osteoporotic fractures. J. Bone Min. Res. 2014, 29, 1718–1728. [Google Scholar] [CrossRef] [PubMed]
- Kelch, S.; Balmayor, E.R.; Seeliger, C.; Vester, H.; Kirschke, J.S.; van Griensven, M. miRNAs in bone tissue correlate to bone mineral density and circulating miRNAs are gender independent in osteoporotic patients. Sci. Rep. 2017, 7, 15861. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, W.; Huang, Y. MiRNA-133a is involved in the regulation of postmenopausal osteoporosis through promoting osteoclast differentiation. Acta Biochim. Biophys. Sin. 2018, 50, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Pickering, M.-E.; Millet, M.; Rousseau, J.-C.; Croset, M.; Szulc, P.; Borel, O.; Sornay Rendu, E.; Chapurlat, R. Selected serum microRNA, abdominal aortic calcification and risk of osteoporotic fracture. PLoS ONE 2019, 14, e0216947. [Google Scholar] [CrossRef] [Green Version]
- Zarecki, P.; Hackl, M.; Grillari, J.; Debono, M.; Eastell, R. Serum microRNAs as novel biomarkers for osteoporotic vertebral fractures. Bone 2020, 130, 115105. [Google Scholar] [CrossRef]
- Wang, C.; He, H.; Wang, L.; Jiang, Y.; Xu, Y. Reduced miR-144-3p expression in serum and bone mediates osteoporosis pathogenesis by targeting RANK. Biochem. Cell Biol. 2018, 96, 627–635. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Luo, R.; Yang, W.; Zhou, Z.; Li, C. miR-363-3p is activated by MYB and regulates osteoporosis pathogenesis via PTEN/PI3K/AKT signaling pathway. In Vitro Cell. Dev. Biol. Anim. 2019, 55, 376–386. [Google Scholar] [CrossRef]
- Li, K.; Chen, S.; Cai, P.; Chen, K.; Li, L.; Yang, X.; Yi, J.; Luo, X.; Du, Y.; Zheng, H. MiRNA-483–5p is involved in the pathogenesis of osteoporosis by promoting osteoclast differentiation. Mol. Cell. Probes 2020, 49, 101479. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Design | OP Diagnosis | c-miR Source | Platforms for c-miR Quantification | Validate c-miR Biomarkers | Normalization Strategy | AUC Value | c-miR Correlations | Ref | |
|---|---|---|---|---|---|---|---|---|---|
| Prescreening | Validation | ||||||||
| PM: OP (40), Ope (40), CTR (40) | DXA | Plasma | / | qPCR | miR-21-5p (↓), miR-133a (↑), in OP and Ope vs. CTR | miR-16 | / | miR-21-5p and miR-133a/h- and BMD (+) and (−) respectively | [25] |
| PM: OP (10), Ope (7) CTR (19) | DXA | Serum | Microarray | qPCR | miR-30-5p (↓) in OP and Ope vs. CTR; miR-328a-3p, miR-103-3p and miR-142-3p (↓) in OP vs. CTR | miR-25-3p | miR-30-5p: 0.79; miR-328a-3p: 0.87; miR-103-3p: 0.8; miR-142-3p: 0.79 | All four miRs/BMD (+) | [26] |
| PM: OP (17), CTR (57) | DXA FRAX | Plasma | / | qPCR | miR-148-3p (↑) in OP vs. CTR | let-7a-5p and miR-16-5p | / | miR-126-3p/BMD (+); miR-423-5p/FRAX (−) | [27] |
| PM OP (20), PRM CTR (20), PM CTR (20) | DXA | Serum | Microarray | qPCR | miR-96 (↑) in OP vs. PM CTR and (↓) in OP vs. PRM CTR | U6 | / | miR-96/BALP (−) | [28] |
| OP (9), CTR (9) | DXA | Serum | Microarray | qPCR | miR-10b-3p and miR-100 (↑), and miR-328-3p and let-7g-5p (↓) in OP vs. CTR | U6 | miR-10b-3p: 0.87 | / | [29] |
