Increased Angiogenesis and Lymphangiogenesis in the Placental Villi of Women with Chronic Venous Disease during Pregnancy

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Results
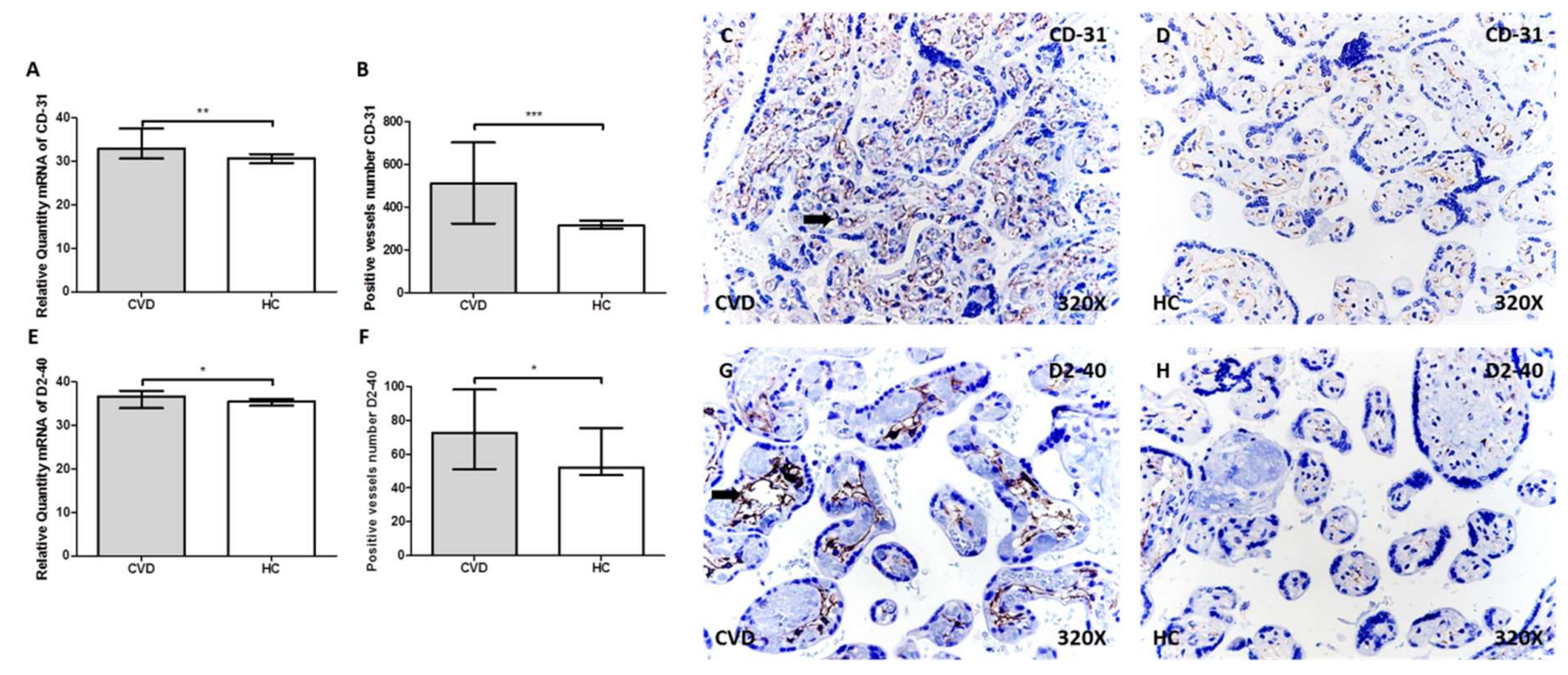
2.1. More Vessels Positive for CD31 and D2-40 in the Placental Villi of Women with CVD
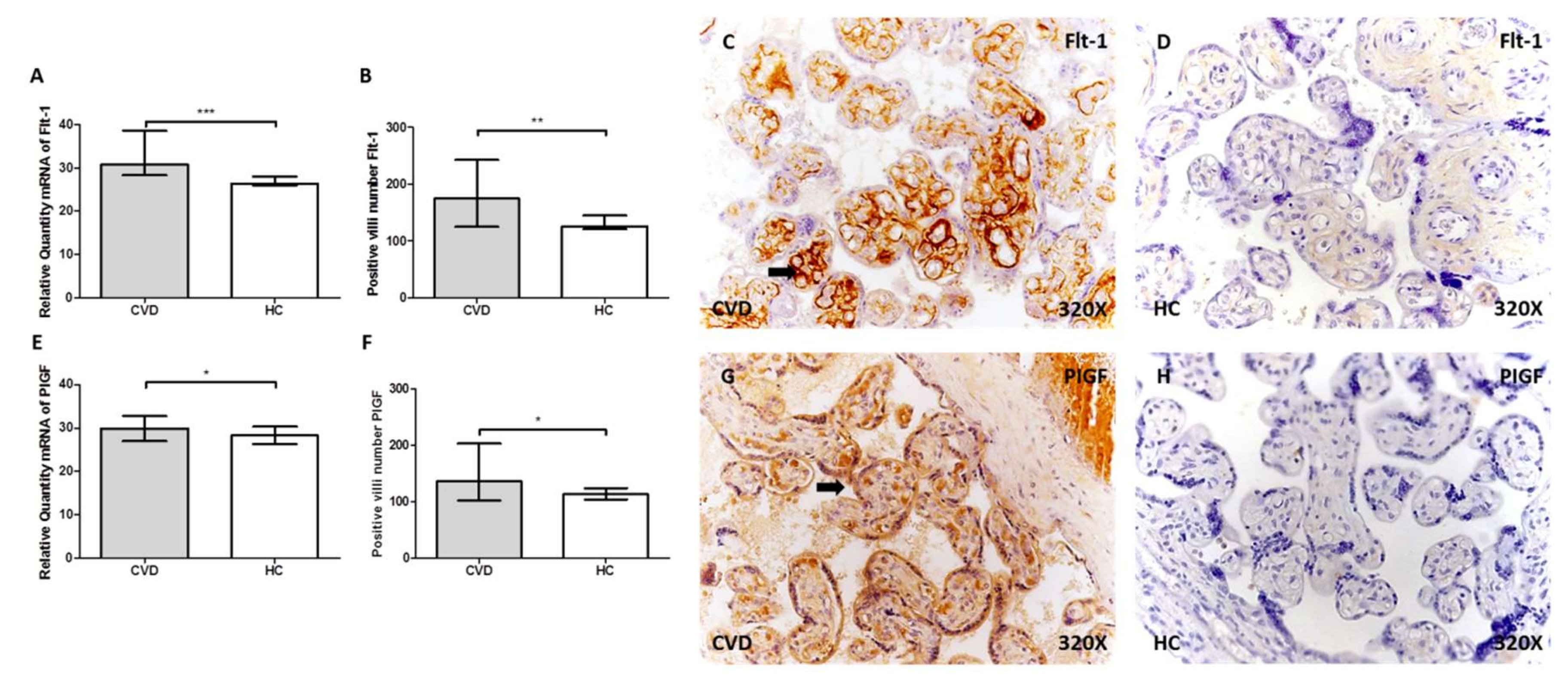
2.2. Women with CVD Show Greater Expression of Flt-1 and PIGF in Placental Villi
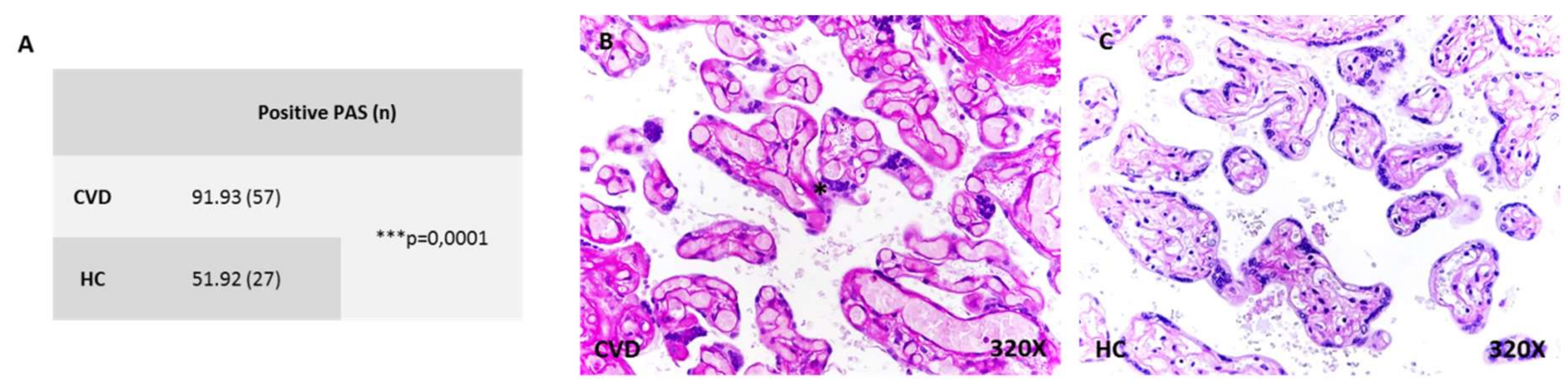
2.3. More Placental Villi with Periodic Acid of Schiff (PAS)-Positive Material in Women with CVD
3. Discussion
4. Material and Methods
4.1. Study Population
4.2. Placental Tissue Samples
4.3. Gene Expression Analysis Using RT-qPCR
4.4. Protein Expression Analysis by Immunohistochemistry
4.5. Periodic Acid of Schiff (PAS) Staining
4.6. Statistical Analysis and Interpretation of Results
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Youn, Y.J.; Lee, J. Chronic venous insufficiency and varicose veins of the lower extremities. Korean J. Intern. Med. 2019, 34, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Boivin, P.; Cornu-Thenard, A.; Charpak, Y. Pregnancy-induced changes in lower extremity superficial veins: An ultrasound scan study. J. Vasc. Surg. 2000, 32, 570–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, L.; Normahani, P.; Standfield, N.J.; Jaffer, U. A systematic review and meta-analysis of the risk for development of varicose veins in women with a history of pregnancy. J. Vasc. Surg. Venous Lymphat. Disord. 2016, 4, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Ropacka-Lesiak, M.; Kasperczak, J.; Breborowicz, G.H. Risk factors for the development of venous insufficiency of the lower limbs during pregnancy--part 1. Ginekol. Pol. 2012, 83, 939–942. [Google Scholar]
- Lohr, J.M.; Bush, R.L. Venous disease in women: Epidemiology, manifestations, and treatment. J. Vasc. Surg. 2013, 57, 37S–45S. [Google Scholar] [CrossRef] [Green Version]
- Ropacka-Lesiak, M.; Jarosław, K.; Bręborowicz, G. Pregnancy-dependent blood flow velocity changes in lower extremities veins in venous insufficiency. Ginekol. Pol. 2015, 86, 659–665. [Google Scholar] [CrossRef]
- Taylor, J.; Hicks, C.W.; Heller, J.A. The hemodynamic effects of pregnancy on the lower extremity venous system. J Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 246–255. [Google Scholar] [CrossRef]
