The IL-17A/IL-17RA Axis Is Not Related to Overall Survival and Cancer Stem Cell Modulation in Pancreatic Cancer

 and
and 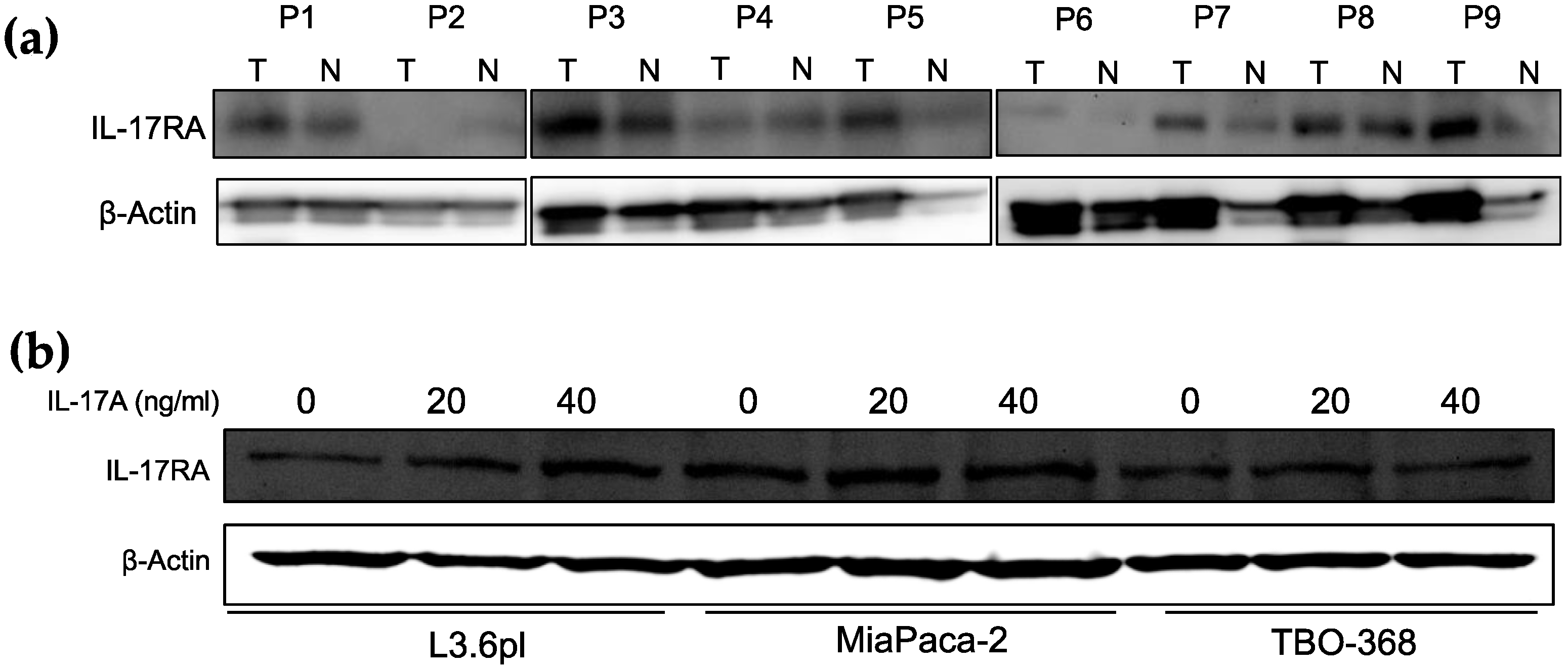{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. High IL-17A and High IL-17RA Expression Does Not Correlate with Overall Survival in Pancreatic Ductal Adenocarcinoma (PDAC) Patients
2.2. Treatment with IL-17A Does Not Induce Stem Cell Features in Pancreatic Cancer Cells In Vitro
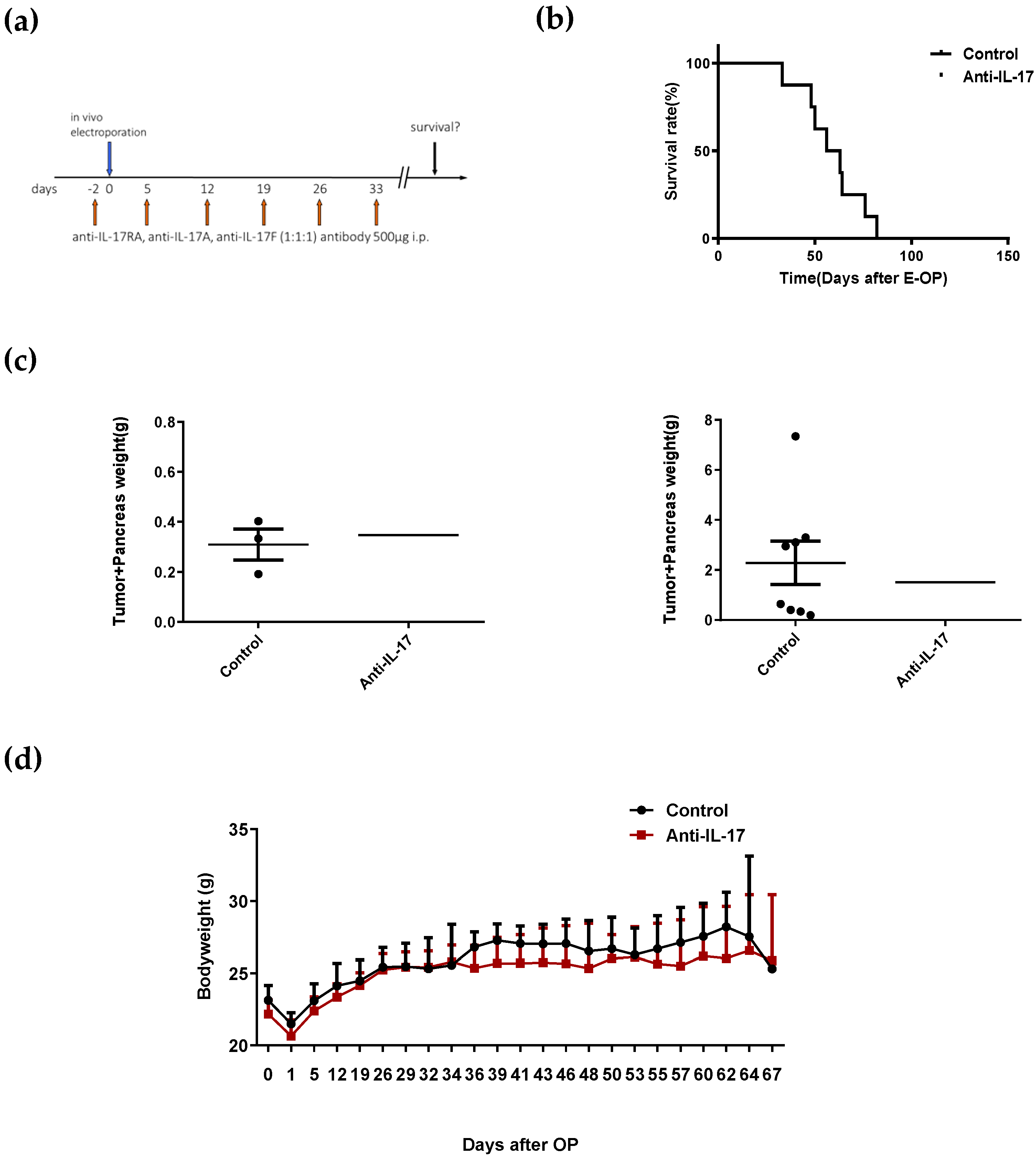
2.3. Blockade of IL-17 with Antibodies Does Not Improve Survival in a Mouse Model of Pancreatic Cancer
3. Discussion
4. Materials and Methods
4.1. Publicly Available Data Analysis
4.2. Cells and Animals
4.3. Pancreatic Cancer Animal Model
4.4. Sphere-Formation Assays
4.5. Wound-Healing Assay
4.6. Immunohistochemical Staining (IHC)
4.7. Flow Cytometry Analysis
4.8. Statistics
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McAllister, F.; Bailey, J.M.; Alsina, J.; Nirschl, C.J.; Sharma, R.; Fan, H.; Rattigan, Y.; Roeser, J.C.; Lankapalli, R.H.; Zhang, H.; et al. Oncogenic Kras activates a hematopoietic-to-epithelial IL-17 signaling axis in preinvasive pancreatic neoplasia. Cancer Cell 2014, 25, 621–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valle, S.; Martin-Hijano, L.; Alcala, S.; Alonso-Nocelo, M.; Sainz, B., Jr. The Ever-Evolving Concept of the Cancer Stem Cell in Pancreatic Cancer. Cancers (Basel) 2018, 10, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smigiel, J.M.; Parameswaran, N.; Jackson, M.W. Targeting