| OP (60), CTR (60)/OP (60), CTR (40) | QCT | Serum | / | qPCR | miR-203 (↓) in OP vs. CTR | / | / | / | [30,31] |
| PM: LBMD (109), CTR (41) | DXA | Plasma | / | qPCR | miR-21-5p (↑) in LBMD vs. CTR | cel-miR-39 | / | miR-21-5p/BMD (−) | [32] |
| PM: LBMD (46), CTR (13) | DXA | Serum | / | qPCR | miR-21-5p, miR-23a-3p (↑), and miR- 125b-5p (↓) in LBMD vs. CTR | miR-16-5p, miR-93-5p, miR-191-5p | / | miR-21-5p and miR-133a-3p/BMD (−) and (+), respectively; miR-23a-3p/TRAP5b (+) | [33] |
| OP (48), CTR (48) | / | Serum | / | qPCR | miR-17, miR-20a, miR-21 and miR-29a (↓) in OP vs. CTR | U6 | / | / | [34] |
| OP (/), CTR (/) | / | Serum | / | qPCR | miR-579-3p (↑) in OP vs. CTR | U6 | / | / | [35] |
| PM: OP (20), CTR (20) | μCT | Serum | / | qPCR | miR-28, miR-101 and miR-373 (↓) in OP vs. CTR | U6 | / | / | [36] |
| OP (/), CTR (/) | / | Serum | / | qPCR | miR-30a-5p (↑) in OP vs. CTR | / | / | / | [37] |
| PM: OP (26), CTR (29) | / | Serum | / | qPCR | miR-410 (↑) in OP vs. CTR | U6 | / | / | [38] |
| PM: OP (15), CTR (15) | / | Serum | / | qPCR | miR-144 (↑) in OP vs. CTR | U6 | / | miR-144/Sfrp1 (+) | [39] |
| OP (30), CTR (30) | / | Serum | / | qPCR | miR-200a-3p (↑) in OP vs. CTR | U6 | / | / | [40] |
| PM: OP (15), CTR (15) | / | Serum | / | qPCR | miR-338-3p and miR-3065-5p (↑) in OP vs. CTR | U6 | miR-338-3p: 0.74; miR-3065-5p: 0.87 | / | [41] |
| OP (42), CTR (42) | / | Serum | / | qPCR | miR-19a-3p (↓) in OP vs. CTR | U6 | / | / | [42] |
| OP (60), CTR (60) | DXA | Serum | / | qPCR | miR-21-5p (↑) in OP vs. CTR | / | / | miR-21-5p/RUNKL and OPG (+) | [43] |
| OP (120), CTR (120) | / | Plasma | / | qPCR | miR-100 (↑) in OP vs. CTR | / | miR-100: 0.89 | miR-100/BMD (−) | [44] |
| OP (30), CTR (30) | / | Serum | / | qPCR | miR-375 (↑) in OP vs. CTR | U6 | / | / | [45] |
| OP (30), CTR (30) | / | Serum | / | qPCR | miR-429 (↑) in OP vs. CTR | / | / | / | [46] |
| OP (/), CTR (/) | / | Serum | / | qPCR | miR-1286 (↑) in OP vs. CTR | / | / | / | [47] |
| OP (/), CTR (/) | / | Serum | / | qPCR | miR-217 (↑) in OP vs. CTR | / | / | / | [48] |
| PM+PRM OP (70), PM+PRM CTR (70) | DXA | Serum | / | qPCR | miR-208a-3p (↑) in OP vs. CTR; miR-155-5p and miR-637 (↑) in PM OP vs. PM CTR; miR-155-5p (↓) PRM OP vs. PRM CTR | SNORD68 | PM OP vs. PM CTR: miR-208a-3p: 0.82; miR-155-5p: 0.9; miR-637: 0.63. PM OP vs. PM CTR: miR-208a-3p: 0.85; miR-155-5p: 0.83; miR-637: 0.81. | All 3 miRs/BMD (−) | [49] |
| PM: LBMD (35), CTR (30) | DXA | Serum | / | qPCR | miR-124 and miR-2861 (↑) LBMD vs. CTR; miR-21-5p, miR-29a-3p, miR-23a-3p (↓) in LBMD vs. CTR | / | miR-21-5p: 0.66; miR-29a-3p: 0.61; miR23a-3p: 0.63 | / | [50] |
| OP (33), Ope (61), CTR (12) | DXA | Serum and plasma | qPCR array | qPCR | miR-122-5p (↓ in serum) OP vs. Ope, OP vs. N, Ope vs. N; miR-4516 (↓ in plasma) OP vs. N | SNORD96A, RNU6–6P | miR-122-5p: 0.67; miR-4516: 0.73; miR-122-5p+miR-4516: 0.75 | miR-122-5p and miR-4516/BMD (+) | [51] |