- García-Honduvilla, N.; Asúnsolo, Á.; Ortega, M.A.; Sainz, F.; Leal, J.; Lopez-Hervas, P.; Pascual, G.; Buján, J. Increase and Redistribution of Sex Hormone Receptors in Premenopausal Women Are Associated with Varicose Vein Remodelling. Oxid. Med. Cell Longev. 2018, 2018, 3974026. [Google Scholar] [CrossRef] [Green Version]
- Kodogo, V.; Azibani, F.; Sliwa, K. Role of pregnancy hormones and hormonal interaction on the maternal cardiovascular system: A literature review. Clin. Res. Cardiol. 2019, 108, 831–846. [Google Scholar] [CrossRef]
- García-Honduvilla, N.; Ortega, M.A.; Asúnsolo, Á.; Álvarez-Rocha, M.J.; Romero, B.; De León-Luis, J.; Álvarez-Mon, M.; Buján, J. Placentas from women with pregnancy-associated venous insufficiency show villi damage with evidence of hypoxic cellular stress. Hum. Pathol. 2018, 77, 45–53. [Google Scholar] [CrossRef]
- Ortega, M.A.; Asúnsolo, Á.; Álvarez-Rocha, M.J.; Romero, B.; De León-Luis, J.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Remodelling of collagen fibres in the placentas of women with venous insufficiency during pregnancy. Histol. Histopathol. 2018, 33, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Saez, M.Á.; Asúnsolo, Á.; Romero, B.; Bravo, C.; Coca, S.; Sainz, F.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Upregulation of VEGF and PEDF in Placentas of Women with Lower Extremity Venous Insufficiency during Pregnancy and Its Implication in Villous Calcification. Biomed Res. Int. 2019, 2019, 5320902. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.C.; Mulcahy, C.; Zombori, G.; Ryan, J.; Downey, P.; McAuliffe, F.M. Placental volume, vasculature and calcification in pregnancies complicated by pre-eclampsia and intra-uterine growth restriction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 195, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Albers, R.E.; Kaufman, M.R.; Natale, B.V.; Keoni, C.; Kulkarni-Datar, K.; Min, S.; Williams, C.R.; Natale, D.R.C.; Brown, T.L. Trophoblast-Specific Expression of Hif-1α Results in Preeclampsia-Like Symptoms and Fetal Growth Restriction. Sci. Rep. 2019, 9, 2742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, L.; Ma, R.; Zhang, L.; Yuan, X.; Wu, J.; He, L.; Liu, G.; Du, R. Inhibition of HIF-1a-mediated TLR4 activation decreases apoptosis and promotes angiogenesis of placental microvascular endothelial cells during severe pre-eclampsia pathogenesis. Placenta 2019, 83, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Pang, V.; Bates, D.O.; Leach, L. Regulation of human