Pancreatic Cancer Cell Plasticity: The Latest in Therapeutics. Cancers (Basel) 2018, 10, 14. [Google Scholar] [CrossRef] [Green Version]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.; Hwu, W.J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [Green Version]
- Le, D.T.; Lutz, E.; Uram, J.N.; Sugar, E.A.; Onners, B.; Solt, S.; Zheng, L.; Diaz, L.A., Jr.; Donehower, R.C.; Jaffee, E.M.; et al. Evaluation of ipilimumab in combination with allogeneic pancreatic tumor cells transfected with a GM-CSF gene in previously treated pancreatic cancer. J. Immunother. 2013, 36, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zoltan, M.; Riquelme, E.; Xu, H.; Sahin, I.; Castro-Pando, S.; Montiel, M.F.; Chang, K.; Jiang, Z.; Ling, J.; et al. Immune Cell Production of Interleukin 17 Induces Stem Cell Features of Pancreatic Intraepithelial Neoplasia Cells. Gastroenterology 2018, 155, 210–223. [Google Scholar] [CrossRef] [PubMed]
- Gendoo, D.M.A.; Zon, M.; Sandhu, V.; Manem, V.S.K.; Ratanasirigulchai, N.; Chen, G.M.; Waldron, L.; Haibe-Kains, B. MetaGxData: Clinically Annotated Breast, Ovarian and Pancreatic Cancer Datasets and their Use in Generating a Multi-Cancer Gene Signature. Sci. Rep. 2019, 9, 8770. [Google Scholar] [CrossRef] [Green Version]
- Bruns, C.J.; Harbison, M.T.; Kuniyasu, H.; Eue, I.; Fidler, I.J. In vivo selection and characterization of metastatic variants from human pancreatic adenocarcinoma by using orthotopic implantation in nude mice. Neoplasia 1999, 1, 50–62. [Google Scholar] [CrossRef] [Green Version]