| PM OP (16), PM Ope (28), PM CTR (22) | DXA or fracture | Serum | miRtaqman array card | qPCR | miR-23b-3p and miR-140-3p (↑) in OP/ Ope vs. CTR; miR-885-5p (↑) in Ope vs. CTR | RNU6-1 | miR-140-3p: 0.96 for OP, 0.84 for Ope; miR-23b-3p: 0.69 for OP, 0.73 for Ope; miR-885-5p: 0.69 for Ope | miR-23b-3p and miR-140-3p/BMD (−) | [52] |
| OP (24), CTR (24) | DXA | Plasma | Microarray | qPCR | miR-19b-3p (↓) in OP vs. CTR | U6 | miR-19b-3p: 0.93 OP, | miR-19b-3p/BMD (+) | [53] |
| PM OP (81), PRM CTR (74) | DXA | Serum | Microarray | qPCR | miR-27a (↓) in OP vs. CTR | U6 | / | / | [55] |
| PM: OP (17), Ope (14), PRM CTR (14) | DXA | Serum | Microarray | qPCR | miR-204-3p (↑) in OP/Ope vs. CTR; miR-181c-5p and miR-497-5p (↓) in OP/Ope vs. CTR | 5S | miR-204-3p: 0.96, miR-181c-5p: 0.87 and miR-497-5p: 0.92 for OP; miR-204-3p: 0.77, miR-181c-5p: 0.69 and miR-497-5p: 0.75 for Ope; | miR-204-3p/BMD (−), BMI and CTx (+); miR-181c-5p and miR-497-5p/BMD (+) | [56] |
| Study Design | OP Diagnosis | c-miRs Source | Platforms for c-miRs Quantification | Validate c-miR Biomarkers | Normalization Strategy | AUC Value | c-miR Correlations | Ref | |
|---|---|---|---|---|---|---|---|---|---|
| Prescreening | Validation | ||||||||
| OP F (18), OP (33), Ope F (15), CTR (12) | DXA | Serum and plasma | qPCR array | qPCR | miR-122-5p (↓ in serum) OP F vs. OP/CTR; miR-4516 (↓ in plasma) LBMD F vs. LBMD | SNORD96A, RNU6–6P | miR-122-5p: 0.67; miR-4516: 0.73; miR-122-5p+miR-4516: 0.75 | miR-122-5p and miR-4516/BMD (+) | [51] |
| OP F (21), PM CTR (22) | DXA or fracture | Serum | miRtaqman array card | qPCR | miR-23b-3p and miR-140-3p (↑) in OP F vs. CTR; | RNU6-1 | / | miR-23b-3p and miR-140-3p/BMD (−) | [52] |
| OP F (24), CTR (24) | DXA | Plasma | Microarray | qPCR | miR-19b-3p (↓) in OP F vs. CTR | U6 | miR-19b-3p: 0.93 OP, 0.95 OP F | miR-19b-3p/BMD (+) | [53] |
| PM: OP F (19), CTR (18) | Fracture | Serum | qPCR array | qPCR | let-7g-5p, miR-328-3p, miR-22-3p (↓) in OP F vs. CTR | / | / | / | [58] |
| PM: OP F (15), OA CTR (12) | DXA | Serum | qPCR array | qPCR | miR-21-5p (↑) in OP F vs. CTR | miR-140-3p, miR-93-5p | miR-21-5p: 0.87 | miR-21-5p/CTx and OCN (+) | [59] |
| PM: OP F (20), CTR (20) | DXA | Serum | / | low density qPCR array | miR-550a-5p, miR-203a and miR-330-3p (↑) and miR-328-3p (↓) in OP F vs. CTR | / | / | / | [60] |
| PM OP F (10), IOP F (26), PM CTR (11), PMR/male CTR (28) | / | Serum | / | qPCR array | miR-152-3p, miR- 335-5p and miR-320a (↑), and let-7b-5p, miR-7-5p, miR- 16-5p, miR-19a-3p, miR-19b-3p, miR-29b-3p, miR-30e-5p, miR- 93-5p, miR-140-5p, miR-215-5p, miR-186-5p, miR-324-3p, miR-365a-3p, miR-378a-5p, miR-532-5p, and miR-550a-3p (↓) in fractured group vs. CTR | miRs Ct average | miR-152-3p: 0.96, miR-30e-5p: 0.96, miR-324-3p: 0.95, miR-140-5p: 0.95, miR-19b-3p: 0.94, miR-335-5p: 0.94, miR-19a-3p: 0.93, miR-550a-3p: 0.91, miR-186-5p: 0.9, miR-532-5p: 0.9, miR-378a-5p: 0.87, miR-320a: 0.87, miR-93-5p: 0.88, miR-16-5p: 0.86, miR-215-5p: 0.85, let-7b-5p: 0.85, miR-7-5p: 0.82, miR-29b-3p: 0.84, and miR- 365a-3p: 0.81 for fracture group vs. CTR | miR-140-5p/BMI (−); miR-320a/BMI (+); miR-29b-3p/PIPN (+); miR-365a-3p/PTH, TRAP5, PIPN, OCN (+); miR19a-3p, miR-324-3p, miR-532-5p and miR-93-5p/BMD (+) | [61] |