feto-placental endothelial barrier integrity by vascular endothelial growth factors: Competitive interplay between VEGF-A165a, VEGF-A165b, PIGF and VE-cadherin. Clin. Sci. 2017, 131, 2763–2775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahay, A.S.; Jadhav, A.T.; Sundrani, D.P.; Wagh, G.N.; Mehendale, S.S.; Chavan-Gautam, P.; Joshi, S.R. VEGF and VEGFR1 levels in different regions of the normal and preeclampsia placentae. Mol. Cell Biochem. 2018, 438, 141–152. [Google Scholar] [CrossRef]
- Shibuya, M. Vascular endothelial growth factor and its receptor system: Physiological functions in angiogenesis and pathological roles in various diseases. J. Biochem. 2013, 153, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Istrate, M.; Mihu, C.; Şuşman, S.; Melincovici, C.S.; Măluţan, A.M.; Buiga, R.; Bolboacă, S.D.; Mihu, C.M. Highlighting the R1 and R2 VEGF receptors in placentas resulting from normal development pregnancies and from pregnancies complicated by preeclampsia. Rom. J. Morphol. Embryol. 2018, 59, 139–146. [Google Scholar]
- Xiao, Z.; Li, S.; Yu, Y.; Li, M.; Chen, J.; Wang, F.; Zhang, J.; Deng, W.; Yang, Q.; Fan, X. VEGF-A regulates sFlt-1 production in trophoblasts through both Flt-1 and KDR receptors. Mol. Cell Biochem. 2018, 449, 1–8. [Google Scholar] [CrossRef]
- Kurtoglu, E.; Avci, B.; Kokcu, A.; Celik, H.; Cengiz Dura, M.; Malatyalioglu, E.; Zehra Ozdemir, A. Serum VEGF and PGF may be significant markers in prediction of severity of preeclampsia. J. Matern. Fetal Neonatal Med. 2016, 29, 1987–1992. [Google Scholar] [CrossRef] [PubMed]
- Lecarpentier, É.; Vieillefosse, S.; Haddad, B.; Fournier, T.; Leguy, M.C.; Guibourdenche, J.; Tsatsaris, V. Placental growth factor (PlGF) and sFlt-1 during pregnancy: Physiology, assay and interest in preeclampsia. Ann. Biol. Clin. 2016, 74, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Fukaya, E.; Flores, A.M.; Lindholm, D.; Gustafsson, S.; Zanetti, D.; Ingelsson, E.; Leeper, N.J. Clinical and Genetic Determinants of Varicose Veins. Circulation 2018, 138, 2869–2880. [Google Scholar] [CrossRef] [PubMed]
- Uras, N.; Oguz, S.S.; Zergeroglu, S.; Akdag, A.; Polat, B.; Dizdar, E.A.; Dilmen, U. CD31 and Factor VIII in angiogenesis of normal and pre-eclamptic human placentas. J. Obstet. Gynaecol. 2012, 32, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Vangrieken, P.; Vanterpool, S.F.; van Schooten, F.J.; Al-Nasiry, S.; Andriessen, P.; Degreef, E.; Alfer, J.; Kramer, B.W.; von Rango, U. Histological villous maturation in placentas of complicated pregnancies. Histol. Histopathol. 2020, 27, 18205. [Google Scholar] [CrossRef]