- Gurlevik, E.; Fleischmann-Mundt, B.; Brooks, J.; Demir, I.E.; Steiger, K.; Ribback, S.; Yevsa, T.; Woller, N.; Kloos, A.; Ostroumov, D.; et al. Administration of Gemcitabine After Pancreatic Tumor Resection in Mice Induces an Antitumor Immune Response Mediated by Natural Killer Cells. Gastroenterology 2016, 151, 338–350. [Google Scholar] [CrossRef] [Green Version]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Betzler, C.; Lohneis, P.; Popp, M.C.; Qin, J.; Kalinski, T.; Wartmann, T.; Bruns, C.J.; Zhao, Y.; Popp, F.C. The IL-17A/IL-17RA Axis Is Not Related to Overall Survival and Cancer Stem Cell Modulation in Pancreatic Cancer. Int. J. Mol. Sci. 2020, 21, 2215. https://doi.org/10.3390/ijms21062215
Li J, Betzler C, Lohneis P, Popp MC, Qin J, Kalinski T, Wartmann T, Bruns CJ, Zhao Y, Popp FC. The IL-17A/IL-17RA Axis Is Not Related to Overall Survival and Cancer Stem Cell Modulation in Pancreatic Cancer. International Journal of Molecular Sciences. 2020; 21(6):2215. https://doi.org/10.3390/ijms21062215
Chicago/Turabian StyleLi, Jiahui, Christopher Betzler, Philipp Lohneis, Marie Christine Popp, Jiwei Qin, Thomas Kalinski, Thomas Wartmann, Christiane J. Bruns, Yue Zhao, and Felix C. Popp. 2020. "The IL-17A/IL-17RA Axis Is Not Related to Overall Survival and Cancer Stem Cell Modulation in Pancreatic Cancer" International Journal of Molecular Sciences 21, no. 6: 2215. https://doi.org/10.3390/ijms21062215