| PM: OP F (30), CTR (30) | Fracture | Serum | Microarray | qPCR | miR-30, miR-96, miR-125b, miR-5914, miR-4665-3p (↑) in OP vs. CTR | U6 | miR-125b: 0.9; miR-30: 0.76; miR-5914: 0.7 | / | [63] |
| PM: OP F (14), CTR (14) | DXA | Serum | / | qPCR | miR-21-5p, miR-24-3p, miR-23a-3p, miR-122-5p, miR-124-3p, miR-148a-3p and miR-100-5p (↑) in OP F vs. CTR; miR-93-5p and miR-125b-5p (↑) in OP female vs. CTR | SNORD96a | / | / | [65] |
| PM OP F (10), CTR (10) | DXA | Serum | / | qPCR | miR-133a (↑) in OP F vs. CTR | U6 | / | miR-133a/BMD (−) | [66] |
| PM: LBMD (35), LBMD F (24), CTR (40) | DXA | Serum | / | qPCR | miR-375, miR-532-5p, miR-19b-3p, miR-152-3p, miR-23a-3p, miR-335-5p, and miR-21-5p (↑) in LBMD F vs. LBMD and CTR | miR-451a | / | miR-19b-3p/OCN, BALP and CTx (+) | [68] |
| Study Design | OP Diagnosis | c-miRs Source | Platforms for c-miR Quantification | Validate c-miR Biomarkers | Normalization Strategy | AUC Value | c-miR Correlations | Ref | |
|---|---|---|---|---|---|---|---|---|---|
| Prescreening | Validation | ||||||||
| OP F (40), CTR wnOF (40) | DXA | Serum | qPCR array | qPCR | miR-21-5p, miR-23a-3p, miR-24-3p, miR-100-5p, miR-122-5p, miR-124-3p, miR-125-5p, miR-148a-3p and miR-93 (↑) in OP F vs. CTR | SNORD96a and RNU6 | miR-21-5p: 0.63, miR-23a-3p: 0.63, miR-24-3p: 0.63, miR-100-5p: 0.69, miR-122a-5p: 0.77, miR-124a-3p: 0.69, miR-125b-5p: 0.76, miR-148a-3p and miR-93: 0.68 | / | [64] |
| OP F (45), wnOF CTR (15) | / | Serum | / | qPCR | miR-24-3p, miR-27a-3p, miR-100, miR-125b, miR-122a and miR-145-5p (↑) in OP F vs. CTR | U6 | / | / | [69] |
| OP F (6), wnOF CTR (6) | / | Serum | / | qPCR | miR-363-3p, miR-214, miR-103a, miR-148a (↑), and miR-2861, miR-34a, miR-503 (↓) in OP F vs. CTR | / | / | / | [70] |
| PM: OP F (30), wnOF CTR (36) | DXA | Serum | / | qPCR | miR-483 (↑) in OP F vs. CTR | U6 | / | / | [71] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciuffi, S.; Donati, S.; Marini, F.; Palmini, G.; Luzi, E.; Brandi, M.L. Circulating MicroRNAs as Novel Biomarkers for Osteoporosis and Fragility Fracture Risk: Is There a Use in Assessment Risk? Int. J. Mol. Sci. 2020, 21, 6927. https://doi.org/10.3390/ijms21186927
Ciuffi S, Donati S, Marini F, Palmini G, Luzi E, Brandi ML. Circulating MicroRNAs as Novel Biomarkers for Osteoporosis and Fragility Fracture Risk: Is There a Use in Assessment Risk? International Journal of Molecular Sciences. 2020; 21(18):6927. https://doi.org/10.3390/ijms21186927
Chicago/Turabian StyleCiuffi, Simone, Simone Donati, Francesca Marini, Gaia Palmini, Ettore Luzi, and Maria Luisa Brandi. 2020. "Circulating MicroRNAs as Novel Biomarkers for Osteoporosis and Fragility Fracture Risk: Is There a Use in Assessment Risk?" International Journal of Molecular Sciences 21, no. 18: 6927. https://doi.org/10.3390/ijms21186927