- Goksu Erol, A.Y.; Nazli, M.; Elis Yildiz, S. Significance of platelet endothelial cell adhesion molecule-1 (PECAM-1) and intercellular adhesion molecule-1 (ICAM-1) expressions in preeclamptic placentae. Endocrine 2012, 42, 125–131. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, Y.J.; Zou, Q.Y.; Zhang, K.; Wu, Y.M.; Zhou, C.; Wang, K.; Zheng, J. Preeclampsia does not alter vascular growth and expression of CD31 and vascular endothelial cadherin in human placentas. J. Histochem. Cytochem. 2015, 63, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Li, Y.; Zhang, J.; Rao, M.; Liang, H.; Liu, G. The defect of both angiogenesis and lymphangiogenesis is involved in preeclampsia. Placenta 2015, 36, 279–286. [Google Scholar] [CrossRef]
- Onak Kandemir, N.; Barut, F.; Barut, A.; Birol, İ.E.; Dogan Gun, B.; Ozdamar, S.O. Biological importance of podoplanin expression in chorionic villous stromal cells and its relationship to placental pathologies. Sci. Rep. 2019, 9, 14230. [Google Scholar] [CrossRef]
- Takemoto, A.; Miyata, K.; Fujita, N. Platelet-activating factor podoplanin: From discovery to drug development. Cancer Metastasis Rev. 2017, 36, 225–234. [Google Scholar] [CrossRef]
- Bellini, C.; Rutigliani, M.; Boccardo, F.; Campisi, C.; Bellini, T.; Bonioli, E.; Fulcheri, E. Are there lymphatic vessels in the placenta? Lymphology 2012, 45, 34–36. [Google Scholar] [PubMed]
- Wang, Y.; Sun, J.; Gu, Y.; Zhao, S.; Groome, L.J.; Alexander, J.S. D2-40/podoplanin expression in the human placenta. Placenta 2011, 32, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volchek, M.; Girling, J.E.; Lash, G.E.; Cann, L.; Kumar, B.; Robson, S.C.; Bulmer, J.N.; Rogers, P.A. Lymphatics in the human endometrium disappear during decidualization. Hum. Reprod. 2010, 25, 2455–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuya, M.; Kurasawa, K.; Nagahama, K.; Kawachi, K.; Nozawa, A.; Takahashi, T. Disrupted balance of angiogenic and antiangiogenic signalings in preeclampsia. J. Pregnancy. 2011, 2011, 123717. [Google Scholar] [CrossRef] [Green Version]
- Birdir, C.; Droste, L.; Fox, L.; Frank, M.; Fryze, J.; Enekwe, A.; Köninger, A.; Kimmig, R.; Schmidt, B.; Gellhaus, A. Predictive value of sFlt-1, PlGF, sFlt-1/PlGF ratio and PAPP-A for late-onset preeclampsia and IUGR between 32 and 37 weeks of pregnancy. Pregnancy Hypertens. 2018, 12, 124–128. [Google Scholar] [CrossRef]
- Herraiz, I.; Simón, E.; Gómez-Arriaga, P.I.; Quezada, M.S.; García-Burguillo, A.; López-Jiménez, E.A.; Galindo, A. Clinical implementation of the sFlt-1/PlGF ratio to identify preeclampsia and fetal growth restriction: A prospective cohort study. Pregnancy Hypertens. 2018, 13, 279–285. [Google Scholar] [CrossRef]
- Perry, H.; Binder, J.; Kalafat, E.; Jones, S.; Thilaganathan, B.; Khalil, A. Angiogenic Marker Prognostic Models in Pregnant Women With Hypertension. Hypertension 2020, 75, 755–761. [Google Scholar] [CrossRef]
- Kienast, C.; Moya, W.; Rodriguez, O.; Jijón, A.; Geipel, A. Predictive value of angiogenic factors, clinical risk factors and uterine artery Doppler for pre-eclampsia and fetal growth restriction in second and third trimester pregnancies in an Ecuadorian population. J. Matern. Fetal Neonatal Med. 2016, 29, 537–543. [Google Scholar] [CrossRef]
- Myatt, L.; Webster, R.P. Vascular biology of preeclampsia. J. Thromb. Haemost. 2009, 7, 375–384. [Google Scholar] [CrossRef]
- Travaglino, A.; Raffone, A.; Saccone, G.; Migliorini, S.; Maruotti, G.M.; Esposito, G.; Mollo, A.; Martinelli, P.; Zullo, F.; D’Armiento, M. Placental morphology, apoptosis, angiogenesis and epithelial mechanisms in early-onset preeclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 234, 200–206. [Google Scholar] [CrossRef]
- Ortega, M.A.; Asúnsolo, Á.; Leal, J.; Romero, B.; Alvarez-Rocha, M.J.; Sainz, F.; Álvarez-Mon, M.; Buján, J.; García-Honduvilla, N. Implication of the PI3K/Akt/mTOR Pathway in the Process of Incompetent Valves in Patients with Chronic Venous Insufficiency and the Relationship with Aging. Oxid. Med. Cell Longev. 2018, 2018, 1495170. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Coulouris, G.; Zaretskaya, I.; Cutcutache, I.; Rozen, S.; Madden, T.L. Primer-BLAST: A tool to design target-specific primers for polymerase chain reaction. BMC Bioinform. 2012, 13, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, M.A.; Romero, B.; Asúnsolo, Á.; Sola, M.; Álavrez-Rocha, M.J.; Sainz, F.; Álavrez-Mon, M.; Buján, J.; García-Honduvilla, N. Patients with Incompetent Valves in Chronic Venous Insufficiency Show Increased Systematic Lipid Peroxidation and Cellular Oxidative Stress Markers. Oxid. Med. Cell Longev. 2019, 2019, 5164576. [Google Scholar] [CrossRef] [PubMed]
- Cristóbal, L.; de Los Reyes, N.; Ortega, M.A.; Álvarez-Mon, M.; García-Honduvilla, N.; Buján, J.; Maldonado, A.A. Local Growth Hormone Therapy for Pressure Ulcer Healing on a Human Skin Mouse Model. Int. J. Mol. Sci. 2019, 20, 4157. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| GENE | SEQUENCE Fwd (5′→3′) | SEQUENCE Rev (5′→3′) | Temp |
|---|---|---|---|
| TBP | TGCACAGGAGCCAAGAGTGAA | CACATCACAGCTCCCCACCA | 60 °C |
| CD-31 | ACTGCACAGCCTTCAACAGA | TTCTTCCATGGGGCAAG | 60 °C |
| D2-40 | TGACTCCAGGAACCAGCGAAG | GCGAATGCCTGTTACACTGTTGA | 50 °C |
| Flt-1 | TCAGCTACTGGGACACCGG | CCTGAACTAGATCCTGTGAGAAGCA | 60 °C |
| PIGF | CAGAGGTGGAAGTGGTACCCTTCC | CGGATCTTTAGGAGCTGCATGGTGAC | 58 °C |
| A | ||||
| Antigen | Species | Dilution | Provider | Protocol specifications |
| CD-31 | Mouse monoclonal | 1:100 | P-8590 (Sigma-Aldrich) | |
| D2-40 | Mouse monoclonal | 1:100 | M3619 (Agilent, Dako) | |
| Flt-1 | Mouse monoclonal | 1:500 | sc-271789 (Santa cruz biotechnology) | Citrate tampon in heat (pH =6) |
| PlGF | Rabbit polyclonal | 1:250 | ab230516 (Abcam) | EDTA pH = 9 before incubation with blocking solution |
| B | ||||
| Antigen | Species | Dilution | Provider | Protocol specifications |
| IgG (Mouse) | Goat polyclonal | 1:300 | Sigma-Aldrich (F2012/045K6072 ) | |
| IgG (Rabbit) | Mouse polyclonal | 1:1000 | Sigma-Aldrich (RG-96/ B5283) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, M.A.; Saez, M.A.; Fraile-Martínez, O.; Asúnsolo, Á.; Pekarek, L.; Bravo, C.; Coca, S.; Sainz, F.; Mon, M.Á.-; Buján, J.; et al. Increased Angiogenesis and Lymphangiogenesis in the Placental Villi of Women with Chronic Venous Disease during Pregnancy. Int. J. Mol. Sci. 2020, 21, 2487. https://doi.org/10.3390/ijms21072487
Ortega MA, Saez MA, Fraile-Martínez O, Asúnsolo Á, Pekarek L, Bravo C, Coca S, Sainz F, Mon MÁ-, Buján J, et al. Increased Angiogenesis and Lymphangiogenesis in the Placental Villi of Women with Chronic Venous Disease during Pregnancy. International Journal of Molecular Sciences. 2020; 21(7):2487. https://doi.org/10.3390/ijms21072487
Chicago/Turabian StyleOrtega, Miguel A, Miguel A Saez, Oscar Fraile-Martínez, Ángel Asúnsolo, Leonel Pekarek, Coral Bravo, Santiago Coca, Felipe Sainz, Melchor Álvarez- Mon, Julia Buján, and et al. 2020. "Increased Angiogenesis and Lymphangiogenesis in the Placental Villi of Women with Chronic Venous Disease during Pregnancy" International Journal of Molecular Sciences 21, no. 7: 2487. https://doi.org/10.3390/ijms21072487